
Abstract
Opioids were declared a public health emergency in British Columbia, Canada, in 2016, and from that year through 2021, 29,894 Canadians lost their lives to opioid overdoses. More than two-thirds of those victims were employed in the five years prior to their deaths, and this study aims to quantify their lost productivity to the Canadian economy. We apply two human capital model variants in our analysis, projecting forward the future economic output of individuals who died from opioids, from their deaths to what would have been their eventual retirements, based on the industries in which they were employed. The total estimated productivity loss to Canada is at least $8.8 billion, with the equivalent “value of statistical life” calculations an order of magnitude higher; these are based on estimates of the amount of money that individuals would pay to avoid death. Our results challenge the notion that the opioid crisis predominantly affects unproductive members of society.
Keywords
The opioid crisis is present in countries across the globe, but the magnitude of its effects is highest in North America. Canada has closely paralleled the U.S. in both the timing and the severity of its opioid crisis. While Massachusetts was the first U.S. state to declare opioids an emergency to public health on March 27, 2014, British Columbia was the first Canadian province to do so only two years later, on April 14, 2016. However, the U.S. declared a nationwide public health emergency just a year and a half after that, on October 26, 2017, and Canada has yet to reciprocate, but such an announcement seems almost inevitable.
The U.S. and Canada have the first and second highest number of per capita opioid users globally (Belzak and Halverson 2018). Historically, up to one in five Canadians were using a medical-grade opioid by 2010 (Fischer, Pang, and Tyndall 2019). Similarly, one in four Americans were prescribed an opioid medication annually, and 259 million opioid prescriptions had already been dispensed by 2012. Even worse, the U.S. and Canada held the dubious distinction of having had the first and second highest opioid-related deaths per million inhabitants across twenty-five countries from 2011 to 2016 (Organisation for Economic Co-operation and Development [OECD] 2019). And unfortunately, this issue has not abated, with both the U.S. and Canada still having the highest amounts of drug overdose deaths in the early 2020s, even in conjunction with the COVID-19 pandemic and its death toll.
The opioid crisis has been so severe in magnitude in North America that it caused overall declines in life expectancy and increases in overall mortality rates. Illicit drug deaths are now the number one cause of unnatural deaths in both Canada and the U.S. More generally, the “deaths of despair” from alcohol, opioids, and suicide have been linked to an alarming and dramatic increase in the mortality rate between 1999 and 2013 in the U.S., which was especially pronounced among White non-Hispanic Americans (Case and Deaton 2015). This trend for the U.S. showed a progression when updated to 2015; and while Canada’s mortality rate was lower, the rate of its decrease was trending downward, which raised a warning flag (Case and Deaton 2017).
One way to quantify the magnitude of such a loss of life is through the labor market, which has already been previously linked to opioids in several U.S. studies (one of the four main conclusions of the review by Maclean et al. 2021). For example, local increases in per capita opioid prescriptions have been subsequently associated with reduced labor force participation rates (Aliprantis, Fee, and Schweitzer 2019; Krueger 2017; Harris et al. 2019; Powell 2021), and opioids have had a small positive effect on the employment-to-population ratio for women but not for men (Currie, Jin, and Schnell 2019). Looking the other way around, a one percent increase in the local county unemployment rate was associated with a three-and-a-half percent increase in the opioid death rate (Hollingsworth, Ruhm, and Simon 2017). And, opioid overdose deaths significantly increased in U.S. counties within five years of having an automotive plant closure (Venkataramani et al. 2020).
In the current study, the labor market is used to quantify the impact the opioid crisis has had in Canada through several calculations of lost labor productivity among its opioid overdose victims. Two variants of the human capital (HC) model, one based on the industry the individuals were employed in prior to death and one based on the age of the individual at the time of death, are applied under varying and alternate assumptions. These losses are then compared with the equivalent value of statistical life calculation. Quantifying lost labor productivity to the Canadian economy due to premature deaths from opioids is an important step in understanding the scale and scope of the opioid crisis, with lost labor productivity often overlooked given the belief that the opioid crisis primarily affects unproductive members of society.
The findings of the current study challenge that notion of opioid users not being productive, as it will indeed be shown that over two-thirds of opioid overdose victims in Canada were employed and contributing to the economy in the five years before they died. We particularly focus on the four-year period covering the years from when British Columbia declared opioids a public health emergency in 2016, up to the onset of the COVID-19 pandemic at the end of 2019, during which time 15,393 Canadians prematurely died from opioid overdoses.
While the entire human cost of the opioid crisis is immeasurable, we calculate HC productivity losses ranging from $8.8 billion to $10.9 billion, and comparable value of statistical life losses ranging from $65.7 billion to $178.3 billion.1 Once the entire burden of the economic loss is understood, the resources needed to mitigate the loss of life and manage the crisis can more appropriately be allocated, as we additionally highlight the steps policy-makers can take to reduce illicit drug deaths. The study concludes by examining the loss calculations and recommendations in several different ways, most notably with that of the U.S.
Getting Specific about Canadian Opioid Deaths
Although opioids were first designated as a crisis in Canada in 2016, when a public health emergency was declared under the Public Health Act in British Columbia on April 14th, its origins began much earlier. Between 1990 and 2014, the years of life lost due to opioid-related mortality increased by 142 percent in Canada, as compared to a 10 percent increase globally (Orpana et al. 2018). Interestingly, the opioid-related death rates per 100,000 individuals for Canada overtook the global rates in the mid-1990s, between 1996 and 1997, which was true for both males and females.
Another earlier study looking at the burden of premature opioid-related mortality found that in Ontario, Canada’s most populous province, there were 5,935 premature opioid deaths between 1991 and 2010 (Gomes et al. 2014). These deaths represented a 242 percent increase in the mortality rate, based on data from the Office of the Chief Coroner for Ontario. The authors also noted an increase in the dispensing of opioid prescriptions. This finding would suggest that opioid use disorder was a growing problem well before 2016 and continues presently.
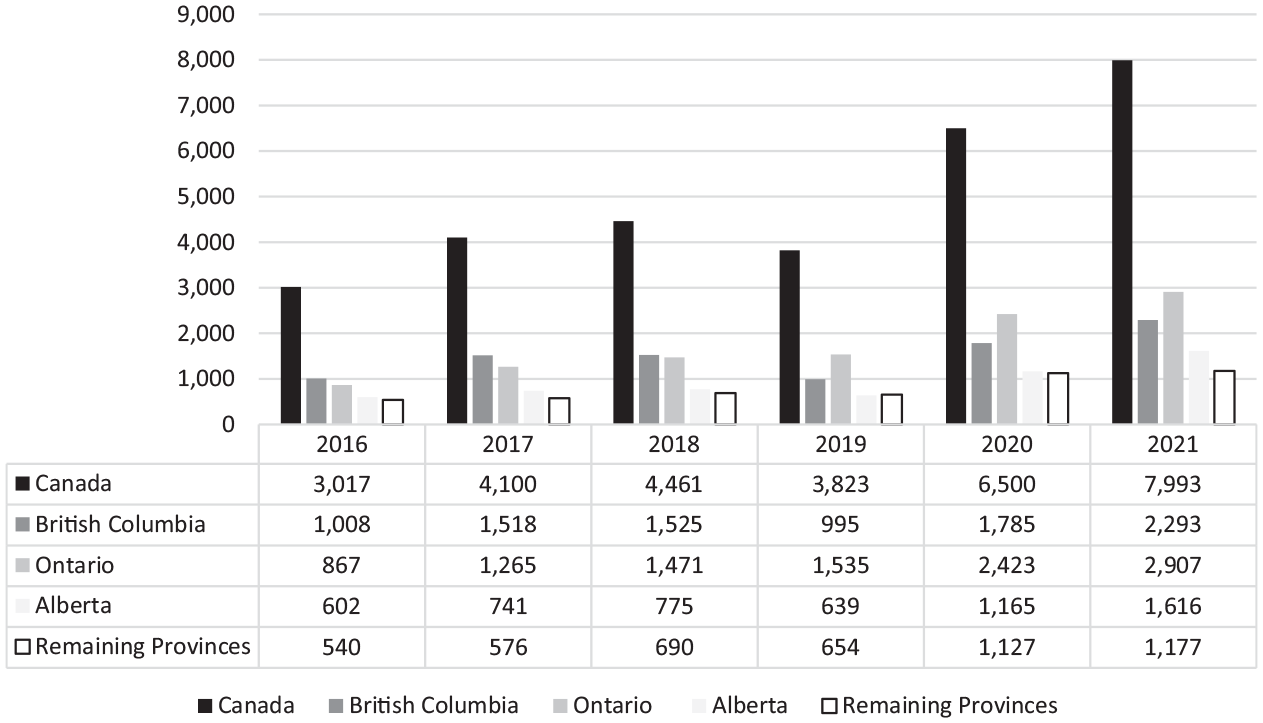
Our study begins by showing all of the opioid-related deaths for Canada in the post-crisis declaration period from 2016 to 2021 using data from the Public Health Agency of Canada (2020, 2022), as displayed in Figure 1. Over this period, a total of 29,894 Canadians died from opioid overdoses, moving from 3,017 deaths in 2016 and increasing to 7,993 by 2021. This is a 165 percent increase over this six-year period.
Opioid-Related Deaths in Canada, 2016–2021
More specifically, however, our study focuses on the post-crisis declaration and pre-COVID-19 period, that is, the 15,393 deaths that occurred in Canada from 2016 to 2019. To put this in perspective with the United States, opioids were involved in 49,860 American overdose deaths in 2019, as compared with the 3,823 Canadian opioid-related deaths that year, which is 7.6 percent that of the U.S. Also in that year, the Canadian population was 37.6 million versus the U.S. population of 328.3 million, which is 11.5 percent. Taking the populations differences into account, Canada’s national opioid mortality rate was 9.8 deaths per 100,000 individuals, and the mortality rate in the United States was 21.6 deaths per 100,000: more than double.
Within Canada, from 2016 through 2018, the province of British Columbia led in annual deaths, comprising over a third of deaths nationally, with Ontario and Alberta following suit, as seen in Figure 1. However, in 2019, opioid-related deaths were highest in the most populous province of Ontario, followed by British Columbia and Alberta, respectively. That said, given that Ontario’s percentage of opioid deaths in that year (~40 percent) roughly match its share of Canada’s population (~38 percent), British Columbia was still the hardest-hit province at 19.9 deaths per 100,000 people, followed by 14.3 for Alberta, and then 10.5 in Ontario. Saskatchewan, although not isolated in the figure, was the only other province to be above the national average, at 10.0 opioid-related deaths per 100,000. In contrast, West Virginia was the hardest-hit state within the U.S. at 52.8 deaths per 100,000 in population, with Delaware and the District of Columbia next highest at 48.0 and 43.2, respectively.
It is unclear why the westernmost provinces of British Columbia and Alberta have significantly higher per capita opioid death rates. It has been suggested that the gap between Central Canada (Ontario) and Western Canada (British Columbia and Alberta) may come down to different opioid prescribing practices, opioid use patterns, or even the respective overall health between the two regions. For example, in the province of Quebec, which has far fewer opioid deaths, opioids are less frequently prescribed, potentially due to greater access to psychotherapy, physiotherapy, and other non-drug treatments for pain (Vogel 2016).
Although our focus in this study remains on the post-crisis but prepandemic period, the COVID-19 pandemic, which began in early 2020, has seemingly exacerbated opioid use disorders (OUDs) and fatal opioid overdoses in Canada. In June 2020 alone, 183 people in the Canadian province of British Columbia lost their lives to the opioid crisis—a 141 percent spike over June of the previous year in 2019 (76 deaths) and the highest single-month death rate on record at the time. Conversely, during the entire summer of 2020, 284 people in British Columbia lost their lives to COVID-19 (Norton and Kerr 2020).
In Ontario, 2,423 people died from opioid overdoses in 2020. This was a 60 percent increase from 2019 (1,517 deaths) and a 64 percent increase from 2018 (1,475 deaths). Possible explanations for this sudden and sharp rise in opioid deaths include physical distancing and isolation, increased drug toxicity from disrupted drug supplies (i.e., sudden border and travel restrictions), housing instability, as well as worsening mental health, all of which were brought on by the COVID-19 pandemic (Friesen et al. 2021).
Linking Opioid Deaths to Losses in the Labor Market
Every one of the 15,393 deaths that occurred in Canada in the pre-COVID-19 and post-crisis declaration years from 2016 to 2019 was a tragic social loss to their families and friends that cannot be quantified. But many of these individuals were also making contributions to society through their time and energy devoted to pay in the labor market. This type of economic loss can be quantified, as the premature deaths will result in an aggregate loss of economic output through all those individual years of potential productivity.
The main approach of our study is to calculate the economic footprint of the opioid crisis for Canada using what is known as an HC model. The HC model captures society’s losses when an employed person dies by modeling an individual’s future economic contributions, also known as years of potential life lost. The HC model was developed by researchers in the 1960s who sought a robust way of measuring the economic burden suffered by society due to workplace deaths and injuries. These researchers answered this question by framing it in the following perspective: if a workplace death could be somehow prevented, how much would this person, now alive, have been able to contribute to society?
The HC model that we now follow for Canada is described by the Institut de recherche Robert-Sauvé en santé et en sécurité du travail (IRSST), which was established in Quebec in 1980 to study occupational injury and death (IRSST 2011). This type of model is also used by the Centers for Disease Control and Prevention (CDC) and the National Institute for Occupational Safety and Health (NIOSH) to measure the economic burden of occupational fatal injuries in the United States (CDC 2017). The HC model used by the CDC is very similar to that used by the IRSST, but the U.S. considers race and lost household production, whereas the Canadian studies do not.
To date, there is an absence of literature quantifying these types of losses from the labor market in Canada due to premature death from OUDs. Our study uses data from publicly available sources, which include Statistics Canada, the British Columbia Coroner’s service, the Canadian Revenue Agency, and other governmental agencies (Public Health Agency of Canada 2020, 2022; Statistics Canada 2018), to fill in the gap in the literature. These data allow us to build a picture of these Canadian opioid overdose victims as contributing members of society.
Unfortunately, however, there are two broad limitations of the data. First, the industry of employment before the death of these overdose victims is not available at a national level, but it is available at the provincial level for British Columbia. Second, the data on overdose victims is not individualized, but it is rather reported in averages and ranges, such as in 10-year age bands. Each of these limitations leads us to quantify the loss through two different HC models: one based on industry, and one based on age.
Cost of burden analysis and the associated assumptions that follow are often unavoidable, so this study performs several analyses using varying assumptions, including a different approach altogether called the value of statistical life, and compares the results. The value of statistical life is a tool that economists have developed to quantify the value of a human life in a particular group, based on the choices that people in that group make in order to avoid risk that might result in a death among them.
Extrapolating Industry Employed from Province to Nation
The first HC model uses earnings derived from the industry in which the overdose victim was previously employed. Earnings derived from industry estimates can potentially provide a better picture of an OUD victim’s actual output. It will additionally use assumptions, such as an average retirement age of 64 and that the average victim died at age 42. It relies on average industry earnings and does not account for nonlinearity in earnings through time. Because of this, corrections are provided to better model the projected streams of lost output.
As previously mentioned, the only province with robust industry of employment data of fatal opioid overdose victims is British Columbia. While the Public Health Agency of Canada collects data from other provinces, this data is unfortunately quite limited. For example, the province of Ontario tracks only basic information, such as the number of deaths and age groupings. Alternatively, British Columbia’s data is of much higher quality, as it includes provincial information sharing done between agencies, such as Statistics Canada, the Canada Revenue Agency (CRA), health agencies, the Royal Canadian Mounted Police, and the Coroner’s service.
Due to the absence of robust national data on the industries of overdose victims, the Canada-wide industry data for this study is extrapolated from British Columbia’s data. This extrapolation of British Columbian data for the absent national data can be considered as an acceptable substitute for Canada for two reasons. First, as previously shown in Figure 1, the province of British Columbia is overly represented among opioid deaths in Canada, comprising approximately one-third. Given that its population is about 13 percent of Canada’s (~5 million to ~38 million), it results in BC having the highest death rate from opioids per 100,000 individuals. Second, the labor force characteristics between British Columbia and Canada will be shown to be relatively homogenous. For example, from 1999 to 2019, the average unemployment rate for Canada was 7 percent, whereas it was 6.5 percent for British Columbia, with only a half a percentage point difference over 20 years.
As for the general industry composition, Canada’s goods-producing sector makes up 21.2 percent of the workforce, whereas it is 19.8 percent for British Columbia—a 1.4 percentage point difference. Conversely, the service sector makes up 79.8 percent of the workforce in Canada to British Columbia’s 80.2 percent. One lone NAICS (North American Industry Classification System) industry has a larger than 1.5 percent difference between Canada and the province of British Columbia, manufacturing, which makes up 9.4 percent of the national workforce compared to 6.8 percent in British Columbia—a 2.6 percent difference. But by and large, the labor force characteristics by industry between Canada and British Columbia are similar (see Statistics Canada, Labour Force Survey, Table 14-10-0023-01).
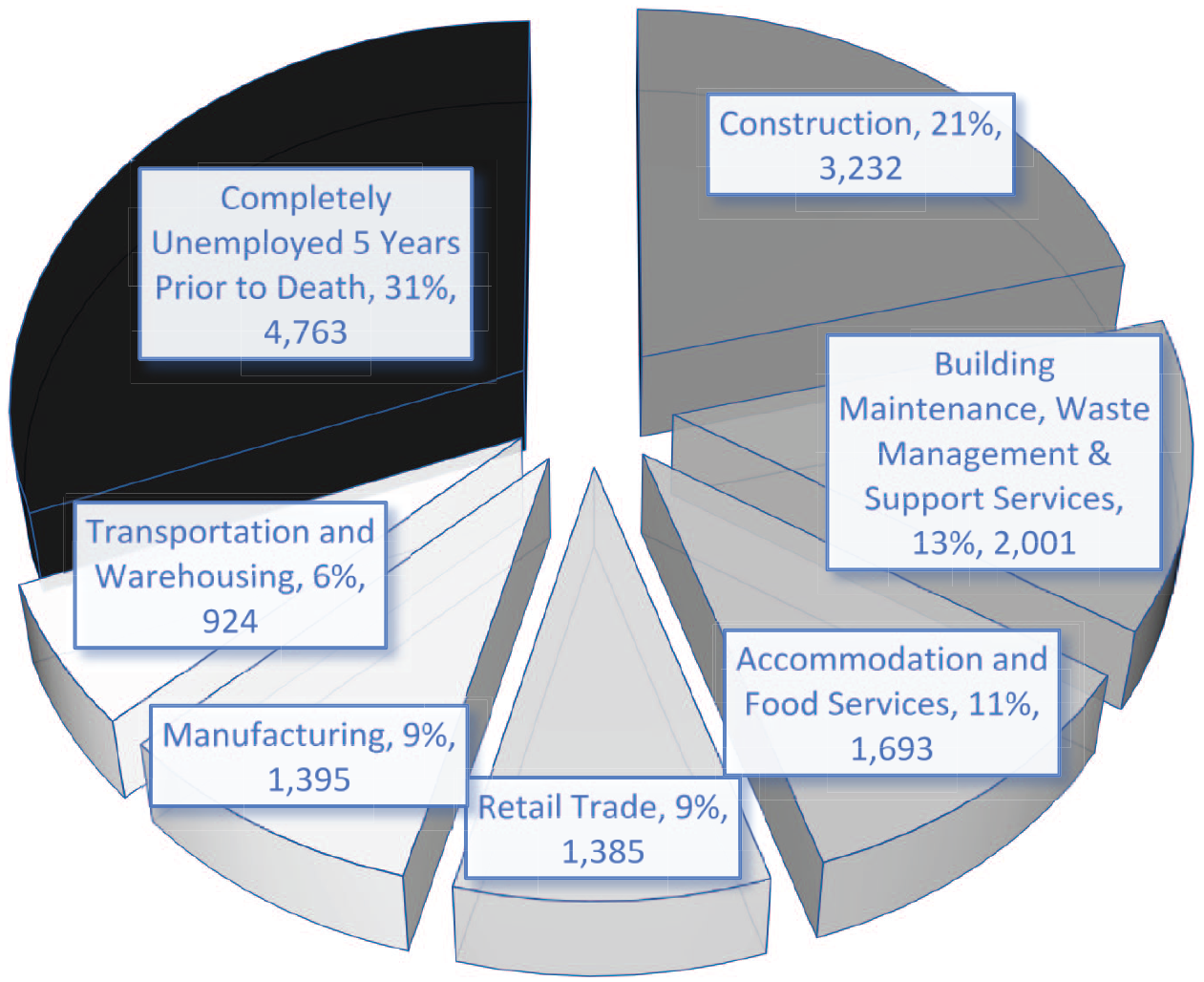
For our victims of opioid-related deaths, the composition of employment in their last main job in the five years prior to death is shown in percentages for British Columbia, along with the representative relative Canadian opioid death counts, in Figure 2. Approximately 69 percent (69.06 percent) of British Columbia opioid overdose victims were employed in the five years before dying (2011–2016). Multiplying that percentage by the national 15,393 opioid overdose victims results in approximately 10,630 of these Canadians being employed sometime in the five years before they died, which is also done for each of their industries. 2 Therefore, the figure reports industry counts that reflect the total number of nationally represented employed victims. This also means that approximately 31 percent (30.94 percent) were unemployed in the five years before they died, resulting in a count of approximately 4,763 of the Canadian victims.
Industries of Last Main Job in the Five Years prior to Death from British Columbia, 2011–2016
Among the 69 percent of employed victims, six broad industries are represented in Figure 2: accommodation and food services (11 percent); building maintenance, waste management, and support services (13 percent); construction (21 percent); manufacturing (9 percent); retail trade (9 percent); and transportation and warehousing (6 percent). There is an obvious overrepresentation of construction workers among opioid overdose fatalities at 21 percent or 3,232 of the victims across Canada, an industry where skillsets can take years to acquire and develop. This is perhaps not that surprising when considering that an average of 74 percent of opioid overdose victims were male and construction is a male-dominated industry.
Loss of Canadian Productivity Using Last Industry Employed
Each death from an employed overdose victim irreversibly depletes Canada’s supply of labor and trained employees, hence the “human capital” loss component, as measured by the HC model. To perform the first HC calculation to capture long-term lost productivity, the average annual industry earnings of the 10,630 working overdose victims are projected forward in time and summed from the time of death, which we set to 42 years old, until age 64, which is the current average Canadian retirement age.
Because the average overdose victim was 42 at the time of death, each victim lost an average of 22 working life years, or 22 years of potential life lost. Due to the absence of individual age data at the time of death, the mean values of age are used instead. And in Canada, goods-producing industries report later retirements than service-producing sectors. For example, the median age of retirement for a construction worker is 63.3 years, close to the average age of 64 (Statistics Canada 2003). Physically demanding industries, such as construction and agriculture, have retirement ages close to or exceeding the average retirement age of 64. For those reasons, this study uses 64 as the age of retirement.
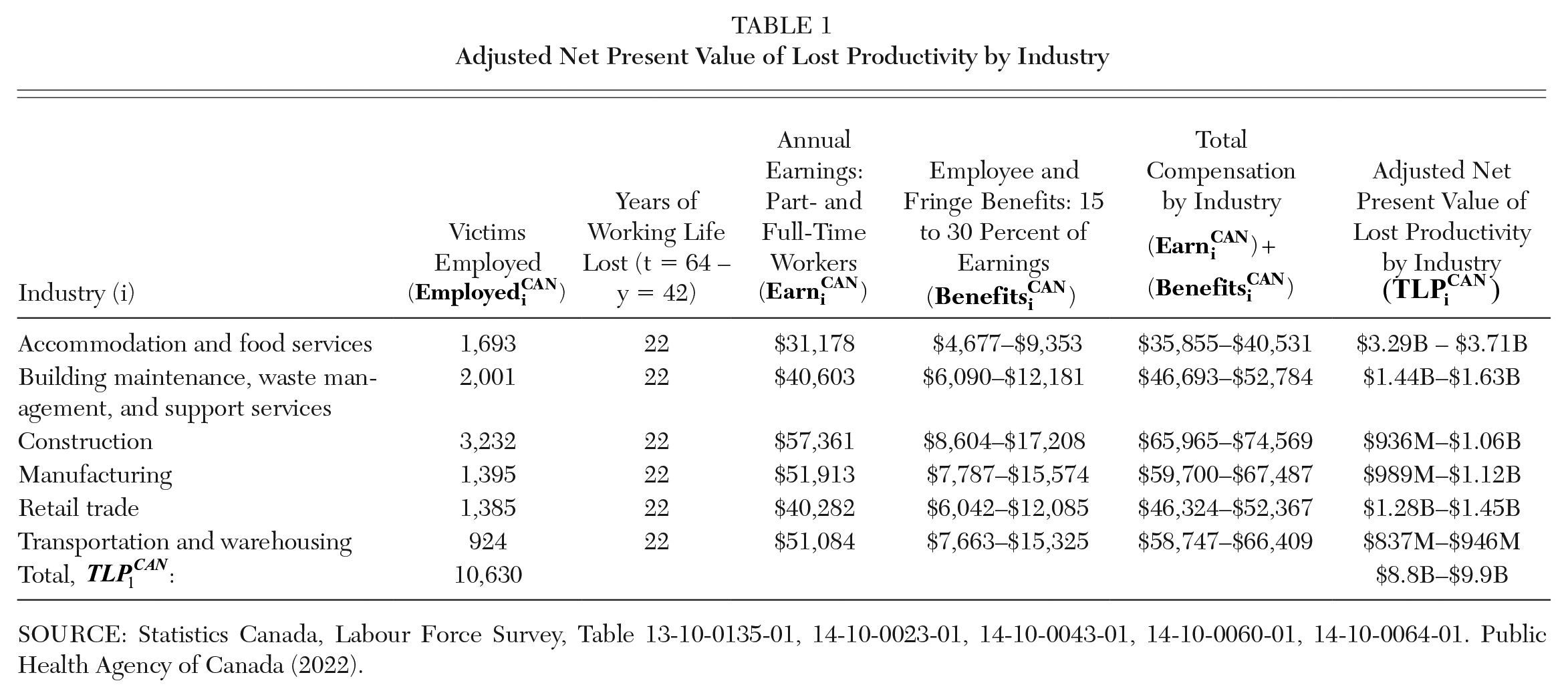
To calculate the annual earnings per employed overdose victims, we use the average hourly earnings of the victim’s industry multiplied by the average hours worked per week and the number of weeks worked. 3 The projected workweek is set to 37.7 hours, which was the usual average hours worked for both full- and part-time employees in Canada in 2018. In addition, a 50-week work year is used out of the 52 weeks each year to account for vacation time. These earnings streams by industry are displayed in the fourth column of Table 1.
Adjusted Net Present Value of Lost Productivity by Industry
SOURCE: Statistics Canada, Labour Force Survey, Table 13-10-0135-01, 14-10-0023-01, 14-10-0043-01, 14-10-0060-01, 14-10-0064-01. Public Health Agency of Canada (2022).
Earnings act as a proxy for lost productivity, because neoclassical economic theory dictates that workers are paid a value commensurate to their contribution to society. However, this does not tell the whole story. To fully quantify a worker’s total contribution to the economy, one must consider further remuneration beyond earnings alone. Examples of this include bonuses, allowances, commissions, employer pension payments, and benefits, among other things. To estimate this, this study uses a range which equates to 15-30 percent of annual earnings. 4 These employee and fringe benefits are shown by industry in the fifth column of Table 1. Putting earnings and benefits together results in the total compensation, shown in the sixth column of Table 1 by industry.
Therefore, the initial HC approach, for calculating total productivity losses based on the last industry employed from each of the components already introduced, is shown in equation (1), with some further adjustments to be discussed:
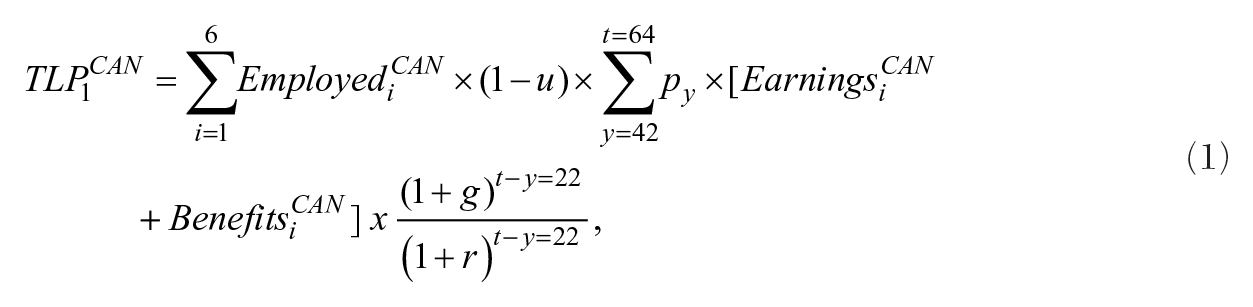
where TLP1CAN is the total adjusted net present value of lost productivity for all employed opioid overdose victims; Employedi CAN is the number of overdose victims employed by industry, i; Earningsi CAN is the annual earnings per employed overdose by the victim’s industry, i; Benefitsi CAN is the remunerations beyond earnings alone which amounts to a range between 15 and 30 percent of Earningsi CAN ; u is the average unemployment rate for Canada over the past 30 years (7.9 percent); t is the average Canadian retirement age of 64; y is the average age of the victim at time of death of 42; py is the probability of an opioid overdose victim of age y surviving to age 64 (88 percent); g is the average annual real earnings growth in Canada (1 percent); and r is the real discount rate (3 percent).
To better model a person’s lifetime earnings, adjustments were made to measure this annual stream of lost productivity more accurately, beyond the model used by the IRSST. For example, the IRSST model did not consider potential bouts of unemployment in an individual’s life that may be experienced even if they survived. Accounting for the direct (and even indirect) cost of lost earnings from unemployment in illness studies is common practice (Li, Gignac, and Anis 2006). This is done by reducing an opioid overdose victim’s expected economic output by the average unemployment rate over the preceding 30 years from 2019, which is 7.9 percent.
The probability of a victim avoiding their overdose fatality, but dying from natural mortality instead, is accounted for as well. This reduces a person’s expected lifetime economic output by another 7.3 percent. To capture the inevitable introduction of newer technologies and innovations into the Canadian workforce (e.g., the introduction of new computer software which makes employees more efficient), the projected annual real earnings growth of 1 percent is used as an approximation for the increases in workplace productivity that such innovations invariably provide (IRSST 2011).
Perhaps most importantly, the average 22 years of lost labor productivity that the estimated 10,630 employed opioid overdose victims lost is discounted through a finite geometric series using a real discount rate of 3 percent, which is common in Canadian workplace studies (IRSST 2011). This is done for all 10,630 employed victims and then summed for a final value. This delivers the net present discounted value of total lost productivity, TLP1CAN, which measures future projected economic output in terms of today’s dollars and lets us value future goods and services across periods for a more direct and accurate comparison. The final, adjusted value of lost productivity for the 15,393 Canadians who died from a fatal opioid overdose between the 2016 and 2019 calendar years is estimated to be between $8.8 and $9.9 billion using this HC variant.
Loss of Canadian Productivity Using Age at Time of Death
The second HC variant alternatively uses the average earnings by 10-year age groups. Unlike the previous model, earnings will now generally grow through time following a lifecycle earnings profile. Employee earnings rise with increasing work experience, before falling as an employee approaches retirement. The benefit of using annual earnings is that the lost labor output can better follow earnings growth through time, as earnings by age group are known. Again, corrections are provided to better model the projected streams of lost output.
Figure 3 displays the breakdown of the 15,393 overdose victims by age group. While these 10-year age ranges (i.e., 10–20 years old, 30–40 years old, etc.) provide some insight into the age distribution of opioid overdose victims, the utilization of averaged age data for parts of the forthcoming calculation limits sensitivity analysis in this study. The average age of death for overdose victims was 42 years, with aged 30 to 39 accounting for the largest proportion of opioid fatalities (27 percent), followed by 40- to 49- and 50- to 59-year-olds (each with 21 percent). In essence, the burden of this crisis has been on middle-aged individuals with around two decades of work experience. The only other age group with a large portion of opioid deaths was 20- to 29-year-olds (19 percent), whereas 0- to 19-year-olds and 60+-year-olds were in single digits (of 2 and 9 percent, respectively).
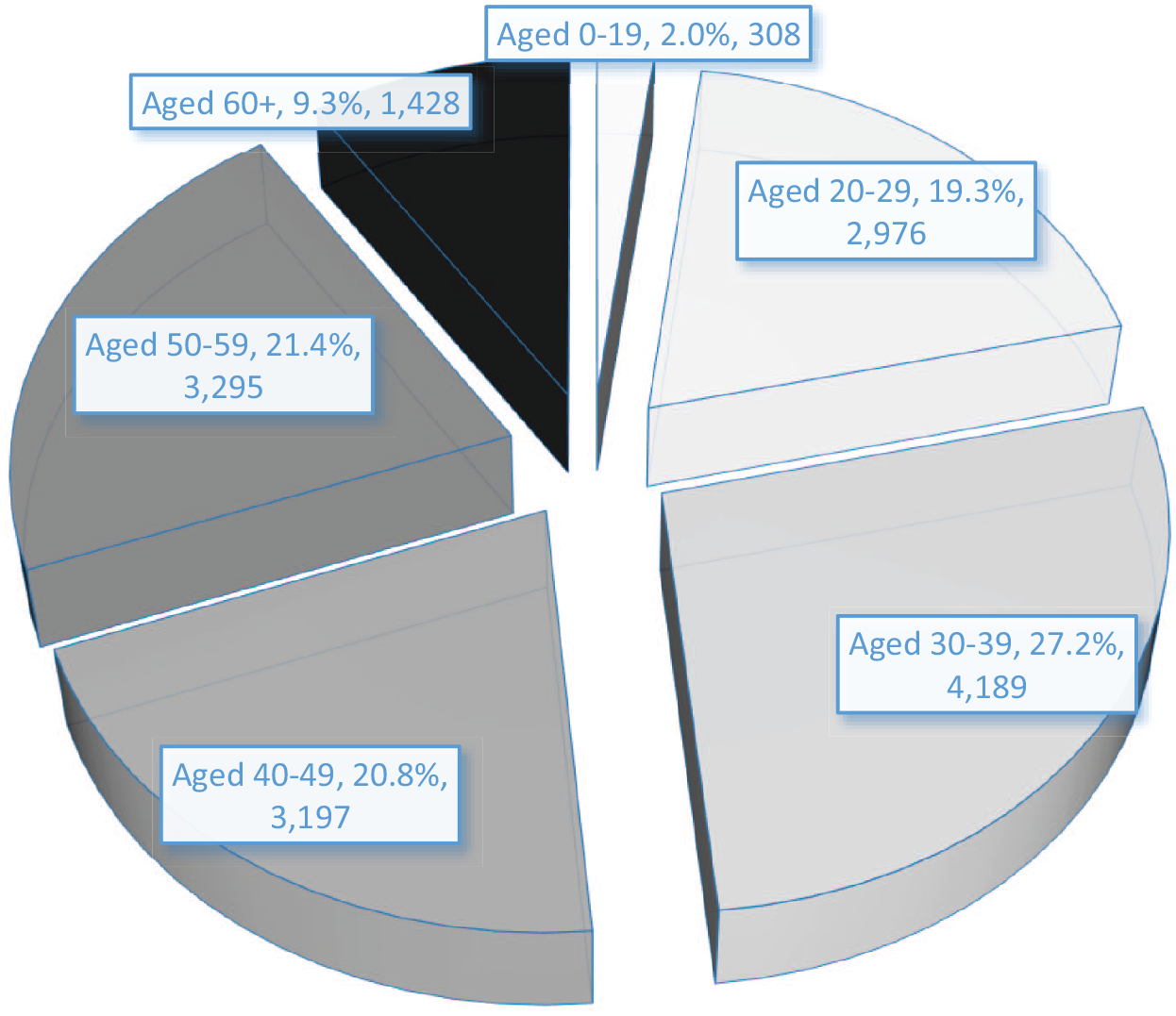
Breakdown of the 15,393 Opioid Overdose Victims by Age Group
This second analysis continues with the HC model previously presented; however, several assumptions are modified. While using wage profiles derived from industry data may have provided a superior OUD victim’s earnings profile, the analysis relied on mean rather than individualized data. For example, all victims were assumed to have lost an average of 22 years of labor productivity, and earnings were consistent over time. To test an alternative set of assumptions, deaths and average earnings by age group are used. While this still is not as precise as individualized death data, deaths by age group offer more granularity when calculating years of lost labor productivity.
For example, if an OUD victim died in the 20 to 29 age group, we would take the midpoint age (i.e., 25), and subtract it against 64, the average retirement age. On average, that would mean that a victim who died between 20 and 29 would lose 40 working years. The only exception to this is the 0 to 19 age group, because using the midpoint of 10 years would not make much sense. To overcome this, we set this midpoint to age 15, which is the first year to enter the working-age population in Canada. As such, 64 subtracted by 15 results in an average of 50 working years lost. This would make intuitive sense, because someone dying of an opioid overdose before the age of 19 essentially forfeits their entire working life.
The most significant change is that the second analysis will account for the nonlinearity of earnings through time, as presented in Table 2. This generally follows a lifecycle profile of earnings, with earnings rising with age, before falling as one approaches retirement. For example, someone aged 20 to 29 is expected to have average annual earnings of $31,900 over each of the 10 years. Conversely, someone aged 40 to 49 would be expected to have much higher average earnings of $64,650 over each of those 10 years. An OUD victim who died aged 20 to 29 would lose, on average, five years of earnings at $31,900 annually, $53,950 annually from 30 to 39, $64,650 annually from 40 to 49, $61,850 annually from 50 to 59, and around five years of earnings at $48,400 annually for ages 60+.
Adjusted Net Present Value of Lost Productivity by Age Group
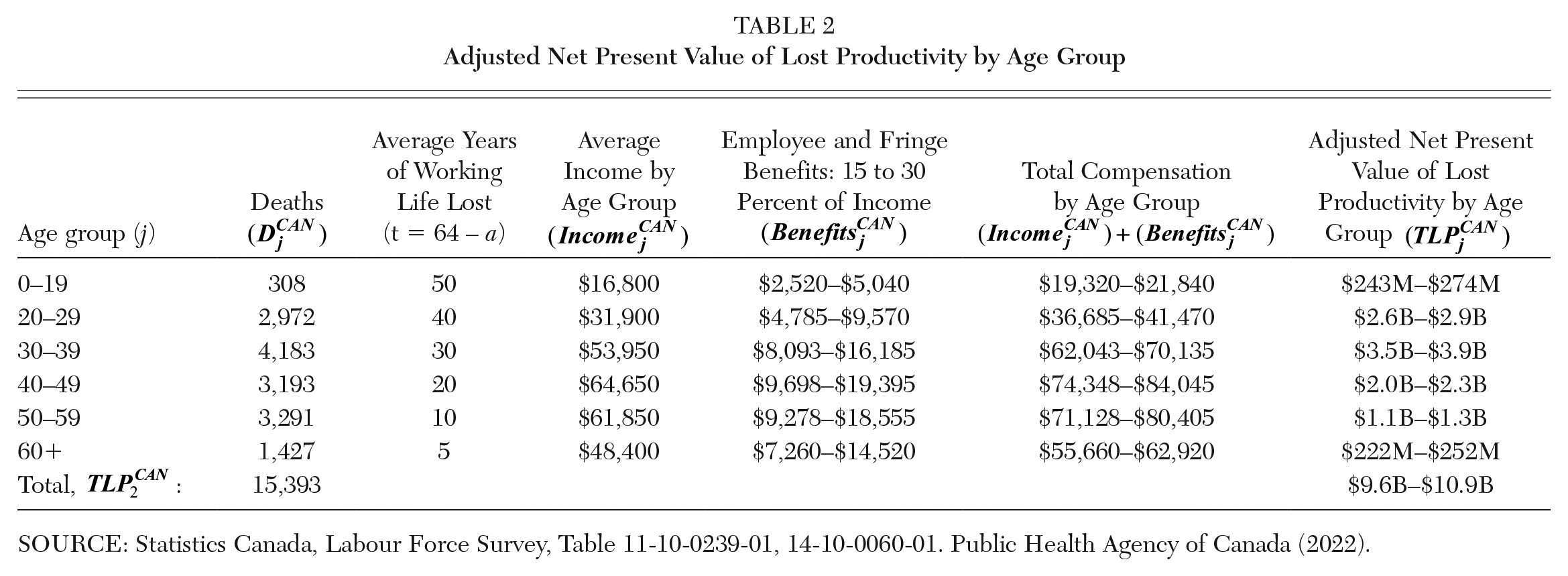
SOURCE: Statistics Canada, Labour Force Survey, Table 11-10-0239-01, 14-10-0060-01. Public Health Agency of Canada (2022).
To calculate the total lost labor productivity, equation (2) is used:

where TLP2CAN is the present discounted value of total lost productivity for all opioid overdose victims when measuring deaths by age group at time of death; Deathsj CAN refers to the number of OUD victims by age group, j; Earningsj CAN refers to the average income by age group, j; Benefitsj CAN refers to employee and fringe benefits which range from 15 to 30 percent of Earningsj CAN ; a refers to the midpoint age for age group, j; and with r and t referring to the real interest rate of 3 percent and time in years, respectively.
Further corrections include reducing an opioid overdose victim’s expected economic output by the average unemployment rate, u, which was 7.9 percent over the preceding 30 years from 2019. Also, natural mortality, py, reduces a person’s expected lifetime economic output by another 7.3 percent. Finally, the total lost productivity must be discounted by 30 percent, because only around 10,630 of the original 15,393 OUD victims were working in the five years before they died. Our results place the present discounted value of total lost productivity for all opioid overdose victims using age at time of death between $9.6 and $10.9 billion.
Comparing Human Capital Losses with Value of Statistical Life
Economists have several tools available to quantify the loss of productivity in the labor market from a tragedy such as the opioid crisis. One such tool that economists have used in this literature and related literatures is the concept of the value of a statistical life. This approach shares similarities to that of the HC model in the current study, in that the goal is to quantify the magnitude of a loss, in our case due to opioid deaths, in dollar terms, which is typically done by relying on a set of assumptions. However, both types of calculations will provide different estimates, with value of statistical life estimates tending to yield larger numerical results.
The value of statistical life (VSL) approach is a different concept than methods that use earnings, like the HC model, which project forward adjusted earnings streams that are lost when someone dies prematurely. Instead, VSL estimates are determined by the hypothetical monetary amounts that a group of people would be willing to pay to avoid the risk of a death happening to an individual within their group. This is based on the fact that the group, when exposed to the risk of death, would not know which individual among them would die, so they would all pay a little bit to avoid a death altogether.
Thus, the VSL can help gauge the benefits and costs of not only various health policies, but also of the environment, transportation networks, and so on. There are two main ways of estimating a VSL value: revealed preferences, where researchers calculate a wage premium that someone implicitly accepts when taking on a higher paying but riskier occupation; and stated preferences, where research participants are asked how much they would pay to reduce the probability of a potential death by a small amount.
The Government of Canada recommends the value of statistical life to be around $7.9 million for Canadians, with a lower range of $4.3 million and an upper range of $11.6 million (Canada Treasury Board 2007; Chesnut and De Civita 2009). Multiplying the Canadian VSL values by the 15,393 overdose victims would lead to a low value of $65.7 billion, a central value of $122 billion, and a high value of $178.3 billion. An additional conclusion of the review of economic studies on the opioid crisis by Maclean et al. (2021), besides that labor markets played a role in and are affected by opioids, was that economic cost estimates of the crisis are high and vary widely. Table 3 supports this point by summarizing the previous results from the HC model with those of the values of statistical life.
Summary of Human Capital and Value of Statistical Life Estimates
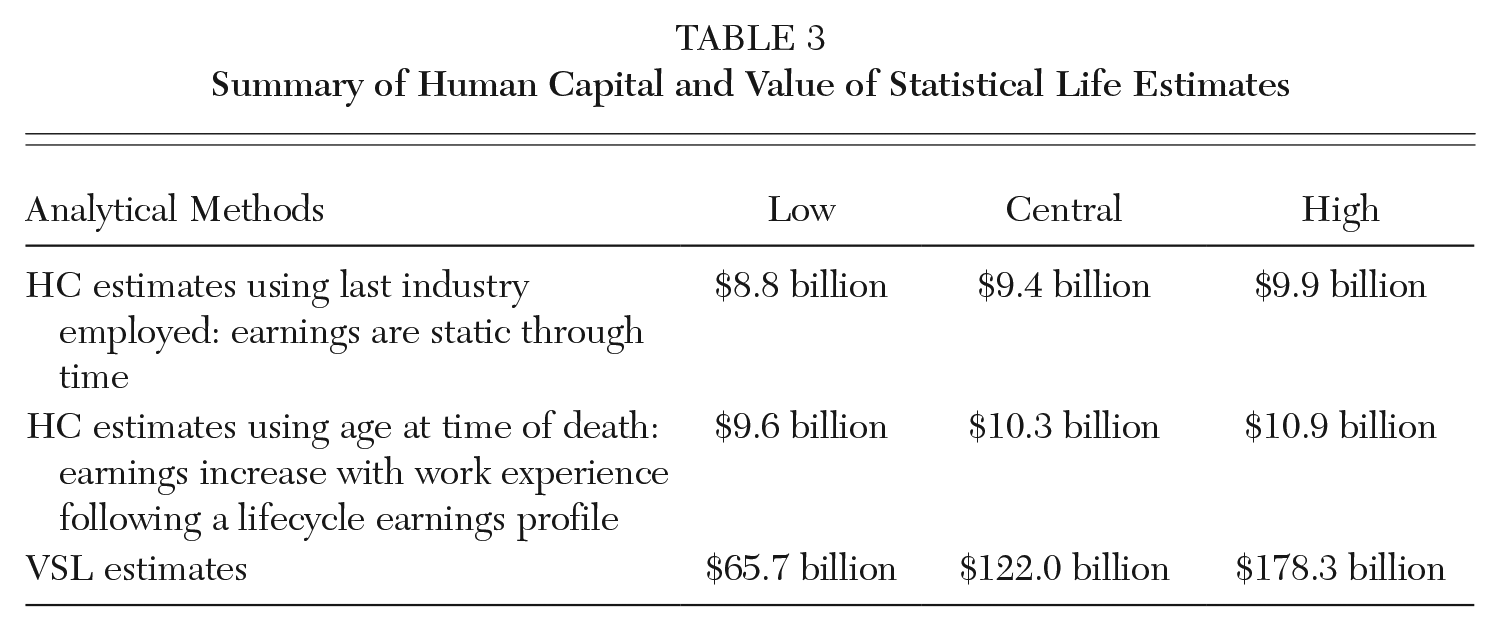
The net present value of lost labor productivity from the HC models ranged from a low of $8.8 billion to a high of $10.9 billion. The variant using average earnings by age group resulted in approximately 10 percent higher estimates than those performed with industry earnings estimates. The cause for this likely lies with how the second analysis accounted for the victims by earnings and age group; this would allow the model to capture losses through time, especially from younger victims. That said, estimates between the models remain within approximately 10 percent of the other, regardless of the calculation method. In contrast, the VSL estimates are much larger, ranging from $65.7 to $178.3 billion and, at the high range, are upwards of ten times the amount from the HC models. Therefore, our HC productivity losses can be considered on the low end of the range of these estimates.
To provide some additional context on the magnitude of this lost output for Canada, the entirety of the city of Montreal’s 2019 operating budget was $5.7 billion (City of Montreal, Department of Finance 2019). So, the high estimate from the HC model of $10.9 billion for opioid deaths across the country is only slightly less than Montreal’s 2018 and 2019 combined budgets. And this does not even account for productivity losses due to OUD absenteeism and reduced labor force participation. An American study that estimated productivity loss from absenteeism and reduced participation found that those losses were about 38 percent of the mortality loss (Davenport, Weaver, and Caverly 2019). We lack data to make similar estimates for Canada, but applying the percentage loss from the American study gives a crude estimate of an additional $3.3 to $4.1 billion in lost productivity to the Canadian economy.
For the U.S., a recent “meta-analysis of meta-analyses” regarding the value of a statistical life put the baseline estimate at close to 7.0 million U.S. dollars (USD) for an American, with a 90 percent confidence interval from 2.4 to 11.2 million USD (Banzhaf 2021). Using an exchange rate of 0.8 USD being roughly equivalent to 1 Canadian dollar (CAD), this would range from 3 million to 14 million CAD per life, which is slightly wider than the bounds of the Canadian per life VSL estimates.
Elsewhere in this volume, Bifulco and Shybulkina construct an aggregate loss estimate for the U.S. from opioid misuse based on local and state government expenditure needs. Their estimates range from around 53 to 59 million USD over the same four-year period as the current study from 2016 to 2019. Taking the population difference of Canada, at just over a tenth of that of the United States and equivalent to the population of the state of California, this sounds reasonable but relatively low when considering our estimates and the differences in opioid deaths.
Much like in Canada, the U.S. also witnessed a rise in opioid overdoses in 2020, with record deaths occurring throughout the COVID-19 pandemic (Manchikanti et al. 2021). It is unclear if this trend will persist or dissipate going into the future. Overdose deaths beyond 2020 were not included in this study primarily because using prepandemic estimates of victim industry breakdowns for 2020 and beyond could produce erroneous estimates. The industry and age breakdowns of opioid overdose victims used to estimate lost productivity may have significantly changed during and following the COVID-19 pandemic.
Future Steps for Mitigating the Opioid Crisis
The opioid crisis has severely affected both the U.S. and Canada and will likely continue to do so for many years to come. The COVID-19 pandemic has only exacerbated opioid-related harms and deaths. It has been predicted that up to 1.2 million people could lose their life to an opioid overdose in the U.S. by 2029 without substantial policy reform (Rao, Humphreys, and Brandean 2021). One challenge to creating a single unified approach to managing the opioid crisis is the diversity of the population suffering from OUDs. For example, certain rural areas, such as the Yukon in Canada or Appalachia in the U.S., were hit harder than urban areas. Furthermore, First Nations populations are five times more likely to overdose and three times more likely to die than non–First Nations populations (Belzak and Halverson 2018). Individuals living in poverty or with housing instability are also more vulnerable, as are those affected by mental health disorders.
When it comes to the labor market, construction is the hardest-hit industry in both the U.S. and Canada. In Canada, 30 percent of employed overdose victims were in the construction industry when they died. In the U.S. State of Massachusetts, a construction worker is over seven times more likely to overdose compared to all other workers (Hawkins et al. 2019; Dong, Brooks, and Brown 2020). The trades and transportation industries have also been hard hit by the opioid crisis, and there are several reasons why this may be the case:
• Construction workers and those employed in the trades are more likely to suffer workplace musculoskeletal injuries than other workers; and they are more likely to be prescribed opioid prescriptions, which can lead to OUDs.
• Physically demanding jobs, such as construction, often lack proper paid sick leave, which means OUD victims often use opioids to continue working.
• Male-dominated industries, such as construction, are less likely to talk about mental health or substance abuse problems due to stigma.
Solutions for reducing deaths include improving ergonomic solutions for construction workers; improving paid sick leave for trades, transportation, and construction industries (to allow workers to heal their workplace injuries properly); and supporting effective injury pain management.
Another challenge of the opioid crisis includes the supply of toxic street drugs in both Canada and the U.S., which has only become more toxic in recent years. The British Columbia Coroner’s Office and the 2022 Stanford-Lancet commission on the opioid crisis recommend providing easily accessible, low-barrier, pharmaceutical-grade opioid alternatives; and high-quality, fast drug testing services to reduce illicit drug deaths (Government of British Columbia 2022; Humphreys et al. 2022).
The legacy of the “war on drugs” still influences the public perception of drug users. For example, drug use is often perceived as deviant and shameful. In Canada, the decriminalization of illicit drugs for personal consumption is supported by the Canadian Association of Police Chiefs, numerous academics, and the government of British Columbia. In fact, on June 1, 2022, British Columbia was granted an exemption from the Controlled Drugs and Substances Act by Health Canada, decriminalizing the possession of small amounts of certain drugs from January 31, 2023, to 2026. The destigmatization of drug use is important, because stigmas on drug use create barriers for people to access potentially life-saving treatment. In the U.S., some OUD victims hide their drug use for fear of criminal repercussions (Humphreys et al. 2022).
Take-home naloxone kits (THNs) will also remain an essential component of combating the opioid crisis. Since June 2019, every province and territory in Canada has offered free, publicly available Naloxone kits, distributing over 590,000 THNs through over 8,700 sites across Canada. These THNs have reportedly reversed over 61,000 overdoses, highlighting their importance (Canadian Institutes of Health Research 2019). Recent research has found no evidence that THNs have been associated with increased opioid use or overdose, and concerns that THNs may lead to increased substance abuse were also not supported by the literature (Tse et al. 2022).
Conclusion
The U.S. and Canada have been and continue to be outliers in the opioid epidemic. These two countries consistently place first and second, respectively, as the countries with the highest rates of opioid-related overdose deaths, making North America the most affected continent. In Canada, the opioid crisis took 15,393 lives from 2016 to 2019, with 74 percent of victims being male and the average age at death being 42. Extrapolating from British Columbian data, approximately two-thirds of OUD victims in Canada were working in the five years before they died, and construction workers and those of middle-age were overrepresented in fatal overdoses: around 21 and 27 percent of OUD victims, respectively. Thus, the opioid crisis most affected working, middle-aged males in labor-intensive occupations.
We used two HC models to estimate lost productivity for Canada. The first model used industry estimates to generate victim earnings profiles: the analysis was linear, assuming each victim lost 22 working life years and static annual earnings. This model estimated lost productivity at $8.8 to $9.9 billion. The second analysis accounted for the nonlinearity of earnings with age (a lifecycle earning profile) and dropped industry earnings completely, relying on average earnings by age group instead. This second model yielded somewhat larger estimates between $9.6 and $10.9 billion. The high end of the HC estimate of $10.9 billion is similar to the city of Montreal’s combined 2018 and 2019 municipal operating budget, whereas the comparable value of statistical life estimates were much larger, between $65.7 and $178.3 billion.
These productivity loss estimates challenge the notion that the opioid crisis has only affected unproductive members of society. While this study relies on numerous statistics and models to calculate lost labor productivity to the Canadian economy, each of the 15,393 victims represented an individual person. No model or formula can, or ever will be able to fully quantify the devastating impact that the opioid crisis has had on families, communities, and society as a whole. Understanding the economic burden of the opioid crisis will allow policy-makers to better allocate the resources needed to mitigate the loss of life and manage the crisis. Further research into the opioid crisis will be needed to fully factor in the unprecedented social, economic, and cultural upheavals of the COVID-19 pandemic.
In terms of solutions, a country should try to minimize death in its populace as best it can, especially for preventable deaths like opioid overdoses. In general, the government response at the federal level should follow where the numbers are worse within the country. This would mean that Canada should target those provinces where the death rates are highest: British Columbia and Alberta, followed by Ontario and Saskatchewan. Given the fact that provinces in Canada oversee their own public health care, this can also be done by targeting resources within provinces as well, such as towards those working in the construction industry or toward middle-aged males. For the U.S., this top-down approach would mean targeting states such as West Virginia and Delaware, as well as the District of Columbia, although the lack of a public healthcare system will bring its own additional complications as compared with Canada.
The exact impact opioids may have had on labor markets remains unclear. While there are inherent similarities between U.S. and Canadian labor markets, generalizability should be approached with caution. Each country has different health and labor policies, and Canada’s social safety net provides more generous unemployment compensation. Research into the specific impact of opioids on Canadian labor markets has been limited, so it will remain an area of potential future research beyond this article.
Footnotes
Notes
Alexander Cheung is a master of economics student at the University of Alberta in Edmonton, Alberta, Canada. Prior to his graduate studies, he was an undergraduate student in economics and a recipient of a Roger S. Smith Undergraduate Researcher Award at the University of Alberta.
Joseph Marchand is a professor in the Department of Economics at the University of Alberta in Edmonton, Alberta, Canada. He is a labor economist who served as the chair of the Minimum Wage Expert Panel for the Government of Alberta and as an expert witness for the Senate of Canada.
Patricia Mark was an addictions medicine physician with the Vancouver Island Health Authority in British Columbia, Canada. She was a pioneer of methadone treatment on Central Vancouver Island in the 1990s and spent her career working with marginalized and unhoused populations. She passed away on April 8, 2021.