
Abstract
Regulation of long-term care service provision is a case of hybrid accountabilities. How do inspectors who are responsible for the implementation of regulations handle the uncertainties arising from hybrid accountabilities? While the prevailing scholarly consensus is that hybridity creates tensions that have a negative impact on the quality of regulation, this article shows that different accountabilities can reinforce each other. However, situations in which inspectors can develop a positive stance toward hybridity and integrate competing logics are rare. Hybrid professionalism among inspectors requires training, education, and resources as well as a joint regulatory culture with inspectees—preconditions that are hardly present in recent institutional settings of long-term care regulation.
Accountability in the regulatory welfare state is hybrid: providers are held accountable for different, sometimes conflicting, goals. As a result of the intentional mix of the logics of the market, hierarchy, and professionalism, service providers are, for instance, expected to deliver services of high quality, but only for a minimum price to keep public healthcare spending sustainable; service providers should also establish efficient structures and processes without, however, compromising standards regarding the quality of work and the participation of users.
This study analyzes the implementation of a hybrid regulatory framework from the inspectors’ perspective. The guiding research question is: How do inspectors, who are responsible for the implementation and enforcement of the regulatory framework, make sense of hybridity? In the literature, we find ample empirical evidence that hybridity creates tensions that are difficult for inspectors to handle. Inspectors—and professionals in general—might even reject the policy they are expected to implement because they cannot make sense of it, a reaction pattern that Tummers (2011) described as policy alienation. However, others are observing the evolution of hybrid professionalism with professionals who have attained new skills and are able to go beyond traditional professionalism by integrating and blending different logics (Noordegraaf 2015). Inspectors who are open to hybrid professionalism are, for instance, willing to learn managerial competences and improve their adaptation skills to navigate contradictions between performance schemes and professional standards.
The article provides an empirical case study of quality inspection in the German long-term care sector, which is a prime example of the regulatory welfare state. The idea of delivering public goods with market means was a guiding principle when the new social insurance for long-term care was introduced as a fifth pillar of the German welfare state in 1995. In subsequent years, the sector developed into a highly competitive field; although, in a parallel movement, we could also observe the rise of a regulatory welfare state (Levi-Faur 2014). A complex regulatory framework has been gradually set up to control clients’ access to the services, audit structures, processes, and outcomes of service delivery. So far, the scarce research on the regulation of the German long-term care market has focused mainly on regulatory strategy, or on the tools and instruments and their adjustments to an increasingly hybrid environment (Herr, Nguyen, and Schmitz 2016; Nies and Leichsenring 2018). Views from below, however, are missing: the process of implementing the regulatory framework has remained a black box.
The article proceeds as follows. Section two presents the theoretical background of this study, which draws on three bodies of literature: accountability, hybridity, and street-level bureaucracy. The bodies of literature are closely connected to the research on the regulatory (welfare) state. The rise of the regulatory (welfare) state has fueled an intense debate about accountability. While there were strong concerns about declining accountability in the early years of the regulatory welfare state, particularly with respect to public and democratic accountability, it is today widely accepted in the literature that accountability in regulation is not a question of more or less accountability but of multiple accountabilities and the relationships among them (Benish and Mattei 2019). This is where the literature on hybridity comes in, which acknowledges that accountability in regulation is multifaceted, fluid, and—as a rule—full of tensions. The literature on street-level bureaucracy, in turn, reminds us that inspectors need to implement and enforce accountability mechanisms. Their discretion and their (lack of) ability to cope with hybridity are crucial factors that have substantial impacts on regulatory performance.
In the third section of the article, more information about the institutional background of the German long-term care sector and recent reforms is provided. I then go on to explain the methods for data collection (policy documents, semi-structured expert interviews, and vignettes) and analysis (qualitative content analysis). Next, I present the empirical findings. The empirical analyses show that inspectors fall into different groups. While one group shows active resistance to hybridity, others are able to reconcile the hybrid regulatory framework with their identity as a professional. However, their coping strategy is rather passive: they let situations happen, without bothering about contradictions and dilemmas. The most important finding is that no cases of hybrid professionalism were found.
Based on these findings, the discussion section suggests a refined analytical framework: to understand how inspectors deal with hybridity, both the inspectors’ attitudes toward hybridity (accepting or rejecting) and their willingness or capacity to use a reflexive approach need to be taken into consideration. The findings also allow us to reflect on the preconditions for hybrid professionalism and to draw conclusions for the design of regulatory architecture. Lessons can be learned from this study, for both quality regulation in the German long-term care market and for accountability systems in the regulatory welfare state in general.
Theory: Hybridity, Accountability, and Street-Level Bureaucracy
From an institutional perspective, quasi-markets are hybrid arrangements. They deliver public goods—in our case, professional care services—with private means. Hybridity results from the intentional mixture of different logics: market, hierarchy, and professionalism. How to hold providers in the service market accountable for their actions is a central topic in the literature on regulatory welfare state governance (Benish 2014; Jann and Lægreid 2015). The accountability literature assumes that there is an elective affinity between different institutional logics and different accountability mechanisms: hierarchies, markets, and professional networks do not only have their own goals, values, and typical modes of interaction but also ideal typical mechanisms of accountability (Mashaw 2006). In hybrid governance arrangements, where the realms of the state, the market, and civil society collide, accountability relations, too, are hybrid. Providers of public services are held accountable through competition, professional norms, and the hierarchical interventions of regulatory agencies. Often there is not only one but several regulatory agencies to which service providers have to render account (Benish and Mattei 2019; Levi-Faur 2005), and often the accountability obligations of the different regulatory agencies are in conflict. It may even be possible for one regulatory agency to have accountability obligations that are themselves hybrid.
Accountability mechanisms need to be put into effect by some agent (Moore 2014). This is particularly true for laws and legal prescriptions that bear only the potential for accountability but do not put it into effect by themselves. The implementation and enforcement of regulatory policies are mainly the responsibilities of inspectors who are what Lipsky (2010) has called “street-level bureaucrats”—that is, actors who fulfill a public task and who are thereby in direct interaction with the target group. Inspectors shadow the people they are inspecting; let them explain how well daily operations are performed; check off boxes on inspection lists; and negotiate with inspected organizations before they decide whether they should hand out inspection tags, issue verbal warnings, or impose fines. Inspectors are thus the human face of regulatory policy (Van de Walle and Raaphorst 2019, 2).
Like every social interaction, the regulatory encounter is shaped by the postures and attitudes of those who interact. Braithwaite (1995) and Braithwaite and Cleland (2017) point to the relational dimension between inspectors and their inspectees, which is often overlooked in the regulatory literature but has a significant impact on both the actual use of enforcement styles and the effectiveness of the regulatory architecture. Among inspectees, we can find a group that is antagonistic toward regulation and expresses this, for example, by treating a regulatory authority as if it is irrelevant or by questioning the legitimacy of a regulator. Others might be willing to “play the regulatory game” and to comply but lack knowledge and/or capacity to do so. Both types of inspectee behavior (and the mixed types in between) can be differentiated for analytical purposes. However, it is even more important to differentiate them in policy practice because they require different treatment. Inspectors thus should be able to adapt their enforcement styles to the situation and look at cues to understand inspectee behavior.
Inspectors thus need the discretion to choose among different enforcement styles, to adapt laws to the circumstances of cases in a manner consistent with policy and hierarchical authority, and to cope with the uncertainties and pressures of their daily work (Van de Walle and Raaphorst 2019). Uncertainties may arise because information is ambiguous or even lacking, because evaluation standards could be interpreted in different ways, or because it is difficult to decide whether an inspected organization or an inspected individual is trustworthy.
However, in light of the ideas of New Public Management (NPM) in the late-twentieth century, discretion in regulation—and in street-level bureaucracy in general—was considered more and more critical. In the scientific but also in the political debate, an increased risk of regulatory capture has been perceived due to the increasing number of private for-profit and semi-autonomous providers as well as the increased choice options of customers (Benish, Halevy, and Spiro 2018; Cohen, Benish, and Shamriz-Ilouz 2016). As a result, political actors have introduced new guidelines and wide-ranging documentation requirements, often on top of already existing practices, to diminish the discretion of street-level bureaucrats. The inspector’s role is to ensure the compliance of service providers without, however, giving extensive advice. While hybrid accountability is nothing new in long-term care, the NPM reforms have considerably intensified hybridity through marketization, managerialization, and customer choice.
How do inspectors relate to hybrid accountabilities? When multiple competing logics are in play in the same setting, they can trigger conflict or generate new types of activity. In the literature on inspectors in the care sector, the prevailing interpretation of the NPM accountability reforms is critical: instead of improving the safety and quality of life of patients, NPM practices of routinization and standardization have intensified problems of gaming and ritualistic use of regulatory instruments (Braithwaite, Makkai, and Braithwaite 2007).
Similar empirical findings of professionals who cannot manage competing logics are also reported in other parts of public administration. Tummers (2011) refers to the notion of policy alienation when street-level bureaucrats are not able to make sense of hybridity and thus refuse the policies they are expected to implement. Policy alienation is often caused by feelings of powerlessness or meaninglessness. Street-level bureaucrats can feel powerless when they do not have any influence on the types, quantity, and quality of the policies they implement. Meaninglessness indicates that street-level bureaucrats have the impression that the policies they are expected to implement have no beneficial outcome for society.
However, in the literature on street-level bureaucrats, we also find more positive assumptions about their ability to cope with hybridity. Schott, Kleef, and Noordegraaf (2016, 8) stress the ability of street-level bureaucrats to master hybridity, for instance, by actively integrating and blending competing logics into a new logic. As a result, these street-level bureaucrats become hybridized professionals with new skills that allow them to link professional practices to organizational objectives, as well as to broader social and economic developments. In a similar vein, Benish (this volume) draws attention to situations in which different logics of accountability are perceived as compatible and thus lead to mutual reinforcement.
This article uses the two contrasting modes of coping with hybridity—hybrid professionalism and policy alienation—as a starting point to develop a two-dimensional framework that offers a differentiated understanding of handling hybridity. Thereby, attitudes and postures toward hybridity on one hand, and the degree of activity (or passivity) on the other hand, are considered as relevant to categorizing empirical findings.
Long-Term Care Regulation in Germany: Hybrid Accountability Arrangements
Long-term care services are provided in Germany in an institutional setting that combines competition among providers and choice for consumers with public funding and public regulation. The Long-Term Care Insurance Act of 1995 not only aimed to provide care for patients for a reasonable price but also to foster innovation in the field through competition. Private for-profit providers were thus explicitly given the same status and the same rights as public and voluntary providers to facilitate their access to the market. Today, the market for ambulatory care is even dominated by private for-profit providers: in 2017, 65.8 percent of the providers had a private for-profit legal form, 32.8 percent were voluntary providers, and only a negligible number of providers (1.4 percent) had a public legal form. Voluntary providers still outweigh the share of private for-profit providers in the market for statutory care, but the share of the latter is on the rise (all numbers are taken from Statistisches Bundesamt [Destatis] 2018).
Parallel to the creation of the new care market, an encompassing and, over the years, even growing regulatory framework has been set up to hold the competing service providers accountable to public values. The regulatory framework was not developed from scratch; rather, it has grown stepwise in a path-dependent way by layering new regulatory mechanisms on top of already existing ones.
The SHI Medical Review Board, which is one of three regulatory agencies, conducts the bulk of the quality inspections. The agency, which is jointly run by the statutory health insurance firms, is thus considered the main regulatory agency. Its regulatory mission is hybrid: the quality care inspections have at least four different objectives that serve different stakeholders (Herr, Nguyen, and Schmitz 2016):
• First, quality inspections aim to improve the transparency of the care market. In particular, they should enable people in need of care to make informed choices among care providers. Collecting and disseminating information is thus one major objective of quality inspections;
• Second, inspections should help to reduce malpractice and fraud among service providers (policing). The preventive and detective functions of quality inspections are of particular importance for funding agencies;
• Third, inspections should help managers and the professional staff of service providers to improve the quality of their services (organizational and individual learning objectives); and
• Finally, quality inspections should contribute to the development of policy recommendations based on the inspection results (policy learning).
The SHI Medical Review Board is thus simultaneously an advisory, control, educative, and policy board. It has vulnerable clients, profit-seeking entrepreneurs, care-providing professionals, bureaucrats, and politicians as stakeholders. From the perspective of the single inspector, this hybrid organizational environment creates dilemmas and paradoxical injunctions. Its missions are not only directed toward different stakeholders but are partly conflicting and require different implementation styles. The preventive and detective functions of quality inspections call for a strict top-down implementation style, whereby compliance is enforced with sanctions. Individual, organizational, and policy learning functions, on the contrary, succeed best in an organizational culture that embraces the lessons that can be learned from failure and that encourages an open discussion about mistakes without immediately blaming the responsible actors. The market transparency expected by citizens, too, might have detrimental effects for individual and organizational learning because it is based on the assumption that compliance is best achieved through public naming and shaming.
The main instruments of the regulatory strategy in force at the time of writing are mandatory quality management for all providers and unannounced inspections. During their inspections, inspectors check the quality according to a standardized list of criteria and pay visits to randomly selected nursing home residents. A particular focus is put on the plausibility of care documentation. The inspector cannot sanction noncompliant providers directly but has to inform the Local Residential Homes Authorities (Heimaufsicht), which have the final say about sanctions. To create transparency, the inspection results are published online. From 2009 to 2016, the school grade–based system 1 was used to rate providers according to the results of the inspection. It was, however, withdrawn after a critical public debate. Patient representatives and critical care professionals’ associations blamed the system for not being neutral. Indeed, the neutrality of the quality inspections was questioned because the care transparency agreement (CTA) was jointly negotiated by representatives of the funding agencies and service providers, while representatives of patient organizations or nursing associations were not involved at all in the development of quality standards.
In light of the ongoing critical public debate, the regulatory strategy for long-term care quality inspection has been subject to reform initiatives (Wollmann and Bönker 2018). A new regulatory strategy has just become effective during the writing of this article. Instead of putting emphasis on formal compliance (measured by taking the quality of care documentation as a proxy), the new regulatory approach aims to strengthen consultative elements, for instance, thereby providing more room for expert discussions and interviews with care professionals, managers, and residents during the inspection visits (Wingenfeld et al. 2018). We come back to the new regulatory framework and assess the reforms in light of the empirical findings of this study.
Methods
This is a qualitative study. First, we collected data through an analysis of policy documents, such as reports from expert commissions (e.g., Wingenfeld et al. 2018) and policy statements from different stakeholder groups (e.g., consumer organizations, the umbrella organizations of the health insurance funds, and service providers). Second, we checked the annual reports of the SHI Medical Review Board to assess the administrative capacity of the regulatory agency. The data collected include the number of employees, staff qualifications, training opportunities, and organizational structures.
The main data source, however, was expert interviews with inspectors. We conducted twenty interviews in total, each lasting an average of 60 minutes. As already described, regulating long-term care in Germany is a controversial field, and the regulatory strategy is subject to ongoing reform debates. Because of this, recruiting interviewees was challenging. Potential interview partners could be identified quite easily through the homepage of the SHI Medical Review Board, but there was an atmosphere of fear and distrust that made it difficult to convince inspectors to participate in our research. However, we continued to collect expert interviews until we had saturation, meaning that no new codes occurred in the data but mounting instances of the same codes occurred.
For the interviews, we combined a semi-structured questionnaire with the vignette technique. Whereas the semi-structured questionnaire allowed new ideas to be brought up during the interview while keeping the focus on the topics at hand, the vignette technique helped to explore sensitive topics (e.g., coping strategies for challenging situations such as difficult-to-handle managers of nursing homes). We collected the scenarios for the vignettes through preparatory discussions with scholars, nurses, and service provider managers. After reacting to the vignettes, we asked the inspectors to describe their daily work, how they perceived their role in the long-term care system, and whether the instruments they had on hand were appropriate for their work objectives. We also invited them to report challenging situations during quality inspections and their ways of dealing with such situations. Finally, we asked them to assess the impact the increasing marketization of the long-term care system has had on their work.
We analyzed data along the lines of qualitative content analysis. We developed themes and codes in an iterative process, going back and forth among interview data, secondary empirical material, and the relevant literature. To categorize findings, we used hybrid professionalism and policy alienation—two reactions of street-level bureaucrats toward NPM reform policies previously described in the literature (Noordegraaf 2015; Tummers 2011)—as starting points. In light of the empirical findings, we again refined the framework.
Findings
Hybrid accountabilities and role perception
The interviewed inspectors were sensitive to the complex accountability relations in which their work is embedded. When asked to describe their daily work, they reported that they felt obliged to manage diverse expectations generated within and outside the organization: When we conduct our work, we are in touch with very different actors: patients, providers, insurances, and also our peers, the professional staff in the nursing homes. And each of these actors wants us to do different things. For insurance firms, ensuring quality means having an eye on financial sustainability; they want us to detect overuse and misuse. Providers want to get the most out of the system, and they push us to approve higher levels of care. The same goes for patients. (Interview 5)
However, inspectors were also aware that they did not have a neutral position in this hybrid setting. When asked about their role, they indicated without hesitation: “We are service providers, and the health insurance firms are our main customers” (Interview 8). Indeed, the institutional framework of quality inspection in Germany encourages inspectors to take sides and adopt a partial perspective. While the regulatory mission of the SHI Medical Review Board, according to law, is fourfold and combines creating transparency, inspection and policing, consultancy for providers, and policy recommendations, inspectors maintain that inspection and policing with a focus on financial issues outweigh other regulatory goals.
Attitudes toward (limited) discretion
From the inspectors’ descriptions of their daily work, it becomes clear how the SHI Medical Review Board as an organization addresses the challenge of hybrid accountability relations: through strict rules and procedures that should help inspectors to cope with administrative ambiguity. Inspectors are expected to implement a predefined work program; they have only limited opportunities to develop their own daily routines. Every evening, they receive a list of where to appear the next day for an unannounced inspection; the quality assessment, too, follows a strictly defined procedure. The inspectors’ daily work thus more closely resembles that of bureaucrats than professionals who have leeway to make decisions about the organization of their work. In addition, the regulatory framework has become increasingly dense over the years as a result of regulatory adjustments after scandals. While all interviewees agreed on the result, shrinking room for discretion, their opinions of this development varied. Some of the inspectors explained that they found the detailed form helpful and supportive for navigating difficult situations (Interview 5; Interview 3), such as critical debates with annoyed representatives of the inspected organization: “The detailed regulatory framework helps me to explain my assessment to upset patients or nursing home managers. I can say to them: ‘Look, it is not me; it is the law that prescribes doing this or that. I just follow the regulatory guidelines.’” Inspectors, however, referred not only to blame shifting to the regulatory guidelines, but also considered the implementation of these guidelines as their very mission: “When I manage to stick strictly to the official guidelines, then I am truly professional” (Interview 11).
However, some inspectors were more critical about the inspection instruments. They felt restricted in their professional judgment: “I see a lot of deficiencies in nursing homes, which I cannot document just because there are no relevant entry fields in my form!” (Interview 3). Inspectors recognized conflicts between the values and principles of professional care and the regulatory guidelines: “For instance, violence in nursing homes cannot be documented. If I have a reasonable suspicion, I have to depart from the official assessment form and ask in a more hidden way whether patients have experienced inappropriate behavior from nursing staff.”
Enforcement styles
When asked to describe their enforcement style, it became clear that inspectors viewed their own styles as different from that of the SHI Medical Review Board’s hybrid regulatory mission. While some state clearly, “My role is to control. I have worked in the past as a nurse; I definitely know that control is necessary for this field” (Interview 8), others described their enforcement style as advisory, deliberative, and accommodative: “The inspected staff has a huge knowledge and experience of giving care. During my inspections, I try to discuss at eye-level with the inspected organizations and try to find compromises between my expertise and their expertise” (Interview 12).
Inspectors favoring an advisory enforcement style, however, complained that practicing in that way was hampered by their working conditions. Stress from the high workload was indeed a recurring issue in the interviews. Due to the increasing number of people in need of care and the growing number of service providers, as well as the increasing density of the regulatory framework, the daily inspection workload has risen greatly and steadily in recent years. However, it is difficult for the regulatory agency to find well-trained staff, and workforce shortage has become a severe problem. Because of the workload compression, inspectors are concerned that the working conditions do not allow them to conduct the inspections according to their professional standards. The continual time pressure hinders them from handling quality checks with the necessary thoroughness. “The regulatory guidelines have become more and more complex in recent years. New standards were introduced that entailed considerable paperwork—we put more and more effort into the inspection visit without, however, receiving more time per visit!” (Interview 12).
Relational postures in welfare markets
When asked about challenging situations in their daily work, inspectors often referred to the emotional dimension in the inspector-inspectee relationship, which is quite complex. Several of them stated that they were usually confronted with a hostile atmosphere that prevented them from acting as benevolent and supportive consultants: “Staff and managers don’t believe that we are here to support them doing their job in a better way; they only see us as an additional administrative burden and don’t see the visit as an opportunity to learn” (Interview 15). It is not only the fact of being assessed and controlled that induces inspected organizations to adopt a critical and sometimes even hostile stance toward the inspectors. The SHI Medical Review Board suffers from a bad organizational reputation: “The Medical Review Board has such a poor standing in the community, but also in the general public debate. It is tough to work against this poor image” (Interview 8); “People pass the buck to the SHI Medical Review Board—we are accused of everything negative in the long-term care system” (Interview 4).
Inspectors also reported that they were accused of having abandoned their former colleagues. “Why are you no longer a nurse? We need you here; we are urgently searching for qualified staff. Why have you escaped to the SHI Medical Review Board?” (Interview 15). The underlying accusation is that the inspectors decided to quit stressful and tiring care work to do a “lazy and unpretentious bureaucratic job.” Despite their professional backgrounds, inspectors are no longer considered “one of them”: “They ignore the fact that I was once a nurse, that I was their colleague. I’m an outsider now—even worse, they consider me the bad guy” (Interview 6).
Sometimes it is also the nursing home management that labels inspectors as the “bad guys.” Inspectors reported experiences in which nurses had confided that their management uses the results of the quality inspections to put additional pressure on their staff to intimidate them and to expect them to do more with fewer resources (Interview 8). Inspectors explained that this type of situation made them feel that they were being instrumentalized—and, at the same time, it made them feel helpless because they did not know how to react.
Another inspector referred explicitly to the management of private for-profit providers that creates challenging conditions: I can see a clear difference in the behavior of private for-profit and voluntary providers. Private for-profit providers are new actors in the field and are aware that their legitimacy is still contested. They thus take the issue of service quality very seriously. Their internal quality management schemes are considerably better developed than those of the long-established voluntary providers. Taking quality seriously, however, also implies that the managers of the private providers watch me closely when I conduct my quality control. They know the guidelines by heart and are better prepared than their colleagues from the voluntary providers. They are often accompanied by lawyers who monitor my work constantly. (Interview 8)
From their daily work experiences, inspectors can see how much the provider landscape has changed in recent years as a result of privatization and marketization. Interestingly, none of the interviewed inspectors referred in a positive way to market-based governance. Instead, they had a rather critical stance toward the recent governance structures of the field, and this critical perspective influenced their inspection styles: “The field is underfunded. If I impose sanctions, I punish the staff—but they are not responsible for the misery” (Interview 14). Inspectors are of the opinion that they cannot hold the staff accountable for quality deficits. Even if they become aware of serious quality deficits in the nursing homes they inspect, they hesitate to impose sanctions: “The nurses do their best—quality problems in nursing homes are produced at the political level, not at the organizational level of the nursing homes or even by individual nurses” (Interview 8). The inspectors’ own role in the quality inspection game is considered as rather weak: “We don’t have the power to change the structures of the field” (Interview 3); “We cannot impose sanctions, we can only report to other agencies that decide about sanctions” (Interview 12).
Discussion
The literature suggests that an increasingly hybrid working environment allows street-level bureaucrats to become professionals who have acquired new abilities and skills. In particular, they have internalized managerial thinking that helps them to link professional practices to organizational objectives (Schott, van Kleef, and Noordegraaf 2016, 8). How do our empirical findings relate to this literature?
First, we conclude that inspectors are indeed conscious of the different logics that structure the field of long-term care and are aware of the challenges and conflicts that institutional hybridity causes. They report that they are often confronted with the incompatible demands of their different stakeholders, such as the wish of patients in nursing homes for staff to have time for them and to listen to them versus the expectation of the employer for staff to stick strictly to the schedule. Repeatedly, they see their own professional identity in conflict with external demands, such as when they miss the chance to document the misbehavior of staff or management, or when they lack the opportunity to substantially discuss the results of the visit with those being inspected.
Second, the empirical material reveals that inspectors make sense of hybridity in different ways. Some find it difficult to handle the various logics and thus complain or even reject hybridity, while others are conscious of the competing logics but accept hybridity as a given fact. However, their coping strategy cannot be classified as an active integration or the blending of the different logics into a new one. The inspectors in our sample did not consider themselves the forerunners of renewed professionalism. They did not describe themselves as market regulators controlling a competitive field while at the same time being able to respect professional values. Instead of actively integrating the different logics and combining them, the coping strategy they described is more passive and can be called pragmatic tolerance. Inspectors had value conflicts, but they did not have a clear concept of how to navigate the conflicts. Instead, they let situations happen and relied on formal arrangements to manage them.
While we did not find cases of hybrid professionalism, cases of policy alienation did occur. Inspectors were particularly critical of the increasing marketization of the long-term care field and thus rejected the recent hybrid mode of governance. Inspectors experienced meaninglessness when they wondered whether their interventions made any difference at all. Feelings of powerlessness surfaced when they described the inadequate available instruments they had for sanctioning noncompliant providers. They bowed out because they realized that they could not handle the different expectations of providers. Not all of the inspectors who had a critical stance toward hybrid accountability reacted with inner resignation. Instead, some solved inherent value conflicts by clearly prioritizing one logic. Interestingly, we find both the prioritization of hierarchy (“My main task is to control”) as well as the prioritization of professionalism (“I understand inspection as the reflection of professional standards, together with staff and management”).
As a single case study, the empirical material is too limited to provide explanations for the inspectors’ behavior and to make generalizations. However, the findings allow for the refinement of the analytical framework for how street-level bureaucrats experience hybridity. The findings suggest that two dimensions are relevant for classifying the inspectors’ coping strategies. The first is their attitude toward hybridity: do they accept or reject hybridity? The second is the degree of activity and reflexivity in their reaction patterns: are their attempts to deal with hybridity more active and reflexive (either by trying to integrate competing logics or by prioritizing one logic) or more passive (either tolerance or alienation)? Table 1 represents this classification scheme.
Classifying Coping Strategies for Hybrid Accountabilities
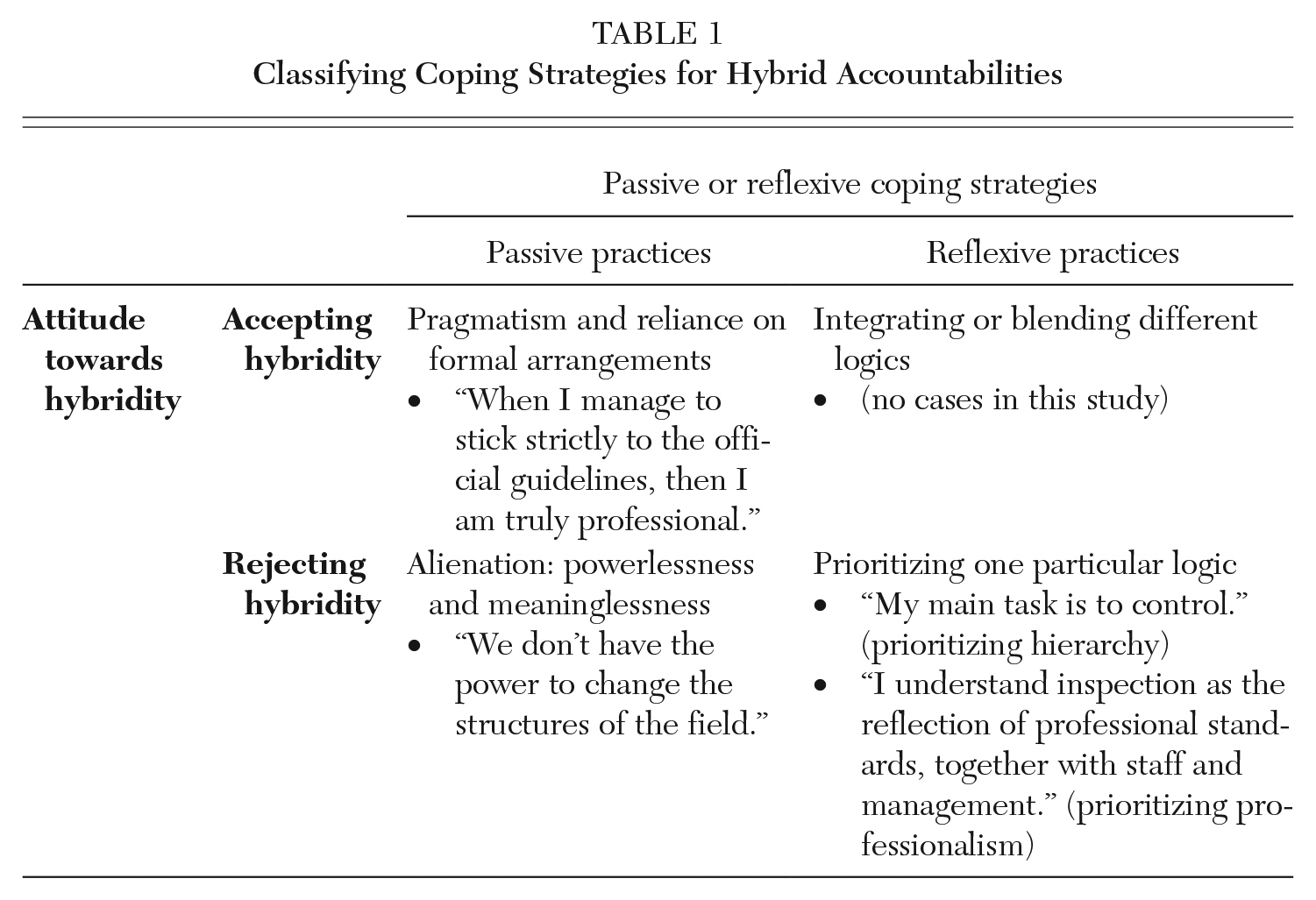
When looking at Table 1, it is indeed striking that no cases of reflexive integration of different logics appeared in the analyzed sample. It is interesting to relate this observation to the literature. Noordegraaf (2015, 11) has argued that when the complexity of the work rises, professionalism increasingly becomes organizing work: “Organizing becomes crucial for ‘professional’ professional action—organizing becomes an intricate part of professional work.” Traditional professional and new managerial, hierarchical steering practices are integrated in a reflexive way. However, Noordegraaf (2015, 14) acknowledges that such organization of professional processes cannot suddenly occur within organizational settings. Leveraging the adaptation of inspection processes in a hybrid working environment requires training and education as well as resources (staff, time, financial opportunities, and new technologies). However, in the case of long-term care quality inspection in Germany, the hybridization of accountability relations has occurred alongside a deterioration in the inspectors’ working conditions. Inspectors are expected to handle an increasingly complex regulatory framework and a rising number of cases without a complementary improvement in working resources (time, staff, etc.). Thus, inspectors experience hybridization as more demanding—and it is difficult for them to judge whether the hybridization per se or the workload is to blame.
The literature on relational postures in regulatory encounters (Braithwaite 1995; Braithwaite and Cleland 2017) points to the complex inspector-inspectee relationship as another factor that might explain why the inspectors in this case study were not able to integrate different accountability logics in a meaningful way. Effective regulation requires that inspectees be willing to accept the “regulatory game.” However, in welfare markets with fierce competition among providers, it is more likely that we find nursing home managers who are not only eager to maximize their profit margins at the expense of regulatory compliance but are also in principle antagonistic toward regulation. Indeed, the inspectors who we interviewed stated frequently that they felt challenged or even blocked and powerless because their counterparts considered the regulatory authority as irrelevant or questioned their legitimacy as a regulator. Interestingly, resistance seems to come more often from voluntary providers who fear losing their market position than from for-profit providers who still seek to stabilize their organizational legitimacy in the social service market, but this assumption needs to be examined more closely in future research.
Conclusion
Taking the results of this study into consideration, the most recent reforms of the regulatory framework of long-term care in Germany have to be viewed critically. As we described, a new hybrid regulatory approach that emphasizes the importance of organizational learning in the regulatory encounter became effective in fall 2019 (Wingenfeld et al. 2018). While the overall objective of the reform—to encourage learning instead of assessing the quality of documentation—is to be appreciated, it is doubtful that the reforms will increase the effectiveness of the system. The new regulatory strategy requires a trust-based and collaborative relationship between inspectors and inspectees and needs to be accompanied by appropriate resource allocation. An appropriate adjustment of resources, however, was not part of the reform process, nor was the reform of the regulatory strategy accompanied by reforms of the overall governance of the field. Without adjusting the working conditions of the inspectors (e.g., time and workload) and without decreasing the fierce competition in the field, inspectors will not be able to integrate the different logics of the new strategy and carry out the learning approach in a convincing way.
Going beyond the case of Germany, the observations of this study are also relevant for a general reflection about accountability in the regulatory welfare state. Gaps in implementation have been identified, the underlying reasons have been investigated, and possible reasons for regulatory failure can therefore be better understood. Regulatory failure does not occur because accountabilities in recent settings of the regulatory welfare state have become hybrid (accountability in the welfare state has always been hybrid), but because the preconditions for hybrid professionalism are poorly understood.
The results of the study can inform both research and policy practice, leading to the design of more effective accountability relations. In light of the empirical finding that dissatisfaction with working conditions was a recurring issue, we consider the working conditions of quality care inspectors to be a crucial issue for future research. Decent work seems to be a necessary, although very likely not sufficient, condition for enabling inspectors to integrate competing logics in a meaningful way. The empirical results also indicate that welfare markets with fierce competition result in relational postures in the inspector-inspectee relationship that hamper the establishment of a joint regulatory culture.
To be clear, these insights have been stated before in the literature on regulation, but they need to be discussed again for two reasons: they are still ignored in policy practice, and they have become even more pressing in a period in which austerity policies are combined with marketized and managerialized welfare state governance.
Footnotes
Notes
Tanja Klenk is a professor of public administration and public policy at the Helmut-Schmidt-University Hamburg. Her research interests include institutional and organizational change in public and social policy. Recently, she has been working on the marketization and managerialization of welfare state governance, as well as accountability, quality, and performance management.