
Abstract
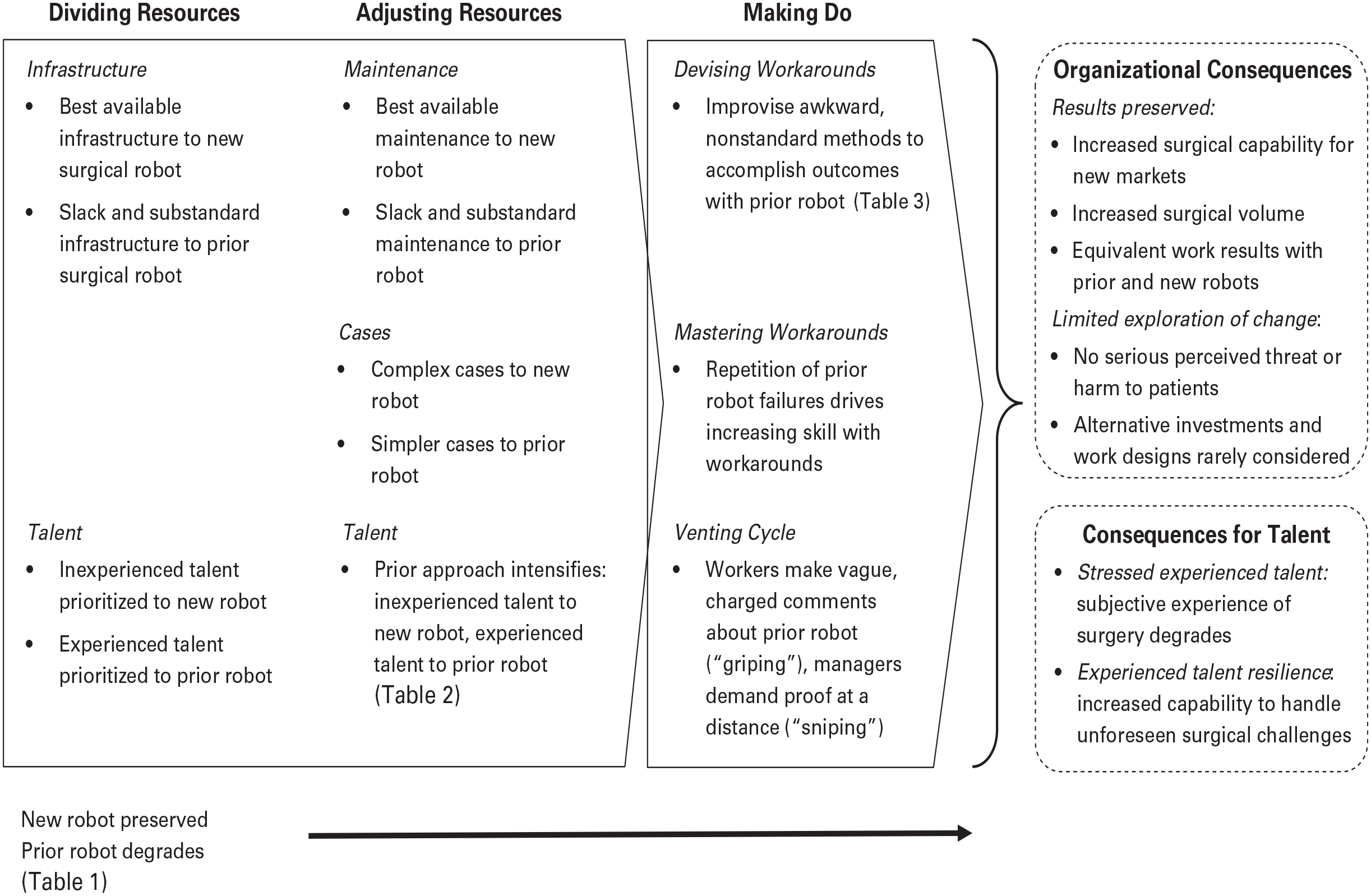
Here I theorize about a common challenge that research on technology and organizing has not yet considered: how organizations preserve results given the challenges of managing increasingly heterogeneous technological portfolios. I do so via a study of how a top-tier hospital allocated scarce resources across two surgical robots. After acquiring its second robot, the hospital divided resources between the older and newer robots to build its surgical capacity: it allocated the best available infrastructure to the new robot, and it prioritized assigning inexperienced talent to the new technology to facilitate use and skill development. The hospital then adjusted its resources to build on initial successes, committing both the best available maintenance and more-complex surgical cases to the newer robot. These dynamics inadvertently degraded the older robot, making it increasingly difficult to use. In response, more-experienced surgeons and staff made do with the degrading system: they developed and mastered workarounds, and they developed a venting cycle with management. Their actions reduced concerns about the older technology and stabilized the situation for the hospital, such that for years this portfolio resourcing process facilitated satisfactory outcomes on organizational goals such as growth, new capability, and patient care. But by shunting scarce resources away from the older technology, this process also stressed the experienced talent (even as it built their resilience) and limited exploration of changes that could benefit the hospital.
Organizations are torn between new and familiar technologies. New technology arrives regularly, driven by factors such as increasing cost efficiency (Barley, 2015), open innovation methods that involve millions of minds (Lifshitz-Assaf, 2018), standards allowing different vendors’ technologies to interoperate smoothly (Bailey, Leonardi, and Chong, 2010), and modular designs that allow rapid, lower cost prototyping and repair (Baldwin and Clark, 2000). Organizations must acquire new technologies to survive and grow, and the challenges of adapting to them have been a fixture in research on technology and organizing for 70 years (Trist and Bamforth, 1951; Gouldner, 1954; Morison, 1966). When this adaptation succeeds, it produces more familiar processes and tools that organizations will retain and invest in for some time, because the technologies reliably deliver improved results and competitive advantage (Morison, 1966; Tripsas, 1997; Bailey and Leonardi, 2015). Yet, the velocity and diversity of technical development means that new technology does not neatly arrive just as organizations are ready to decommission prior technologies. So, organizations and workers rely on a dynamic portfolio of technologies that includes the new and the old, the unfamiliar and the familiar.
Technological portfolios present a significant challenge because organizations must support them with limited resources (Bower, 1972; Barney, 1991; Eisenhardt and Martin, 2000). Putting a technology to use in an organization requires resources such as capital (Christensen and Bower, 1996; Danneels, 2007) and talent (Sull, 1999; Gilbert, 2006). Such resources must support a wide range of technological implementations, and no organization has these resources in unlimited, immediate supply. Thus, allocating resources to support the implementation of a new technology often means diverting resources from other technologies in the organization. Most technology also requires an ongoing commitment of resources such as maintenance (e.g., Orr, 1996; Vinsel and Russell, 2020) to remain effective, so this resource allocation problem often persists long after the memory of initial investments fades. Finally, informed resource allocation is challenging because firms find it difficult to secure up-to-date, comparable data on their full portfolio of technological efforts (Klingebiel and Rammer, 2014; Eckert and Hüsig, 2021). Allocating resources across a technological portfolio is therefore likely to be a perennial problem marked by significant inefficiency.
This technological portfolio problem is likely more pervasive and significant than we know. First, the challenge does not just involve allocating resources between qualitatively different technologies, such as heavy equipment and artificial intelligence. Organizations also have strong incentives to use multiple versions of any given technology: newer versions (e.g., Windows 11 vs. Windows 10) promise better functionality and performance via only slightly modified means (Barki and Pinsonneault, 2005; Berente et al., 2016; Kellogg et al., 2021), yet older versions are familiar and often still useful (Sull, 1999; Benner and Tushman, 2002; Danneels, 2007). The organization must divide its limited resources to put multiple generations of a technology to work. Second, these resource allocation decisions involve risk. Quantitative studies in technological R&D (Klingebiel and Rammer, 2014) and internal IT projects (Weill and Broadbent, 1998) show that only a minority of firms get good returns on their technological portfolios. And data from qualitative studies indicate that dealing with multiple versions of a technology may risk outcomes such as harmful work practices (Barley, 1990; Tucker et al., 2020) and costly differences in organizational routines (Goh, Gao, and Agarwal, 2011). Yet, portfolio-related catastrophes are not evident in prior research, suggesting that powerful, unidentified mechanisms may preserve outcomes despite these challenges.
Prior research on technology and organizing does not provide much insight into how organizations manage this technological portfolio problem. Instead, the literature has focused on the challenges that flow from shifting to new technologies such as computer-aided design (Bailey, Leonardi, and Barley, 2012), databases (Nelson and Irwin, 2014), and robots (Beane and Orlikowski, 2015). These studies are centered on how we make sense of new technologies (Weick, 1990) and rapidly integrate them into standing organizational processes (Tyre and Orlikowski, 1994). Another stream in this literature has focused on how organizations and particular technologies reconfigure each other through small-scale, local action (Barley, 1986; Orlikowski, 1996). This process of adaptation occurs as workers make the technology workable in emergent conditions (Leonardi, 2011). Both streams of work have assumed that after a discontinuous technological change, choppy organizational waters will again become smooth as the adaptation process becomes more incremental. But we have no direct knowledge of how organizations accomplish this transition given the challenges associated with managing a technological portfolio. Thus, I ask, how do organizations preserve outcomes as their technological portfolio becomes more heterogeneous, and with what consequences?
I explore these questions through a two-year field study of robotic surgery at Fairtown, a top-tier teaching hospital. 1 It acquired an upgraded robotic surgical system to address a range of strategic objectives, and its medical staff had to contend with both the newer and older models. Although Fairtown divided key resources (Barney, 1991; Noda and Bower, 1996; Eisenhardt and Martin, 2000) between these two systems in ways that appeared sensible at the time, these resource allocations slowly degraded the older robot, and experienced talent was increasingly and disproportionately allocated to work with it. To adjust to the increasingly unreliable robot, these workers developed workarounds (Gasser, 1986; Tucker, Heisler, and Janisse, 2014), the skill to enact these workarounds fluidly, and a venting cycle with management. Their efforts preserved surgical outcomes and limited actors’ assessments of the threat posed by the hospital’s technology portfolio, thus stabilizing the situation. But this portfolio resourcing process also compromised the work experience of these top surgeons and staff members (despite increasing their resilience), and it limited strategic exploration for the hospital. The findings I present here increase our understanding of how allocating limited resources across a technological portfolio can change organizational capability.
The Problem of Organizing Around a Technological Portfolio
It is common and very challenging for organizations to manage portfolios of technologies (Piening, Salge, and Schäfer, 2016; Brasil and Eggers, 2019; Miller and Toh, 2022). To survive, organizations must acquire many types of technology (Barley and Beane, 2021; Beane and Leonardi, 2022). Even the list of mundane technologies is long, including computation (Brynjolfsson, Hitt, and Yang, 2002), sensors and instrumentation (Bechky, 2020), software (Bailey, Leonardi, and Chong, 2010), and buildings (Gonsalves, 2023). Putting each technology into service requires a portion of the organization’s available resources, including tangible (e.g., space, electricity), human (e.g., talent), financial, and other resources (Noda and Bower, 1996; Eckert and Hüsig, 2021). Research on technological portfolios has shown that the volume and diversity of resources required to deploy technologies often dwarf those required for acquiring them (Weill and Broadbent, 1998; Klingebiel and Rammer, 2014).
The challenges of managing a technological portfolio do not end with deployment. Keeping each technology running takes additional resources, such as preventative maintenance and repair (Orr, 1996; Henke, 1999), and even if an organization could ensure equal and perfect maintenance across the entire stock of its deployed technologies (Jacobs and Cairns, 2011), doing so is often not cost effective. Further, organizations do not always have the luxury of retiring older technologies every time something new and more useful arrives; they must keep older technologies in value-adding service long enough to show they have earned a satisfactory return, even as they acquire new ones (Gordon and Shapiro, 1956). Finally, organizations struggle to manage their technological portfolios because securing high-quality information about the status of a firm’s full range of technological efforts is often practically impossible (Klingebiel and Rammer, 2014; Eckert and Hüsig, 2021).
Organizations likely seek to minimize the disruption that comes from introducing wholly new technologies into their portfolios by acquiring incrementally improved versions of prior technologies (Barki and Pinsonneault, 2005; Berente et al., 2016; Kellogg et al., 2021). Fewer training resources are required for these ostensibly familiar tools, and integrating them into existing processes is less costly because inputs and outputs will differ less than if the technology were wholly new (Sull, 1999; Benner and Tushman, 2002; Danneels, 2007). But even new versions require resources from the same limited pool available for more-discontinuous technological change, and in some cases organizations may prioritize resources for novel technologies, for signaling purposes (Beane, 2020). Together, these challenges likely place significant, often simultaneous, and imperfectly understood demands on an organization’s scarce resources, and these demands are unlikely to be fully apparent or easily managed.
Research on technology and organizing does not show how organizations meet this portfolio challenge, as studies have alternatively considered the disruptions and adaptation that come with a single technology. Yet, findings in these streams of work are relevant to questions surrounding technological portfolios. The stream focused on disruption (Trist and Bamforth, 1951; Barley, 1986; Edmondson, Bohmer, and Pisano, 2001) has shown that a great deal of costly and uncertain experimentation occurs just after an organization acquires a new technology, that most alternatives are discarded, and that usage patterns often quickly settle down or the technology is rejected (Orlikowski and Gash, 1994; Tyre and Orlikowski, 1994; Leonardi, 2009). For instance, Kellogg’s (2021) study of the introduction of a clinical decision support system in a hospital showed how managers addressed this disruption through an approach characterized by experimentalist governance. Likewise, Tyre and Orlikowski’s (1994: 98) research found early “windows of opportunity” for technological change, and that production pressures, usage habits, decreased expectations, and the erosion of team membership then impeded adaptation. Yet, these and comparable studies have examined a single system and set of practices replacing another; they did not consider the implications of these dynamics for the ongoing acquisition and use of multiple versions of such a system, let alone other technologies in the organization.
The other relevant stream in the technology and organizing literature has focused on the incremental adaptation that comes after the initial shocks associated with a new technology’s introduction have faded through recurrent use (Orlikowski, 1996; Graham and Thrift, 2007; Anthony, 2021). Far from showing an optimal resting place for a given technology, this literature shows slow adaptation on an indeterminate yet often effective trajectory somewhat akin to Lindblom’s (1959: 79) “muddling through.” Yet, this stream, too, has failed to consider how organizations contend with increasingly heterogeneous technological portfolios, because it has focused on technologies in isolation from other technologies in use in their settings.
Leonardi’s (2011: 151) study of computer-aided crash simulation, for instance, showed that engineers assessed whether the technology enabled or constrained their next project; their resulting decisions left an organizational “residue” that conditioned years of choices about whether to modify work processes or the technology itself. Likewise, Berente et al.’s (2016) eight-year study of a Systems, Applications, and Products (SAP) implementation at NASA explored how scientists, project managers, and other professionals slowly adjusted policies, routines, and features of their SAP system to facilitate efficient pursuit of various organizational goals. Despite the longitudinal and incremental focus of these and comparable works, they have not examined how organizations engage with multiple versions of a technology or the heterogeneous collections of technologies that workers rely on.
Together, these research streams show how organizations quickly settle into usage patterns after acquiring a new technology and then shift into a slow adaptation with the technology that is stable enough for managers and workers to rely on for results. This research has not asked how these dynamics might play out across a portfolio of incrementally improved technologies, however, or whether managing such a portfolio involves additional, consequential dynamics. These questions are important to consider because much technological change is of this accretive kind, so firms must commonly contend with increasingly heterogeneous technological portfolios. My field study of robotic surgery at a preeminent teaching hospital drove me to engage such questions.
Methods
Research Setting
To understand how organizations manage increasingly heterogeneous technological portfolios, I conducted an ethnographic study of robotic surgery at Fairtown. This facility, in a competitive urban-centered market, had over 400 patient beds; 500 physicians and 4,000 nurses, technicians, and support staff; as well as 24 operating rooms (ORs) and two of Intuitive Surgical’s da Vinci surgical systems. 2 Fairtown’s OR committee—composed of senior surgeons and administrators and chaired by Fairtown’s chief of surgery and chief operating officer (COO)—authorized spending $1.2 to $1.5 million to acquire each system, as well as annual service and maintenance contracts of at least $125,000 per robot. These systems were used for minimally invasive surgery and consisted of three moveable components: a control console, a computing tower, and what most referred to as “the robot”—a 1,000-pound, four-armed surgical device. Three arms on the robot held interchangeable instruments such as scissors or graspers, while one arm held a stereoscopic camera. The console had foot pedals and two multi-jointed “masters” for hand control; smooth surgery required coordinated, complex foot and hand movement. The tower both translated the surgeon’s manipulations of the console to the robot and transmitted a three-dimensional (3D) video signal from the robot to the binocular console display and two-dimensional (2D) video from one of the camera’s “eyes” to screens around the OR.
Despite the da Vinci system’s difference from existing methods and its extreme cost, in the mid-2000s Fairtown and most other top-tier hospitals made a strategic bet on this system as the future of urologic surgery. Fairtown acquired a newer version of this system in January 2013. When I arrived in March 2013, da Vinci procedures were performed in ORs that measured approximately 30×40 feet and were equipped with technologies such as movable, ceiling-mounted lights, equipment “booms” (repositionable, ceiling-mounted conduits) and monitors, an adjustable surgical bed, a nurse’s desk with a networked PC, a glass-walled supply closet for frequently used items, and three large high-definition displays on three different walls. Much of this equipment was moved between the time the patient was brought in and the time the patient was moved elsewhere. These ORs were big enough to allow this reconfiguration but cramped enough that hasty or ill-planned moves could create significant trouble.
Members of five occupational groups performed robotic surgery at Fairtown: surgeons, anesthesiologists, residents, nurses, and scrub technicians. Surgeons were senior specialists, having performed each procedure hundreds or thousands of times. In addition to receiving base pay, they were compensated per procedure, and they bore ultimate responsibility for procedure quality and for mentoring residents. Surgeons specialized in robotic or nonrobotic technique, given the stark differences between techniques and the steep retraining costs. Anesthesiologists managed patients’ consciousness and rarely interacted with surgical staff. Residents had received their medical degrees and were undergoing six years of specialized training as surgeons. Nurses had specialized degrees and were known as “circulators” because they worked outside the sterile field, moving around and doing what was needed to ensure that each procedure was smooth and well documented. Scrub technicians, or “scrubs,” set and worked in the sterile field, facilitating safe and efficient access to equipment and disposables and operating sterile equipment.
Performing Robotic Surgical Procedures at Fairtown
As with most surgery, efficiency and quality pressures were high for robotic urologic surgeries at Fairtown. Surgical workers and executives valued patient well-being and cost efficiency (Bosk, 2003; Kellogg, 2010). They all understood that surgical patients tended to do better and that Fairtown gained financially when more procedures were booked and when these procedures did not take longer than expected. They also understood that the price of failure was extreme: patients could experience extended hospital stays, disease recurrence, permanent impairment, or even death, and as a result the ensuing treatments and legal costs could be great. Everyone involved prepared for and adjusted to dynamic surgical conditions to avoid negative outcomes.
The scrub and circulator began each robotic procedure. First, they configured basic equipment. They then ran through a call-and-response check of all required supplies, draped each robot arm with sterile sleeves, and calibrated the camera’s color sensitivity and stereoscopic vision. Staff had approximately 45 minutes to perform this work. After the patient was brought in, an anesthesiologist put the patient under general anesthesia. The surgeon and residents arrived, positioned and draped the patient, and docked the robot to the patient’s abdomen via keyhole incisions. The surgeon then operated from the console. The scrub and a resident stood by and managed the patient and the robot, supervised by the surgeon. After the surgeon finished, the team backed the robot away, and the surgeon, scrub, and resident “closed,” sealing and cleaning all prior incisions. Then the anesthesiologist roused the patient, and the resident wheeled them out. The scrub and circulator undraped the robot, disposed certain materials, and left as the room was cleaned by support staff.
Data Collection
This project draws on two years of ethnographic comparative study and ten years of quantitative data on urologic surgical procedures performed through two different models of the da Vinci surgical robot at Fairtown. Early data made it clear that work involving the newer robot model went quite smoothly compared to work involving the older one and that staff greatly preferred the newer model. But for years, the top robotic surgeons and staff used the older system more frequently than the new one, and there seemed to be no serious efforts to change this fact. In part I designed my data collection approach to explain this unexpected pattern.
Participant observation and interviews
Over two years, I gathered observational data during 30 procedures involving the older robot and 20 involving the newer robot. Most procedures took approximately four hours. I took time-stamped notes documenting staff interactions and the flow of work before, during, and after each procedure. In each of these procedures and for numerous others, I helped with scutwork in the OR (e.g., running for supplies, helping people scrub in), was trained to move the robot’s arms around for sterile draping, and sat in the trainee console during procedures. I also spent many hours of informal time with staff and administrators. I also draw on 44 formal, private interviews with six surgeons, three senior hospital administrators, four scrub technicians, five circulating nurses, and nine residents. Interviews typically lasted 30 minutes and were recorded for transcription.
With six weeks remaining in my study, I produced two documents to share, in sequence: the first was a list of “hassles” that staff experienced with the old robot, and the second added a list of “ways you all deal with those hassles.” Three weeks later, I presented a draft summary of my findings to a group of experienced staff in all roles. At their request, I then presented revised findings to top hospital executives. Both presentations were recorded and transcribed. My goal was never to create change that many staff would have welcomed, though such change did occur after I left. Rather, I sought my informants’ assessment of my findings. This crucial difference aside, my late, pointed member checks on a stable yet highly irritating phenomenon bore some similarity to action research in that I provoked my informants and treated their reactions as data (Salancik, 1979; Argyris and Schön, 1989), and I handled inquiry as a potentially consequential intervention in the system I was studying (Bartunek and Moch, 1987; Van Maanen, 1988).
Archival data
I secured, cleaned, and combined several sets of medical records pertaining to each robotic procedure performed at Fairtown from January 2006–July 2015. This dataset contains several indicators of efficiency (e.g., time under anesthesia) and effectiveness (e.g., length of stay), as well as a wide variety of data that can be used as controls in statistical analysis (e.g., date, staff present, procedure, patient age, OR number). I also secured Fairtown robot maintenance logs from 2013–2015.
Data Analysis
The motivation for this study crystallized as an experienced surgeon speculated on compromised patient outcomes while struggling to operate “blind” via a compromised camera on the older robot. Workers at all levels had regularly exhibited a great deal of frustration during procedures involving this robot throughout my time at Fairtown, and safety and efficiency seemed threatened in these procedures. Roughly the opposite seemed to be true with the newer system. A full explanation for these dynamics was apparent only upon consideration of a set of interconnected practices that extended well beyond the operating room (e.g., staffing, OR allocation). I thus settled on practices (Feldman and Orlikowski, 2011) as the primary unit of analysis for this study.
This study involved two interdependent and iterative analytical streams enacted through two rounds of analysis. The first stream of analytical work involved open and axial coding of my data, multiple readings of field notes and interview transcripts, consideration of various literatures, discussion of exploratory memos with colleagues (Glaser and Strauss, 1967), and a focus on surprises and contrast (Abbott, 2004) as a way of inducing meaningful and novel perspectives that could powerfully explain the work under study. My first round of analysis yielded themes related to contrasts between work involving the older and newer robots. Some of these themes centered on organizational processes (e.g., directing more-complex cases to the newer robot), some on the practicalities of use (e.g., compromised robot functionality), and others on responses (e.g., workarounds). These themes shifted given additional, more-focused data collection and in response to interim findings from the second stream of analytical work.
The second stream involved requesting, aggregating, cleaning, and performing statistical analysis of data collected at Fairtown on various aspects of robotic surgical work (e.g., staffing, patient age, length of stay, time under anesthesia, OR number). In my first round of analysis, I produced descriptive statistics for and performed simple correlation checks, exploratory classic hypothesis tests (e.g., t-tests), and linear regressions on these data. The second round of analysis allowed for additional insights that would likely not otherwise have become apparent. Consideration of these data showed, for example, that over time, surgeons who had the most experience with the older robot performed an increasing percentage of their procedures via that robot. This was puzzling given that these top-performing surgeons detested such work. A significant proportion of key themes became evident through analysis of my field notes on the actual performance of work and records regarding such work.
In my second round of analysis, I came to see Fairtown as facing a portfolio problem: it had to contend with heterogeneous technological assets, and investment in one had implications for the other. This framing led me to build on the resource allocation (Bower, 1972; Burgleman, 1983; Christensen and Bower, 1996; Sull, 1999; Maritan, 2001; Gilbert, 2006) literature, focusing on how Fairtown allocated scarce resources across its robotic surgical systems and the implications of this allocation for the systems’ use. 3 Taking this perspective drove me to account for how resources were allocated in pursuit of Fairtown’s goals, the benefits and challenges this allocation created, and how key parties addressed these challenges to preserve results. I attended to allocations of infrastructure, talent, maintenance, and cases (i.e., patients). This drove me to attend to staff’s development of workarounds, skills, and interaction patterns with management, as these differed across the two robots in significant ways. I tracked the ways in which resource allocation and responses shifted given that these dynamics played out over several years.
By addressing the allocation of diverse resources, this new frame helped explain the dynamics after the acquisition of the second robot in ways that the current literature on technology and organizing could not. Fairtown’s OR committee acquired a newer-model robot and retained its prior model, to grow in the robotic surgery space. Fairtown’s resourcing of its robotic portfolio then proceeded through three phases: dividing available resources in ways that allowed locally sensible initial usage patterns yet began to degrade the older technology, adjusting resources in ways that extended successes yet further degraded the older technology, and making do with the degrading technology in ways that preserved results and limited the hospital’s motivation for change. To develop my findings, I explored how these resourcing dynamics preserved results with both robots, and I considered other consequences for workers and the organization. The findings that I present in descriptive form are corroborated by multiple interviews, direct observation, or both. I include data or references to sources to substantiate points central to my analysis.
Resourcing a Technological Portfolio: The Case of Fairtown’s Surgical Robot
Before the Portfolio—Allocating Resources to a Single New Technology
Fairtown contended with its first da Vinci robot in predictable ways, which shaped the conditions that would later be relevant to the more complex and fraught task of fielding two. Fairtown’s OR committee purchased its first da Vinci in 2006:
So, one day in 2005, [top surgeon] comes to me and he says, “We need a robot.” So, I said, “Okay, fine.” I want to be contemporary; I want to be on the cutting edge. So, I . . . convince them [administration] to spend two million bucks and about 200,000 a year for a service contract, and we get the robot right away. (Chair, Urology)
The robot was unfamiliar, but the OR committee saw it as likely disruptive to the practice of urologic oncologic surgery. They therefore saw it as a threat to market share and status in their competitive local market. The OR committee then allocated preferred infrastructure and experienced talent to create market-winning robotic surgical capability, and surgical staff drew on these resources to develop tools and procedures to facilitate progress toward these goals.
Allocating best available infrastructure
For this first robot, infrastructure took the form of OR15: a well-equipped, sufficient space with proximity to physical resources such as supplies. For several months, Fairtown had relied on the robot’s mobility to run robotic procedures in a variety of ORs. But executives rejected this practice in favor of a dedicated OR, as moving the robot around damaged it:
We made the decision, largely due to repair history, that we would no longer allow the robot to be transported around. It doesn’t take much to hit a door . . . to put it out of calibration. So, we kept that in OR15. That’s pretty much best standard around the country, you don’t want to be transporting that around. We treat that thing like a CT scanner. It needs to be used all of the time. So, we made that an exclusively robotic room. (Fairtown COO)
Allocating OR15 to Fairtown’s only robot reduced the need for costly repairs and related downtime, but this OR was also one of the two most preferred by all surgical disciplines in the hospital. OR15 was among the largest, which greatly facilitated smooth setup and repositioning required to run an efficient robotic procedure. OR15’s size also meant increased closet space in and just outside the OR, which could be used for storing backup equipment related to robotic surgical procedures. This OR was also directly across the hall from the single elevator leading down to Fairtown’s central supply department and was directly adjacent to the hospital’s main automated dispensary for surgical supplies and medications. All experienced surgical staff knew that when they worked in OR15, they could expect the most accurate and rapid restocking of surgical supplies possible at Fairtown. Allocating this preferred infrastructural resource to the robot thus significantly reduced the likelihood of surprise, which allowed workers to focus and perform their work well.
Allocating best available talent
Allocating talent took the form of leadership focus, specialist hires, and top talent specialization. On the leadership front, the chair of Urology took the unprecedented step of handing off his caseload and related personal revenue to be the first surgeon to go through vendor-led training on the robotic system. But he struggled with the technology, so he hired two surgeons who had just completed robotic surgical fellowships: “I recognized [after training] even though I had done about 3,000 open prostates I was going to hurt people doing this [robotic surgery]. So, then I went out and got two fellowship-trained people.”
Fellows commanded premium pay, and recruiting just one would have been a major expenditure; attracting both represented an extraordinary outlay. Fairtown’s world-renowned expert with conventional tools also made the leap to robotic surgery, and over the next year and a half, this master and the two fellows developed a set of best robotic surgical practices at the institution. They preferred to work with experienced staff, so the best OR nurses and scrubs shifted to robotic surgery as well. And finally, the OR committee decided to create a robotics program coordinator (RPC) position, selecting an OR nurse to be responsible for robotic maintenance and sending her for two weeks of training. Thus, the full panoply of top surgical talent was allocated to support the new-to-Fairtown practice of robotic surgery, greatly accelerating the development of individual and collective robotic surgical capability.
Developing tools and procedures
Top OR nurses then drew on these resources to develop tools and procedures to support work involving the new robot. They created checklists for materials and steps in robotic procedures, adding these as custom forms into key information systems and printing copies of these for the OR. Experienced surgical staff also crafted a standard set of procedures for OR preparation and cleanup with the environmental health and safety department. All relevant staff were trained in these tools and procedures as well. The RPC drafted and secured central supply’s signoff on standard equipment requests (e.g., instruments, sterile drapes) based on staff and surgeon input; labeled locations for standard supplies in OR15; moved the robot components into permanent, standard positions in the OR; and created dozens of self-adhesive signs outlining standard operating procedures (e.g., “KIDNEY CASES—THIS ARM TOWARDS PATIENT’S FEET”). These tools and procedures, as well as related allocations of infrastructure and talent, generally enhanced efficiency and mostly remained in place for the duration of this study.
Experienced talent settled routines for robotic surgery within a matter of weeks. The OR committee adapted a “block time” system for sharing costly OR time, allowing surgeons to anticipate when they might book a robotic procedure. This system privileged the three people who could already operate robotically, so they could rapidly build surgical volume, but it left slack for other urologic surgeons to build skill so they could take on more patients. Central staffing created a 2+1 model to support each robotic procedure: a circulating nurse, a scrub, and a “float”—a scrub who split their time between two or three procedures, prioritizing support for robotic ones. All these roles and routines were fairly stable and in place through the acquisition of the second robot in early 2013, allowing everyone involved to build appreciable skill.
Thus, as the literature on technology and organizing would predict, Fairtown staff at all levels aggressively allocated experienced talent and top infrastructure to support the rapid development of routines that delivered strong robotic surgical capability. These resource allocations endured, and staff made ongoing, relatively minor adjustments over time, such that staffing and executing a robotic procedure remained predictable and efficient.
The Imperative for a Technological Portfolio: Growth
With each passing year, top teaching hospitals further accepted robotic surgery, demand for urologic robotic surgery increased markedly, and other surgical disciplines began developing robotic capability. Given that Fairtown was leading the way with this technology, it noted these shifts earlier than many hospitals did. Soon after Fairtown acquired the first robot, the OR committee drove urologic surgeons to higher utilization and brought other specialties online. Thus, beyond seeking new revenue in established specialties, the OR committee pushed adjacent disciplines to develop robotic capability. They expected this change to be cost effective compared to the first effort, as they could take advantage of infrastructure, routines, and skills developed during the first robotic push.
Utilization went up. The OB-GYN and colorectal teams engaged as they discovered that other top institutions were offering robotics fellowships and the best medical students were prioritizing these programs in their residency searches:
I took it to the [colorectal] group [in 2008] as like, “This is something we should think about. I’d like to start doing it.” And I think there was a lot of attachment to the laparoscopic way of doing things. But I think what happened in those next few years [from 2009–2012] is that a lot of the other big [colorectal] training programs started to pop up with people doing robotics. So, it’s almost like peer pressure in a way, see what I mean? (colorectal surgeon)
In addition, in 2009, Intuitive Surgical announced the Si, a new model of surgical robot that offered incremental feature additions such as a dual console for instruction and new instruments for cancer detection and for colorectal procedures. Such activities were possible with the prior model, but the new features facilitated them for a broader and less skilled user base. In mid-2012, then, the OR committee accepted surgeon-supplied evidence showing that Fairtown could no longer meet rising demand with a single robotic system.
Managing a Portfolio of Technologies: Dividing Resources Among Newer and Older Technologies
After its purchase of the new robot model, which arrived in January 2013, Fairtown’s resourcing of its robotic portfolio proceeded through three phases: dividing limited resources between technologies, adjusting resources, and making do. Two resources were most salient in the first phase: infrastructure and talent. The findings that I detail here and in the next two sections are represented in Figure 1.
Overview of Findings: How Fairtown Preserved Outcomes as Its Surgical Robot Portfolio Became More Heterogeneous
Dividing infrastructure
Fairtown’s OR committee allocated the best available infrastructure to the new robot, primarily by moving it into the best space: OR15. This decision was made to facilitate smooth operations and to develop OB-GYN and colorectal robotic skill and enthusiasm within these groups—all necessary outcomes to ensure a satisfactory return on this investment. Achieving these goals was ostensibly easier with the new system in this space: by that time, staff had well-worn robotic surgical routines that made operating conditions more predictable, and new surgeons could ask for relevant resources and receive them quickly. Existing routines needed only minor modifications to accommodate the new robot, and in general these changes reduced complexity; for example, the camera on the new robot did not require manual calibration and white balancing, so it could simply be attached and turned on.
With OR15 claimed for the new system, Fairtown allocated slack, substandard infrastructure to the older model. Fairtown did not have the robotic surgical volume to allocate a dedicated OR to the older robot. Thus, the OR committee and logistics staff now deployed it to OR4, OR5, and OR11 as these spaces became available, even though, as a circulator recalled, they had previously rejected the practice because it damaged the first robot: “[two] years ago, they [administration] thought . . . ‘look the robot can roll around it has wheels we can just put it in any room,’ and it was just insane they would put it in [ORs] 5 or 11.”
The ideal storage location for this robot was the large closet just outside OR15, as this location would have facilitated rapid resupply and movement to adjacent ORs. But this closet had been appropriated for higher-value equipment, so another closet—a tenth of a mile away from relevant ORs—was allocated to house the older robot. This meant that for each procedure, the 2,500-pound older system was moved from this distant closet by nonmedical, entry-level logistics staff through three sets of double doors to OR4, OR5, or OR11. It was set up, used, broken down, and returned by other entry-level logistics staff to the closet. Large scuffs, cracks, and gouges became increasingly evident on parts of the console and robot that touched walls and doors en route, indicating regular, forceful collisions.
In addition, central supply withheld specialized attention from the older system. They had reoriented their routines to accommodate the new robot, and so they packed case carts with drapes and cameras suitable only for the newer robot, even when preparing for procedures involving the older model. From the new robot’s arrival in January 2013 until I left in 2015, the older robot received only slack, substandard infrastructural resources. It began to degrade as a result, eventually making it more difficult to use.
Dividing talent
The newer system made it easier for inexperienced talent to learn how to perform robotic surgeries. For example, the system’s dual console facilitated proctoring (i.e., mentorship) by experienced surgeons:
We pushed them [GYN]. They wanted to learn, so N [urologic robotic surgeon] helped train them. He proctored every case they did in the beginning [via dual console] so they wouldn’t screw it up. Because they wanted to do it. They were losing, they thought, market share. (Chief of Surgery, Urology)
Experienced surgeons offered mentorship and shared the new robot with inexperienced surgeons because doing so offered a clear, quick path to sustainable success in adjacent markets, with obvious financial benefits for both groups and for the hospital.
Thus, in the initial phase of dividing scarce resources between the two systems, inexperienced surgeons were scheduled to use the newer robot, while experienced surgeons could use either system: they could perform procedures in OR15, and they could also use the older system in other ORs to fill out their schedules. The newness of the technology attracted inexperienced surgeons (Beane, 2019), who benefited from the new system’s availability, the quality of instruction they received from experienced surgeons, and the general smoothness of operations. To make this capacity development feasible, surgical staff modified standard staffing processes to support the new working arrangements, such as by ensuring that proctors’ time was not double counted against their standard block time in OR15.
Short-run consequences of infrastructure and talent allocations
The initial division of infrastructure and talent meant that each influenced the other in important ways. In early 2013, experienced surgical teams performed procedures using the older robot in ORs that were too small; these procedures did not go well. System components and cabling were packed too tightly in these spaces, which compromised safety, sterility, and access to components. When a top robotic surgeon entered OR5 to perform her first procedure there, she canceled the surgery after the patient was anesthetized. She concluded that if the patient went into cardiac arrest, it would be impossible to respond appropriately: “[I]t was so small, I actually have pictures because it was dangerous, and I complained, because I said if you had a code [cardiac arrest], there would be no way to access the patient” with necessary equipment and supplies.
The OR committee immediately responded by booking cases involving the older robot only in OR4, thus eliminating this perceived threat. The resulting infrastructure allocated to the older system was far from ideal, however. For instance, OR4 was far from needed supplies:
It’s the robot, not the room. [Sigh] Unless of course, they want something that’s down by room 4, such as cysto[scopy] supplies or something. Or if they are starting to put the foley [catheter] in and they need to dilate the patient’s urethra, we have to run down to room 21. Or if you need spare parts, you have to run to 15. They had to call me in Jamaica to find the spare camera I had [stashed]. I told a few people about it but [makes over-the-head gesture and whooshing noise]. (RPC)
Nonetheless, Fairtown’s most experienced talent followed the older robot to OR4. These surgeons and a small group of top circulators and scrubs were so familiar with the older robot, and faced so much demand, that they accepted this arrangement as adequate. Though none of my informants could recall any explicit conversation or decision along these lines, all of them understood that they had the case volumes to warrant such usage, and it was up to them to establish the way forward with the older system. Fairtown’s norms dictated demand-driven usage by all staff, but everyone understood that some staff members were better able than others to handle problems with the older robot, so experienced robotic surgical talent was preferentially staffed to work with it.
The lack of expanded functionality and dynamic, operationally constraining locations for procedures led to a rapid preference for the new system and aversion to the older one. Thus, within the first few months of 2013, the newer system became known as the “new robot” and the previously prized system as the “old robot.” Most cases were soon performed with the new robot, allowing Fairtown and the surgical teams involved to make good progress on revenue and capability goals.
Adjusting Resources for Newer and Older Technologies: Maintenance, Cases, and Talent
After getting the new and old robots situated and functional, Fairtown adjusted resource allocations as it further settled work involving both systems. Talent allocations intensified, and two additional resources became relevant in this phase: maintenance (the provision of preventative and reactive technological repair) and cases (patients with different problems of varying complexity).
Adjusting maintenance allocation
Maintenance resources were preferentially allocated to the new robot, which compounded initial usability challenges with the old robot. Repair logs and my email correspondence with the RPC indicate that minor preventative maintenance greatly decreased on the older model shortly after it was moved out of OR15, while such maintenance never waned on the newer model. These patterns became more exaggerated over time, as the older robot saw six major repairs during 2013, while the newer robot had none, for example:
Since we use the Si [newer robot] more often, the cannula mounts become loose, so they have to be replaced [very minor repair]. (call Intuitive, arrange for repair guy to come at a good time). The S [older robot] issues do tend to be more of the major sort—camera head/cable or other fiberoptic cables. (RPC, email)
The major repairs on the older robot involved replacing key parts: the masters, camera and camera cables, clutch pedal, and various arm components. By early 2014, these components had degraded to the point that they compromised functionality: surgical vision and motion became increasingly difficult, and instruments were less reliable. Other degradation that did not lead to major repairs also became increasingly evident: the lamp that illuminated the inside of the patient failed with increasing frequency, one of the two lenses in one of its cameras became incurably “foggy,” instruments (e.g., scissors) failed to load or stay in place because the components that held them in place had weakened, and diverse faults with aging fiber-optic cables led to dramatic surprise degradation and reinstatement of the video signal captured by the robot’s camera.
Fairtown consistently provided top-notch preventative maintenance for the newer system, ensuring near-pristine functionality for most robotic surgery. But the degradation of the older robot continued such that in the second half of 2015, surgery involving this robot evinced a tangle of serious, intermittent problems that, if left unaddressed, would likely have threatened safety and efficiency:
New robot, easier to drape and coordinate. Older shitty robot, harder to manage, breaks down, so it causes some stress to begin with. . . . people aren’t as happy because it’s the older shitty robot, surgeons are on edge, room’s on edge,
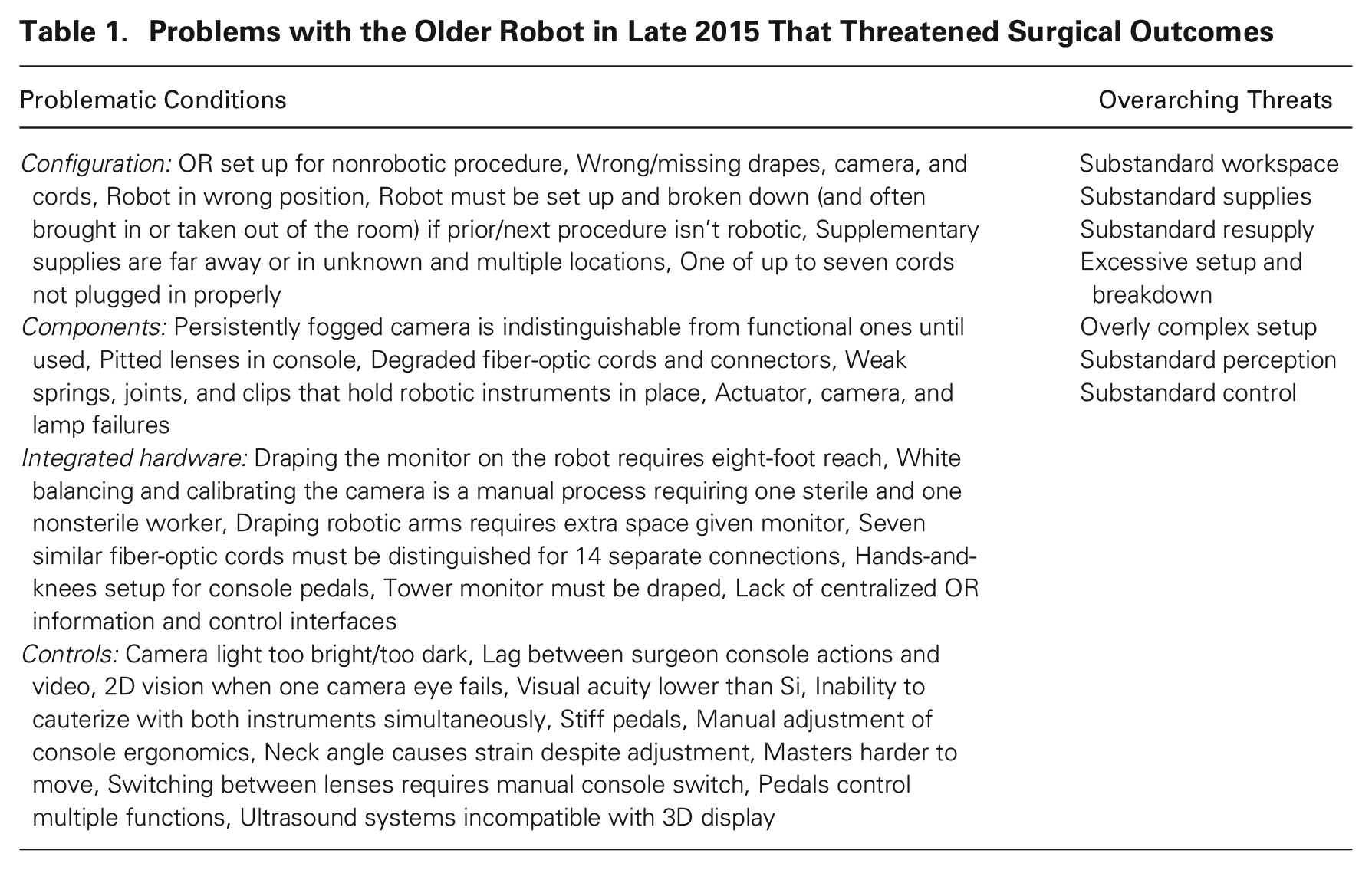
As Table 1 shows, the allocation of maintenance produced 38 significant obstacles by late 2015 related to setting up, breaking down, supplying, staffing, and operating with the older robot during procedures. No one obstacle was a severe threat; aggregated, however, they presented a formidable challenge, and no one quite knew when many would happen.
Problems with the Older Robot in Late 2015 That Threatened Surgical Outcomes
Adjusting case allocation
Shortly after OR4 was designated for procedures with the older robot, I observed that the OR committee allocated cases differently between the two robotic systems. Specifically, patients with complex problems were scheduled to the new robot and patients with simpler problems to the old robot, even when this allocation meant delays and logistical inconvenience. This practice increased over time, but most surgical staff, including surgeons, had limited or no exposure to the OR committee’s deliberation processes. When I asked how cases were distributed across robots, no surgical staff in any role mentioned the possibility of allocating based on case complexity; they instead indicated that policy and norms dictated scheduling cases on whatever robot was available, to maximize utilization and throughput. Yet, allocating by case complexity slowly became common and was apparently first discussed by surgical staff toward the end of my study when I presented my findings to the group of professionals most often responsible for robotic surgery with the old robot:
In almost all ways, operating with the new robot was easier, and this allowed surgeons to do top work on their hardest cases. And as the surgeon noted above, allocating complex cases to well-resourced technology likely contributed to more-comparable work experiences between the old and the new robot, making the difficulty of operating via the older robot less apparent to everyone.
Adjusting talent allocation
Around the same time, initial patterns of talent allocation across robots intensified: experienced talent was allocated to the old and less-experienced talent to the new. In particular, the more that experienced surgeons, circulators, and scrubs worked with the older robot, the more they did so going forward. This occurred for different reasons, as people in different roles had more or less discretion in the matter. From 2013 to 2015, the two most prolific robotic surgeons at Fairtown performed a disproportionate and increasing percentage of their procedures on the old robot, while the 16 other robotic surgeons at the hospital secured preferred and expanding access to the new robot (see Table 2). These two experienced surgeons knew they faced more demand, so they used the old robot more than the others did, but they were not aware (until I shared the data) that they were using the older system more as time went on: “I’m surprised it’s increasing,” one of the two told me. “I didn’t feel that increase. Part of me is like, are they sneaking this in? Are they looking at my schedule and masterminding this?”
Robotic Surgeries Performed at Fairtown by Surgeons’ Experience with the Old Robot
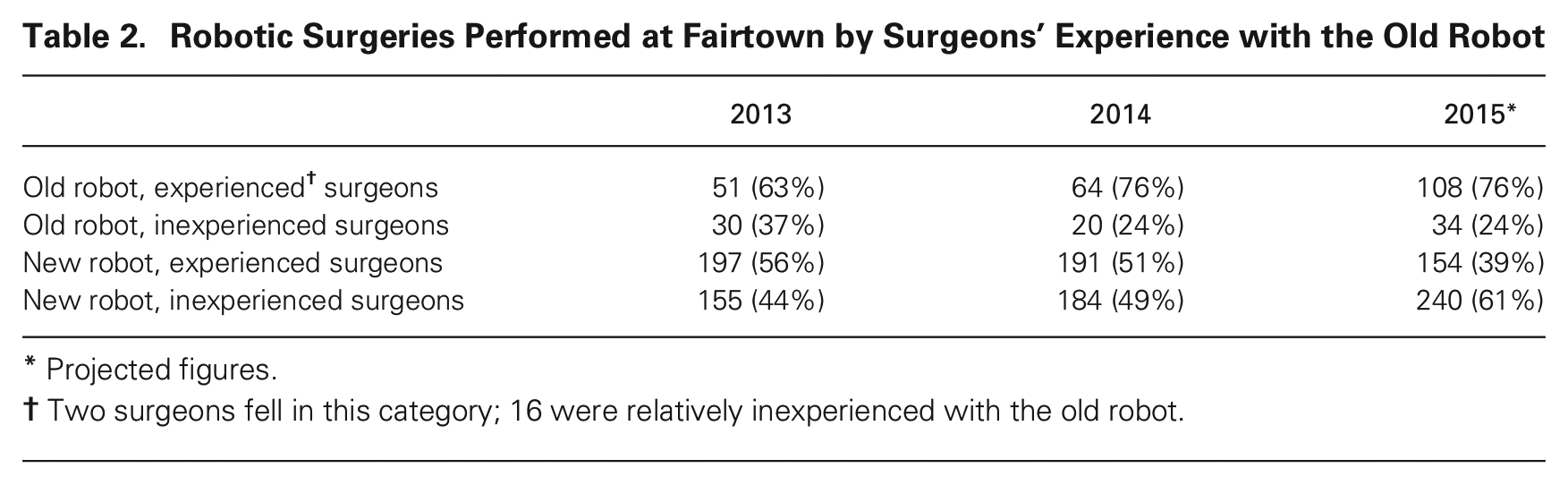
Projected figures.
Two surgeons fell in this category; 16 were relatively inexperienced with the old robot.
This adjustment also occurred because the 16 other surgeons became increasingly aggressive about avoiding the older system, claiming that it lacked critical features or that they could not use it safely or efficiently. Referring to a single OB-GYN surgeon willing to use the older robot, the RPC said, “GYN’s the only other service that uses it [old robot]. Colorectal won’t. Flat out.” Finally, less-experienced talent was also allocated to the newer system to facilitate the proctoring required to create colorectal and OB-GYN robotic surgical capacity. The newer system’s dual-console setup was designed and purchased to facilitate just this sort of activity, and the operational conditions in OR15 reduced distractions, helping everyone to cope with this additional complexity.
The adjustment to talent allocation was more challenging for surgical staff than for surgeons. First, the scrubs and circulators who had the most experience with the old robot were almost always formally staffed to procedures with that robot. Everyone, including top scrubs and circulators, understood that experience with the old robot mattered a great deal in these procedures:
They do try to keep teams together [who know the old robot]. It’s almost like an unwritten rule, like K [top scrub] and I work together [with the old robot] probably 90 percent of the time. . . . we’re just a team that kind of gels and just works really well together. (Circulator)
Second, supplementary staff, in the form of the “third person” to be shared among simultaneous procedures, was preferentially allocated to the new robot, thus amplifying the difficulty for experienced scrubs and circulators with the older one:
The scrubs and circulators who were involved only in procedures with the newer robot often had less robotics experience than those staffed to procedures with the older robot. Thus, as with OB-GYN and colorectal surgeons with less experience, these less-experienced surgical staff were treated as if they required more help with the newer robot than a lone top scrub or circulator did with the older robot.
Finally, the RPC was preferentially allocated to deal with crisis-oriented repairs to the old robot. Whenever either unit needed repairs or troubleshooting, she became involved either on her own or with vendor technicians. She had not analyzed her workload by robot, but at my request she went over her email and troubleshooting logs and counted the volume of her interactions regarding these responsibilities. The following email to me indicates that she spent a disproportionate amount of her time and effort with the old robot, even though (primarily preventative) repairs to the newer unit were more frequent: “15–20% of my time is spent coordinating repairs—10% S [old model]; 5% Si [new model].” Thus, regardless of their formal role, all experienced robotic surgical staff were assigned a disproportionate and increasing set of opportunities to work with the old robot as others’ opportunities waned in this regard.
Making Do with Prior Technology via Workarounds, Workaround Mastery, and a Venting Cycle
The division and adjustment of resources degraded the older robot, and no further resource allocations were forthcoming, leaving experienced staff to contend with related difficulties. Despite the apparent safety and ease with the new robot and risk and trouble with the old robot, however, my inquiries about quality and outcomes in procedures using the older system were met with confidence. An experienced surgeon told me, “I think that my outcomes are the same [regardless of the robot].” And an experienced circulator said, “You might actually see it [case length] get shortened [with the old robot] because K [experienced surgeon] gets so pissed off. I don’t think there’s going to be that much of a difference [in outcomes] because of the skill of the surgeons.”
Without explicit evidence to support this view, these experts proceeded as if the mounting challenges associated with the older robot did not seriously threaten critical outcomes. And their confidence was not unfounded. They had rich access to informal evidence that outcomes were not significantly threatened: their own extensive, increasingly masterful workarounds with the older robot. At the same time, their limited concern about the old robot was reinforced via a venting cycle: a pattern of interactions with management that limited inquiry by all parties regarding the troubles with the older system. These dynamics constituted a collective effort to make do with the older system despite its ongoing and increasing degradation.
Making do with prior technology by devising workarounds
Significant work was required to preserve results, given that resource allocation had steadily degraded the older robot. To start, experienced talent developed a range of workarounds to contend with the degradation-related difficulties listed in Table 1. These ostensibly awkward and inappropriate alternatives to standard surgical techniques addressed problems resulting from limited infrastructural and maintenance resources. Notably, these workarounds had to be completed within the time restrictions associated with robotic surgical procedures generally, and the time restrictions were set with the new robot as a template. Thus, staff had to do more work with the old robot to equal standards in the same amount of time. Table 3 categorizes and exemplifies all the workarounds involving the older robot by the end of my fieldwork. I present examples in this section and throughout the rest of the article.
Workarounds Enacted as of Late 2015 to Preserve Outcomes with the “Shitty” Robot
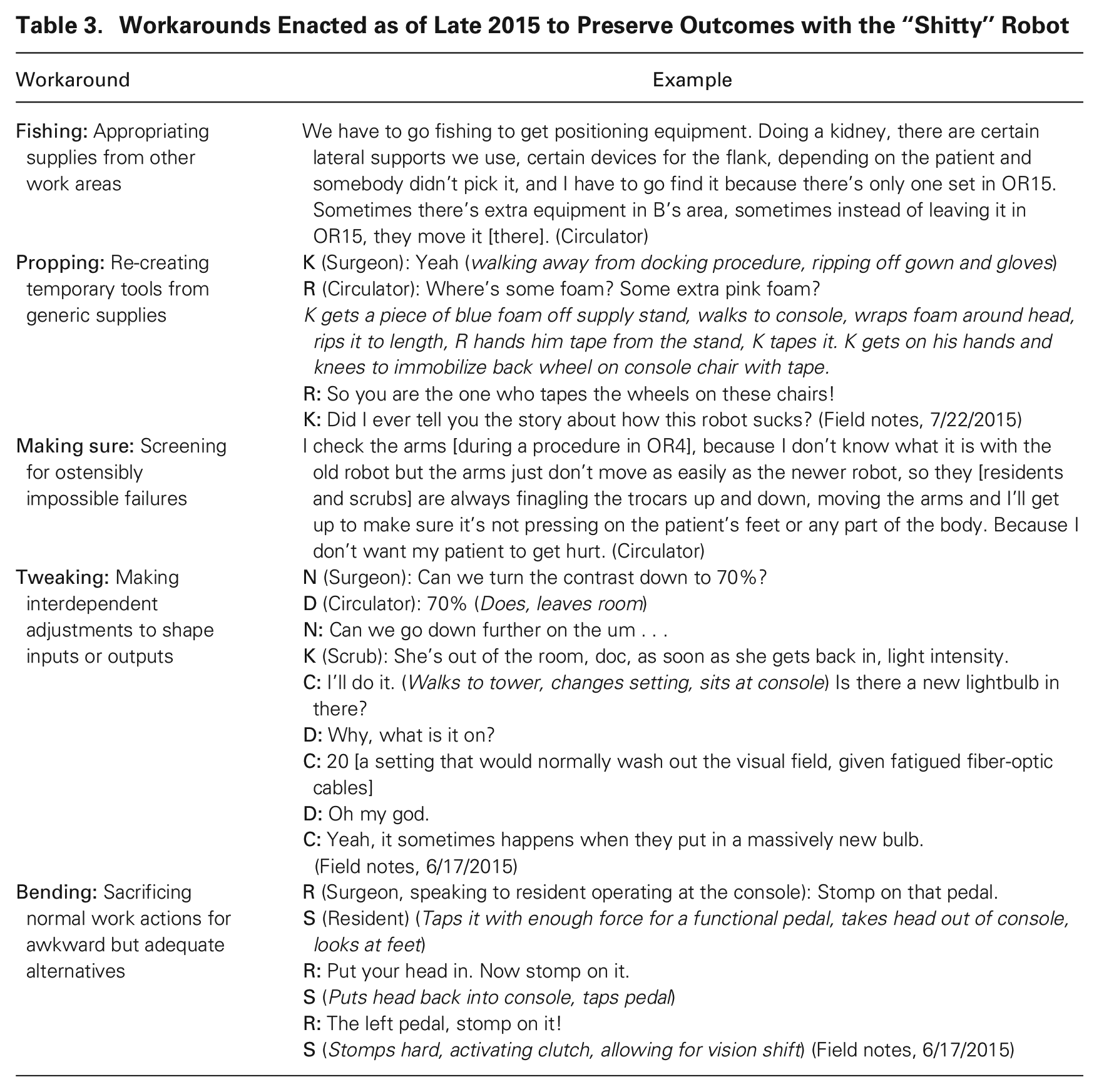
Some workarounds were preemptive, as some difficulties with the old robot required remediation well before the patient arrived in the room. For example, supplies were far away and were often not delivered, so nurses found and stashed spares on an ad hoc basis. Scrubs and nurses also quickly found rarely needed equipment such as lumbar braces (needed for kidney cases) from other operating rooms before heading to their procedures for the day. Three workaround types were salient here: “fishing,” or appropriating supplies from other work areas; “propping,” or re-creating temporary tools from generic supplies; and “making sure,” or screening for ostensibly impossible failures. Given that these practices focused on preparatory work and required interaction with surgical staff in other ORs, the burden for enacting them largely fell on scrubs and circulators.
Other workarounds were responsive, focusing on coaxing adequate functionality out of the degrading robot in the heat of the moment. Surgeons devised awkward, nonstandard means of accomplishing critical surgical tasks, such as operating with monocular vision. Staff did the same, such as finding ways to adjust contrast and brightness in the system lamp that conveyed light into the patient, to make up for failing fiber-optic cables. Staff also rushed their work, given that performing workarounds meant more tasks without more time to do them. Two workaround types were salient here: “tweaking,” or making interdependent adjustments to shape input or outputs; and “bending,” or sacrificing normal work actions for awkward but adequate alternatives. Given that these workarounds focused on the performance of surgical work, the burden for enacting them largely fell on surgeons.
Beyond the workarounds mentioned here, medical staff attempted and abandoned additional workarounds during my study period, either because these were not effective or because conditions changed to make them unnecessary. None of this incremental invention was codified, discussed in detail, or formally analyzed for improvement. It was simply done, and my informants almost never discussed their workarounds in interviews away from the OR.
Making do with prior technology by mastering workarounds
Given the decreasing functionality of the older robot, inventing workarounds was not enough to preserve results; experienced surgical talent also had to master these workarounds through repetitive practice. Staff learned to adjust surgical instruments and lighting systems in unconventional ways to allow for proper technique; they moved their materials stash to a single cart, stowed it in a standard location, and expanded it to include backup robotic components; surgeons refined techniques so they could operate with compromised vision and control capability; and everyone learned to force sticky or unresponsive components more effectively. Such mastery was feasible because these degradation-driven issues recurred. Each time they did, workers got practice with their workarounds and refined them. The resultant skill thus left surgeons, scrubs, and nurses better prepared to enact their workarounds for a range of familiar surprises:
The mastery they had developed to enact and modify these workarounds limited experts’ perceptions of threat from their use of the older robot. These experts became confident in their improvised techniques, and so they assessed the work with the old robot as problematic but manageable and normal. Thus, no one problem or change associated with the degrading robot was cause for alarm, work stoppage, or formal calls for change; problems were experienced as bumps in the road on the way to results. None of these professionals identified the complete range of problems and workarounds with the degrading robot, nor did they discuss the long list of problems in detail. They just performed workarounds to get their jobs done and then moved on. As an experienced circulator said, “The surgeons have no idea what it takes to get a [old robot] case going, I don’t think. They have no idea. All they do is come in and say ‘Are you ready, are you going to be ready?’”
From 2013 to 2015, no one—neither surgical workers nor managers—was deeply motivated to significantly reconfigure work involving the old robot. Mastery with workarounds stabilized the situation and, in particular, kept experienced talent involved; they did not treat the situation as a significant threat until I prompted them at the end of my study.
On another level, however, the increasing difficulty and nonstandard operating procedure were threatening. As documented in the literature (e.g., Fox, 1996; Tucker, Edmondson, and Spear, 2002), improvisation and workarounds are required for everyday medical practice, and this was true at Fairtown. But the workarounds needed to do effective surgery with the old robot, such as surreptitiously taking supplies from other ORs or operating with only one eye (i.e., with 2D instead of 3D vision), violated professional norms to an unusual degree. Results seemed threatened as well. Taking supplies from other ORs could leave other teams without them and disrupt inventory tracking systems. Operating with one eye could slow the work and cause injury or cancer to spread. And at the very least, any of these practices could have earned reprimand or limited career prospects. All of this grated against these professionals’ standards for surgical technique. No one could pinpoint when the older system was renamed, but by the fifth major repair—replacing the right master on June 10, 2014—all experienced staff consistently referred to the older system as “the shitty robot.”
Making do with prior technology through a venting cycle
If the staff perceived conditions involving surgery with the “shitty” robot as a serious threat, as they had in early 2013 before the system was moved, prior resource allocation patterns would likely have been disrupted and reconfigured. But the perception of a serious threat did not occur. In part, talent was mollified by using the newer system to perform most robotic surgeries and by their mastery of the workarounds noted in Table 3. In addition, the potential for threat perception diminished as surgical workers and hospital executives enacted what I call a “venting cycle”: a new interaction pattern regarding work with the older robot. The cycle involved two practices: “griping,” or the surgical staff making vague, negatively charged claims about work involving the old robot, and “sniping,” or managers skeptically demanding proof of these claims at a distance, without follow-up.
Griping
Despite their surprise at my presentation of findings at the end of my time at Fairtown, surgical staff were not unaware of their plight. This was evident when they expressed vague frustration while working with the older robot:
[The same eye of the camera fogs again within two minutes.]
Their expressions of frustration increased over time and sometimes occurred outside the OR. Staff (primarily surgeons) selectively expressed frustration to hospital executives, most notably to Fairtown’s COO and chief of surgery. The bulk of their feedback was vague and emotionally charged. For example,
It’s financial. That’s it. It’s all about money. They don’t want to spend a nickel at this point. They are going to ride this pony [aging robot] until the pony doesn’t ride anymore. And if I suffer, and I do more on that old robot than any other person in this institution, right? I mean it’s unbelievable. They don’t give a shit. (Surgeon)
The talent who rarely worked with the old robot had limited (though quite difficult) experiences with it, and experienced talent had become accustomed to the difficulties. And most cases were done via the new robot. Thus, even though both inexperienced and experienced talent expressed frustration, they did so with little specificity, which limited executives’ focus on the situation.
Experienced surgeons also kept their griping vague because they were concerned that the COO and chief of surgery perceived it as unsubstantiated complaining without follow-through to address related problems. They therefore limited their attempts to raise concerns about performing surgery with the older robot. I saw this most poignantly revealed in a reply-all email to the experienced surgical team from one of these surgeons. I had asked whether anyone had any reservations about inviting the COO and chief of surgery to my first findings presentation on 9/24/15. One surgeon responded, “Yes I don’t want to get ‘labeled’ a ‘disruptive physician’ (any more than already).” While the concern limited their griping, it did not lead them to willfully hide profound safety or efficiency concerns: instead, they vaguely named any troubles in the private confines of the work and moved on, retaining less detail for any subsequent griping to executives.
Sniping
For their part, the COO and the chief of surgery, himself a surgeon with over 20 years of experience, did perceive these sporadic comments as griping and judged surgeons harshly for engaging in it. Responding to my presentation of findings on trouble and workarounds with the older robot, the chief of surgery said, “A lot of that, you do that, that’s what you do as a surgeon. It’s a bad workman that blames his tools.” On a certain level, these executives agreed with the experienced surgical talent: the difficulties with the older robot were not good, but they were rare and workable, and experienced talent should proceed without making much of them. Thus, when they heard griping, executives sniped back at these surgeons, demanding firm evidence or categorical claims that using the old robot threatened key outcomes:
I tried to pin it on the guys [surgeons] the other day. They don’t want to use the old robot. It drives them crazy, they’re like “[COO], the new one is so much better!” I said okay, tell me that it’s dangerous. They won’t do that just yet. Give me that and I can do something. I’m not a clinician. I can only tell you it’s working technology. (COO)
The rarity of serious problems and the apparent effectiveness of the surgical staff’s workarounds left them poorly equipped to make sweeping claims about the danger of the old robot. None of these workers kept a list of the technical troubles with the robot. None had named, listed, or captured processual data on their workarounds. And I did the first and only data collection and statistical analysis with respect to robotic surgical outcomes at Fairtown.
Executives could more easily justify focusing on problems that represented clear threats via explicit information or firm claims about trouble. They had neither in this case. They therefore did not follow up on these challenges to learn more, whether by watching a procedure with the old robot, assigning someone to do an audit, or simply asking for empirically concrete examples of the nature and scope of the difficulties in the work. The lack of follow-up contributed to experienced surgical staff’s assessment of the COO and chief of surgery as indifferent to their suffering and practical trouble, thus reinforcing the cycle:
It’s all I have to operate on this ridiculousness, in the corner of my vision, so I can see what I’m doing. Otherwise, if I put it in the center of my vision, it lights up, see? [Does so, surgical site glares, detail washes out]
I was particularly surprised that this venting cycle limited threat perceptions so much. First, this was life-and-death work: if anyone, anywhere was going to note potential threats to efficiency and safety in the workplace, it should have been here. Second, I listed the 38 technical problems in 2015 on my own but had solicited them from experienced staff, presumably raising awareness as I did so. Third, these were the same workers who had followed the old robot to OR4, faced a growing mass of technical trouble, and developed workarounds to compensate. And fourth, these workers did most of their robotic surgical work via the newer robot; I expected this stark contrast with the older robot to increase threat perception. And yet the empirics were unequivocal: as I presented my list of problems and related workarounds to experienced surgical staff, all of them expressed strong and wide-ranging surprise. A scrub responded, “Wow, I’ve never really thought about all of the things that go wrong. I would agree that this is very accurate.” When I asked a surgeon why they were surprised at the list of hassles I identified, they responded, “These are all subtleties. But if you do it [work with the old robot] it becomes an automatic . . . you achieve some autonomy so you do some movements automatically, [so] using the old one is [only] a pain.”
The RPC, who was the first stop in the formal reporting chain regarding safety or other quality issues related to robotic surgery at Fairtown, saw things similarly to these surgeons and staff members. She routinely reported and resolved relatively extreme, time-bound threats to safety and efficiency regarding the robotic systems; for example, she was instrumental in resolving the initial crowding problems with the older robot in too-small ORs. Yet, she was involved directly in much of the remaining work, griped with her colleagues, and did not generate reports on the relatively minor problems that accreted in this work as time went on.
Many of the factors I identified above were critical for limiting perceptions of threat and thus ensuring the stability of this arrangement. Experienced talent did not much problematize their work with the older robot and therefore did not deliberately call much attention to the situation. These surgeons used the older robot to earn money and to help patients with simpler problems. Most of their work was performed with the newer system. And everyone began to see positive results from allocating inexperienced talent to the new robot, as proctoring and straightforward operating conditions had offered the colorectal and OB-GYN groups greatly expanded opportunities to build capability and expand their patient bases. Thus, experienced talent allowed the situation to continue, and the older robot became more an irritant than a threat.
Organizational Consequences
The dynamics involved in Fairtown’s resourcing of its technology portfolio produced several results that the organization valued from the outset: increased capability for new markets, increased productivity, and equivalent work results from newer and older technology.
Results preserved
The escalating allocation of inexperienced OB-GYN and colorectal robotic surgeons to the new system greatly reduced internal barriers to capability for adjacent surgical markets. The OR committee was therefore satisfied to see expanding volume of colorectal and OB-GYN robotic procedures (and the implied creation of surgical capability) from 2013–2015, relative to 2012. Relatedly, this change allowed these disciplines to more rapidly and credibly present themselves as emerging centers of expertise, thus improving their ability to attract top talent. Surgeons were likewise glad to perform most of their procedures using the new system. After a week of operating on the older robot, an experienced surgeon sitting down at the new robot spoke for most in this regard: “I love you, you little robot, I’ve missed you” (Field notes, 6/18/2014).
And while use of both systems was never ideal, preferentially allocating experienced talent to the old robot satisfied both top surgeons and the OR committee: experienced surgeons could meet surplus demand and expand the urologic market share by booking more cases on the older robot. Thus, robotic surgical productivity increased across the board.
These resourcing patterns also ensured comparable patient outcomes in all robotic surgery at Fairtown. It took me nearly a year to collect the records required to assess staff claims of clinical efficacy, as no one had done so and the data lived in different departmental databases. My analysis of these records verified workers’ intuitions: an independent-samples t-test on data from 2013–2015 shows that when surgeons were experienced with the older robot, their patients were under anesthesia for amounts of time comparable to those in procedures using the new robot (old robot: M = 233 minutes, S.D. = 56; new robot: M = 238 minutes, S.D. = 62) (t(449) = .32, p = .7488). Their patients likewise stayed at Fairtown for comparable recovery periods (old robot: M = 1.51 days, S.D. = .89; new robot: M = 1.45 days, S.D. = .87) (t(449) = .4138, p = .6792).
Case allocations, interview comments, and my statistical analysis indicate that patient risk would likely have increased if complex cases and staff with less robotic skill had not been allocated to the newer robot. And it became particularly clear late in this study that work could not proceed with the older robot without the host of workarounds that experienced talent had developed to address each of the 38 technical problems with the system. Further, these were slowly mastered and enacted by experienced talent alone:
Who can handle that robot, the new guy or the gal you already know who knows how to do it really well? It is true, I can handle room 4 [and the old robot] and so can N, better than, I mean, we can muscle our way through, it is true. (Surgeon)
In contrast to the experienced surgeons and staff members, talent with less robotic experience would likely have failed or taken an unacceptably long time to accomplish the focal surgical acts with the older robot, as they did not have the supplemental mastery of these challenging, interconnected workarounds.
Limited exploration of change
The resourcing patterns identified above drew executives’ focus away from strategy to operations and disproportionately allocated experienced talent to substandard work at the expense of other, potentially more fulfilling and fruitful, allocations. Overall, this valuable but otherwise problematic situation with the older robot would more likely have been seen as threatening if the venting cycle between workers and executives had not limited executives’ focus on it. The development and mastery of workarounds and the venting cycle reduced the perception of threat or failure, which in turn decreased the likelihood of disruptive change to the complex and ostensibly advantageous allocation of resources across Fairtown’s robotic portfolio.
In my presentation of findings to the COO and chief of surgery, it became apparent that they were unaware of most of the empirical detail associated with work involving the older robot. My supplying this detail led them to reassess the costs associated with the status quo:
When I asked for clarification on this last comment, the chief of surgery said he thought the organization was allocating substantial prized resources to an organizational domain such that the hospital yielded a disproportionately low return. The executives then used this robotic example to reflect on the implications for their ongoing management of current resources and processes. Both discussed their shared responsibility for being “thrifty” with their limited budget for 22 ORs and dozens of million-dollar pieces of constantly degrading equipment, each with service contracts, set up more or less well and becoming obsolete as new versions became available:
Thus, these executives anticipated that the challenges of resourcing their technological portfolio extended far beyond robotic surgery and would continue. Both indicated that they believed this challenge was endemic to their organization, given capital constraints and a dynamic market, and that they would have to adjust their management approach to account for this challenge. Critically, these operations-related considerations dominated this and similar conversations. Yet, these were the two individuals who bore primary strategic responsibility for allocating scarce organizational resources to pursue ever-more-valuable opportunities, and this operational focus distracted them from doing so.
Consequences for Talent
Beyond ensuring satisfactory results on Fairtown’s goals, the dynamics of dividing resources, adjusting resources, and making do led to two key outcomes for experienced talent: stress, or a significantly compromised subjective work experience, and increased resilience, or a deepened ability to handle unforeseen surprises.
Stress for experienced talent
Resourcing the technology portfolio compromised the subjective quality of the work experience for the most experienced robotic surgical workers in the organization. These workers were increasingly shunted to operations involving a burgeoning list of nonstandard tasks with no additional time to do them. And while they were able to cope via the workarounds they developed and mastered, doing so was stressful. Stress arose during parts of each procedure with the old robot—parts that staff experienced as relatively relaxed with the newer one. Preparation became a heated affair, straightforward portions of surgeons’ work became tense, and staff became agitated as they prepared to undock and undrape the robot, for example. With the newer unit, these parts of procedures were characterized by chatting, gossiping, joking, discussing other interesting cases, listening to music, and generally building positive relationships and energy for the work. As an experienced surgeon noted, operating with the older robot “does suck the joy right out of doing the work. You need those times in operation where you’re totally relaxed, where you’re kind of enjoying yourself, where you’re kind of having fun.” To the contrary, people suffered emotionally and physically when working with the older robot. A surgeon reflected on this fact after I showed her my list of hassles:
You can’t put a metric on my pain and suffering, you know, the psychological damage it does to me. The inferior quality of visualization, the operating in 2D instead of 3D, the neck strain. I may be able to compensate for all of those things [so] that maybe the case time won’t be longer, blood loss won’t be more, patient outcomes won’t change. Because I have to change my ways to make the shortcomings . . . [irrelevant]. I tend to lose my cool more in [OR]4 [with the old robot], meltdowns are more likely to occur more there. It’s just a very bad place.
The stress was particularly acute for individuals in lower-paid, lower-status roles who were nonetheless among the most talented workers in those roles in the organization. Experienced surgeons at least were choosing to use the “shitty” robot and received significant compensation each time they did so. Scrubs and circulators were not so fortunate. These workers had to set up the older robot in the same time allotted to setup in ideal conditions. The setup task was particularly stressful as it required numerous additional tasks, some of which were preparatory, to offset the significant distance to central supply:
I bring extra everything [to OR4]. With a partial [removal of a kidney tumor] if he says to put in a needle driver to start sewing, and I put it in and the needle driver’s expired, then that’s waiting time, then that’s bleeding, bleeding, so I always bring a needle driver, and an extra scissors, and an extra clip applier, because N is running down there [to OR15], and we’re bleeding, and N is not always good to know where to look for things. (Scrub)
Likewise, many additional tasks were required in the OR itself, such as adding a sterile drape on a monitor attached to the top of the robot tower (approximately six feet from the ground):
As this excerpt illustrates, time pressure and increased complexity translated to rushing the work and occasionally applying excessive force to get it done. Professionals with high standards for their work found this situation very stressful.
As I have already shown, Fairtown’s resourcing patterns also caused stress outside the OR between experienced talent and executives. Engaging in a venting cycle drove each group to harbor anger, mistrust, and condescension toward the other, straining workplace relations. Yet, this stress was never so extreme as to induce a strong perception of threat or changes in resourcing patterns. Thus, these resourcing patterns protected Fairtown’s goals at the expense of experienced talent’s work experience.
Increased resilience for experienced talent
Experienced talent’s mastery of the workarounds with the old robot fostered their resilience to as-yet unexperienced surprises. Everyone who worked with the older robot came to expect new, irritating failures: additional components would fail, there would be more supply troubles, and accumulating damage would create calibration and connectivity problems, for example. But the surprises rapidly became predictable, as everyone knew that this was the “shitty” robot and things would go “sideways” in new ways. This sensitization to surprise enhanced workers’ ability to contend with novel, workable problems the moment they arose, as in this first instance of a new calibration problem:
Developing new workarounds became an increasingly common response to such situations. Surgeons took the lead when they had formal leadership: during the procedure. Support staff led workaround development when they enjoyed such leadership: during preparation and breakdown. Given the distance to and poor communications with central supply, experienced circulators and nurses appropriated a transport cart and stocked it with extra materials required to run a case with the older robot, for example:
We take the old stuff . . . there’s like a different tray of instruments, there’s a different drape pack, you need an extra monitor drape and camera cover, so it’s like four or five things. So we all know that now—it’s all outside of [OR]15 on a rollaway cart type thing, so they [central supply] just roll the cart outside [OR]4. (Scrub)
Thus, the very sources of stress in this work environment also drove the formation of a meta skill: beyond the skill that any particular workaround created and required, these workers’ resilience flowed from their regular experience improvising solutions for new problems. These workers thus built the skill required to develop and test new, useful practices and skill in this life-or-death work.
Given the way that cases and talent were allocated across Fairtown’s two surgical robots, this relatively rare exposure to surprising and trying working conditions disproportionately presented unusual challenges for experienced talent to overcome. Thus, resourcing the portfolio of robots developed deeper resilience to unforeseen challenges but did so preferentially for staff who already had the most capability.
Presentation of Theory Provoked Perceptions of Threat
To assess the validity of my findings, quite close to the end of my study I presented my working theory of the situation to experienced surgical staff as a group. I offered my account of the empirical dynamics surrounding the acquisition and use of the new and old robots, situating this account in an explicit, conceptualized representation of the system for robotic surgery at Fairtown (e.g., matching experienced talent to technical trouble) and substantiating key points with data (e.g., equivalent patient outcomes across the two robots). This account motivated my audiences to significantly reinterpret their experiences. In my first presentation to experienced surgical staff, I asked if I had missed anything or gotten anything wrong. A raft of comments followed, indicating they were now perceiving the old robot as a serious threat:
At some point you have to be a voice for the providers providing for the provided! Someone has finally been able to articulate and present what we have felt for years. Please present this to [chief of surgery] and [COO]. (Surgeon)
The next day, this surgeon sent (and then forwarded to me) an email to the chief of surgery and COO that relied deeply on the theorization and data in my presentation:
[COO]. The time to get rid of the “s” is now. I feel that as the most experienced robotic user I am personally penalized and forced to use the older system more than other providers. . . . I suggest you, [chief of surgery], and any others involved in decision making re the robot acquisition, set up a time to hear Matt Beane’s unbiased results (MIT research) after studying old vs newer robot for the last couple years. Although the data will show similar pt [patient] related outcomes in terms of OR time, blood loss, etc it also presents a convincing case of the extent all OR staff have to go through to make it so. The only reason I get away with the older system is because of prior surgical case experience. This likely is the reason that other surgeons from the other departments refuse to use it. If you or [chief of surgery] wanted me to operate on you, I would tell you to wait for a day when I had the newer robot. Enough is enough. (Surgeon)
Prior to my presentations in 2015, the lack of serious failure, the mastery of workarounds, and the venting cycle greatly limited everyone’s focus on the problem, thus stabilizing operations. My presentations provided substantial empirical detail and a theorized picture of these dynamics and their consequences, thereby disrupting processes that had limited awareness from within. This disruption seemed to contribute to the threat perceptions necessary to motivate change: four months afterward, the older robot was replaced with Intuitive Surgical’s latest model surgical robot, despite the fact that Fairtown saw no marked changes in demand, competitive conditions, or market adjacencies from 2013 through this period.
Discussion
Primary Contribution: Managing Technological Portfolios via Scarce Resources
Whether focused on initial implementation or subsequent adaptation, research on technology and organizing has generally studied only one disruptive technology at a time (Leonardi, 2011; Rahman, 2021; Lebovitz, Lifshitz-Assaf, and Levina, 2022). This research has shown that organizations acquire disruptive technologies, allocate preferred resources to them, quickly settle on new ways of working, and then slowly adapt in efficiency-enhancing ways (Orlikowski, 1996; Anthony, 2021). Fairtown’s use of its first robotic surgical system unfolded according to available theory. Its acquisition of a second, upgraded surgical robot presented a different set of conditions that made an all-in method of resource allocation untenable: newer talent needed to learn in simpler conditions, while experienced talent did not, and the latter could handle more-challenging conditions. I found that under these conditions, initial resource division and subsequent resource adjustment allowed for the basic conditions to achieve results: maintaining surgical outcomes while growing into adjacent, comparable markets and servicing excess demand in preexisting ones. Yet, this resource division and adjustment also created problems—most notably increasing the degradation of prior technology—which were then addressed through making do: workarounds, mastery of those workarounds, and a venting cycle. My primary contribution, summarized in Figure 2, is theory explaining how organizations preserve results given an increasingly heterogeneous technological portfolio.
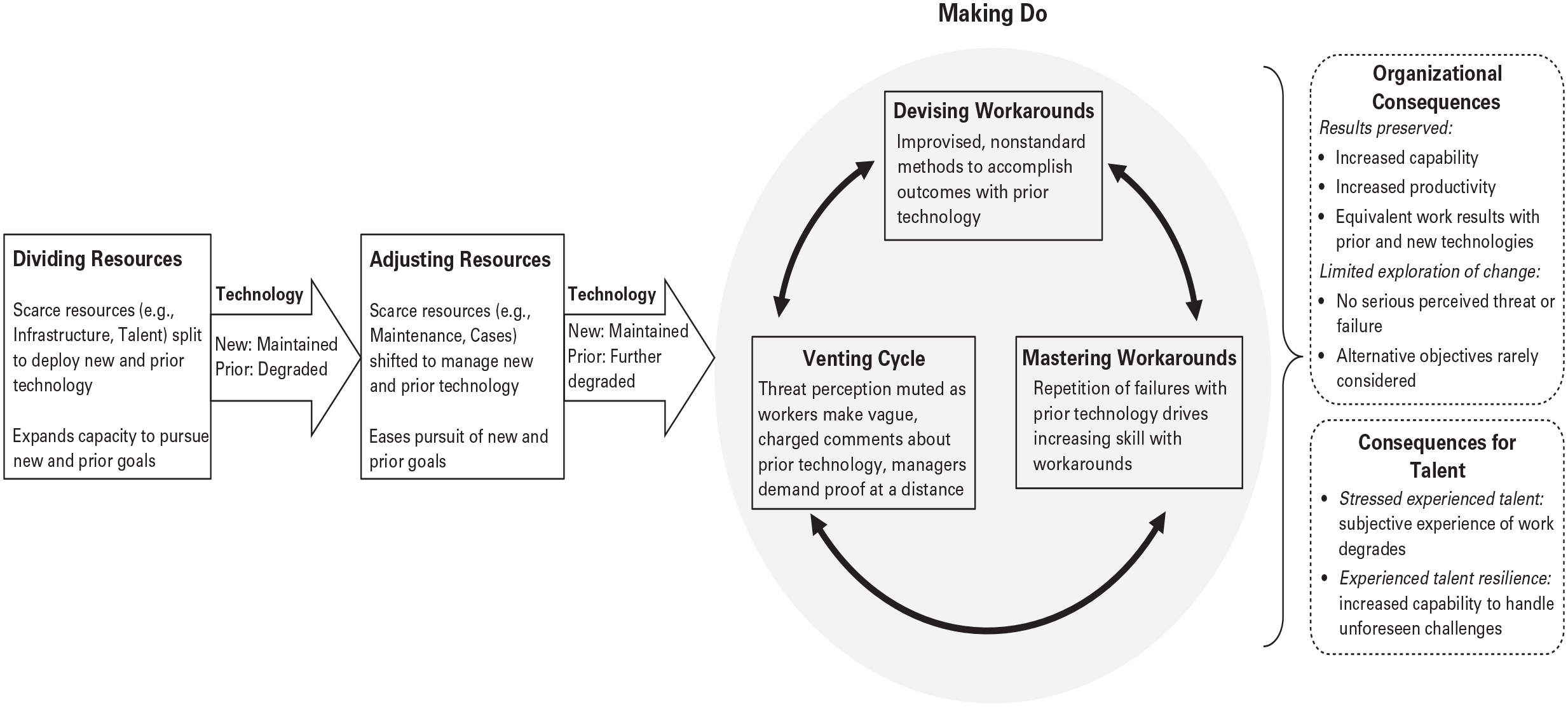
Preserving Outcomes as a Technological Portfolio Becomes More Heterogeneous
More broadly, the literature on technology and organizing has not considered the implications of scarce, fungible resources for technological deployment (Bailey, Leonardi, and Barley, 2012; Shestakofsky, 2017). The theory I present thus contributes to this literature by showing that technology can settle into organizational operations in different ways depending on how resources are allocated to those operations. The uneven, dynamic, and imperfect allocation of key resources across robots in this study suggests that when new versions of a technology are acquired and prior versions are retained, neither will receive the very best resources that the organization can muster. In some cases, this outcome may result in routinization patterns that comport with the literature but with different collateral effects, as in the case of the newer robot creating opportunities for new surgical disciplines to develop capability. In other cases, such as when allocation patterns produce degradation, usage patterns may look less like settling and more like chasing technical and infrastructural problems (Schulman, 1993; Pettersen and Schulman, 2019). Many patterns are possible, such as ones characterized by increasingly diverse maintenance (Henke, 2007; Jacobs and Cairns, 2011) to preserve technological utility. Regardless, taking resource allocation patterns into account promises improved theories regarding the long tail of technology and organizing.
Additional Contribution: Degradation as an Organizational Accomplishment
By showing that the prior robot degraded because it was deprived of infrastructural resources such as space and maintenance, this study shows that technological degradation (Henke, 1999; Cohn, 2016) can be an active organizational accomplishment. Organizations often allocate scarce resources across multiple technologies (Piening, Salge, and Schäfer, 2016; Brasil and Eggers, 2019; Miller and Toh, 2022). This study suggests that even if the technologies are identical upon installation, uneven resource allocation will accelerate degradation of some of them. Further, newer technologies have, by definition, lower return on investment than previously acquired technologies, so firms seeking improvement on this metric may preferentially devote resources to newer instantiations of a given technology, thus degrading the old. These dynamics have implications beyond the problem focused on here. Organizations allocate scarce resources against a host of different, interconnected capabilities—human capital, marketing, research and development, and public relations, for instance—that produce differing value for different stakeholders over varying timescales. No organization has unlimited resources, nor can any perfectly allocate these resources against its capabilities. Thus, while nature has a way of breaking capabilities down, the primary force for decay in organizations may not be entropy. If this study is any guide, we might instead look to conditions such as growth given scarce resources for an explanation.
Relatedly, technology plays a critical role in a broad range of organizational phenomena such as conflict (Hinds and Bailey, 2003), strategy (Kaplan, 2011), cross-occupational collaboration (Barley, 2015), valuation (Orlikowski and Scott, 2014), and innovation (Lifshitz-Assaf, 2018). This study suggests that we could offer more-useful explanations by considering the degradation of technologies that are deeply implicated in the work examined. In many of these studies, for example, limiting resources has been seen as creating constraint that drove workers to create new, valuable options (Kellogg et al., 2021). Yet, as in this study, resource deprivation might also produce more-tangible constraints: the very tool needed to perform critical work can be degraded as infrastructural resources are directed elsewhere, making the work more challenging as time goes on. This study thus raises new questions about how technological degradation is implicated in organizational processes of interest.
Additional Contribution: Making More of Making Do
Finally, this study contributes by offering an enriched account of how workers proceed despite irritants and inadequacy in their work (Weick, 1979; Orlikowski, 1996; Sarasvathy, 2001; Christiansen et al., 2009). First, though a range of literatures has shown that figuring out how to “muddle through” (Lindblom, 1959: 79) takes time and effort (Baker and Nelson, 2005; Koppel et al., 2008; Azad and King, 2012), they have not conceived of workers as developing skill in the process. Indeed, prior work has shown organizations failing to learn from workarounds that nonetheless sustain critical outcomes (Tucker and Edmondson, 2003). Yet, in this case workers had to develop significant skill with their invented techniques to operate effectively with the “shitty” robot. This study therefore suggests that individuals will build skill to the extent that they repeatedly make do in similar ways. The literature on skill has quite a bit to say on the implications: skill with making do will likely accrue at predictable rates (Darr, Argote, and Epple, 1995), maintaining it will take practice at regular intervals (Bailey, 1989), workers will build such skill vicariously as they support work from the periphery (Hutchins, 1995), and such skill may be transferrable to other contexts (Soderstrom and Bjork, 2015), for example.
This study also helps us see that making do can provide sustainable results but that considerable work may be needed to render it tolerable. While scholars have long been aware of various forms of making do, such as workarounds (Tucker, 2016), these have been treated as practically invisible, given management inattention or employees hiding it (Bernstein, 2012). This study provides an alternative view: workers can chafe against conditions that drive them to rely on well-honed workarounds to get results. But this situation can persist for quite some time because venting cycles mute concern from within and inquiry from without. Further, this pattern of griping and sniping may come at the cost of strained management–worker relations. Making do is common, and skill is intimately bound up with outcomes, so these contributions should allow for new analysis of a range of organizational phenomena.
Limitations and Generalizability
Most organizations manage increasingly heterogeneous technological portfolios. But the applicability of this study’s theory to these situations will vary. The technology in this study was expensive to acquire and maintain, was shared by multiple users, required significant training and organizational infrastructure to use, and had the potential for valuable use in various adjacent yet comparable markets. Furthermore, the work itself was routinized and collaborative, guided by strong norms in a highly institutionalized context, and led by high-status actors in a space not readily observable by outsiders. Additionally, the portfolio heterogeneity in focus here was related to the addition of new versions of prior, familiar technology. And, finally, the resource allocation gaps here led to slow degradation of prior technology. These characteristics will differ in many other settings but seem evident in large-scale computing, warfare, litigation, semiconductor manufacture, and filmmaking, so these findings seem most likely to resonate in these and comparable contexts.
There is good reason to believe that these findings may apply to organizations in a broader set of contexts, however. In settings with less technological diversity than in this study—in which organizations routinely buy numerous instances of the same version of a technology, for example—organizations may avoid many of the challenges described in this article. Yet, it seems quite unlikely that these organizations equally resource all of these ostensibly identical tools; some problems will be more valuable than others, for instance, drawing more-generous allocations of infrastructure and talent to support them. Similar problems may also emerge as organizations manage technological portfolios with far greater diversity. Fairtown’s executives aptly noted that they struggled to allocate scarce resources not only to different versions of the same robot but across dozens of radically different technologies, ranging from multimillion-dollar MRI machines to $10,000 endoscopes, each core to the work of different occupational subgroups, each replaced and maintained with different frequencies. This study suggests that organizations will degrade some technology in the pursuit of goals such as growth; will allocate infrastructure, talent, maintenance, and cases to adjust; and will rely on experts to make do with the result.
Practical Implications
While the dynamics outlined in this article may seem painful and wasteful up close, wise managers may sometimes allow them to persist. From one point of view, allocating ever more experienced surgical talent to work with the older robot while decreasing related maintenance seems like the worst of all possible scenarios for robotic surgery at Fairtown. Yet, this approach preserved client outcomes, boosted financial return, allowed for expansion into current and adjacent markets, and powerfully extended organizational resilience (Williams et al., 2017) by ensuring that someone, somewhere, could handle exceptions that a dynamic world presents. It is also possible that leaving these dynamics intact allowed for far more advantageous allocation of surplus resources related to other departments or technologies at Fairtown. My intervention disrupted these dynamics and may therefore have been the organizational equivalent of killing the goose that was laying a pareto-optimal egg. By seeking out and quashing these dynamics, managers may sometimes do the same. Further, organizations may lose critical flexibility as workers and management become more crisply aware of the extensive work being done to prop up a technological portfolio: experienced talent may be far less willing to engage in a regular, awkward dance with degrading tools to extract a return for the firm, for example.
That said, we can clearly let the challenges associated with technological portfolios go too far. Absent my intervention, Fairtown may have retained the “shitty” robot for quite some time, barring many other more-fruitful allocations of scarce organizational resources. The trouble and workarounds required to extract satisfactory value out of previously acquired technologies may be invisible to managers yet hedge against undesirable outcomes. Managers will thus keep problematic technologies in service longer than is wise and miss the significant drain on scarce organizational resources and opportunities. Organizations reap disproportionate returns to superstar talent, for example (Rosen, 1981). Typical approaches to technological portfolios may significantly limit these returns and make it quite difficult to perceive that fact. This study shows one way that managers can assess the costs and benefits of these dynamics: pay the work a visit. When given specific examples of technical trouble and workarounds with the older robot, Fairtown’s COO and chief of surgery decided that things had gone too far. They, and many managers like them, could have gotten this information for themselves by attending one or two procedures involving the technology that their experienced talent was griping about.
Finally, and more broadly, we focus a great deal on novel technologies and related discontinuities, and this study suggests casting our gaze back to the mundane and the incremental. We must of course understand the dramatic, as it can have dramatic effects. But this leaves the subtle bulk of our experience with technology in organizations to surprise us. While perhaps more difficult to observe, dynamics such as those associated with managing a technological portfolio can be quite durable and can determine long-run organizational behavior and outcomes that managers, experts, and customers value. Noticing such dynamics may become ever more important as we develop and deploy technologies that learn from experience, especially as these technologies become connected and can learn from one another. Thus, it may be that incremental adaptation to—and not rapid transformation from—these incrementally self-modifying technologies will take us by surprise unless we develop theories to account for processes that humans are not well attuned to perceive and understand.
Footnotes
Acknowledgements
I am deeply grateful to my research informants for so openly contributing data to this study. Also, I offer my sincere thanks to those who helped with this manuscript: first and foremost to Mike Pratt and three anonymous reviewers but also to my dissertation committee—Wanda Orlikowski, Kate Kellogg, and John Van Maanen. Likewise, I am grateful to Leslie Perlow and the members of her seminar on the Craft of Qualitative, Inductive Research, Curtis Chan, Julia DiBenigno, Arvind Karunakaran, Steve Barley, Mary Tripsas, and the members of UC Santa Barbara’s Technology and Organizing Research Seminar.
1
The hospital’s name and other key details have been obscured to preserve subjects’ anonymity.
3
Recent work (e.g., Feldman, 2004; Dutton et al., 2006; Quinn and Worline, 2008) fruitfully treats all resources as produced in practice. On this view, resources are not fixed or scarce in and of themselves, and creation of resources (e.g., argumentation, social networks) is as salient a part of the resourcing process as allocation is. In my context, it was the significant, periodic allocation of a few relatively fungible, at least temporarily scarce resources (e.g., capital, talent) that put key dynamics in motion and led to key consequences, so I adopted a more traditional view of resources in this article for analytical purposes.