
Abstract
Organizational life is rife with conflict between groups that pursue different goals, particularly when groups have strong commitments to professional identities developed outside the organization. I use data from a 30-month comparative ethnographic field study of four U.S. Army combat brigades to examine conflict between commanders who had a goal of fielding a mission-ready force and mental health providers who had a goal of providing rehabilitative mental health care to soldiers. All commanders and providers faced goal and identity conflict and had access to similar integrative mechanisms. Yet only those associated with two brigades addressed these conflicts in ways that accomplished the army’s superordinate goal of having both mission-ready and mentally healthy soldiers. Both successful brigades used what I call “anchored personalization” practices, which included developing personalized relations across groups, anchoring members in their home group identity, and co-constructing integrative solutions to conflict. These practices were supported by an organizational structure in which professionals were assigned to work with specific members of the other group, while remaining embedded within their home group. In contrast, an organizational structure promoting only anchoring in one’s home group identity led to failure when each group pursued its own goals at the expense of the other group’s goals. A structure promoting only personalization across groups without anchoring in one’s home group identity led to failure from cooptation by the dominant group. This study contributes to our understanding of how groups with strong professional identities can work together in service of their organization’s superordinate goals when traditional mechanisms fail.
Keywords
Organizations are rife with conflict between groups, such as labor versus management, physicians versus hospital administrators, and engineering versus marketing departments (e.g., Pondy, 1967). Such conflict is woven into the fabric of organizational life through the division of labor (Durkheim, 1893; March and Simon, 1958; Strauss et al., 1963). Members of specialized departments and subunits develop their own interests and often pursue goals that conflict with those of other groups and may even be at odds with the overall goals of the organization (e.g., Cyert and March, 1963). Because groups are entrenched in their own points of view, they often have difficulty appreciating the perspective of other groups in the organization (e.g., Dearborn and Simon, 1958; Dess, 1987; Parker and Axtell, 2001), so integration or “unity of effort” across groups is an ongoing achievement (Lawrence and Lorsch, 1967a; Bechky, 2011). Understanding how and when organizations can productively manage these goal conflicts is a central pursuit of administrative science.
Multiple streams of literature have described how goal conflicts can be managed, including foundational literature on the behavioral theory of the firm (e.g., Simon, 1947; Cyert and March, 1963) and scholarship on mechanisms that promote integration across different subunits to achieve superordinate organizational goals (e.g., Galbraith, 1984; Pinto, Pinto, and Prescott, 1993; Okhuysen and Bechky, 2009). Yet many group conflicts have proven immune to these mechanisms (e.g., O’Connor, Fiol, and Guthrie, 2006; Jarzabkowski and Balogun, 2009), perhaps because existing scholarship has not considered how deeply held differences in professional identities between members of different subunits, often developed outside the organization, may make these intraorganizational mechanisms ineffective.
Identity research suggests that differences between organizational groups can be reconciled by promoting a superordinate identification with the organization (e.g., Dutton, Dukerich, and Harquail, 1994; Elsbach, 1999; Besharov, 2014), but this approach may fail when subunit members are committed to professional identities and perspectives developed outside organizational boundaries through professional training and socialization (Van Maanen and Barley, 1982; Battilana and Dorado, 2010; Turco, 2012). Addressing underlying professional identity differences that often shape subunit perspectives is critical for goal alignment. When identity is implicated in a conflict, conflict can become personal or intractable, such that it is no longer about the rational pursuit of different goals but is seen as a personal affront to who one is (e.g., Fiol, Pratt, and O’Connor, 2009), leading to stereotyping across groups and other cognitive distortions that impede cooperation (e.g., Friedman and Davidson, 1999).
I focus on how and when subunits comprising professional groups with differing identities can develop integrative solutions to goal conflict. I examine how an organizational structure and set of practices can facilitate goal alignment by helping professional groups overcome identity differences without becoming coopted by personalized contact with the other group. I draw on data from a comparative ethnographic field study of four U.S. Army combat brigades in which there was conflict between commanders privileging the goal of fielding a mission-ready force and mental health providers privileging the goal of providing rehabilitative mental health care to active-duty soldiers with conditions such as posttraumatic stress disorder. Even though the U.S. Army desired both goals, and ultimately a mentally healthy soldier was in the interest of both groups, commanders and providers had to overcome professional identity differences to align their goals and accomplish both mission readiness and soldier rehabilitation.
Goal Conflict in Organizations
The Carnegie School has long argued that organizations comprise coalitions with different interests that often pursue different goals (March, 1962; for reviews, see Argote and Greve, 2007; Gavetti, Levinthal, and Ocasio, 2007; Gavetti et al., 2012). Even though integrative, overarching organizational goals exist (e.g., Simon, 1964; Warner and Havens, 1968), different groups have difficulty achieving them due to entrenchment in their own perspectives and interests that stem from their distinct positions in the organizational structure and immersion in separate cognitive communities (e.g., March and Simon, 1958; Porac, Thomas, and Baden-Fuller, 1989; Dougherty, 1992; Joseph and Ocasio, 2012; Nigam, Huising, and Golden, 2016). Such differences can lead to regular conflict between groups and suboptimal outcomes for the organization (e.g., Cyert and March, 1963; Bechky, 2003; Truelove and Kellogg, 2016).
Two streams of literature have examined how such goal conflict can be managed. The first shows that conflicts between organizational coalitions are in a constant state of quasi-resolution, managed through mechanisms such as sequential attention to goals (e.g., Greve, 2008), organizational slack, inducements such as incentives or policy prescriptions (e.g., Cyert and March, 1963), political bargaining (Kaplan, 2008), the spatial and temporal differentiation of goals, goal myopia (Ethiraj and Levinthal, 2009), organizational socialization (Simon, 1947; March and Simon, 1958), and hierarchy in which the more powerful group holds ultimate decision rights (Perrow, 1961; Cyert and March, 1963; Fligstein, 1987).
A second stream of scholarship demonstrates that a host of integrative mechanisms can help align the goals of different groups in an organization, primarily by providing exposure to the other group’s perspective, formalizing interaction practices, and increasing incentives to cooperate. Such mechanisms include formal procedures for interaction (e.g., March and Simon, 1958), cross-functional groupings (e.g., Pinto, Pinto, and Prescott, 1993; Turkulainen and Ketokivi, 2012), collaborative incentives (Kretschmer and Puranam, 2008), integrator roles (Lawrence and Lorsch, 1967b; Levina and Vaast, 2005), inclusive strategic planning (Ketokivi and Castañer, 2004), and integrative organizational designs such as co-location or matrix structures (e.g., Lawrence and Lorsch, 1967a; Mintzberg, 1979, 1993; Van den Bulte and Moenaert, 1998). But these mechanisms may not always work because they often do not effectively address fundamental differences in professional identities between members of different subunits, which can be central drivers of behavior (e.g., Anteby, 2008a, 2008b; Ashforth, Harrison, and Corley, 2008; Petriglieri, 2015). Professional identity often transcends the boundary of the organization, making it difficult to control with intraorganizational integration mechanisms like organizational socialization. Given the increase in professional and occupational groups working inside organizations (e.g., Gorman and Sandefur, 2011) and the rising salience of professional (or occupational) identity resulting from increased interorganizational mobility (e.g., Bidwell and Briscoe, 2010; Anteby, Chan, and DiBenigno, 2016), we must understand how groups with goal conflict stemming from strong commitments to their professional identities can achieve organizational goals.
Professional Identity, Personalization, and Organizational Structure
Professional groups are unique in that their identities—the beliefs, values, and definitions of who they are and what it means to be a good group member (e.g., Ashforth, Harrison, and Corley, 2008; Bartel, Blader, and Wrzesniewski, 2012; Ramarajan, 2014)—are deeply entwined with what they do (e.g., Kreiner, Hollensbe, and Sheep, 2006; Pratt, Rockmann, and Kaufmann, 2006; Lepisto, Crosina, and Pratt, 2015; Howard-Grenville et al., 2017). These identities are enacted and often evident through group differences in language, demeanor, and even dress (Pratt and Rafaeli, 1997; Perlow and Weeks, 2002; Ashforth, Rogers, and Corley, 2011). Members of professional groups are often strongly committed to pursuing goals and advancing perspectives that align with their professional identities (e.g., Abbott, 1988; Ranganathan, 2013; Huising, 2014; Kellogg, 2014; Almandoz and Tilcsik, 2016). Traditional integration efforts to socialize subunit members to support the organization’s superordinate goals and promote a superordinate organizational identification may fail because professional group members may identify more strongly with their profession than their organization, given years of professional socialization and training (Gouldner, 1957; Merton, 1957; Van Maanen and Barley, 1982; Barley and Tolbert, 1991; Pratt and Foreman, 2000; Turco, 2012). Because organizations have multiple goals that are often hard to accomplish simultaneously, shared membership in the organizational collective and efforts to promote superordinate organizational identification may prove fruitless if professional groups focus on the parts of the superordinate goal that align best with their extra-organizational professional identity and values. For example, Battilana and Dorado (2010) studied a failed microfinance firm with the superordinate goal of both making a profit and improving the social welfare of its clientele. They showed that the firm’s failure resulted from the strong extra-organizational professional identity commitments of those they hired—finance and social work professionals—who each privileged the part of the organization’s goal that aligned with their professional identity.
While scholars of professions have highlighted how professional identity is deeply entwined with professionals’ work, scholars of identity have highlighted how conflict may become personal and intractable when group-based identities are involved. Intractable identity conflict between groups is evident when groups use simplifying stereotypes of one another, believe that a gain for one group is a loss for the other, and engage in “dis-identification” by defining themselves, in part, by their differences with the other group (for reviews see Fiol, Pratt, and O’Connor, 2009; Rothman, 1997; Dukerich, Kramer, and Parks, 1998; Rouhana and Bar-Tal, 1998; Coleman, 2003; Petriglieri, 2011). Such processes can lead to cognitive distortions across groups in their interpretations of one another’s behavior and intentions, limiting both their ability to accurately perceive and comprehend the perspective of the other group and their motivation to engage constructively with one another (Tajfel and Turner, 1979; Northrup, 1989; Friedman and Davidson, 1999). For example, O’Connor, Fiol, and Guthrie (2006) showed that inviting administrator and physician groups with different goals (managing an efficiently run hospital and providing quality care) to a strategic planning retreat without addressing their longstanding identity conflict—physicians stereotyped administrators as concerned only with their careers and cost-cutting, and administrators stereotyped physicians as out of touch with the realities of running a hospital—backfired and further fueled conflict between them, as both groups continued to stereotype one another and view gains for one group as losses for the other.
When traditional approaches to solving such conflicts are ineffectual, an alternative approach that I call “anchored personalization” may hold promise. The intergroup relations literature has advanced the concept of personalization, which is distinct from mere contact (Allport, 1954) and involves regular, personalized interaction with a member of another group that results in familiarity with and knowledge about that person as an individual, rather than as a stereotypical member of an outgroup (Brewer and Miller, 1984, 1988; Hewstone, 1996; Okhuysen, 2001; Miller, 2002; Hinds and Cramton, 2013). In situations of racial or ethnic group differences, personalization has been found to reduce intergroup stereotyping and lead to increased perspective-taking (Ensari and Miller, 2006) from increased liking and the discovery of similarities that can reduce outgroup categorizations and prejudices (Ensari et al., 2012).
Personalization depends on opportunities for regular contact across groups, which may or may not occur organically. Organizations can design jobs and structures to foster personalization, but previous scholarship has not examined how particular structures might support it, likely because most research on personalization either has been conducted on ethnic or racial groups rather than on professional groups in organizations or has been conducted in laboratory rather than organizational settings. In addition, existing scholarship on personalization has primarily explored its positive benefits, but personalized relations in organizations may lead to negative outcomes through cooptation, such as loan officers becoming too close to their clients and making deals that are bad for the bank (Canales, 2013) or diplomats privileging their host countries’ interests by going native (e.g., Jenoff, 2011).
Organizational structures can both enable and constrain the quality and type of interactions members have with each other (McPherson and Smith-Lovin, 1987; Blau, 1994; Sorenson and Stuart, 2001; Chown and Liu, 2015), but we do not know which structures might promote the benefits of personalization to neutralize identity conflict between groups and prevent cooptation. In the study presented here, I examine the effects of different organizational structures and the processes they enabled on the resolution of conflicts between professional groups.
Methods
Context
I conducted a 30-month ethnographic field study from 2012 to 2015 of goal conflict between two professional groups—U.S. Army commanders and mental health professionals that focused on different parts of their organization’s overarching goal to have both mentally healthy and mission-ready soldiers. I employed an inductive approach to build new theory by examining variation across multiple matched cases (Eisenhardt, Graebner, and Sonenshein, 2016).
Over the last decade, soldiers’ mental health problems have increased dramatically in the U.S. Army—notably posttraumatic stress disorder (PTSD) and suicide (Ramsawh et al., 2014). The U.S. wars in Iraq and Afghanistan were unique in that the military relied on an all-volunteer force without resorting to a draft, despite severe shortages of soldiers (Korb and Duggan, 2007). As a result, soldiers deployed more often than in the past and for longer periods of time with less time for rest and recovery in between (De Angelis and Segal, 2009; Bolger, 2010). In some cases, soldiers had as many as six or seven deployments. The psychological tolls of these wars (e.g., de Rond and Lok, 2016) began to receive widespread attention in 2007 after the publication of studies noting an increase in soldier suicides and mental health conditions (U.S. Department of Defense Taskforce on Mental Health, 2007; Tanielian and Jaycox, 2008).
In response, the U.S. Congress allocated billions of dollars to improve mental health services for soldiers, and the army hired hundreds of mental health professionals to provide more extensive rehabilitative care services. While mental health problems were previously treated as a “career ender,” these “invisible wounds” of mental illness would now be treated the same as physical injuries, allowing soldiers to remain on active duty in their units and keep their jobs while recovering (U.S. Department of Defense, 2014; Hoge et al., 2015). I observed that two professional groups—commanders and mental health providers—directly affected whether active-duty soldiers benefited from using these services. While mental health providers were tasked with providing mental health care services to soldiers, soldiers’ subunit commanders had an enormous impact on whether they benefited from these services. Commanders had discretion over whether to comply with duty-limiting treatment recommendations made by mental health providers regarding soldiers’ recoveries, such as whether to deploy soldiers, take them on training exercises, and comply with workload or schedule reductions. When soldiers used mental health services, they missed work during the day to attend appointments or were sometimes given duty-limiting work restrictions by their providers that “took them out of the fight,” making it more challenging for commanders to meet their targets for fielding a mission-ready force. When subunit commanders overrode the recommendations of mental health professionals, it could limit the effectiveness of a soldier’s rehabilitation. This situation created high levels of conflict between commanders and mental health providers.
Data Collection
I spent the first 12 months of data collection on an interdisciplinary team studying the U.S. Army’s mental health system where I served as a note taker or co-interviewer for 132 interviews, 46 focus groups, and dozens of informal meetings with a wide range of mental health and army stakeholders at seven army posts (Srinivasan, Carroll, and DiBenigno, 2016). This first year taught me to “speak Army” and develop my ability to converse with commanders and soldiers, as well as with mental health professionals. I spent the remaining 18 months conducting my own study to uncover mechanisms accounting for differences in how providers and commanders worked together (or not) toward the organization’s superordinate goal of having mentally healthy and mission-ready soldiers. I used a relational ethnographic approach (Desmond, 2014), studying the relations between groups that were mutually dependent on and in conflict with one another: subunit commanders and outpatient mental health professionals.
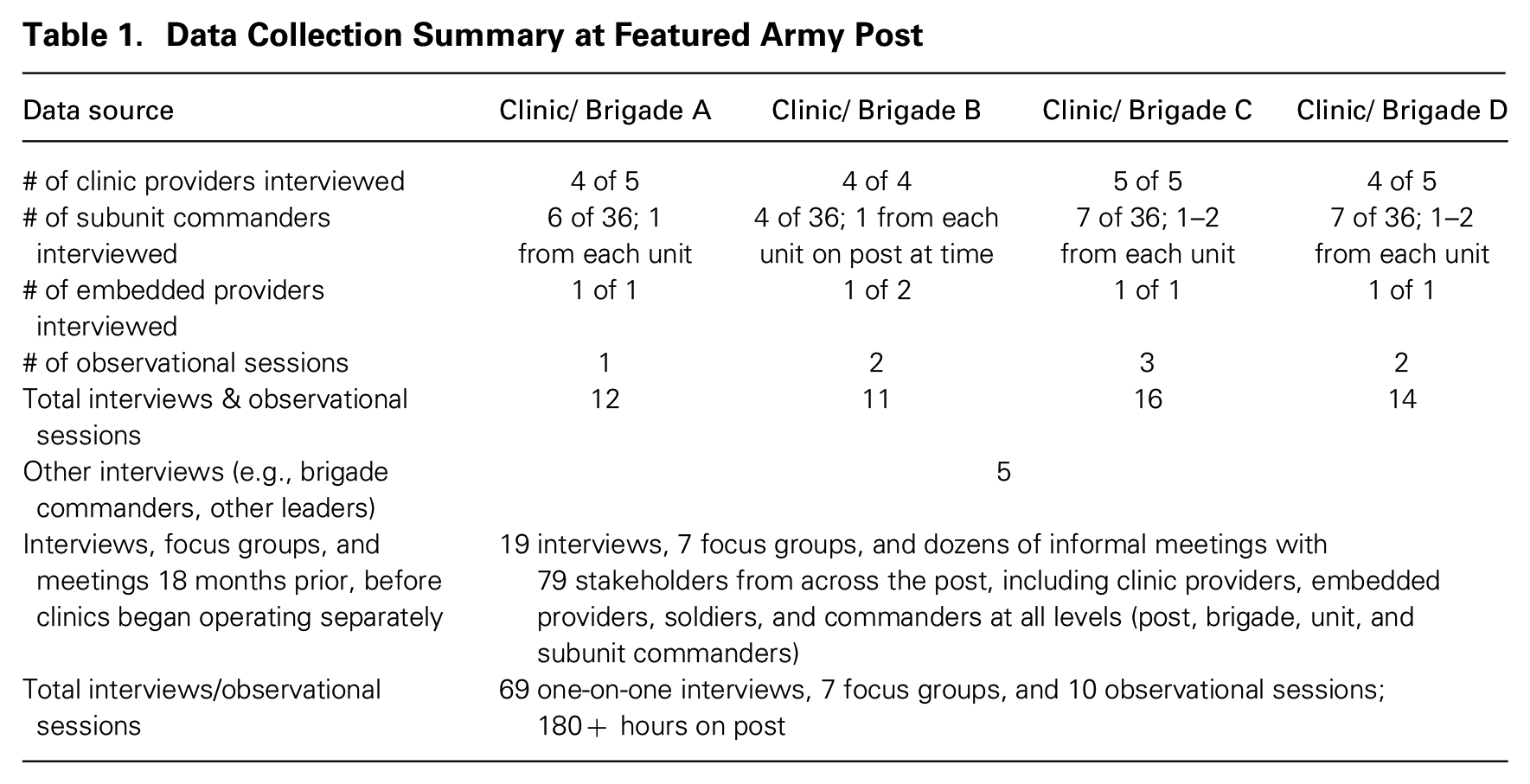
Data for this paper come primarily from one U.S. Army post where I spent over 180 hours on site and conducted 69 interviews, 14 focus groups, and ten observational sessions, in addition to dozens of informal interviews, observations, and attendance at social events. At this post, I selected four (out of six) mental health clinics to study (Clinics A, B, C, and D) because they were similar on most dimensions. Each clinic served combat brigades of approximately 3,600 soldiers in the same division, which reported to the same division commander, and was co-located near the brigade it served. Each brigade was divided into units of approximately 600 soldiers (“battalions,” referred to as “units”), further divided into subunits of approximately 100 soldiers (“companies,” referred to as “subunits"), and structured similarly in terms of the types of soldiers’ occupational specialties in each unit and subunit (e.g., infantry, cavalry, etc.). All brigades had returned from deployment/field within the last year with similar levels of combat exposure. Providers at the four clinics reported to the head of mental health for the post, were evaluated by professional colleagues of the same discipline, and were expected to see about six patients a day. Clinics A, C, and D had five providers, and Clinic B had four. All had access to the same integrative mechanisms to align their goals with those of the commanders in the brigades served (e.g., the same access to cross-functional team meetings, etc.).
When I first traveled to this post during my first month of fieldwork as part of the interdisciplinary team, it was transitioning from housing all mental health providers together in one hospital to co-locating providers in smaller freestanding clinics supporting each brigade. Relations between mental health providers and subunit commanders were poor at the time, and commanders were resistant to providers’ duty-limiting treatment recommendations for soldiers. When I returned to this post to conduct my own study, I was surprised to find that subunit commanders and providers associated with two of the four brigades were engaging in constructive ways that benefited both patient care and mission readiness. I spent the remainder of my time at this post interviewing and observing these providers and commanders to understand how and why some clinics and brigades were achieving better outcomes than others.
My sampling strategy was to interview the majority of mental health providers in each of the four clinics and a representative sample of subunit commanders they engaged with: at least one subunit commander from each of the six units in each brigade. 1 I also interviewed other key stakeholders, including embedded providers assigned to each brigade, higher-level commanders, chaplains, and mental health leaders who oversaw the entire post. Interviews were semi-structured and lasted between one and three hours, with most lasting an hour. When given permission, I recorded and transcribed interviews; otherwise I took extensive notes. I could then triangulate interviews to corroborate different points of view within clinics and brigades. A summary of my data collection at this post is reported in table 1.
Data Collection Summary at Featured Army Post
Inductive Data Analysis
My inductive analysis (Glaser and Strauss, 1967; Strauss and Corbin, 1990) consisted of reading my field and interview notes multiple times, writing analytical memos, and tracking patterned activities and issues related to goal alignment between providers and commanders over time. Analysis occurred in three phases. Phase one analysis of interview transcripts and field notes occurred during my preliminary year of fieldwork. It revealed a pervasive theme of conflict between outpatient (clinic) mental health providers and subunit commanders that negatively affected soldiers’ ability to benefit from the treatment recommendations providers made for them, despite explicit efforts by army and medical leadership to adopt the superordinate goal of having both mentally healthy and mission-ready soldiers. As the army experimented with different care delivery models (described below), I observed variation in relations and outcomes achieved by providers and subunit commanders. I then conducted an in-depth analysis of my data from the post featured in this paper, because it provided the best comparison opportunity to uncover mechanisms promoting intergroup goal alignment, as the clinics and brigades on this post were so similar.
In the second phase of analysis, I coded all provider and subunit commander interview and observational data first by individual and then (when possible) by commander–provider dyad. During this process, the theme of professional identity differences emerged as a source of conflict between providers and commanders. I then read the literature on identity conflicts and coded my data using theoretical codes for indicators of intractable identity conflict (e.g., stereotyping, dis-identification, and zero-sum conceptualization). I next coded instances of provider and commander conflict situations in which the goal pursued by one group was perceived to conflict with that of the other group.
I then analyzed 132 of these situations for which I had sufficient data on the conflict, how it was handled, and the outcomes associated with it. I found that in Clinics C and D, the majority (89 percent of 70 conflicts) were resolved in ways that resulted in integrative outcomes that were good for both patient rehabilitation and mission readiness, but very few resulted in integrative outcomes in Clinics A or B (5 percent of 62 conflicts). I then compared how providers and commanders across these brigades resolved similar types of conflicts, as well as the outcomes of each conflict. I did this by writing a summary of each conflict, triangulating accounts from providers, their clinic colleagues, and commanders involved in the same conflicts when possible to create a holistic account of each situation, providers’ and commanders’ responses to it, and its outcome.
In the third phase of analysis, I sought to understand why and how providers and commanders in Clinics C and D were achieving dramatically better outcomes than those in Clinics A and B. I examined how each clinic was organized and the experiences of providers and commanders over time. I then contrasted these cases to identify organizational structures and practices associated with these outcomes. The main difference between these clinics and the brigades they served was a subtle difference in the clinics’ organizational role assignment structure that was not explicitly recognized by army leadership as noteworthy. I coded my data to identify three main practices associated with working in this structure that were used by the vast majority of providers and commanders. In my final phase of analysis, I shared my interpretations with key informants and assessed whether the mechanisms and associated outcomes identified at this post held at the other posts I studied.
Findings
Professional Group Conflict around the Superordinate Organizational Goal
Since 2007, the U.S. government and top U.S. Army leadership have dedicated unprecedented resources to improving army mental health care services, which were viewed as an important complement to the army’s core mission to “fight and win our nation’s wars” and as a major component of the army’s “Ready and Resilient” campaign to promote not only physical readiness for war but also mental readiness and resilience (United States Army, 2013). 2 In my interviews and observations, the majority of the army’s organizational leaders, defined as “field-grade” commanders (above the level of subunit commanders), indicated they supported soldiers using mental health services and reported that a mentally healthy soldier was in everyone’s best interest. But I observed variation in levels of such support among the subunit commanders below them who were directly accountable for fielding a mission-ready subunit. I refer to subunit commanders as simply “commanders” here.
Commanders and mental health providers, as members of two distinct groups in the army’s division of labor, regularly experienced conflict over how to accomplish the army’s superordinate goal. Commanders privileged one part of this goal, fielding a mission-ready force, while providers privileged the other part, ensuring mentally healthy soldiers. Conflicts emerged in three main areas: (1) prioritizing subunits’ welfare vs. individual soldiers’ welfare; (2) sharing vs. protecting soldiers’ health information; and (3) instilling mental toughness vs. reducing the stigma of seeking help.
Prioritizing subunits’ vs. individual soldiers’ welfare
From the commander’s perspective, the needs of the subunit and mission came before the needs of any one individual soldier. Commanders were regularly assessed on whether their subunits were typically at least 90 percent deployable and 85 percent trained on “mission-essential” tasks. But providers’ treatment recommendations sometimes took soldiers “out of the fight,” causing them to miss work to attend appointments or limiting what they did at work. One commander noted, “Every time I lose a soldier to Mental Health, it degrades our troops’ ability to accomplish our mission.”
In contrast, mental health providers were concerned with doing what they considered right for their individual patients’ recoveries, regardless of the impact on the larger subunits to which these soldiers belonged. Providers worried that patients’ participation in training exercises might aggravate their mental health conditions or put them at risk of harming themselves or others, and they privileged the long-term health of their patients over the short-term needs of commanders to field a mission-ready subunit. One provider explained, “That’s my goal right now, rehabilitation. And even if I can’t get him back to duty, it’s also about helping someone become a good human being when they go back to society.”
Commanders had discretion over whether to comply with providers’ recommendations that limited what soldiers could do at work, which affected whether providers’ patients could benefit from treatment. These differences in prioritization of goals created conflict when commanders challenged or overrode providers’ recommendations that they perceived to negatively affect their subunits’ mission readiness.
Sharing vs. protecting soldiers’ health information
Providers and commanders also experienced conflict over their differing perspectives on the appropriateness of discussing a soldier’s mental health treatment progress and status. Commanders said they needed as much information as possible to make informed decisions about their subunits’ missions (e.g., Can this soldier deploy? Lead others? Manage sensitive intelligence? Operate expensive equipment?), but mental health professionals were trained to protect patients’ privacy and adhere to Health Insurance Portability and Accountability Act (HIPAA) laws. Providers reported that protecting patients’ privacy was also critical for maintaining a therapeutic relationship so patients felt comfortable sharing traumatic experiences. One provider related, “Command wants to know everything. But we were trained to protect patient confidentiality, otherwise patients won’t trust us and they won’t come. . . . So a lot of conflict emerges.” In contrast, commanders were trained to “know their soldiers” and have “situational awareness” on all aspects of their soldiers’ lives, including their health problems, and the army has rules that formally limit soldiers’ privacy. Under the Privacy Act in the Uniform Code of Military Justice, soldiers waive the right to the same medical privacy protections enjoyed by civilians. Army medical professionals can share information about soldiers’ mental health conditions with their commanders if the soldiers are considered at risk of harming themselves or others or if the soldiers’ conditions might affect the mission. But all providers reported that knowing whether a soldier’s condition affected the mission was a gray area. These different perspectives led to conflict, with commanders regularly “pushing” providers to share information, and providers ignoring or rebuffing these commanders (e.g., by not returning their calls). One commander explained this frustration:
If the soldier goes to (Mental Health) every week and I don’t know when I take him to combat that he has issues and is on all these crazy pills, he could seem good to go, but is having dreams of killing people and now he’s in combat and this comes out. We find out the information too late. They [providers] will say, “Well because of HIPPA and the soldier has rights.” But a soldier has no rights to me. We need to know.
Instilling mental toughness and self-reliance vs. reducing the stigma of seeking help
Commanders were responsible for training their soldiers to be physically and mentally prepared for combat. They emphasized mental toughness and self-reliance, and they trained soldiers to “push through” pain and fear and “suck it up and drive on” to develop the capacity to handle difficult situations. This directly conflicted with mental health providers’ goal of reducing the stigma around seeking help, which meant encouraging soldiers and commanders to acknowledge pain and fear and get professional help. One commander said:
We are becoming a “kinder and gentler army,” but our enemy, like ISIS [Islamic State of Iraq and Syria], hasn’t become any kinder or gentler. Do you think ISIS fighters go to Mental Health? . . . I have guys who tried to save a friend who was ripped in half and they had to just keep charging on anyway. It is necessary to do the job, to keep going. If we were all getting help, we would be dysfunctional.
Conflict over these different perspectives was especially salient regarding the mental health care of leaders such as commanders and senior sergeants. Mental Health was positioned as a service for soldiers, not leaders. Providers often pursued strategies to reduce the stigma of seeking care that commanders perceived undermined their image as exemplifying mental toughness, such as insisting that leaders sit in the waiting room with junior enlisted soldiers. One provider explained, “Nothing is more powerful than a junior soldier seeing a leader in the waiting room. We talk about breaking the stigma. That’s what it looks like.”
Identity Differences between Professional Groups
Goal conflict between providers and commanders was exacerbated by and rooted in their differing professional identities, which were evident in their differing self-definitions, values, professional training, common demographic profile, language, demeanor, and dress. These identity differences contributed to both commanders and providers characterizing their longstanding intergroup relations as extremely poor. Their interactions exhibited signs of intractable identity conflict (Fiol, Pratt, and O’Connor, 2009), meaning that each group defined itself by what the other group was not (“warriors” vs. “experts”), they stereotyped one another (“bullies” vs. “Berkeley hippies”), and they held zero-sum conceptualizations of their relationship.
The majority of commanders were men in their late 20s and early 30s who had graduated from West Point, Officer Candidate School, or Reserve Officers’ Training Corp (ROTC) and had deployed at least twice. They viewed themselves as seasoned “warriors” and “leaders” and were skeptical of listening to anyone who had not deployed or who had “textbook knowledge” rather than “real-world” experience. One commander explained how he saw the mental health providers: “Who is this person? So you have a Ph.D.? How can you relate to me? . . . A doctor—generally a doctor went to college, then grad school and has probably been spoon-fed their whole life and never faced real hardship.” In contrast, mental health professionals, who were an even mix of men and women ranging from their early 30s to late 50s, had years of clinical and professional training (master’s degrees or doctorates were required) and viewed themselves as “subject matter experts” in diagnosing and treating mental illness. They valued clinical knowledge from years of professional training and experience. One provider noted, “It can be frustrating when they (commanders) don’t follow your recommendations. I try to remind them that, ‘Hey, I have the Ph.D. here, not you!’ I try to remind them that I’m the expert and they’re not.”
Commanders tended to view providers, most of whom were civilians, as anti-military “Berkeley hippies” who were naïve about military culture, “coddling soldiers,” and easily duped by soldiers whom commanders often considered “faking the funk” (faking sick) to “get out of work.” One commander offered a stereotyped view of providers: “It’s a huge problem. If the soldier has a legitimate problem, they have to go see one of those ladies in [Mental Health] with cat pictures all over their walls. . . . Go and talk to Miss Dandelion Hippie Lady!?” Providers similarly stereotyped commanders as “intimidating” “bullies.” They generally assumed that commanders were unsupportive of soldiers with mental health problems and that commanders believed soldiers were faking their problems. Providers were also bombarded with negative stories about commanders from the soldiers they treated who were unhappy with their experience in the army. One provider explained the dominant way most providers saw commanders: “. . . they’re bullies and single-minded about their missions.”
Commanders defined their professional identity in large part by their responsibility for “taking care of soldiers,” saying they believed a “good commander” “took care of his own” rather than “punted” his soldiers to “outside agencies” like Mental Health for help. Mental health professionals also defined a core aspect of their identity as being responsible for “taking care of patients.” These two professional groups believed they each knew what was best for “their” soldiers/patients. One commander noted how he always seemed to be at odds with providers in a seemingly zero-sum game: “There’s a lot of bumping heads with them [providers]. . . . It’s like they’re the defense for the soldier and I’m the prosecution.”
Observations of these two professional groups also revealed notable differences in identity displays in terms of their language, demeanor, and dress. Commanders were well-versed in using the acronyms, jargon, and idioms common in the army, so much so that outsiders often described it as a foreign language (e.g., “I speak a little Army”). Commanders, trained to begin any briefing with the “BLUF” (“bottom line up front”), used a direct and deductive communication style and were generally intolerant of lengthy, inductive, or ambiguous speech. In contrast, mental health professionals generally were not fluent in “Army” and used their own technical medical language (e.g., “active versus passive suicidal ideation”). In addition, the providers’ clinical language accounted for evolving symptoms, making it difficult for them to make the direct, black-and-white statements commanders desired.
Regarding dress and demeanor, while commanders were always formally dressed in their green camouflaged ACUs (army combat uniforms) with standard regulation haircuts and rigid posture, the majority of mental health professionals wore casual civilian attire, carried themselves with a relaxed posture, and looked rather unkempt by comparison. Finally, in contrast to providers, who encouraged expressing vulnerability and seeking help, combat commanders were notorious for hyper-masculine displays of bravado as self-described “alpha males” who showed no physical or mental weakness by seeking any kind of help. One commander noted, “Soldiers can’t see that their commander is not Superman. They need to believe he is to have confidence in him . . . just like when I broke my foot, I would not wear a cast. You would not catch me wearing that boot!”
Integrative Mechanisms Available to Achieve Goal Alignment
Providers and commanders had access to a host of integrative mechanisms identified by the literature to promote goal alignment between different groups, including particular organizational structures (described below), strategic planning by leadership of both groups, cross-functional team meetings, and promotion of the army’s superordinate goal through a “Ready and Resilient” campaign. But these and other integrative mechanisms, listed in Online Appendix A (http://journals.sagepub.com/doi/suppl/10.1177/0001839217714024), did not explicitly address identity differences between providers and commanders. 3 Only one mechanism, organizational socialization to promote a shared, superordinate identification, addressed identity differences. But professionals are often highly resistant to organizational socialization efforts because they have spent years being socialized into the identity of their profession (e.g., Battilana and Dorado, 2010). Repeated efforts to teach providers “Army 101” failed; most providers reported that these socialization efforts made little impact because they considered themselves mental health clinicians first and government employees working for the army second. And efforts to modify the organizational socialization of commanders to increase support for Mental Health also failed; commanders were generally skeptical of the value of these efforts because they took time away from what they considered their “real work”—fielding a mission-ready subunit.
There were two integration mechanisms that the army hoped would be particularly effective for promoting goal alignment between commanders and providers. The first was a major army-wide initiative to move mental health providers out of centralized post hospitals and into freestanding clinics located within the geographical “footprints” of the different brigades on post. It was hoped that co-location would allow soldiers to more easily walk in and attend appointments near where they lived and worked and that commanders and providers could more easily connect and communicate given their greater physical proximity. Each clinic was aligned to serve one brigade and was staffed by a team of mental health professionals, including therapists (licensed clinical social workers and psychologists), a psychiatrist for prescribing medications, and a team lead to oversee the clinic and also provide care. Co-located clinics were in self-contained buildings close to, but still apart from, brigade personnel.
The second integration mechanism was assigning a subset of providers, which I refer to as “embedded providers,” to work in a matrix structure (e.g., Mintzberg, 1979) as part of both the clinical world of mental health and “the line” world of a combat brigade. These few embedded providers worked primarily outside the clinics as both practicing mental health providers who treated soldiers half-time and uniformed officers who trained and deployed overseas as the primary mental health resource for their brigade. They were “dual-hatted” and were accountable to both the combat brigade they were a part of and the army’s medical organization. The army hoped these embedded providers would be fully acculturated to the unique context of the army and develop closer relationships with commanders. According to the literature, these two integration mechanisms should have helped commanders and providers overcome entrenchment in their own group’s perspective to align their differing goals toward achieving the organization’s superordinate goal, but they did not.
Failed co-location in Clinics A and B
Co-locating clinics with the brigades should have helped overcome goal conflict, but on its own, it did not. Close observation of providers and commanders associated with two of these co-located clinics, Clinics A and B, revealed that intergroup relations were as bad as before co-location. Strong identity-related conflict, including stereotyping, dis-identification, and zero-sum conceptualizations across groups, continued in A and B. Even though providers and commanders in A and B were located close to one another and providers in each clinic engaged with commanders in only one brigade, A and B providers still interacted with dozens of commanders, and commanders dealt with many different providers treating their soldiers. As a result, commanders were generally unable to name the providers with whom they interacted. One noted, “I don’t know the people over there [in the clinic]. I get a different person every time. . . . I couldn’t tell you their names.”
The existing negative relations between providers and commanders persisted in A and B, and their conflict over privileging different goals remained exacerbated by seemingly intractable professional identity differences. One provider explained how being co-located with one brigade had not led to a notable change in relations with command: “Now we serve one brigade, but it’s really not that different than when I sat up in the hospital and saw everyone. There’s too many [commanders] to really feel any sense of ownership, which is what I thought the new model was supposed to promote. So it’s not that different. . . .” Each group continued to view the other in a stereotypical manner, and dis-identification continued: each group, at least in part, defined itself by what the other group was not. One provider explained how she viewed commanders as not caring about soldiers, unlike providers: “I love my patients, I love my [clinic] team—the clinicians here are all good. . . . Command? Not so much. Dealing with command is one of the more unpleasant parts of my job. . . . Commanders only care about the mission; we care about soldiers.” Commanders continued to view Clinic A and B providers as the antithesis to their alpha-male warrior identity: “Mental Health is growing like a cancer. And how much money has been spent on it? Billions? I am tired of all the pussies who say they want to go to Mental Health . . . when I have guys who have really seen and done some messed up shit who wouldn’t go near Mental Health.”
Intractable identity conflict persisted among providers and commanders associated with Clinics A and B, and they were unable to discover integrative approaches to handling goal conflicts in service of the army’s superordinate goal. Each group privileged its goals, often at the expense of the other group’s goals. For example, providers in A and B handled conflict over how much information to share with commanders by erring on the side of sharing as little as possible. They assumed that no good could come from commanders having this information, as they continued to stereotype commanders as caring only about their missions rather than soldiers’ mental health. One provider explained, “They think that little rank on their chest gets them a free ticket to get any information they want. . . . Command will overstep their bounds all the time, and I will say, ‘That’s their private health information; you have no need to know that!’ And it will cause a conflict. . . .” Such decisions by providers in Clinics A and B may have benefited therapist–patient trust but often led to unintended consequences that negatively affected patient care when a soldier’s commander could not assist in a soldier’s recovery or make allowances for poor work performance or minor disciplinary infractions related to a soldier’s mental health condition. In one case, a soldier was punished for falling asleep while manning the unit front desk overnight because his commander did not realize he was on a new sleep medication for insomnia that made him drowsy. In a more serious case, a commander explained his frustration with how a provider’s invocation of professional rules related to HIPAA prevented sharing information, which he perceived contributed to a soldier’s suicide in his unit:
My number one challenge is HIPAA because it puts up barriers between the person who has the information and the person who needs the information. . . . I had a [soldier] who had a trauma in Afghanistan and committed suicide. . . . He had been making appointments [to see Mental Health] on his own [without command knowing about it] and had been seeing shadows and hearing voices and having up to 15 drinks a day. I’ll tell you, [Mental Health] really pissed me off! There is a line somewhere and we were not told because of HIPAA.
Failed matrix structure among embedded providers
The army also tried to align goals between providers and commanders by assigning some providers to work within a matrix structure, but these embedded providers and the commanders they worked with also failed to accomplish the army’s superordinate goal. The embedded providers were uniformed-officer psychologists or social workers assigned to train and deploy with each brigade but were also accountable to the army’s Medical and Mental Health divisions. But they spent limited time with other providers in the clinics, and I found that the high levels of personalization with commanders that these embedded providers experienced, without as much regular interaction with other clinic providers, led many to become coopted by the commanders in whose brigades they were embedded.
After a year in the role, most embedded providers did not report even seeing a conflict between providers’ and commanders’ goals because they believed commanders’ goals overrode those of Mental Health. One embedded provider explained, “To me, we really have one client—the army. There really isn’t a conflict. . . . I’ve never had an ethical dilemma. It’s not like that. What’s good for the army is typically good for the soldier.” Instead of prioritizing patients’ welfare, another embedded provider explained, “Command is your patient. . . . We should always be thinking—how do I ease the suffering of command? We need to be viewed as subject matter experts who can be consulted. Commanders care about one thing—am I ready to go to war?” Finally, embedded providers reported prioritizing their officer identity over their clinician identity. One explained, “You learn from day one—it’s ‘officer first, clinician second.’ You have to keep that in mind in all you do. You are an officer in this brigade first and foremost, then a clinician.”
Though this matrix structure reduced identity-related conflict by promoting personalized relations between providers and commanders, it resulted in failed superordinate goal attainment as embedded providers privileged the goals and perspectives of commanders over those of their own professional group. For example, embedded providers handled a situation most providers found difficult—deciding how much information to share with commanders—by erring on the side of sharing, in the service of the mission, whatever information commanders wanted to know. Faced with a decision about how much to share with a commander inquiring about a patient’s condition, one embedded provider immediately shared the requested information and said he felt obligated to provide the commander with this requested “situational awareness.” Although beneficial to the commander and possibly the mission, such information sharing sometimes came at the patient’s expense. For example, when soldiers learned that embedded providers were liberal in sharing information with command, many reported being more hesitant to seek care from them.
Anchored Personalization and Successful Goal and Identity Conflict Resolution
Providers and commanders associated with two other co-located clinics that served brigades in the same combat division as A and B—Clinics C and D—overcame their identity differences such that they no longer stereotyped, dis-identified, or held zero-sum conceptualizations of one another. Like the embedded providers, the providers in Clinics C and D did this by developing personalized relationships with the commanders. But unlike the embedded providers, the providers in C and D were firmly anchored in their home group identity and did not become coopted by commanders. The main difference in Clinics C and D was an organizational role assignment structure characterized by what I call “anchored personalization,” in which providers and commanders were assigned to work exclusively with specific members of the other group while remaining embedded in their home group. In C and D, each mental health professional was assigned as the point of contact for 6 to 12 commanders; C and D providers were assigned to one or two specific units within the brigade their clinic served and worked only with soldiers and commanders from those units (~6 commanders per unit). 4 Though it was not perfectly efficient, as fewer soldiers could be seen overall when demand was uneven across units, this organizational assignment structure allowed providers and commanders in C and D to develop stable, personal connections and relationships with one another. At the same time, they remained embedded and anchored in their home groups; they worked 40+ hours a week surrounded by their professional colleagues who also had stable, personalized connections to specific members of the other group. This structure provided affordances that differed from those of A and B or the embedded providers. 5
Assigning providers to specific units was part of the army’s standard operating procedure for setting up these new co-located clinics, but it was not emphasized as important by leadership and was inconsistently adopted. Clinic team leads, who oversaw patient scheduling but otherwise had little authority over providers’ behavior, reported initially making the decision casually to staff providers in this way (or not) and did not explicitly recognize its positive effects a priori, as noted along with other alternative explanations in Online Appendix C. Emphasis was on physically building and staffing the co-located clinics, with poor performance attributed to inadequate staffing, even though all clinics at this post were short-staffed.
This unique organizational structure of anchored personalization promoted a set of practices that reduced identity conflict between members of each group and entrenchment in their own group’s perspective, such that they interacted in new ways to collectively work in service of the army’s overarching goal. As described below and illustrated with additional examples in table 2, these practices included developing personalized relationships with members of the other group, anchoring group members in their home group identity, and co-constructing integrative solutions to conflict.
Anchored Personalization Practices in Clinics and Brigades C and D
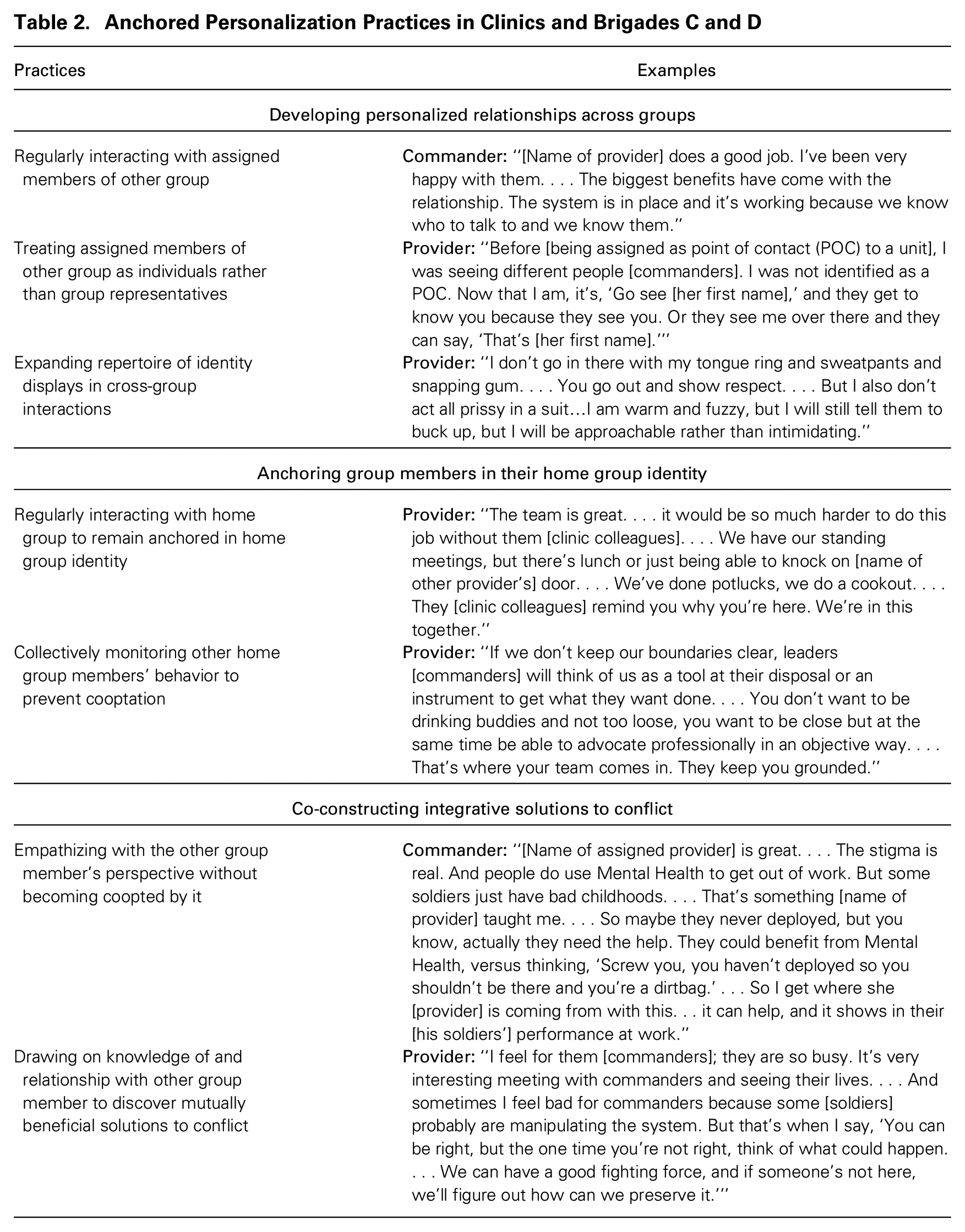
Developing personalized relationships across groups
Providers and commanders developed personalized relationships by regularly interacting with their assigned members of the other group, treating one another as individuals rather than as group representatives, and expanding their repertoire of identity displays in cross-group interactions. Because providers worked with only a handful of commanders and commanders worked with only their one assigned provider, these stable provider–commander dyads in C and D had more opportunities to regularly interact, an essential component for developing a personalized relationship. These interactions occurred through e-mail, phone, and in-person meetings either at the clinic or at commanders’ offices on a weekly or sometimes daily basis as soldiers’ cases arose that required commanders’ cooperation and support. After being assigned to specific units, C and D providers got to know their assigned commanders and their units better by leaving the clinic and visiting commanders in their offices or unit work areas, an act that was nearly impossible in clinics like A and B in which providers worked with dozens of commanders. One Clinic D provider explained, “The beauty of [being assigned to units] is that you really get to know the commanders . . . so I can go to the [unit] and do a walk around and people will know who I am. . . . I think when I first came on board there’s probably a little more resistance—they’re like, ‘Who are you?’” For C and D commanders, instead of interacting with different providers each time they came to the clinic to discuss a soldier, they interacted primarily with one assigned provider. One commander explained his enthusiasm for this arrangement, exclaiming, “Having a POC [point of contact] is awesome. I can see them daily. They are a familiar face and they know how I think and what I’m about.”
The anchored personalization structure also afforded greater opportunities for providers and commanders to set aside stereotypes and get to know one another as individuals rather than as representatives of their respective groups. For example, C and D providers and commanders typically referred to one another by their first names. One provider explained the transformation that occurred after developing personalized relations with commanders: “Now it’s much better . . . we can get to know command and our own group of soldiers. I’m at the point that I have them all [commanders] on speed-dial and they have me on speed-dial. . . . That’s how profound it can be. . . . Now you get to know the person as a person. Like he’s [John] in here with me, not Captain [Smith].” Another provider noted how stereotypes held by both groups were breaking down in the anchored personalization structure: “It was good because it made us less scary to them. And it made me realize they are less scary too.” One of the few providers who switched clinics during the study period moved from Clinic A to Clinic C. She spoke of how she and her former Clinic A colleagues viewed commanders as “adversaries,” while in Clinic C she developed a more positive view of her assigned commanders: “Before [in A], we thought of them [command] as an adversary because they were kind of always on the other side of things. . . . And command—we were trying to keep them more at a distance. . . . Now it is much better. They know me and I know them.”
Similarly, C and D commanders began to view mental health providers in a less negative and stereotypical way after getting to know their assigned provider. One commander said, “I had a pretty negative view of Mental Health. . . . it’s bad, but you think, ‘Oh this [soldier’s] a dirt bag or can’t cut it.’ . . . And you think the doctors over there just don’t get it. . . . Since working with [assigned provider], I have a much better view of Mental Health.” In addition to regularly interacting and treating one another as individuals rather than group representatives, providers and commanders in C and D also used an expanded repertoire of identity displays during cross-group interactions. By subtly adjusting the language they used, their style of speech, and their demeanor during their interactions, these providers and commanders demonstrated respect for the other group’s preferred interaction style, which helped them develop relationships. For example, providers in C and D used proper army terminology more regularly, and some even began cursing and speaking in a more direct manner when interacting with their assigned commanders. At the same time, they remained anchored in their professional identities and drew the line so as not to go too far, such as by not using derogatory army slang. One noted:
. . . it helps to use their language. . . . Like I will even say “roger” instead of “yeah.” . . . I try to use their language and their words. . . . If they start cussing, I will. Then I know it’s okay. . . . So I just try to relate to them and be blunt and to the point with them and use their language. I don’t say shit bag. I don’t like that judgmental stuff. But I don’t soften up what I have to say.
Commanders also altered their identity displays by using clinical terminology when discussing soldiers’ mental health conditions. For example, commanders in C and D used more-accurate terminology like “manic episode” in lieu of language mental health professionals considered derogatory, such as “bat shit crazy.” Many C and D providers also commented on how their commanders “let their guard down” more often with them than in the past, engaging more as “human beings” than as supermen. One provider noted, “Well [name of commander] is so intimidating . . . but he’s a softy inside. . . . He scared me a bit at first. But now I know he’s a class clown, a real funny-guy with a big heart.”
Anchoring group members in their home group identity
Group members in C and D stayed anchored in their professional identities by regularly interacting with their home group and collectively monitoring other home group members’ behavior to prevent cooptation. Providers and commanders had daily interaction with other home group members at work despite more personalized cross-group relations. Providers regularly interacted with their clinic colleagues during daily morning “stand up” meetings as well as during weekly “multi-disciplinary treatment planning meetings” in which they discussed difficult cases. In addition, providers engaged with their clinic colleagues informally over lunch and outside of work. Commanders likewise regularly interacted with other commanders in their units. C and D providers said that they felt grounded as clinicians and members of their clinic “team.” One provider explained, “I think that our success is because we [the clinic team] are also very grounded. We are very solid . . . we have . . . clear boundaries. . . . We . . . have that support." A provider from Clinic D noted:
Being on the [clinic] team has been wonderful, a real benefit. Hands down, I personally find it highly advantageous especially with all these tensions with the mission and patient care and talking with leadership [commanders]. It helps you maintain your professional distance. . . . I would be afraid to practice independently, because I would lose the opportunity to have this kind of fluid consultation with peers.
The anchored personalization structure also afforded C and D providers and commanders the opportunity to collectively monitor other home group members’ behavior to prevent cooptation, which was especially important for providers given that commanders were the more dominant group as members of the “line” rather than “support” function of the organization. C and D providers said their “clinic team” members helped “keep you grounded” or “pulled you back” if they saw someone beginning to get “too caught up” with what their command counterparts wanted.
6
One provider noted:
While developing friendships and relationships with leaders are important, you need to . . . distinguish yourself as a professional, and establish clear boundaries, and not become too enmeshed with them . . . it can be easy as you get to know command to start going along with what they want. But your [clinic] team can help with that. They’ll pull you back when you need it.
Such collective monitoring was enabled in part because each provider was connected to a different set of commanders, so they could keep one another “in check,” as they did not have personalized relations with the same people. Another provider noted how his clinic team kept him true to his home group’s goals even as he developed closer relationships with commanders: “I had begun to be less objective, but because I get feedback from the [clinic] team, the patient and army benefited, because otherwise my personal relationship with this [commander] may have clouded my judgment. But because of the team, I was able to stay grounded.” In one case, a provider had begun to spend extended periods of the day doing “walkabouts” in the brigade outside the clinic. He was “reined in” by his clinic team during a meeting in which this behavior was called out, and a discussion ensued about the importance of “setting boundaries” and providing therapy exclusively in the clinic.
Co-constructing integrative solutions to conflict
C and D providers and commanders co-constructed integrative solutions to conflict by empathizing with the perspective of their assigned members of the other group and drawing on their knowledge of and relationship with one another to discover mutually beneficial solutions. Regular personalized contact between assigned providers and commanders in the anchored personalization structure led to increased empathetic perspective-taking, consistent with studies on the effects of personalization (e.g., Brewer and Miller, 1984, 1988), without enabling cooptation. This was critical for discovering common ground (i.e., identifying an area of mutual agreement). One Clinic C provider explained, “I can see both sides. I feel the pressure they are under when I think about the pressure to deploy, I get that. But the other side of me is a member of this clinic. . . . Clinically, it may not be right for that patient to deploy. So it creates conflict, but I can see it both ways.” Commanders also came to better understand the perspective of providers regarding the risks of aggravating a soldier’s condition from exposure to stressful situations and regarding providers’ intentions. One commander noted, “The big difference is now I realize they’re [mental health providers] not trying to screw over my mission. They actually want to help my soldiers.”
As providers and commanders came to understand and appreciate each other’s points of view, they started to realize their differing perspectives were not zero-sum. One Clinic C provider explained how she now took commanders’ perspectives seriously, without becoming coopted, to help craft win–win solutions to conflict:
. . . I’m not just a pawn of the commander. I just don’t do whatever he says. . . . But again, if you keep on the same purpose, where what you recommend is good for everyone, then anything can get done. . . . I don’t think it’s command wins and the patient loses, or the patient wins and command loses. My job is about what can I do . . . so we can all win.
C and D providers and commanders were able to draw on their relationship and knowledge about the other person to discover shared objectives they previously assumed did not exist. Many providers said they realized that engaging with commanders actually helped their soldiers’ recoveries more than if they shut them out. One provider said, regarding commanders, “Who doesn’t want their soldier to be productive and healthy? Who does not want that?” Providers also said they had expanded their perspective as a result of their relationship with their assigned commanders and greater knowledge of what their subunits were like to think about the patient not only as a patient but also as a soldier embedded in a larger army environment that shaped that person’s recovery. One explained, “With civilian training, it’s only about the patient—that’s really only what you’re concerned about, and there’s no bigger picture to it. [But after being assigned to a specific unit] . . . to me the patient still comes first, but the army is part of it, too.” Commanders took notice of providers’ improved understanding of their needs and units. One said, “They don’t know everything about the army, but they understand us better. . . . They know our unit and that makes a huge difference.” In turn, commanders became more open to providers’ perspectives. One commander explained, “Our job is to train soldiers and when we have soldiers who need help, it takes time to help them, and that takes time away from training. But Mental Health works with us. They know that we can’t stop training, it’s our job. But they need to do their job too.” Commanders in C and D discovered mutually beneficial solutions to conflict with providers by realizing how supporting soldiers’ mental health care could also promote their subunit’s mission-readiness by helping soldiers recover faster and addressing their problems earlier. These commanders talked about how Mental Health acted as a “force extender” by providing another avenue for them to fulfill one of their core commander responsibilities of “taking care of soldiers.” Commanders came to appreciate Mental Health while remaining anchored in their core identity as “warriors.” This change was exemplified in how some commanders publicly encouraged their soldiers to get care, but in a way that still appeared “manly.” As one commander noted, “I tell my soldiers now, ‘Just because someone’s in Mental Health, just means they’re man enough to get help.’”
Outcome Differences in Achieving the Superordinate Goal in Clinics A and B versus C and D
Table 3 outlines differences between Clinics and Brigades A and B and C and D in their ability to achieve the army’s superordinate goal of having both mentally healthy and mission-ready soldiers. Of the 132 situations I analyzed in which mental health providers and commanders experienced conflict over how to achieve the part of the organization’s superordinate goal they each privileged, providers and commanders achieved integrative solutions in 89 percent of these situations in C and D, versus in only 5 percent of situations in A and B. An integrative solution is one that resulted in a positive outcome as reported by both the provider and commander most closely involved in the situation. I also report other indicators of the different outcomes achieved in Clinics A and B versus C and D. For example, because providers and commanders working in A and B were more likely to pursue their own group’s goals at the expense of the other group’s goals, this led to situations in which commanders ignored the recommendations made by providers, such as to excuse soldiers from a stressful training exercise. Only 10 percent of commanders reported regularly complying with providers’ recommendations in A and B compared with 86 percent in C and D. To triangulate these accounts, I analyzed 108 providers’ duty-limiting soldier-care recommendations, and commanders’ and providers’ reports of whether these specific recommendations were followed, and found that while only 18 percent of these recommendations were followed by A and B commanders, 90 percent were followed by C and D commanders. Commanders in Clinics A and B said they ignored providers’ recommendations they considered to be “out of touch” or “unnecessary.”
Outcomes Achieved in Clinics and Brigades A and B versus C and D
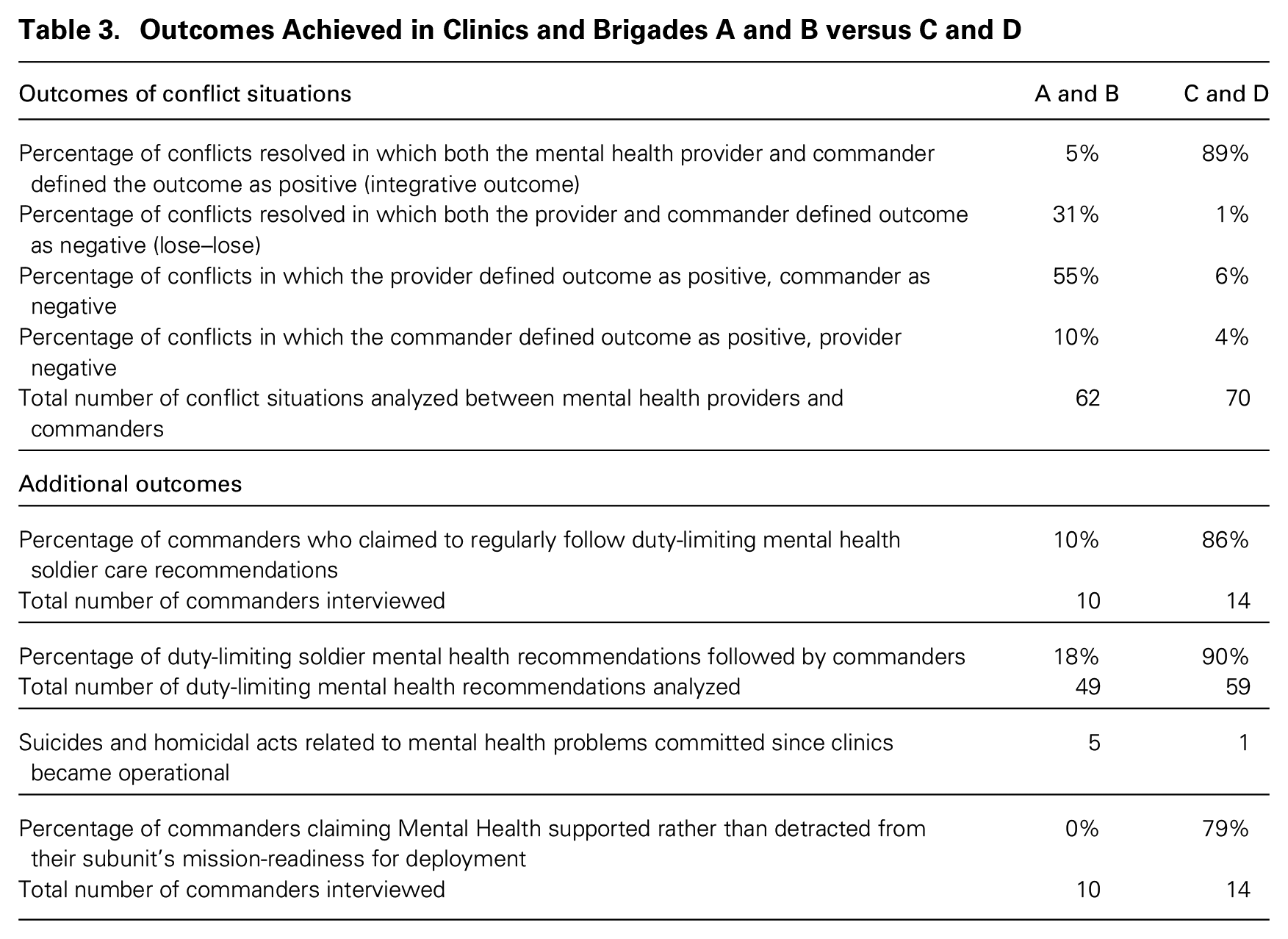
In addition, there were fewer suicides in Brigades C and D than in A and B—one versus four, respectively, since the clinics became operational—and fewer homicidal acts related to mental health problems—zero versus one, respectively. Commanders also reported higher levels of mission-readiness in C and D. Seventy-nine percent of commanders interviewed in C and D indicated that Mental Health supported rather than detracted from their subunit’s readiness for deployment, while all A and B commanders indicated that Mental Health detracted from mission readiness.
Most notably, care decisions from providers in Clinics A and B often inadvertently hurt soldiers’ recoveries and desired career prospects, according to commanders and embedded providers’ reports, which often increased the stigma of seeking care and reduced commanders’ support for soldiers seeking care. In contrast, in C and D, providers responded to similar situations by co-constructing integrative solutions with commanders in ways that not only helped soldiers’ recoveries but also protected soldiers’ desired career prospects, reduced the stigma of seeking care, and improved commanders’ support for mental health care usage, while minimizing negative mission-readiness effects on the unit. These markedly different outcomes were a result of the different ways that providers and commanders in C and D and A and B handled similar conflicts.
Addressing goal conflict over prioritizing individuals’ vs. subunits’ welfare
All providers and commanders were regularly in conflict over their clashing professional group goals on prioritizing individual soldiers’ versus subunits’ welfare. A conflict that occurred both in A and B and in C and D was around a soldier experiencing panic attacks before an important field exercise. In Clinic A, a soldier who had “lost buddies in a tank” in Afghanistan began having panic attacks when inside tanks. His subunit was leaving for a month-long training in the field that his commander had been counting on him to attend to be eligible for their subsequent combat deployment. The soldier wanted to go and not be “left behind,” but his provider was concerned about him going. The provider, who did not have a personalized relationship with this soldier’s commander, privileged the goals and perspective of her professional clinic colleagues and reported that if any soldier was undergoing treatment for PTSD or another moderate to severe anxiety or depressive disorder, she did not take any chances and would not allow the soldier to go to the field. This provider did not consult with the soldier’s commander because she said she believed he cared more about his mission than his soldier’s health, and she put in writing (in a “profile”) that the soldier should not go to the field. Although on the surface this may seem like it was the safest option, in practice, depending on the soldier’s condition and the field exercise, leaving soldiers at home (in “the rear”) and isolating them from fellow soldiers often aggravated their mental health conditions and discouraged other soldiers from seeking care. In this case, the soldier’s commander ignored his provider’s recommendations and took the soldier to the field for training anyway because he said he believed the provider was out of touch with what the field was really like and that the risks of leaving the soldier behind with minimal supervisory oversight were high. In this case, the soldier did not “decompensate” (i.e., have a mental breakdown) while in the field, but the soldier was also unable to fully benefit from the provider’s recommendations designed to support his treatment and recovery.
When facing a similar conflict over prioritizing the welfare of an individual patient versus the subunit, C and D providers and commanders resolved these situations in markedly different ways while operating in a structure that promoted anchored personalization. In a similar case of a soldier experiencing panic attacks before a field exercise, a provider and commander in Clinic C worked together to develop a solution that helped both the patient’s recovery and the subunit’s mission-readiness. The provider called the soldier’s commander before issuing a formal written profile stating that the soldier should not go to the field. She told the commander her concerns and also said that she understood how much pressure the commander was under to have sufficient manpower for the training exercise. The provider explained how she regularly took the perspective of the commander, or “flipped it,” while remaining grounded in her professional commitment to helping soldiers. She explained, “I had to try to educate him on why it’s best for the soldier. But then I will flip it to be about what does the commander feel? . . . I flip it. I reframe it from the commander’s point of view.” The provider learned from the commander what the field exercise entailed, and together they brainstormed alternative tasks the soldier could do that would not aggravate his condition. They found a way to make a portion of the field exercise part of his therapy, as a next step in confronting his fears and to gain useful information about whether he would be able to return to full duty or whether it was time to begin a medical separation for an honorable discharge from the army. The provider also requested that the soldier leave the field after two weeks to check in at the clinic to be cleared to return again. Better to test a soldier in a training simulation than an actual deployment, the provider reasoned, and use it as an opportunity to further the soldier’s recovery. The commander explained his role in co-creating this response:
[Name of assigned provider] contacted me first . . . before doing the profile. . . . We talked about what the provider wanted and we worked it out because it’s hard for a soldier . . . to stay behind because they’d feel like they’re betraying [soldiers], so we worked something out . . . so they could still go to the field.
This provider later noted how helpful her home group of clinic colleagues had been in ensuring she remained anchored in her goals as a mental health professional by not becoming too concerned with the commander’s objectives at the expense of a soldier’s care: “I try to look at the case and see, ‘Am I too caught up in it? Am I missing something?’ So it’s a good thing for them [her clinic colleagues] to come in, and for us to talk. . . . the team helps, they pull me back, so it helps being able to consult with others.”
Addressing goal conflict over sharing soldiers’ health information
Commanders generally wanted to know more information about their soldiers’ mental health problems than providers wanted to share. In one case, a patient had a diagnosis of depression and had begun regular therapy along with medication, and the commander asked the provider to disclose information about this soldier’s treatment progress because he was not performing well at work. The patient’s provider in Clinic B privileged protecting patient privacy above all else in accordance with his professional training and the beliefs of his clinic peers. He refused to share any information on this soldier’s case with his commander whom he did not have a personalized relationship with. The commander responded by using alternative means of extracting this information. Commanders had the option of going around the provider and asking the brigade’s embedded provider for information or of doing a “command directed referral,” by which a soldier is ordered to get a mental health evaluation that is to be shared with the commander, a tactic that is considered humiliating to a soldier and that limits the provider’s ability to restrict what is shared.
In a similar case of a commander inquiring about a depressed soldier in Clinic D, within the anchored personalization structure, the soldier’s provider listened to her assigned commander’s concerns and encouraged the soldier to give her permission to share his situation with his commander to help account for the dip in his performance and minor disciplinary infractions. She explained, “I was thinking, ‘This soldier is not optimally doing his job’ and now his command is going to be looking at him like, ‘you’re just a sorry soldier’ when in fact I know that your wife just left you and you have depression and clinical insomnia. [I encouraged that soldier to] . . . sign that authorization to disclose [his situation to command].” The provider noted that by speaking with the commander about this soldier, she believed she helped the soldier’s recovery more than if command had not been included. She reported that engaging with the commander also improved his overall support for soldier care when he saw the positive benefits to both the soldier’s health and performance at work:
[Command] goes, “Oh! Wow! Great! Thanks!” And then they give you information on how the soldier is at work. And so we kind of work together as a team. . . . Then you have really good outcomes . . . because the soldier says, “You know what, I went [to the clinic] and she talked to my command and they worked it out . . . and now I feel better.” And command said, “Wow! The soldier went to [the clinic] and actually, everything is good.” . . . It builds credibility. It’s no longer being that enemy that we [mental health providers] were.
The commander in this case noted that he no longer “pushed” for more information, because he trusted that his assigned mental health provider knew when and what to share:
As a commander, I get the information I need. Sometimes it’s vague because I can’t be told the details I’m not allowed to know, but I don’t think I need any more than what they tell me. Dr. [name of assigned provider] gets what I need to know, which is basically: can they do their job or are they going to hurt themselves or someone else. . . . Some doctors get confused on being bound by HIPAA. . . . I’m not asking to violate your ethics as a doctor. I am asking because I’m about to put a rifle in his hand.
The provider also explained how she was able to avoid cooptation and pressure to share more information with command than needed by drawing on the anchoring of her home group of clinic colleagues and running things by them first:
. . . a lot of communication with command is something I run by my peers first. Before I share with command, I ask someone else. So we will shout ideas back to one another. . . . I ask my colleagues, can you talk? . . . When you aren’t sure, you should talk to them. . . . Because they might have a different point of view . . . and you can’t make these decisions lightly.
Addressing goal conflict over instilling mental toughness vs. reducing the stigma of seeking care
Another common conflict was around differing professional perspectives on leaders serving as exemplars of mental toughness versus exemplars of help seeking toward reducing the stigma of seeking care. Conflict occurred when commanders requested that providers make special arrangements to see them or other subunit leaders, such as by meeting after hours or outside the clinic. Providers in Clinics A and B, without anchored personalization, generally handled this situation by privileging their goal to prioritize reducing the stigma of seeking help. For example, a commander requested that one of his senior sergeants be allowed to avoid the waiting room so as not to be seen there by junior soldiers, but the provider said her clinic did not make special accommodations to treat leaders any differently than junior enlisted soldiers because they believed treating all patients equally and seeing leaders in the clinics would help break the stigma of seeking care. Though well-intentioned, decisions by A and B providers not to treat leaders differently often backfired, as many leaders in these subunits chose not to seek help at all or reported paying out of pocket to get help off post, as this senior sergeant did. One provider who worked in Clinic A for six months before moving to Clinic C explained that this approach often had a negative effect on whether high-ranking leaders actually sought and stuck with care: “And that’s a big difference between here [Clinic C] and [Clinic A]. In [Clinic A], they would say and tell everyone to ‘leave your rank at the door,’ but not everyone feels comfortable, and then they just wouldn’t come at all.” During this study, several leaders committed suicide at this post, but they had never sought care in Clinics A and B. In one case, it was later found that the leader had called an anonymous suicide hotline. A commander noted, “We had some suicides in [Brigade A], and I have to wonder do we contribute to the problem . . . by not having a confidential option for officers.”
In contrast, providers in Clinics C and D used their personalized understanding of commanders and their units to co-construct mutually beneficial solutions. In a similar situation of a commander asking for discreet accommodations for one of his subunit leaders to avoid the waiting room, his provider made an alternative arrangement to ensure this leader received care. This provider explained how he was able to see both points of view on officers and leaders getting care: “Now there are two views on officers and leaders getting care. One view is it should be a badge of honor, ‘I’m getting help and you can too,’ rather than a badge of weakness and that your men may lose confidence in your ability to lead them. I can see both sides.” The commander involved explained how he encouraged multiple subunit leaders to get help, in part because the providers in this clinic made special accommodations for them:
Overall I am happy with our [name of] clinic. They do a great job. Like I’ve sent more senior guys to them, and told them, “I do not want him in the waiting room,” and they will make it work and get him right in. Like I have a lieutenant I’m sending there, and I don’t want him in the waiting room with the stigma.
Together, C and D providers and their assigned commanders found alternative ways for leaders to receive discreet and sometimes “off the books” care, such as by meeting in leaders’ offices to give the impression they were talking about soldiers or allowing leaders to receive care after hours, during lunch, or even through the back door to avoid the waiting room. One provider explained:
I’ll make time to see the commander late in the day and let them come in the back door or come to their office to meet with them so it looks like a meeting about soldiers. . . . While you could say, “it’s a good thing for the junior soldier to see the senior soldier getting help,” but that’s not the way the junior soldier sees it. I’d rather the leader get care and come through the back door than not get help.
Although it might seem that this would prevent breaking the stigma of seeking care, the leaders in C and D reporting they had used Mental Health services themselves were the ones most open with their soldiers about their experience after personally experiencing the benefits. This made progress toward the providers’ goal of reducing the stigma around seeking care. One commander explained that he now shares his experience to encourage others to get help:
And I tell my soldiers [about his struggles with depression and suicidal thoughts]. I am open to the troops about what I’ve gone through. I was at a low point. . . . But you know I’m about the 100th person to go through this. Lots go through this. So I’ve talked about it. I was scared of getting, I don’t know, I didn’t want to seem like I had problems, but now I am open about it.
Exceptional cases
The anchored personalization structure afforded the opportunity for personalized relations between commanders and their assigned providers, but it did not guarantee these personalized relationships would actually develop. The few conflicts in C and D in which integrative outcomes were not achieved were associated with dyads that had not (or at least not yet) developed a personalized relationship. And the few conflicts between providers and commanders in A and B that were handled in ways that did result in integrative outcomes were associated with dyads that had more personalized relationships. For example, there was one commander–provider dyad in A in which the provider considered himself the informal point of contact for that commander’s subunit because, by chance, he had a patient load dominated by members of that subunit such that he worked with the same commander repeatedly in a short period of time. But this relationship was not maintained given the dozens of other commanders he worked with and informal sanctioning by his clinic colleagues who were disapproving of such close relationships with commanders.
Discussion
All providers and commanders faced longstanding conflict related to their professional groups’ goal and identity differences, and they had access to similar integrative mechanisms to overcome these differences. Yet only those associated with Clinics and Brigades C and D successfully addressed these conflicts by co-constructing integrative solutions that allowed for both mentally healthy and mission-ready soldiers. I draw on these findings to develop a model, shown in figure 1, that explains how and when professional groups with strong commitments to their professional identities can overcome goal conflict to accomplish superordinate organizational goals. An organizational structure of anchored personalization, whereby group members remain embedded in their home groups while they are assigned to work with specific members of the other group, promotes developing personalized relations across groups, anchoring group members in their professional identity, and co-constructing integrative solutions to conflict. Group members can develop personalized relations across groups by regularly interacting with assigned members of the other group, treating them as individuals rather than as group representatives, and expanding their own repertoire of identity displays in cross-group interactions. They can anchor members of their own group in their professional identity by regularly interacting with them and collectively monitoring their behavior to prevent cooptation. And they can co-construct integrative solutions to conflict by empathizing with the perspective of members of the other group without becoming coopted by it and by drawing on their knowledge of and relationship with their assigned other-group members to discover mutually beneficial solutions.
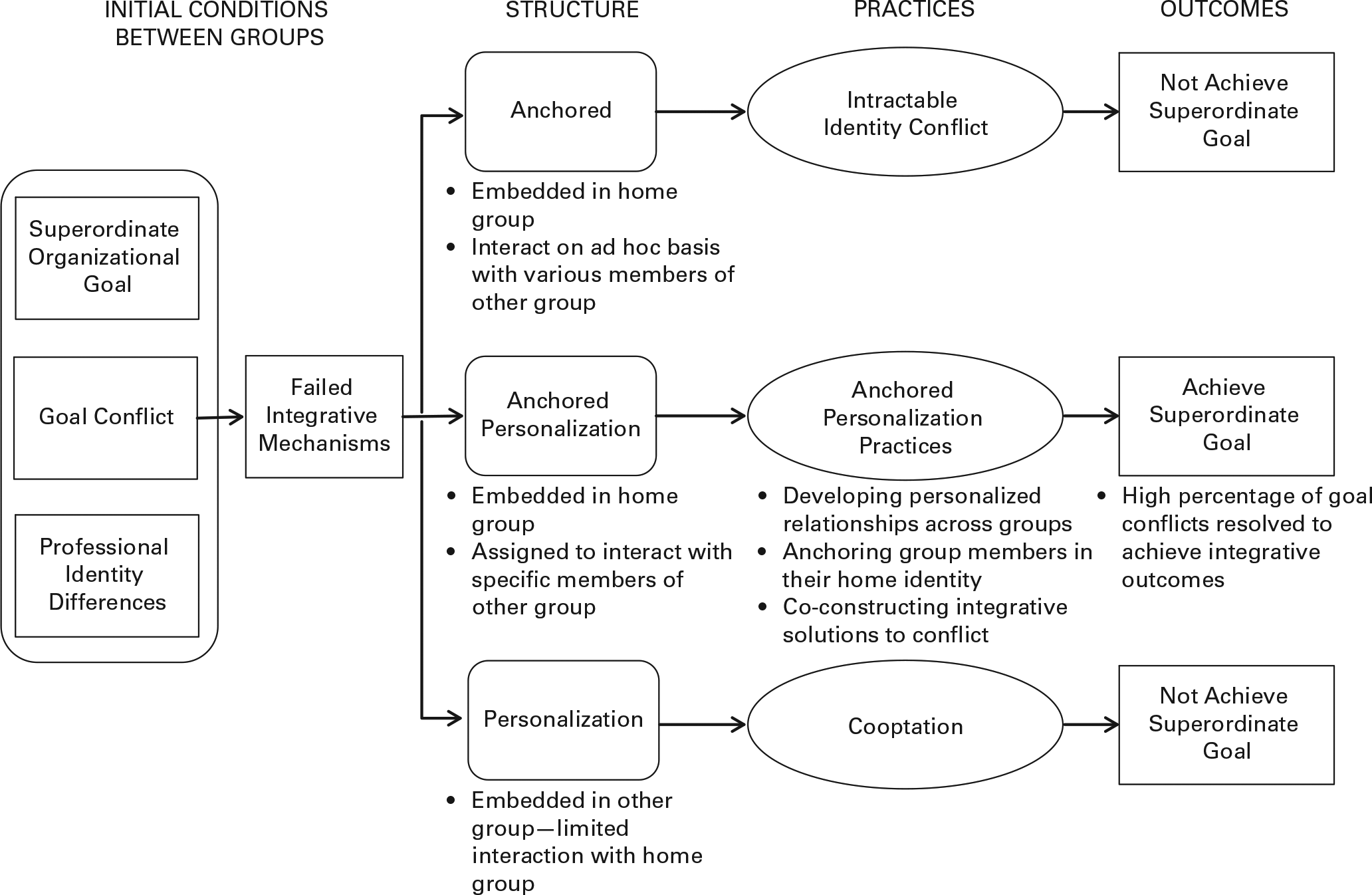
Model of anchored personalization for managing goal conflict between professional groups.
In contrast, structures that promote only anchoring in one’s home group identity without personalization across groups can lead to the continuation of intractable identity conflict, with each group pursuing its own goals at the expense of the other group’s goals. Structures that promote personalization across groups but not anchoring in one’s home group identity can also lead to failure from cooptation to pursue the goals of the more dominant group.
Contributions to Our Understanding of Goal Conflict in Organizations
These findings make multiple contributions to our understanding of managing goal conflict among groups in organizations. First, though the existing literature suggests a host of ways that conflict over goals can be managed, the mechanisms proposed to achieve this integration do not always work (e.g., O’Connor, Fiol, and Guthrie, 2006; Jarzabkowski and Balogun, 2009). Such alignment mechanisms may not be effective when longstanding intractable conflict over differences in professional identity exists, such that each group stereotypes the other, defines itself by what the other is not, and presumes that a gain for one group must come at the expense of the other group. Existing scholarship suggests that identity differences between subunits can be managed by promoting a superordinate organizational identity (e.g., Simon, 1947; March and Simon, 1958), but this approach may be difficult for groups with strong extra-organizational commitments to their professional identities.
Given the increasing prevalence of occupational and professional groups working inside organizations (see Anteby, Chan, and DiBenigno, 2016, for a review), conflict between professional groups in organizations has major practical and theoretical importance. When professional identities are implicated in a conflict, the conflict can present an affront to the professional group members’ sense of who they are. Under this condition, groups must first address these identity conflicts to achieve superordinate goals. Professional identity differences among groups may help explain the mixed findings of previous research, such as Van den Bulte and Moenaert’s (1998) study showing that benefits from co-location were observed only among different R&D groups that shared the same professional identity as scientists. Changing the physical proximity between R&D and marketing personnel did not have an effect on their communication, perhaps because of strong differences in professional identities between scientists and marketers.
Second, I introduce a novel organizational integrative mechanism that addresses the identity-related aspects of conflict between different professional groups in organizations when superordinate organizational identification is difficult—an organizational structure that affords anchored personalization across groups and supports the resolution of identity differences between groups in two ways. First, by providing the opportunity for personalized relationships to develop between members of different groups who are assigned to work with one another, this structure helps reduce intergroup stereotyping and negative outgroup categorizations. Second, by supporting group members spending the majority of their time with their own group, this structure affords collective anchoring in their professional identity to prevent cooptation.
Some integrative mechanisms in the goal conflict literature, such as liaison and intermediary boundary-spanning roles (e.g., Lawrence and Lorsch, 1967b; Mintzberg, 1979, 1993), share commonalities with the anchored personalization structure, yet they are different in important ways. All providers and commanders I studied were in boundary-spanner positions because they regularly interacted with members of the other group, yet only C and D providers and commanders successfully addressed goal conflict. Much has been written about the importance of boundary spanners for integration (e.g., Aldrich and Herker, 1977; Bartel, 2001; Richter et al., 2006), but much has also been written about how difficult boundary spanning can be (Friedman and Podolny, 1992; Stamper and Johlke, 2003; Dokko, Kane, and Tortoriello, 2014). Findings of this study suggest that effectiveness at boundary spanning for achieving integration across professional groups may sometimes require a structure that supports both personalization across groups and anchoring within one’s home group—a team of boundary spanners, all with assigned personalized connections to the other group.
Finally, I contribute to the literature on goal conflict by providing one of the first micro-level examinations of how goal conflict among subunits is addressed on the ground in everyday work. The literature on goal conflict generally does not specify the practices different groups use to align conflicting goals (for reviews, see Argote and Greve, 2007; Gavetti, Levinthal, and Ocasio, 2007; Gavetti et al., 2012). Most studies of goal conflict between groups use survey or archival data looking across firms on self-reported usage of certain mechanisms (e.g., cross-functional teams) and outcomes; they do not collect data on the day-to-day practices used by group members to achieve goal alignment. Structures provide opportunities or occasions for people to act in certain ways (e.g., Giddens, 1979; Barley, 1986), but they do not, in and of themselves, align conflicting group goals. My work suggests that macro-level approaches to goal conflict may be untenable at the micro level. For instance, organization-level decisions to attend to conflicting goals sequentially may not work for frontline professionals coping with tensions from conflicting goals in their daily work who may resist deferring goals they are strongly committed to because of their professional training.
Contributions to Our Understanding of Identity Conflict and Personalization
My findings also make a number of contributions to our understanding of identity conflict and personalization between groups. First, scholarship on intractable identity conflicts has highlighted the importance of addressing identity-related aspects of group conflict (see Fiol, Pratt, and O’Connor, 2009, for a review), but it has not examined how organizational structures might support the management of identity conflict. I find that an organizational structure of anchored personalization can support groups in overcoming identity differences to discover and pursue shared, superordinate goals. Scholarship on identity conflict in organizations has generally not explored structural solutions and instead has primarily emphasized psychological-based interventions such as “promoting mindfulness” between groups (Fiol, Pratt, and O’Connor, 2009). Though powerful, such interventions have been shown to often have only short-term benefits. For example, Pratt et al. (2012) described a promising psychological-based intervention to address identity-related conflict among professional groups in a large hospital—in their case, between physicians and administrators—by promoting mindfulness. This intervention, in which members from each group participated in an academic workshop analyzing a conflict between union and management representatives that they then applied to their own conflict, was successful in the short term but did not last. A structural intervention, in contrast, may have more sustainable effects given that managing identity conflict is built into how work gets done and embedded in role expectations. Various meso-level organizational structural interventions have shown promise for changing traditional relations between groups in other settings, such as “team scaffolds” that allow temporary teams to work effectively with one another (Valentine and Edmondson, 2014) or “relational spaces” in which those from various levels in the organization’s hierarchy can privately convene to effectively challenge the status quo to implement reform (Kellogg, 2009, 2011). Applying my findings to Pratt et al.’s (2012) setting suggests that an organizational structure promoting anchored personalization might entail hospital administrators being assigned to work with a specific set of physicians while remaining embedded with their administrator group.
Second, the identity literature has championed the development of a dual identity to resolve intractable identity conflict, in which group members develop a shared superordinate identity, typically around their common organizational membership (e.g., Argote and Kane, 2009; Besharov, 2014), while simultaneously maintaining their home group identity (e.g., Gaertner, Dovidio, and Bachman, 1996; Fiol, Pratt, and O’Connor, 2009; Brickson, 2013). My study suggests that superordinate identification may not always be necessary and that personalization between different group members might serve as a substitute for it to resolve intractable identity conflict between professional groups. The professional group members I studied did expand their repertoire of identity displays, but only when interacting with assigned members of the other group—their underlying professional identification did not fundamentally shift to embrace a shared, superordinate identification.
Finally, I also contribute to the literature on personalization by demonstrating that personalization without an anchoring in one’s home group identity can have a dark side, leading to cooptation. Despite examples of cooptation resulting from personalization in organizational life—from reports of regulatory capture among regulators of big banks (e.g., Katic and Kim, 2013) to stories of in-house attorneys “going native” (e.g., Jenoff, 2011)—research depicts personalization as having primarily beneficial effects, such as reducing stereotyping and increasing perspective-taking across groups (e.g., Brewer and Miller, 1984; Ensari and Miller, 2006; Shook and Fazio, 2008). The lack of attention to the dark side of personalization may stem from the fact that most studies are of different racial or ethnic groups attempting to reduce prejudice rather than of professional groups in organizations attempting to align their goals. This study suggests that efforts to promote personalization between different groups in organizations may need to be tempered by efforts to simultaneously ensure anchoring in their home group’s identity.
Contributions to Our Understanding of Conflict and Negotiation in Organizations
This study also makes three contributions to our understanding of conflict and negotiation in organizations more broadly. First, the existing literature has described four types of intragroup conflict in organizations—task, relational, process, and status conflict—and has found that moderate amounts of task conflict are beneficial for group performance as long as other forms of conflict are low (e.g., Jehn, 1995, 1997; Bendersky and Hays, 2012). This literature aligns with my findings about the importance of first resolving identity conflict (most akin to relational conflict) between professional groups to later resolve goal conflicts (most akin to task conflict) in an integrative way. Yet this literature has not specified how such relational conflict might be resolved. A structure that promotes anchored personalization across groups may help resolve toxic relational conflict by providing the opportunity for personalized cross-group relationships to form.
Second, researchers who have examined intergroup conflict have found that consolidated demographic differences between groups (Blau and Schwartz, 1984), also known as strong faultlines, can intensify conflict (Lau and Murnighan, 1998; DiBenigno and Kellogg, 2014; Koppman, Mattarelli, and Gupta, 2016). Although this scholarship suggests that a shared superordinate goal can reduce these tensions (e.g., Sherif, 1958; Jehn and Bezrukova, 2010), all of the providers and commanders in my study shared a superordinate goal of fielding a mission-ready force of mentally healthy soldiers, but only those in C and D successfully resolved conflict. This suggests that a superordinate goal may not be sufficient for reducing conflict between groups of professionals, who may focus on only the parts of the superordinate goal that align best with their training and socialization.
Finally, the large literature on negotiation suggests that to achieve integrative outcomes, negotiators must understand the interests of the other party, such as through perspective-taking (e.g., Neale and Bazerman, 1983), but it does not specify how perspective-taking can be facilitated. My findings suggest that perspective-taking can be supported by designing organizational structures that promote anchored personalization. One may also wonder if structure does not matter and if, for instance, commanders and providers could have been taught to improve their perspective-taking abilities through a targeted intervention to identify common ground. I found, however, that even mental health providers with extensive training in perspective-taking with patients were unable to take the perspective of the commanders when they worked in an organizational structure that did not enable anchored personalization. This suggests that interventions designed to teach perspective-taking skills or hire those good at perspective-taking may not facilitate overcoming goal conflict between groups with different professional identities without an organizational structure that supports anchored personalization. Though classic negotiation texts, particularly in the labor relations tradition, have identified structural supports for negotiation between groups, such as third-party mediators and structured bargaining processes (e.g., Brett, 1984; Kochan and Katz, 1988), they have not identified a structure that affords anchored personalization and embeds the management of conflict in daily work relationships.
Scope Conditions and Future Research
These findings should be considered in light of several scope conditions. First, anchored personalization may be necessary only for groups with strong commitments to their professional identities; in situations of minimal identity-related conflict, the literature’s existing set of integrative mechanisms may be sufficient to resolve goal conflicts. Second, a formal structure promoting anchored personalization may not be necessary in organizations characterized by high levels of informal structure such that there are preexisting personalized relationships and friendships across groups outside of work. But given the consolidated demographics between most occupational and professional groups, in which professional group members often share the same salient demographic attributes such as race, gender, and class (Baron and Bielby, 1985; DiBenigno and Kellogg, 2014), and given extensive homophily in friendship networks (e.g., McPherson, Smith-Lovin, and Cook, 2001; Reagans, 2011), such cross-professional friendships may be less likely to spontaneously occur without a formal structural intervention. Finally, consideration should be given to the tradeoffs associated with an anchored personalization structure, given efficiency losses from assigning points of contact relative to operating in a pooling structure in which anyone can work with anyone, which is less sensitive to asymmetries in demand for services. Under conditions of intractable identity conflict, however, these losses may be offset by effectiveness gains.
Given the rise of professional groups working inside organizations with strong commitments to their professional identities and perspectives, including diversity managers, safety managers, and cyber security professionals to name a few, it is likely that many organizations face difficulties aligning the goals of different professional groups. For example, Nike hired an influx of sustainability officer professionals in an effort to improve the environmental and social impact of its products, but this new professional group faced conflict with apparel designers, a group with different goals and identities as well as higher status in the organization (Kaul et al., 2015). An organizational structure that fosters personalized relations between these two groups while ensuring anchoring in their home group’s identity—perhaps by assigning sustainability officers to specific design departments, but not embedding them within those departments—might enable anchored personalization practices so they could co-construct integrative solutions that would result in both more sustainable and fashionable products.
Future research is needed to test and refine this new concept of anchored personalization in other settings with different groups. First, other organizational contexts may require different structural affordances to promote anchored personalization practices. For example, regulators of big banks may need more anchoring, given the well-known revolving door (e.g., Katic and Kim, 2013). Second, the professional groups studied here differ in terms of power. Commanders are more powerful than mental health providers because they can override many of the providers’ recommendations. This may explain why providers expressed concerns about cooptation by commanders but not vice versa, and it highlights the especially important role of anchoring for the less powerful group. Future research is needed to understand dynamics between equally powerful groups. Finally, although the anchored personalization structure afforded an opportunity for a personalized relationship to develop between assigned providers and commanders, it did not guarantee it. Future research could unpack how personalized cross-group relationships are built and maintained over time. As organizations continue to employ professional groups, it is more important than ever to understand how such groups can overcome goal and identity conflict to accomplish overarching organizational goals.
Footnotes
Acknowledgements
This research benefited from the generous feedback and guidance of Kate Kellogg, Lotte Bailyn, Ezra Zuckerman, John Van Maanen, John Carroll, Amy Wrzesniewski, Caroline Bartel, Michel Anteby, Cat Turco, Lakshmi Ramarajan, Jennifer Petriglieri, Mike Pratt, Mabel Abraham, Aruna Ranganathan, Curtis Chan, Emily Truelove, Tiona Zuzul, Anoop Menon, Jillian Chown, and Luciana Silvestri. I received valuable comments from participants in the MIT Economic Sociology Working Group, Craft of Qualitative Inductive Research seminar, Work, Identity, and Meaning group, the 2015 INFORMS dissertation competition, and seminar attendees at Yale SOM, Cornell, HBS, Kellogg, BC, UT Austin, University of Michigan, LBS, University of Oregon, and Purdue. I also thank Forrest Briscoe and three anonymous reviewers for improving the paper during the review process, as well as Linda Johanson and Joan Friedman for expert copy editing. I am especially grateful for the support of Jayakanth Srinivasan on all stages of this research, as well as the soldiers, mental health providers, commanders, and Behavioral Health leadership who made this study possible. This study was supported by grant cooperative agreement W81XWH-12-2-0016. The views and conclusions contained herein are those of the author and do not necessarily reflect the views of the U.S. government or U.S. Army.
1
I chose to conduct in-depth interviews with subunit commanders, as non-field-grade officers, rather than unit commanders or brigade commanders because they had the most interaction with mental health providers around the care of their soldiers. They were the only level of command that could provide a detailed account of interactions with mental health providers on specific soldiers’ cases given that these higher levels of command were more removed from day-to-day issues and given the sheer number of soldiers in their units (600 soldiers in a unit versus 100 in a subunit).
2
Mental health services were referred to as “behavioral” health services in the army. For ease of reading and given that providers only provided mental health services, “behavioral” has been changed to “mental” throughout.
3
Although certain integration mechanisms described in the literature were not present in this context, their absence was consistent across all clinics and brigades. For example, there were low levels of organizational slack at this and all army posts given longstanding shortages of soldiers and reductions in the size of the force since 2013. See ![]() for more detail.
for more detail.
4
Soldiers in all clinics and brigades saw the same provider for the duration of their time in treatment.
5
6
Concerns about cooptation were not an issue for the commanders because they were the more dominant group and engaging with mental health providers was only a very small component of their overall jobs. No commander, even those with the closest personalized relations with their assigned mental health provider, reported concerns about cooptation or was accused of cooptation by other commanders.
Author’s Biography
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.