
Abstract
This article compares how having a child with special needs shapes the labour market adaptations of immigrant and majority mothers. We use longitudinal data from Norwegian public registers including all women who gave birth between 2001 and 2005 (N = 104,988), and follow the mothers from two years before birth to four years after birth. We find generally large differences in employment and income among immigrant and majority mothers. Majority mothers typically adapt to the intensified care responsibilities associated with having a child with special needs by working somewhat less, but most importantly by combining work with high levels of long-term sickness absence. By contrast, immigrant mothers substantially reduce their work intensity (as measured through labour earnings) after childbirth regardless of whether their child has special needs. Among immigrant mothers whose child has special needs, we do not find elevated sickness absence levels comparable to that of majority mothers. Given the already reduced work intensity among immigrant mothers in the years following the birth of their child, we do not find additional labour market consequences of intensified care responsibilities within this group of mothers.
Keywords
Introduction
Studies consistently find that having children impairs women’s attachments to the labour market. Care responsibilities in the family fall on women more than men, leading them to adapt their work ambitions and investments to the needs of the family (Blair-Loy, 2003; Halrynjo and Lyng, 2009). However, how women’s employment is affected by the advent of children differs significantly between groups and between national contexts.
The so-called motherhood penalty on employment is smaller in Norway, and the other Nordic countries, than in other national contexts (Cools and Strøm, 2016; Harkness and Waldfogel, 2003). These countries have high female labour market participation, including mothers of young children, often seen as an outcome of a strong gender equality ideology and institutional arrangements that facilitate the combination of care responsibilities and participation in paid work for women. However, there are large differences between different types of families, and some immigrant groups appear particularly gendered in their adaptations between work and care, with very low employment rates for women (Kavli and Nicolaisen, 2016).
The work–care adaptations of families with intensified care responsibilities are particularly interesting, as they represent a case with an increased conflict between work and care. This article examines how having a child with special needs affects the employment of different groups of mothers, more specifically examining how majority and immigrant mothers adapt to intensified care responsibilities.
Taking care of a child with special needs can be rewarding and many parents feel enriched by their experience despite challenging situations (Kearney and Griffin, 2001). However, caring for a child with special needs may be demanding in terms of both time and resources. Not only because of the intensified need for caregiving, but also because parents of children with special needs often have to struggle to gain access to health services and support arrangements needed (DeRigne, 2012; Eriksen, 2003). At the same time, the impact of having a child with special needs on maternal employment may also vary with the characteristics of the mother. Previous research has, for instance, found stronger effects for less educated women (Wasi et al., 2012).
To date, we have little knowledge about how intensified care responsibilities might shape the labour market adaptations of immigrant and majority mothers differently. Immigrant families tend to have more gender-complementary cultural understandings of gender, parenting and care than non-immigrant families (cf. Kavli, 2015), they often have more vulnerable attachments to the labour market (Revold, 2017) and they may meet special challenges due to communication problems and lack of information about the welfare system (Berg, 2015). These factors are often highlighted as having negative consequences for the maternal employment of immigrant women, and we hypothesize that they may intensify when having a child with special needs. At the same time, immigrant mothers who do work are likely to be more strongly selected into the labour market than working majority mothers. It is, therefore, not clear what we should expect with regard to other forms of work adaptations, such as career adjustments or sickness absence across the two groups.
We address this issue by examining the following question: how do patterns of labour market adaptation among mothers caring for a child with special needs differ for mothers with majority and immigrant background? As a generous welfare state that aims to facilitate the combination of paid work and care responsibilities, Norway represents an interesting case for studying the differing effect of intensified care responsibilities on mothers’ labour market attachment.
In a recent review article, Brown and Clark (2017) conclude that there is a need for more research on work and family life balance in families with disabled children using longitudinal data. To our knowledge, this is the first panel data study on the employment consequences of having a child with special needs where majority–immigrant differences are examined. Longitudinal information on the mothers prior to and after having a child allows for analyses of the effect of having a child with special needs on labour market outcomes and long-term sickness absence over time. The large number of cases in our sample makes it possible to compare immigrant mothers and non-immigrant mothers. Thus, our study contributes to knowledge about mothers’ adaptations to paid work in a welfare state that actively promotes employment among mothers of young children, and supports families with intensified care needs. In particular, we are examining labour market adaptations across different groups of mothers of children with intensified care needs, discussing possible explanations for the similarities and differences that we find.
Previous research on labour market attachment among mothers of children with special needs
It is a consistent finding that women experience a negative career effect of having children (Cools et al., 2017; Gangl and Ziefle, 2009). Having a child with special needs further affects mothers’ labour market attachment. A number of international studies show associations between children’s care needs and reduced maternal employment rates, and more mothers working part-time (DeRigne, 2012; Gordon et al., 2007; Hope et al., 2017; Lu and Zuo, 2010; Seltzer et al., 2001).
While a few studies from Norway found that mothers of children with severe healthcare needs are at risk of being out of paid employment when the child is three years old (Hauge et al., 2013; Tøssebro and Paulsen, 2014), another longitudinal study found that mothers caring for children with special needs do not retract from work, but rather scale back their participation in paid work when the children are young, and they have higher sickness absence compared to mothers in general (Brekke and Nadim, 2017). Another Norwegian study also reports higher sickness absence among parents caring for a child with a disability compared to other parents (Wendelborg and Tøssebro, 2016). Moreover, a study from Australia (Dillon-Wallace et al., 2016) reports no significant difference in the occupational status of mothers who had children with special healthcare needs and mothers whose children did not have special healthcare needs. A recent review article examines work and family balance among parents caring for disabled children and concludes that individual factors such as child age, number of children, childcare availability, perception of work role and type and severity of child’s diagnosis impact parental work and family balance (Brown and Clark, 2017).
Although research on how different types of families adapt to increased care responsibilities is scarce, some studies suggest that the labour market attachment of ethnic minority women is particularly affected by the advent of a child with special needs. Yu and Singh (2009) found that households in the US where English was not a primary language were almost twice as likely to stop employment as a result of the child’s condition than were households where English was the primary language. Similarly, in an older study, Breslau et al. (1982) found that mothers of chronically ill children in the US were less likely to work compared with mothers of healthy children, but that this was particularly the case for lower income and ethnic minority families.
Theoretical framework: cultural differences, opportunity structures and immigrant-specific challenges
There are theoretical reasons to expect differences in labour market adaptations among immigrant and majority mothers of children with special needs. In this section, we explore the relevance of three main types of explanations, emphasizing cultural differences, opportunity structures and immigrant-specific challenges.
Cultural differences between majority and immigrant families may affect the general labour market attachment of mothers of young children, and this tendency may be intensified when the children have special needs. Hakim’s (2002) preference theory emphasizes the role of individual preferences and choice in determining women’s attachment to work. Hakim argues that the vast majority of women in Western societies have genuine opportunities to choose how they wish to balance family and work, and preference theory sees women’s attachment of work primarily as a result of individual choices based on (gender-specific) lifestyle choices.
The male breadwinner model is relatively weak in the Norwegian context, although women adjust their labour market participation according to the needs of the family more than men do (Aboim, 2010; Halrynjo and Lyng, 2009). At the same time, it is the dominant model in many of the immigrant-sending countries to Norway, such as Pakistan, Somalia and Iraq. In the period 2001–2005 (covering the relevant birth cohorts in our study), 47 percent of immigrant women in Norway originated from Asia (including Turkey) Africa, and South and Central America, while 12 percent were from European countries outside EU28/EEC (Statistics Norway, 2001–2005). In some of these immigrant groups, gender-complementary practices and ideals are clearly present also long after migration (Kavli, 2015; Kavli and Nadim, 2009). Having a child with special needs might reinforce gendered adaptations to work and care, especially in families where gender-complementary practices and ideals were already strong.
Hakim’s perspective has been widely criticized, in particular for over-emphasising free choice and neglecting more structural constraints on women’s employment. McRae (2003) emphasizes a range of institutional factors that can shape women’s employment such as the scarcity of childcare arrangements, availability and security of jobs, financial resources and work–family policies.
This perspective underlines how families’ work and care decisions are not only shaped by their cultural understandings, but they are also affected by the families’ opportunity structures in the labour market. Although there are significant variations between immigrant groups, immigrant women generally have a weaker and more unstable attachment to the labour market than non-immigrants, and those immigrants who are employed are more likely to be working in unskilled jobs (Revold, 2017). This can, for several reasons, impact the effect of having a child with special needs on labour market participation. First, conflicts between work and care obligations may be more pronounced because this type of work often does not allow for flexibility and/or regular absences. Children with special needs regularly need specialized medical care, often from many providers (Drummond et al., 2012). Thus, a flexible work situation is essential for the parents to be able to follow up the child’s medical care. Second, socioeconomic status is found to influence the health effect of caring for children with special needs. Skreden (2011) finds that low-educated mothers and fathers who were either unemployed or on welfare had an increased risk of mental health problems following the birth of a child with special healthcare needs. Higher-status employment can give psychological rewards for parents of children with special needs even when it does not increase the family’s net income, as it can be a motivating and health-promoting factor for the individual (Breslau et al., 1982). Because some groups of immigrants are disproportionately represented in low-skilled parts of the labour market, these dynamics may have particular effects on immigrant families with children with special needs.
Finally, immigrant mothers may experience immigrant-specific challenges related to having a child with special needs. Limited knowledge about welfare services, language barriers and limited social networks represent additional challenges for immigrant families that can make everyday life even more challenging than for majority families (Berg, 2015). In a qualitative study of immigrant parents caring for a child with special needs in Norway, Früh et al. (2016) point out that immigrant parents struggle to get access to the benefits and services they are entitled to, because of language barriers and limited knowledge of the Norwegian welfare system. Moreover, the study shows that the mothers’ motivation for participating in paid work is high, but that limited relevant education and work experience, in addition to language problems, impair job opportunities.
These three types of explanations are not competing, and may all contribute to influencing the labour market adaptations of majority and immigrant mothers of children with special needs. In the present study, we focus on three labour market outcomes: employment, labour earnings and long-term sickness absence. The three outcomes reflect different aspects of labour market adaptation. Based on the theoretical framework we have presented in this section, we hypothesize that immigrant mothers who care for a child with special needs will be more severely affected than majority mothers, particularly by reducing their participation in paid work.
The Norwegian context for work and care
The Norwegian welfare state aims to facilitate employment among mothers of young children by offering a generous parental leave scheme and state-sponsored, widely available, high-quality childcare services. Moreover, Norway ranks among the top five Organization for Economic Cooperation and Development (OECD) countries on female employment (OECD, 2017). However, immigrant women have lower employment rates than majority women, and some large immigrant groups, like immigrants from Pakistan and Somalia, have very low female employment rates (Nadim and Fjell, 2019; Østby, 2013).
The Norwegian family policy program also provides cash-for-care benefit (‘kontantstøtte’), which is granted for children between one and two years of age. Contrary to the aim of facilitating employment among mothers of young children, a Norwegian study reports that the cash-for-care reform has affected mothers’ labour market participation negatively, and the effects are stronger for non-Western immigrant mothers than for majority mothers (Hardoy and Schøne, 2010).
Another relevant feature of the Norwegian welfare state is the generous sickness benefit system that entitles workers to receive sick pay from the first day of sickness, if they have been employed for at least four weeks. The sickness benefit is fully wage-compensated up to a set threshold. Employers are responsible for sick pay for the first 16 consecutive days, but after this period, sick pay is fully financed and administered by the Norwegian Labour and Welfare administration (NAV) for up to one year.
Care for people with special needs has largely been deinstitutionalized and transferred to the family, with a range of services and types of assistance available from public agencies, as well as various forms of monetary transfers. Generally, monetary transfers are administered by NAV, while municipal or local welfare agencies provide practical assistance such as respite services, support assistance, personal assistance and short-term institutional care. Family members may also receive a care wage for extraordinary care work due to disability or long-term illness (Eriksen, 2003). All individuals who suffer from a long-term illness and have a lasting need for care or personal nursing may be entitled to attendance benefits. The application form needs to specify the private care arrangements taken to cope with the child’s increased care needs. All families living in Norway are equally entitled to the benefits of the system, and the overall workload of the person providing care or supervision is the determining factor (independent of other incomes). The attendance benefit is paid at four different rates, reflecting mild to severe care needs and ranging from €123 up to €737 per month (NAV, 2018).
Data and methods
Data
The data comes from the Historical Event Database (FD-Trygd) compiled by Statistics Norway. The FD-Trygd panel database contains information on country of origin, age, labour market outcomes and welfare benefits for all individuals in Norway. Many disorders are not detected at birth, and chronic illness and disabilities may also appear after birth. Therefore, we use information on attendance benefits derived from FD-Trygd to identify children with special needs. There are potential challenges related to using attendance benefits to identify children with special needs. However, Wendelborg and Tøssebro (2010: 5) report that 91 percent of the surveyed parents that cared for a disabled child received attendance benefits. This is an indication that the use of attendance benefits is appropriate to identify families that care for a child with special needs. The sample in the present study contains all women (N = 104,988) 1 who gave birth in Norway in the period between 2001 and 2005. For all the mothers, we have panel information for the period from two years prior to birth to four years after birth.
Statistical models
We examine the effect of having a child with special needs on employment, labour earnings and long-term sick leave in the period from two years prior to birth to four years after birth, comparing immigrant and majority mothers. We include a three-way interaction term between the dummy variable children with special needs (SNC), the time dummies and the dummy for immigrant versus majority. These coefficients tell us how the difference between having a child with special needs and having a child without special needs develops over time, relative to a reference period. The analyses of employment are performed using a linear probability model (LPM) – that is, linear regressions on a binary variable. Logistic regression is often used when the outcome variable is binary. However, the coefficients in logistic regression not only reflect the effect of the independent variables but also the size of the unobserved heterogeneity, and, therefore, it is problematic to compare coefficients across samples (Mood, 2010). For that reason, we compute an LPM. This gives results in terms of changes in probability. The second dependent variable is the logarithm of labour earnings. Ordinary linear regression is used. Sickness absences are analysed using negative binomial regression. Negative binomial regression is used to analyse count variables with overdispersion. In our case, the long-term sickness absence outcome variable is overdispersed because a large number of individuals in our sample have no long-term sickness absence in the analysis period. The models estimated in the analyses of all three outcomes include the same independent variables. All results are presented as predicted margins, evaluated at the mean of the explanatory variables.
Variable definitions
We examine three outcome variables: employment, annual earnings and long-term sickness absence. Information on employment and earnings is based on employers’ reports to the mandatory national insurance scheme. Employment is coded 1 if the individual was working or registered as attempting to work, and 0 otherwise. The mothers are classified as employed if they worked at all as paid employees or were self-employed during the reference week, or if they were involved in any job-seeking or job-training program. We argue that mothers who are registered as actively seeking a job are different from mothers who are registered as outside the labour market. Mothers who are seeking a job or are in job training are typically close to employment, and thus have more in common with employed mothers than mothers registered as outside the labour market. Annual earnings covers all income from gainful employment (capital income and transfers not included). Amounts are adjusted according to the consumer price index. A logarithmic transformation is used to ensure a more normal distribution of the outcome variable. For the third dependent variable, long-term sickness absence, we use a duration measure of sickness absence (number of days). We analyse long-term sickness absence, since the register data include sickness absences of 17 days or longer.
We include a number of independent variables in our analysis model. Immigrant background is measured as a categorical variable, distinguishing between mothers born abroad and mothers who are born in Norway to majority parents. 2 The main independent variable is having a child with special needs (SNC). The variable is measured by a dummy variable, taking the value 1 if the child has special needs and 0 if the child does not have any special needs. Children who were granted attendance benefit at any time during the four years after birth that we measure, were classified as children with special needs. For some of these children the special needs might appear during the observation period, as certain diagnoses are not detected at birth but diagnosed later. However, to receive attendance benefit, the care needs must last for two to three years or more – in other words, a chronic condition. It is, therefore, likely that most of the children defined as children with special needs in the present sample have had special needs from a very young age. Age of the mothers is measured as a continuous variable in years. We also include a quadratic term to allow for non-linear associations between age and the outcome variables. Educational level is divided into four levels: compulsory school or lower, upper secondary school, bachelor’s level and master’s level and PhD. Compulsory school or lower is the omitted category. Some mothers did not have information about completed educational level. In the majority population, this is very rare (762 individuals in the original sample), and strongly associated with teenage pregnancies (median age at birth was 16). These mothers were excluded from the analyses. In the immigrant population, missing educational information in Norwegian registries means that the relevant individuals completed their education abroad or in their home country before migrating, and did not complete additional education in Norway. This means that we do not know their level of education. Some 34 percent of the immigrant sample had no registered education completed in Norway. Given that this is such a large part of the sample, the dummy variable completed education abroad is included as a separate category. 3 Unemployment rate in the local labour market (county) is measured each year. In cases where county of residence was missing in some of the years, we replaced the missing information with information about the individual’s county of residence from the adjacent year. We control for region of origin, to distinguish between individuals with Western and non-Western immigrant backgrounds. We also control for birth cohorts of the children. In addition to these variables, we include some control variables based on information about the child’s biological father. We include father’s immigrant status, father’s region of (parental) origin and father’s income. In cases where there was a father present in the data, but information was missing for father’s income in some of the years, we replaced father’s missing income with the reported income from the adjacent year. In order for the analyses to be comparable across models, all cases that were listwise deleted when controls were added, were completely removed from the analyses. This pertained to 3.4 percent of the total sample.
To be included in the analyses of labour earnings and sickness absence, we require that the mothers are employed or in any job-seeking or job-training program in the reference week. We include job seeking and training because it manifests a commitment to being in the labour force, and it also significantly increases the likelihood that the mothers had some form of employment during the year in question, despite being unemployed during the reference week.
There are methodological challenges related to studying the effects of having a child with special needs. The mothers may have unobserved characteristics that affect both employment and sickness absence, and the likelihood of having a child with special needs (Stabile and Allin, 2012). However, since we have longitudinal data for the outcome variables two years prior to and four years after the child was born, we can compare pre-trends in the outcome variables between the two groups of mothers. If the pre-trends are comparable in the two groups, we can assume that differences between the two groups after the child was born are caused by having a child with special needs. Another challenge in our data is that we operationalize having a child with special needs through the registration of monetary transfers to the family. This means that the family must have sufficient knowledge of the Norwegian welfare system to be able to apply for, and be successful at receiving, public assistance. Therefore, we assume that we are underestimating the effect of having a child with special needs on employment-related outcomes, especially for newly arrived immigrants.
Results
Descriptive statistics: comparing immigrant and majority mothers
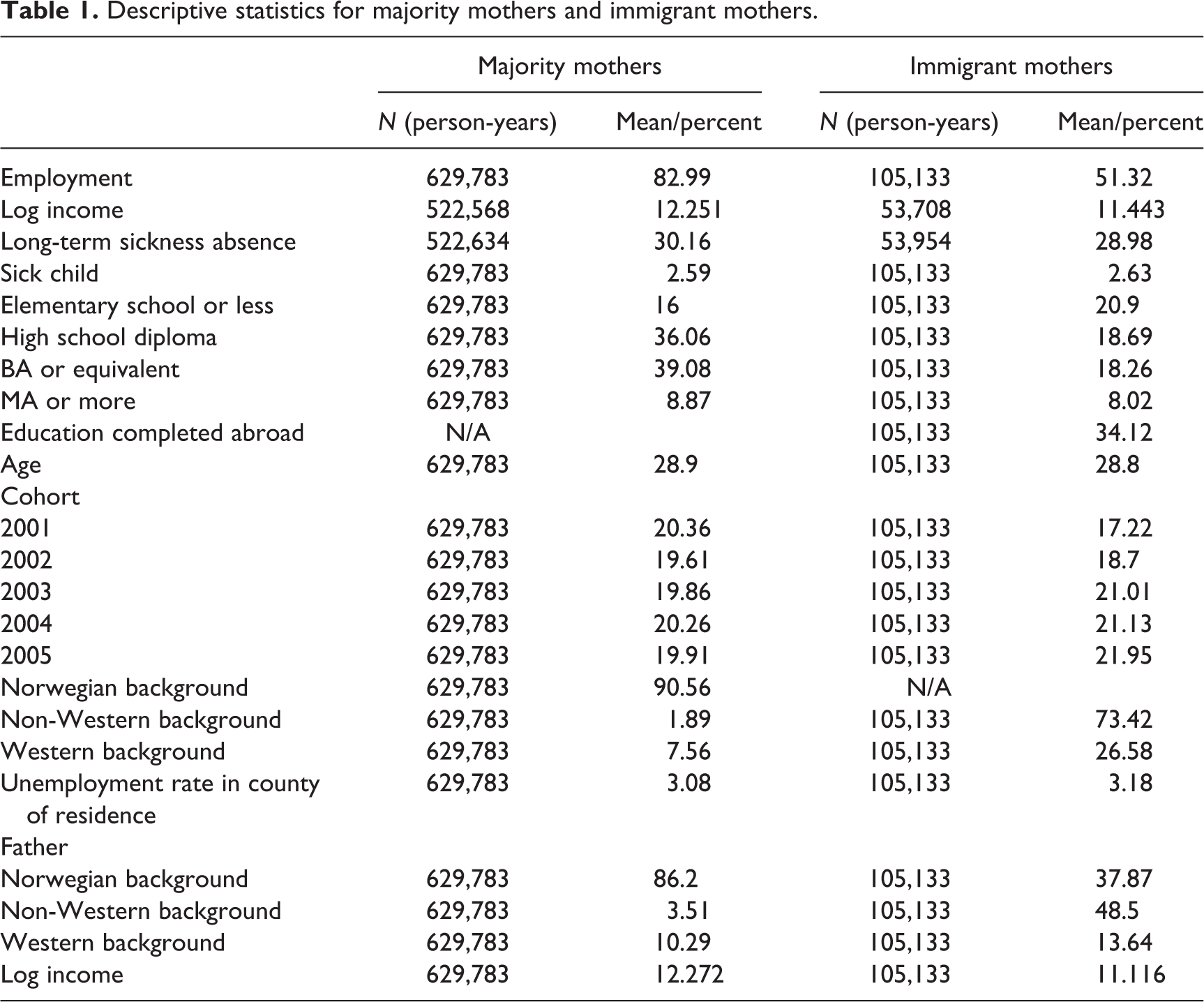
Descriptive statistics for the two populations show large discrepancies in labour market participation and income between majority and immigrant mothers (Table 1). Whereas on average 83 percent of the majority origin mothers work, this only applies to 51 percent of the immigrant mothers, averaged over the seven years we observe the mothers in our data (two years before and four years after the year they gave birth). The differences in log income between the two groups of working mothers is quite substantial. Transformed from the log scale back to Norwegian Kroner (NOK), the average income for majority mothers over the observation period is 209,190 NOK, whereas the average income among immigrant mothers is as low as 93,246 NOK. This means that, on average, majority mothers (who work) earn more than double the annual amount compared to immigrant mothers in the years surrounding the birth of their child. There is much less variation in sickness absence across the two groups, averaging at 30 days for majority mothers and 29 days for immigrant mothers. The share of children with special needs is identical across the two groups, at 2.6 percent. About 27 percent of the immigrant mothers have moved to Norway from other Western countries. As expected, the children’s fathers (most often the mother’s spouse or partner) have lower incomes and are much more likely to be immigrants if the mothers are immigrants.
Descriptive statistics for majority mothers and immigrant mothers.
Multivariate analyses
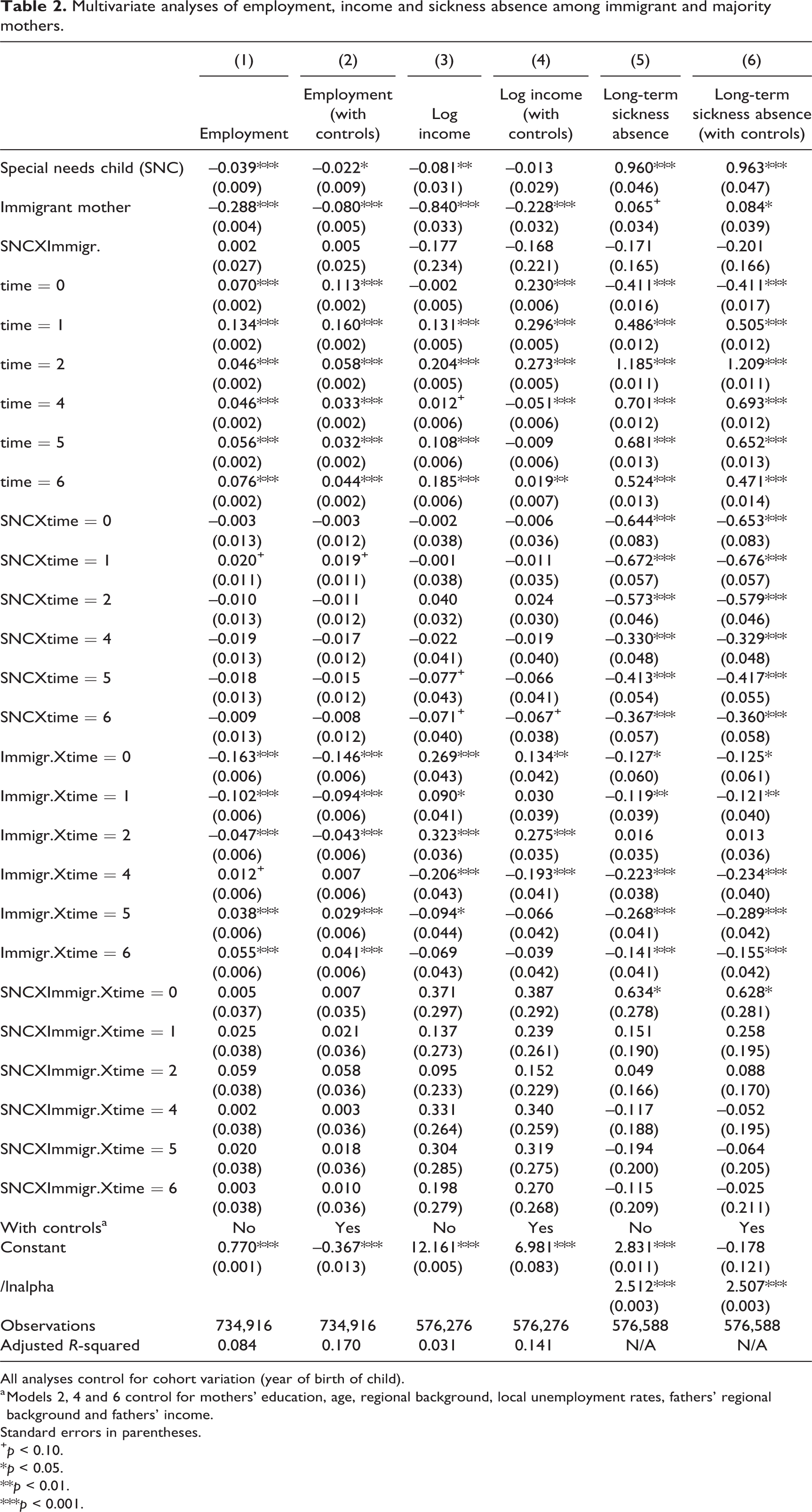
The analyses investigate whether there are systematic differences in employment, labour income and long-term sickness absence among immigrant and majority mothers prior to and after giving birth to a chid with special needs. The results from the multivariate analysis are presented in Figures 1 and 2. First, we present the estimates without controlling for potential confounders (Figure 1). Second, we control for age, education, region of origin, unemployment rate in county of residence, as well as the child’s father’s region of origin and income (Figure 2). The multivariate analyses are presented in Appendix 1.
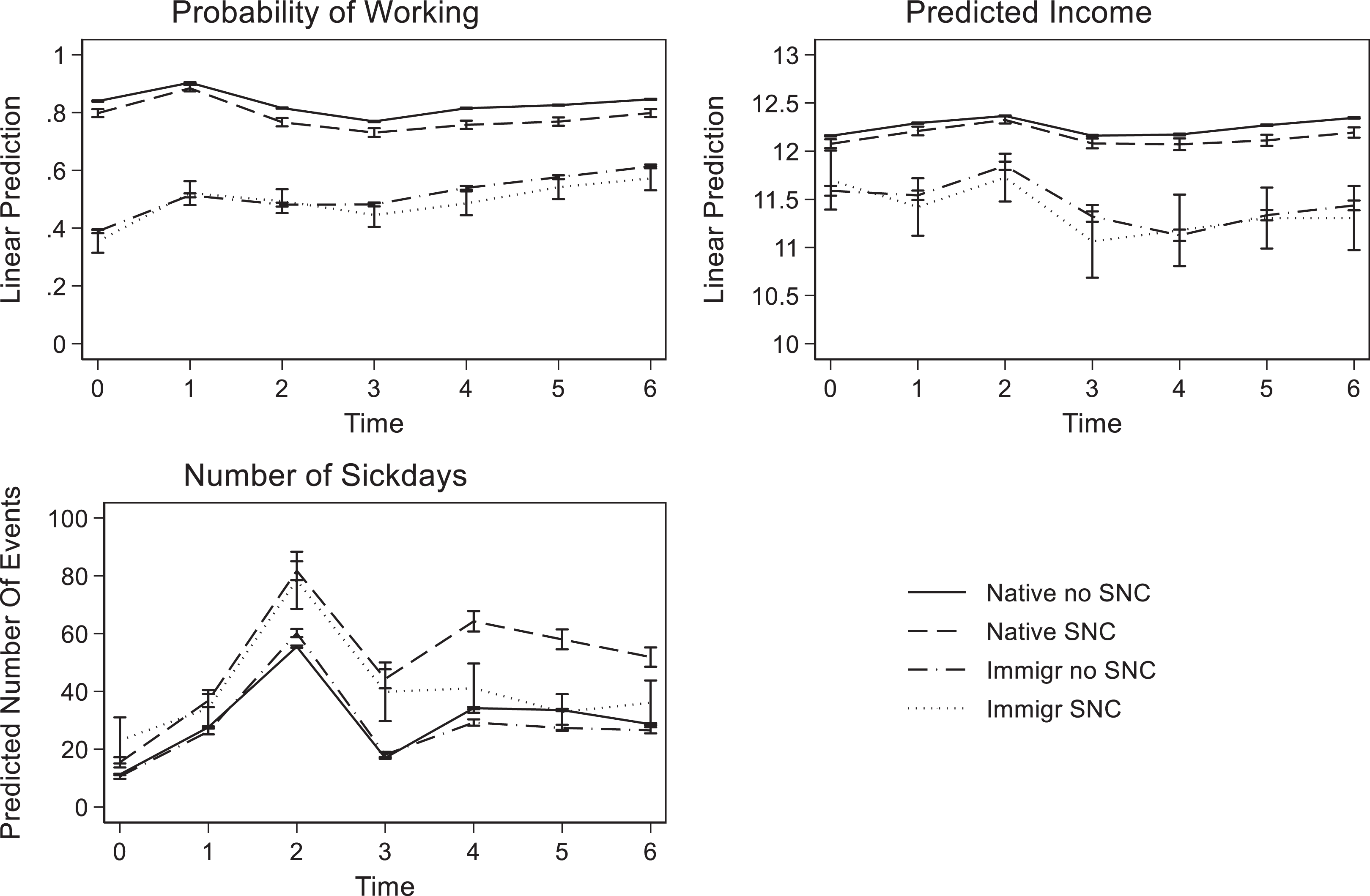
Employment, income and sickness absence among immigrant and majority mothers by child’s healthcare needs (90% confidence intervals).
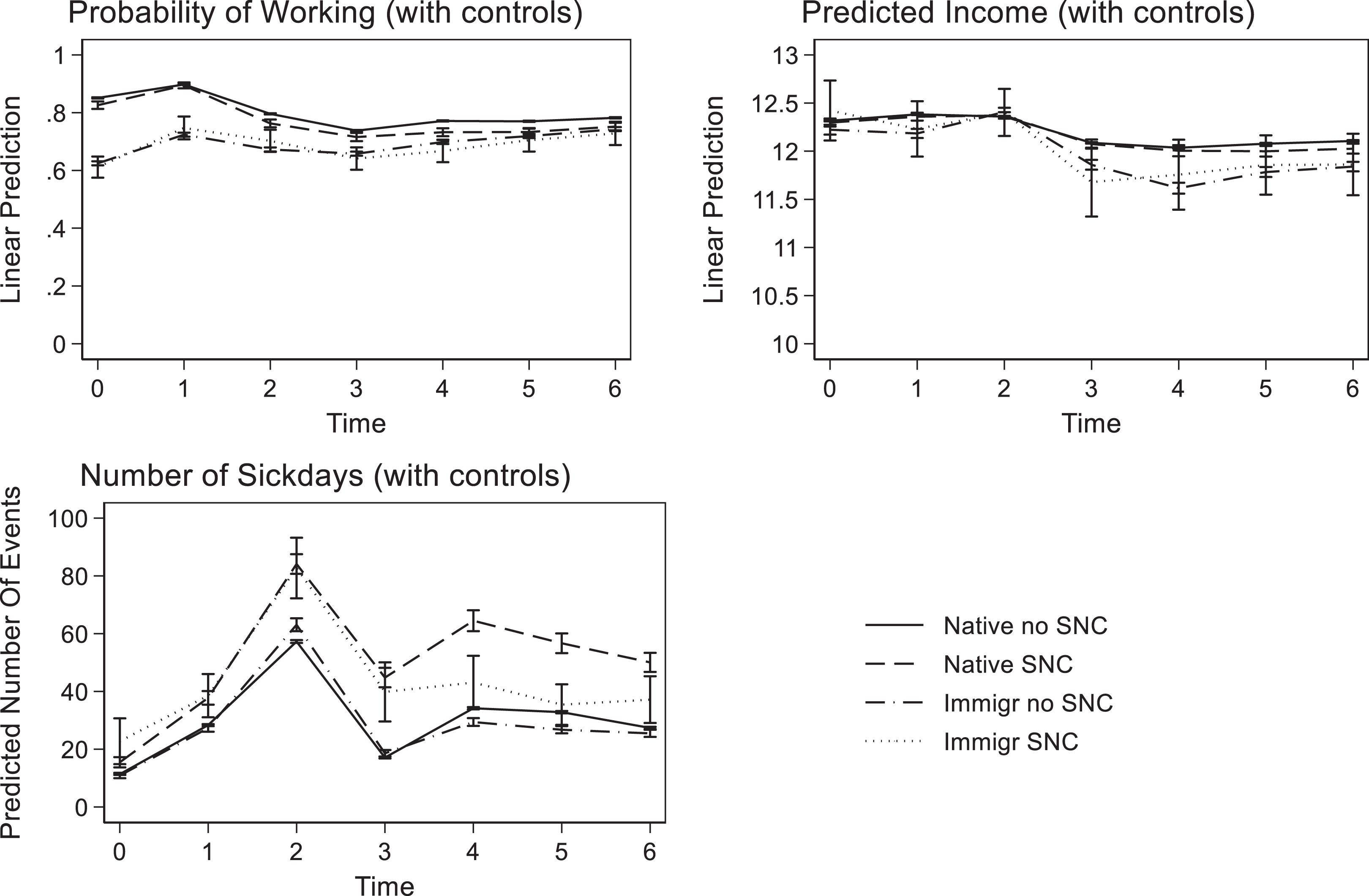
Employment, income and sickness absence among immigrant and majority mothers by child’s healthcare needs, net of potential confounders (90% confidence intervals).
Employment
The analysis of employment shows that both immigrant and majority mothers of children with special needs reduce their labour market participation significantly more than mothers of children who do not have such intensified care needs. However, the differences are small. For both immigrant and majority mothers, the difference amounts to 3.9 percentage points the year after birth, which is a magnitude slightly larger than the average unemployment rate in the country (Appendix 1, Table 2: Model 1). The difference in labour market participation between mothers of a child with special needs and mothers of a child without special needs is relatively stable over the four years after birth for majority mothers. Immigrant mothers have considerably lower probability of labour market participation, regardless of their children’s care needs (–29 percentage points (b = –0.288) for mothers of children without special needs one year after birth). Four years after birth, however, the employment level of immigrant mothers of children without special needs is higher than the pre-birth level (but still much lower than that of majority mothers), and the difference in employment between immigrant mothers of children with special needs and children without special needs is small and does not reach statistical significance.
Labour income
Among those who work, variation in predicted income indicates whether the mothers are able to make labour market advances and also reflects the time they are able to invest in the labour market. Lower incomes after birth, compared to before birth, may indicate reduced work hours or changes in career paths to adjust to family demands. In the analysis of income, we see that the incomes among immigrant mothers are considerably lower than majority mothers one year after the birth of their child (57 percent, b = –0.840), 4 and immigrant mothers’ incomes fall more after birth than majority mothers’ incomes. The gap remains wider than before birth throughout the observation period. After the children are born, majority mothers caring for children with special needs have somewhat lower incomes than majority mothers caring for children without special needs, and this gap seems to widen over time in the four years after birth. At the end of the observation period, majority mothers of children with special needs earn 14 percent less than majority mothers of children without special needs. The results indicate that immigrant mothers caring for children without special needs already have low labour market participation and adjust their working situation more after the birth of their child than majority mothers; hence, the difference between immigrant mothers of children without special needs and immigrant mothers of children with special needs is small and statistically insignificant.
Long-term sickness absence
The analysis of long-term sickness absence indicates that both immigrant mothers and majority mothers who gave birth to children with special needs had longer periods of sick leave in the birth year and for some time after. However, the sickness absence of immigrant mothers of children with special needs goes down over time, and by the third year after birth it is level with majority mothers of children without special needs (33 days). By contrast, long-term sickness absence remains high among majority mothers of children with special needs throughout the four years post-birth we observe (averaging 26 days higher than majority mothers without children with special needs).
Adjusting for potential confounders
The variation between these groups of mothers could be explained by group differences in age, education level or other confounders. As expected, the group differences are significantly reduced when we compare mothers who are more similar with regard to these key characteristics. However, some differences remain. Majority mothers of children without special needs are more likely to work than otherwise similar mothers of children with special needs, from the birth-year and for the duration of our period of observation. When comparing mothers with similar characteristics, the employment gap between majority and immigrant mothers shrinks to only eight percentage points the year after birth. Moreover, immigrant mothers reduce their labour market participation similarly after giving birth, regardless of their child’s healthcare needs. However, immigrant mothers’ employment increases more sharply in the four years following the birth of their child than it does for majority mothers, and the development is similar for immigrant mothers of children with special needs.
Predicted income among those who work, net of controls for confounding variables, show that incomes of otherwise similar majority mothers do not differ with the health status of their child one year after birth. However, majority mothers of children with special needs earn significantly less than majority mothers of children without special needs towards the end of the observation period (diff = –7.7 percent in year 6). Immigrant mothers of children without special needs earn significantly less than similar majority mothers, from the first year after birth and for the remainder of the four-year observation period after birth (26 percent less on average). The income trajectories of immigrant mothers of children with special needs are, overall, very similar to the patterns for immigrant mothers of children without special needs.
In contrast to the analyses of employment and income, the multivariate analyses of long-term sickness absence show that the patterns from Figure 1 are quite robust to the inclusion of potential confounders. This indicates that changes in labour market participation and income are more sensitive to the mothers’ individual characteristics than long-term sickness absence patterns among the mothers who work. According to these analyses, the most substantial difference between immigrant and majority mothers of children with special needs can be found in their rates of sickness absence, where majority mothers seem to maintain much higher rates of sickness absence over time compared to otherwise similar immigrant mothers. Although immigrant mothers work less than majority mothers, and adjust their labour market participation more after the birth of their child, these differences are reduced once we control for confounding factors such as education, place of residence, age and characteristics of the father. Thus, it seems that the variation in sickness absence between majority and immigrant mothers caring for children with special needs cannot be fully explained by their selection into or out of the labour market as a response to having a child with special needs.
Discussion and conclusion
The aim of this study has been to examine differences between majority and immigrant mothers’ labour market adaptations to intensified care responsibilities in terms of having a child with special needs. We hypothesized that immigrant mothers’ employment is more negatively affected than that of majority mothers due to more complementary gender norms and practices, a weaker attachment to the labour market, less flexible work situation and limited knowledge about the support arrangements that are available. Using longitudinal data with information on labour market participation prior to and after birth for both immigrant and majority mothers, we have been able to examine this question.
We find that immigrant mothers generally differ from majority mothers in terms of their employment probability and income. Majority mothers are more likely to be employed, they earn more, but also take out slightly more sick days than immigrant mothers.
When we control for a number of characteristics that may explain the general differences between the two groups of mothers, we find that even when immigrant and majority mothers are similar prior to the birth of their child, their labour market trajectories differ after the child is born. Regardless of whether the child has special needs, immigrant mothers reduce their labour earnings significantly after the birth of their child, and much more so than majority mothers. Although we found small differences in the probability of being employed towards the end of the observation period, we found that having a child with special needs significantly impairs maternal employment for majority women.
Moreover, majority mothers of children with special needs earn significantly less than majority mothers of children without special needs towards the end of the observation period, indicating that they reduce their time spent in paid labour and/or have weaker career advancement. By contrast, the income trajectories of immigrant mothers of children with special needs are very similar to the patterns for immigrant mothers of children without special needs, both being considerably lower than the pre-birth trend.
The results indicate that there is no additional labour earnings disadvantage among immigrant mothers of children with special needs relative to immigrant mothers of children without special needs. These results appear contrary to our initial theoretical assumption that having a child with special needs is of greater consequence for immigrant mothers than for majority mothers. One possible explanation is that immigrant mothers who were employed prior to the birth of their child are a selected group of women, given the low employment rates of immigrant women in the first place. Furthermore, both groups of immigrant mothers reduce the extent of their labour market attachment significantly after the birth of their child, indicating more substantial work–care adjustments among immigrant mothers, regardless of whether their child has special needs or not.
Also, differences in the sickness absence patterns indicate that majority and immigrant mothers do adapt somewhat differently to having a child with special needs. Our results show that majority mothers of children with special needs seem to hold on to their labour market position, while taking a high number of sick days. Immigrant mothers caring for children with special needs do not. By the time the child is four years old, immigrant mothers’ average number of sick days are the same, regardless of whether they have a child with special needs or not. Majority mothers caring for a child with special needs have substantially higher sickness absence compared to similar majority mothers with a child without special needs. The results suggest that majority mothers use sickness absence as a way of handling paid employment and intensified care, while immigrant mothers do not. This may have to do with their differential placement in the labour market, or with cultural differences with regard to the use of sickness absence as a means to handle challenging family situations. Unfortunately, we can only observe the discrepancies in sickness absence based on the data we have available for the analyses in this paper. Future research should investigate the mechanisms that contribute to this significantly different pattern of labour market adaptation among majority and immigrant mothers of children with special needs.
To conclude, we find that majority mothers typically adapt to the intensified care responsibilities associated with having a child with special needs by working somewhat less, but, most importantly, by combining work with high levels of long-term sickness absence. By contrast, immigrant mothers substantially reduce their work intensity (as measured through labour earnings) after childbirth, regardless of whether their child has special needs or not. In other words, immigrant mothers of children without special needs have the same low work intensity as immigrant mothers whose children have special needs in the years after childbirth. Thus, we do not find additional consequences of intensified care responsibilities among immigrant mothers.
We have pointed to cultural differences, differential opportunity structures in the labour market as well as immigrant-specific challenges as relevant factors shaping mothers’ labour market adaptations. Based on our findings in this paper, the immigrant-specific challenges seem to have the weakest explanatory power, given the absence of additional adverse labour market consequences of having a child with special needs among immigrant mothers. Rather, it seems that both labour market position and cultural differences may be at work for explaining the differential use of reduction in work intensity and sickness absence as strategies to manage intensified care responsibilities.
Our results indicate that the high female employment rates and strong emphasis on mothers’ employment characterizing the Norwegian welfare state are challenged when mothers are facing intensified care responsibilities. For immigrant mothers, who are generally much more inclined to reduce their labour market attachment after childbirth, intensified care responsibilities appear to be managed without additional employment adaptations. This might reflect a lack of opportunity to make further adaptations, and it might also indicate that working immigrant mothers are a selected group with strong work motivation. Either way, our results imply that the Norwegian welfare state context does not effectively eliminate differences between majority and immigrant mothers’ care and work adaptations.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Research Council of Norway, through the project ‘Ethnic differences in labour market participation, health and sickness absence among parents caring for disabled or chronically ill children’ (grant number 227022/H20).
Notes
Appendix 1
Multivariate analyses of employment, income and sickness absence among immigrant and majority mothers.
| (1) | (2) | (3) | (4) | (5) | (6) | |
|---|---|---|---|---|---|---|
| Employment | Employment (with controls) | Log income | Log income |
Long-term sickness absence | Long-term sickness absence |
|
| Special needs child (SNC) | –0.039*** | –0.022* | –0.081** | –0.013 | 0.960*** | 0.963*** |
| (0.009) | (0.009) | (0.031) | (0.029) | (0.046) | (0.047) | |
| Immigrant mother | –0.288*** | –0.080*** | –0.840*** | –0.228*** | 0.065+ | 0.084* |
| (0.004) | (0.005) | (0.033) | (0.032) | (0.034) | (0.039) | |
| SNCXImmigr. | 0.002 | 0.005 | –0.177 | –0.168 | –0.171 | –0.201 |
| (0.027) | (0.025) | (0.234) | (0.221) | (0.165) | (0.166) | |
| time = 0 | 0.070*** | 0.113*** | –0.002 | 0.230*** | –0.411*** | –0.411*** |
| (0.002) | (0.002) | (0.005) | (0.006) | (0.016) | (0.017) | |
| time = 1 | 0.134*** | 0.160*** | 0.131*** | 0.296*** | 0.486*** | 0.505*** |
| (0.002) | (0.002) | (0.005) | (0.005) | (0.012) | (0.012) | |
| time = 2 | 0.046*** | 0.058*** | 0.204*** | 0.273*** | 1.185*** | 1.209*** |
| (0.002) | (0.002) | (0.005) | (0.005) | (0.011) | (0.011) | |
| time = 4 | 0.046*** | 0.033*** | 0.012+ | –0.051*** | 0.701*** | 0.693*** |
| (0.002) | (0.002) | (0.006) | (0.006) | (0.012) | (0.012) | |
| time = 5 | 0.056*** | 0.032*** | 0.108*** | –0.009 | 0.681*** | 0.652*** |
| (0.002) | (0.002) | (0.006) | (0.006) | (0.013) | (0.013) | |
| time = 6 | 0.076*** | 0.044*** | 0.185*** | 0.019** | 0.524*** | 0.471*** |
| (0.002) | (0.002) | (0.006) | (0.007) | (0.013) | (0.014) | |
| SNCXtime = 0 | –0.003 | –0.003 | –0.002 | –0.006 | –0.644*** | –0.653*** |
| (0.013) | (0.012) | (0.038) | (0.036) | (0.083) | (0.083) | |
| SNCXtime = 1 | 0.020+ | 0.019+ | –0.001 | –0.011 | –0.672*** | –0.676*** |
| (0.011) | (0.011) | (0.038) | (0.035) | (0.057) | (0.057) | |
| SNCXtime = 2 | –0.010 | –0.011 | 0.040 | 0.024 | –0.573*** | –0.579*** |
| (0.013) | (0.012) | (0.032) | (0.030) | (0.046) | (0.046) | |
| SNCXtime = 4 | –0.019 | –0.017 | –0.022 | –0.019 | –0.330*** | –0.329*** |
| (0.013) | (0.012) | (0.041) | (0.040) | (0.048) | (0.048) | |
| SNCXtime = 5 | –0.018 | –0.015 | –0.077+ | –0.066 | –0.413*** | –0.417*** |
| (0.013) | (0.012) | (0.043) | (0.041) | (0.054) | (0.055) | |
| SNCXtime = 6 | –0.009 | –0.008 | –0.071+ | –0.067+ | –0.367*** | –0.360*** |
| (0.013) | (0.012) | (0.040) | (0.038) | (0.057) | (0.058) | |
| Immigr.Xtime = 0 | –0.163*** | –0.146*** | 0.269*** | 0.134** | –0.127* | –0.125* |
| (0.006) | (0.006) | (0.043) | (0.042) | (0.060) | (0.061) | |
| Immigr.Xtime = 1 | –0.102*** | –0.094*** | 0.090* | 0.030 | –0.119** | –0.121** |
| (0.006) | (0.006) | (0.041) | (0.039) | (0.039) | (0.040) | |
| Immigr.Xtime = 2 | –0.047*** | –0.043*** | 0.323*** | 0.275*** | 0.016 | 0.013 |
| (0.006) | (0.006) | (0.036) | (0.035) | (0.035) | (0.036) | |
| Immigr.Xtime = 4 | 0.012+ | 0.007 | –0.206*** | –0.193*** | –0.223*** | –0.234*** |
| (0.006) | (0.006) | (0.043) | (0.041) | (0.038) | (0.040) | |
| Immigr.Xtime = 5 | 0.038*** | 0.029*** | –0.094* | –0.066 | –0.268*** | –0.289*** |
| (0.006) | (0.006) | (0.044) | (0.042) | (0.041) | (0.042) | |
| Immigr.Xtime = 6 | 0.055*** | 0.041*** | –0.069 | –0.039 | –0.141*** | –0.155*** |
| (0.006) | (0.006) | (0.043) | (0.042) | (0.041) | (0.042) | |
| SNCXImmigr.Xtime = 0 | 0.005 | 0.007 | 0.371 | 0.387 | 0.634* | 0.628* |
| (0.037) | (0.035) | (0.297) | (0.292) | (0.278) | (0.281) | |
| SNCXImmigr.Xtime = 1 | 0.025 | 0.021 | 0.137 | 0.239 | 0.151 | 0.258 |
| (0.038) | (0.036) | (0.273) | (0.261) | (0.190) | (0.195) | |
| SNCXImmigr.Xtime = 2 | 0.059 | 0.058 | 0.095 | 0.152 | 0.049 | 0.088 |
| (0.038) | (0.036) | (0.233) | (0.229) | (0.166) | (0.170) | |
| SNCXImmigr.Xtime = 4 | 0.002 | 0.003 | 0.331 | 0.340 | –0.117 | –0.052 |
| (0.038) | (0.036) | (0.264) | (0.259) | (0.188) | (0.195) | |
| SNCXImmigr.Xtime = 5 | 0.020 | 0.018 | 0.304 | 0.319 | –0.194 | –0.064 |
| (0.038) | (0.036) | (0.285) | (0.275) | (0.200) | (0.205) | |
| SNCXImmigr.Xtime = 6 | 0.003 | 0.010 | 0.198 | 0.270 | –0.115 | –0.025 |
| (0.038) | (0.036) | (0.279) | (0.268) | (0.209) | (0.211) | |
| With controlsa | No | Yes | No | Yes | No | Yes |
| Constant | 0.770*** | –0.367*** | 12.161*** | 6.981*** | 2.831*** | –0.178 |
| (0.001) | (0.013) | (0.005) | (0.083) | (0.011) | (0.121) | |
| /lnalpha | 2.512*** | 2.507*** | ||||
| (0.003) | (0.003) | |||||
| Observations | 734,916 | 734,916 | 576,276 | 576,276 | 576,588 | 576,588 |
| Adjusted R-squared | 0.084 | 0.170 | 0.031 | 0.141 | N/A | N/A |
All analyses control for cohort variation (year of birth of child).
a Models 2, 4 and 6 control for mothers’ education, age, regional background, local unemployment rates, fathers’ regional background and fathers’ income.
Standard errors in parentheses.
+ p < 0.10.
*p < 0.05.
**p < 0.01.
***p < 0.001.