
Abstract
This study investigates whether there are differences in informal social capital between people with a chronic illness and healthy individuals. We also test to what extent this relationship is mediated by individual characteristics and moderated by country-level characteristics. In contrast to previous research, we use representative recent and high-quality data from the European Social Survey of 2012 as well as multilevel analysis. Our results demonstrate that chronically ill people have less informal social capital, all across Europe. Individual characteristics, including depression, subjective health, and perceived income, mediate this relationship almost fully. Welfare regimes and the amount of money countries spend on health care moderate the relationship between chronic illness and informal social capital.
Introduction
Chronic illnesses are one of the major causes of mortality in Europe (Busse et al., 2010). The World Health Organization defines chronic illnesses as: ‘Diseases of long duration and generally slow progression’ (ECDA, 2015). This concept comprises different chronic illnesses such as heart diseases, diabetes, inflammatory bowel diseases, mental illnesses, and many others. Such chronic illnesses hamper the daily lives of many people in terms of informal social capital, that is, meeting friends, relatives or colleagues, which is acknowledged by the European Commission for Public Health (https://ec.europa.eu/health/).
However, our knowledge on the extent to which chronic illnesses hamper informal social capital is limited, that is, mostly based on small, non-representative samples from the United States (Charmaz, 1983; Kawachi et al., 1996). Haas et al. (2010) used a large sample of adolescents and found that poor health increased social isolation and hence, decreased informal social capital. To the best of our knowledge, there are only two studies really based on representative national samples that focused on this relationship – studies that actually provided evidence that those who are restricted by chronic illnesses enjoy less informal social capital (Tijhuis et al., 1998; Oldenkamp et al., 2013). However, in influential studies, the relationship between chronic illnesses and social capital is conspicuous by absence (Portes, 1998; Putnam, 2000). Moreover, even in those that focus on the relationship between (restrictions in) health and social capital (Berkman and Kawachi, 2000; Kawachi et al., 2008; Smith and Christakis, 2008), this relationship is barely touched upon.
In this contribution, therefore, we set out to fill this lacuna in our knowledge in several ways. First, we describe the relationship between chronic illness and informal social capital. Therefore, we propose to assess to what extent chronic illness hampers informal social contacts in daily life rather than the other way around (as was done in previous research), particularly so because this domain is underexplored, as argued above. Second, we do so in a wide range of European countries based on representative samples, using the European Social Survey (ESS, 2012), as an improvement compared to previous research. Third, we set out to explain the relationship between chronic illnesses and informal social capital, proposing and testing mediators. Fourth, we assess whether national characteristics, for example, welfare regimes and health care expenditure, affect informal social capital in European countries (following up on previous research by Kääriäinen and Lehtonen, 2006); and if so, we set out to find to what extent the particular national characteristics of these countries may differentially compensate people suffering from chronic illnesses to continue to access their informal social capital. Therefore, we use multilevel analyses to test whether these national characteristics moderate the relationship between chronic illnesses and informal social capital.
Consequently, our research questions areas follows.
To what extent are there differences between people with a chronic illness and healthy individuals in terms of informal social capital?
To what extent can the relationship between chronic illness and informal social capital be explained by individual level mediators?
A: To what extent do these differences between chronic illnesses and informal social capital vary across European societies? B: And, if so, are these moderated by country characteristics?
Theories and hypotheses
Previous research on social capital often distinguishes formal and informal social capital (Pichler and Wallace, 2007; Savelkoul et al., 2011). We only focus on informal social capital here. The groundwork for the definition of informal social capital was laid down by Bourdieu (1986) and is complemented by many others. Informal social capital mainly consists of informal bonds between people (Pichler and Wallace, 2007).
It is generally proposed that certain resources, such as income and education, affect different forms of social capital (Berkman and Kawachi, 2000; Gesthuizen et al., 2008); people with a higher income can have better access to social capital because they have more economic means to invest in relationships (Tigges et al., 1998). Also, education fosters social capital through socialization at school and within social networks (Gesthuizen et al., 2008). When pursuing this line of thought, we propose that health is another kind of resource; vice versa, a lack of health can reduce opportunities to invest in social contacts. Hogan et al. (1993) argue that good health is a resource whereas bad health is a constraint in the context of social exchanges. Haas et al. (2010) state that people with a chronic illness are often hampered in their physical activities and thus have to cope with chronic constraints to meet others. This was also previously found by Charmaz (1983) and Fougeyrollas (2000). Furthermore, Haas et al. (2010) also state that, for people with a chronic illness, reciprocity is harder to maintain in social relationships because of a lack of energy. Therefore, we overall expect the following.
1. The more people are hampered in their daily activities by any chronic illness, the less informal social capital they have.
Individual level mediators
The lack of resources of people with a chronic illness can also affect other dimensions of health such as depression and subjective general health. Several studies showed that depression is more common among people with a chronic illness (e.g. Moussavi et al., 2007). Moreover, symptoms of depression have been linked to various measures of social capital, such as memberships of and participation in groups (Lin et al., 1999; Pollack and Von dem Knesebeck, 2004). People who are hampered by a chronic illness are more likely to experience feelings of depression, which may reduce their ability to maintain informal social contacts.
2. The negative relationship between chronic illness and informal social capital can be (partly) explained by (feelings of) depression.
A second mediator that we take into account is subjective general health. Liang (1986) and Pinquart (2001) showed that chronic illness is strongly associated with a lower subjective health, which in turn is related to informal social capital (Pollack and Von dem Knesebeck, 2004). Thus, people who are restricted by a chronic illness may also evaluate their subjective health as being worse, which may reduce informal social capital.
3. The negative relationship between chronic illness and informal social capital can be (partly) explained by a lower subjective general health.
People with a chronic illness are also more vulnerable to poverty. This is partly the case because these people may have fewer opportunities to work, reducing their income. Moreover, people with a chronic illness often have higher medical costs, which can make it harder to make ends meet (Van Agt et al., 2000). People with a lower income and higher (medical) costs probably will live less comfortably on their income and have fewer economic resources that can help maintain informal social capital (Tigges et al., 1998).
4. The negative relationship between chronic illness and informal social capital can be (partly) explained by a lower income.
Contextual moderators
Previous research has shown that countries differ in their amount of informal social capital (Gesthuizen et al., 2008; Kääriäinen and Lehtonen, 2006; Scheepers et al., 2002). To provide a theoretical understanding of the differences in the relationships between chronic illness and informal social capital across European countries, we follow the rationale on previous distinctions between types of welfare states: Scandinavian, Anglo-Saxon, Bismarkian (Esping-Andersen, 1990); South European (Bonoli, 1997; Ferrera, 1996); and former USSR-type regimes and post-communist European-type regimes (Fenger, 2007). The underlying rationale, provided by Esping-Andersen (1990: pp.21–22), is that these welfare states have differential policies with regard to (health-care) policies and funding spent on health care to compensate particular individuals for a (temporary) lack of resources to maintain a livelihood without reliance on the market, that is, decommodification.
The (social democratic) Scandinavian regime is characterized by policies that promote social equality through a redistributive social security system (Eikemo et al., 2008) and reduce the influence of the market on distribution (Bambra and Eikemo, 2008). The generous universal and highly redistributive benefits depend little on individual contributions, although recent changes reduced these benefits to some extent (Arts and Gelissen, 2002; Burström, 2015). These redistributive benefits may compensate for the reduced resources of chronically ill people in these countries, reducing differences between them and healthy people in terms of social capital.
The (conservative-corporatist) Bismarkian regime is characterized by a moderate level of decommodification and limited redistribution (Esping-Andersen, 1990). The principle of subsidiarity implies that the state will only interfere when the family’s capacity to serve its members is exhausted (Bambra and Eikemo, 2008). This limited redistribution may also compensate for reduced resources of chronically ill people in these countries in terms of social capital, but less so than in countries belonging to the Scandinavian regime.
The (liberal) Anglo-Saxon regime is characterized by means-tested assistance and modest social insurance plans. There is little redistribution of income in the social security system (Esping-Andersen, 1990). Social rights are rather poor (Scheepers et al., 2002) and recipients are usually stigmatized (Bambra and Eikemo, 2008). This regime has the lowest level of decommodification; the dominance of the market is encouraged by guaranteeing only a minimum and by subsidizing private welfare schemes. This regime may only marginally compensate for reduced resources of chronically ill in terms of social capital, probably far less so than in countries belonging to the Scandinavian regime.
After these initial distinctions, the South European regime (the Latin Rim) has been described as ‘rudimentary’, because the welfare provision is fragmented and consists of diverse income maintenance schemes of varying heights. There is a high degree of familialism, moderate decommodification and modest redistributive effects (Trifiletti, 1999). The health sector, in particular, provides only limited and partial coverage (Bambra and Eikemo, 2008). This regime may (marginally) compensate for chronically ill people, especially in terms of social contacts with family, but less so than in countries belonging to the Scandinavian regime.
After the collapse of the communist system, former member countries in the Union of Soviet Socialist Republics (USSR) were also considered to be distinct welfare regimes; they resemble the conservative-corporatist type when looking at total government expenditures (Fenger, 2007). However, all other governmental programs are below the Western European types. This regime spends the least on health and social protection in comparison to all other regimes. Inequality in these countries is (almost) as high as in the Anglo-Saxon regime (Fenger, 2007). Therefore, this welfare regime is expected to compensate chronically ill people the least compared to all other regimes and to differ the most from the Scandinavian regime.
The post-communist European-type regime shows similarities with the former USSR-type regimes, but it can be distinguished because it is clearly more egalitarian. These countries have experienced a shift towards marketization and decentralization (Bambra and Eikemo, 2008). Post-communist European-type regimes spend more on social protection and health than former USSR countries. These differences may be due to economic developments over recent decades, which makes this regime more similar to the Bismarkian regime (Fenger, 2007). This regime may marginally compensate for chronically ill people and differ from the Scandinavian regime, but less so than the former USSR-type regime.
Overall, we propose to test an (exploratory) hypothesis on the differential relationships between chronic illness and social capital that may be related to the nature of the welfare state.
5. Informal social capital of chronically ill people will be the highest in Scandinavian welfare regimes; next, it will be somewhat lower in Southern European regimes, Bismarkian regimes, and Anglo-Saxon regimes; then post-communist countries; and then the lowest in USSR countries.
Chronically ill people may have fewer resources than healthy people, in terms of a lower income and higher medical costs (Van Agt et al., 2000), and thus are less able to invest in their social capital. States might compensate for this lack of resources by spending money on health care. When states compensate for medical costs to a high extent, we expect that people have more financial resources left to invest in their informal social capital. Since European states differ in the amount they spend on health care (World Bank, 2011), differences in social capital between healthy people and chronically ill people can be reduced to a different extent in European countries.
6. The more a country spends on health care, the weaker the relationship between individual chronic illness and informal social capital will be.
Data and methods
This study analyzes high-quality data from the ESS (2012). The ESS, which has been conducted every 2 years since 2002, charts the attitudes, beliefs and behavior of citizens in a variety of European countries. Samples of the population of each country are representative and selected by strict at-random probability methods. All stages of sampling, data gathering and translation of the questionnaires are governed by expert groups. For more information about the ESS data, we refer the reader to the official ESS website (http://www.europeansocialsurvey.org). Wave 6, which is used for this research, contains 29 countries with 54,673 individuals. After the exclusion of all respondents with missing values (except for those on income), the final dataset for our analyses consists of 27 countries and 47,543 individuals.
Individual level characteristics
We measured informal social capital with the question: ‘How often do you socially meet with friends, relatives or colleagues?’. Answer categories were ‘never’, ‘less than once a month’, ‘once a month’, ‘several times a month’, ‘once a week’, ‘several times a week’, and ‘every day’. Previous studies used this variable to measure informal social capital as well (e.g. Savelkoul et al., 2011).
Chronic illness was measured by asking respondents to what extent they were hampered in their daily activities by a chronic illness. Answer categories were ‘not at all’, ‘to some extent’, and ‘a lot’. This item was previously used to indicate chronic health conditions (Erlinghagen et al., 2008).
To examine feelings of depression, we used the Center of Epidemiological Studies-Depression Scale. Respondents were asked to fill in how often they experienced certain feelings over the past week on a 4-point scale (from ‘none or almost none of the time’ to ‘all or almost all of the time’) 1 . This scale of depression has been widely used in research on depressive affect (Shafer, 2006). It was found to have very high internal consistency and adequate test-retest reliability (Chabrol et al., 2001). The Cronbach’s alpha of 0.836 indicated that this is a reliable scale.
We measured subjective general health by the question ‘How is your health in general? Would you say it is “very good”, “good”, “fair”, “bad”, or “very bad”’. This measurement indicates both physical and mental health (Huijts, 2011). Moreover, this measurement was used in several studies as an indicator to examine health (Eikemo, 2010).
To indicate (perceived) income, respondents were asked: ‘Which of the descriptions comes closest to how you feel about your household’s income nowadays? “Living comfortably on present income”, “coping on present income”, “finding it difficult on present income”, or “finding it very difficult on present income”’. We used this question because it measures financial constraints (Halleröd and Larsson, 2008; Paugam, 1996), next to actual income.
Contextual variables
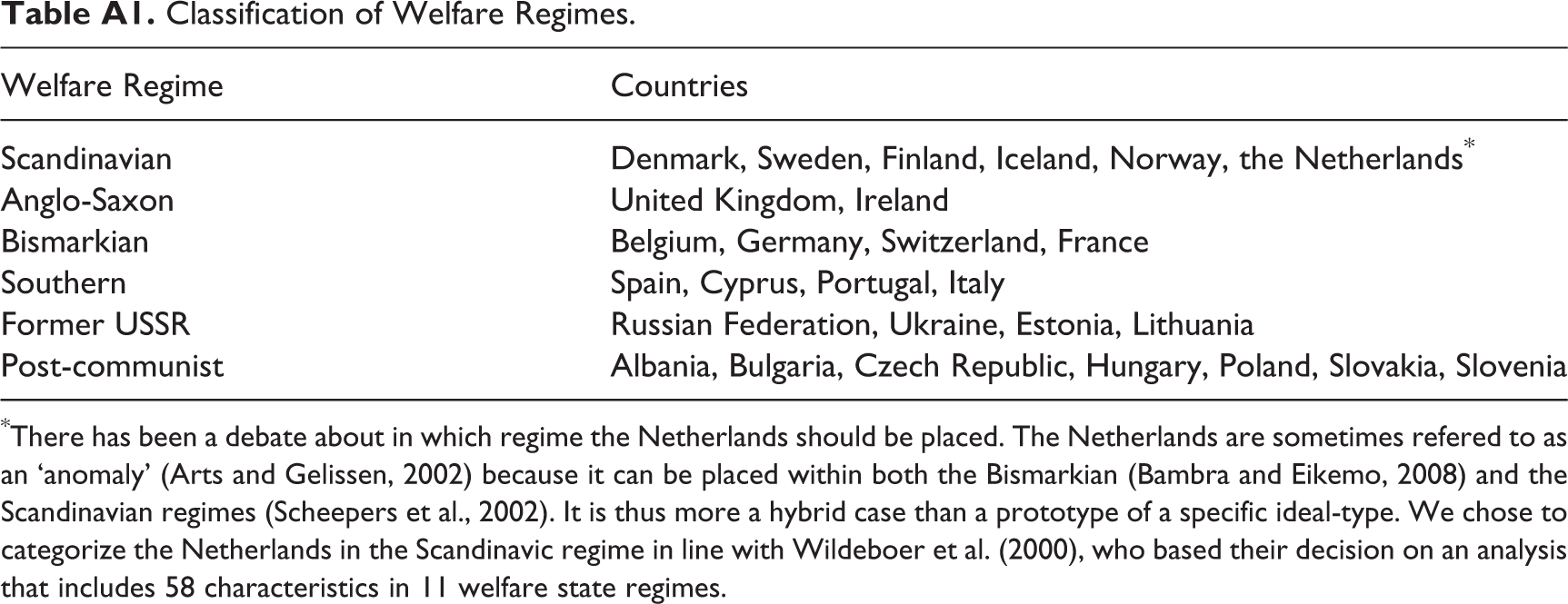
We created a variable for welfare regimes by distinguishing six types of welfare states: Scandinavian, Anglo-Saxon, Bismarkian (Esping-Andersen, 1990), South European (Bonoli, 1997; Ferrera, 1996), former USSR, and post-communist (Fenger, 2007). The classification of countries in these regimes can be found in Appendix Table A1.
For health-care expenditure, the percentage of gross domestic product (GDP) spent on health care was retrieved from the World Bank (2011). Descriptives of health-care expenditure can be found in Tables 1 and 2.
Control variables
We controlled for a variety of resources related to social capital or health in accordance with the existing literature. These were ‘education’ (Cutler and Lleras-Muney, 2006), ‘income’ (Berkman and Kawachi, 2000), ‘marital status’ (Lindström, 2009; Putnam, 2000), ‘having children’ (Gray, 2009; Lin, 2000), and ‘religious attendance’ (Huijts and Kraaykamp, 2011). Also, ‘gender’, ‘age’ (Gray, 2009; Huijts, 2011), and ‘ethnicity ‘(Lin, 2000) were expected to be related to social capital and health and were therefore taken into account.
Education was measured with the use of the ‘International Standard Classification of Education’ scale, which is designed to facilitate cross-cultural comparisons concerning educational levels (UNESCO, 2015). It contains seven categories ranging from pre-primary education to the second stage of tertiary education. Income was classified in 10 deciles, with an added ‘unknown’ category for our missing values on income.
Furthermore, we distinguished ‘people who are married/living together’, ‘divorced’, ‘widowed’, and ‘people who were never together with a partner’. We also took into account whether people have children (who live at home).
Religious attendance was included using a 6-point scale ranging from ‘attending religious services never’ to ‘attending religious services every day’. Gender (1 = female), age (15–103), and whether respondents belong to a minority group (1 = yes) were taken into account. Descriptive statistics of all variables can be found in Tables 1 and 2.
Descriptive statistics.
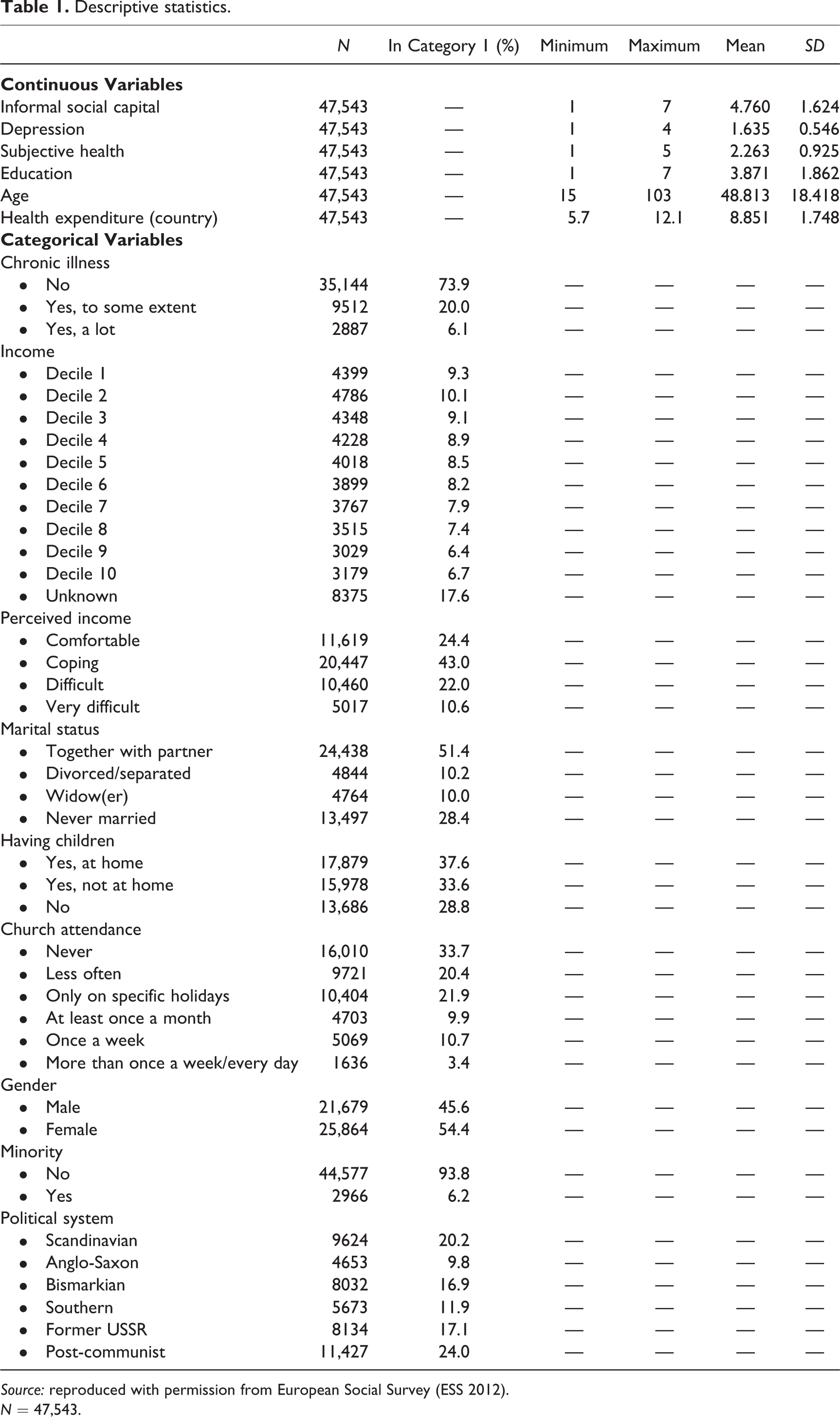
Source: reproduced with permission from European Social Survey (ESS 2012).
N = 47,543.
Descriptive information on country characteristics.
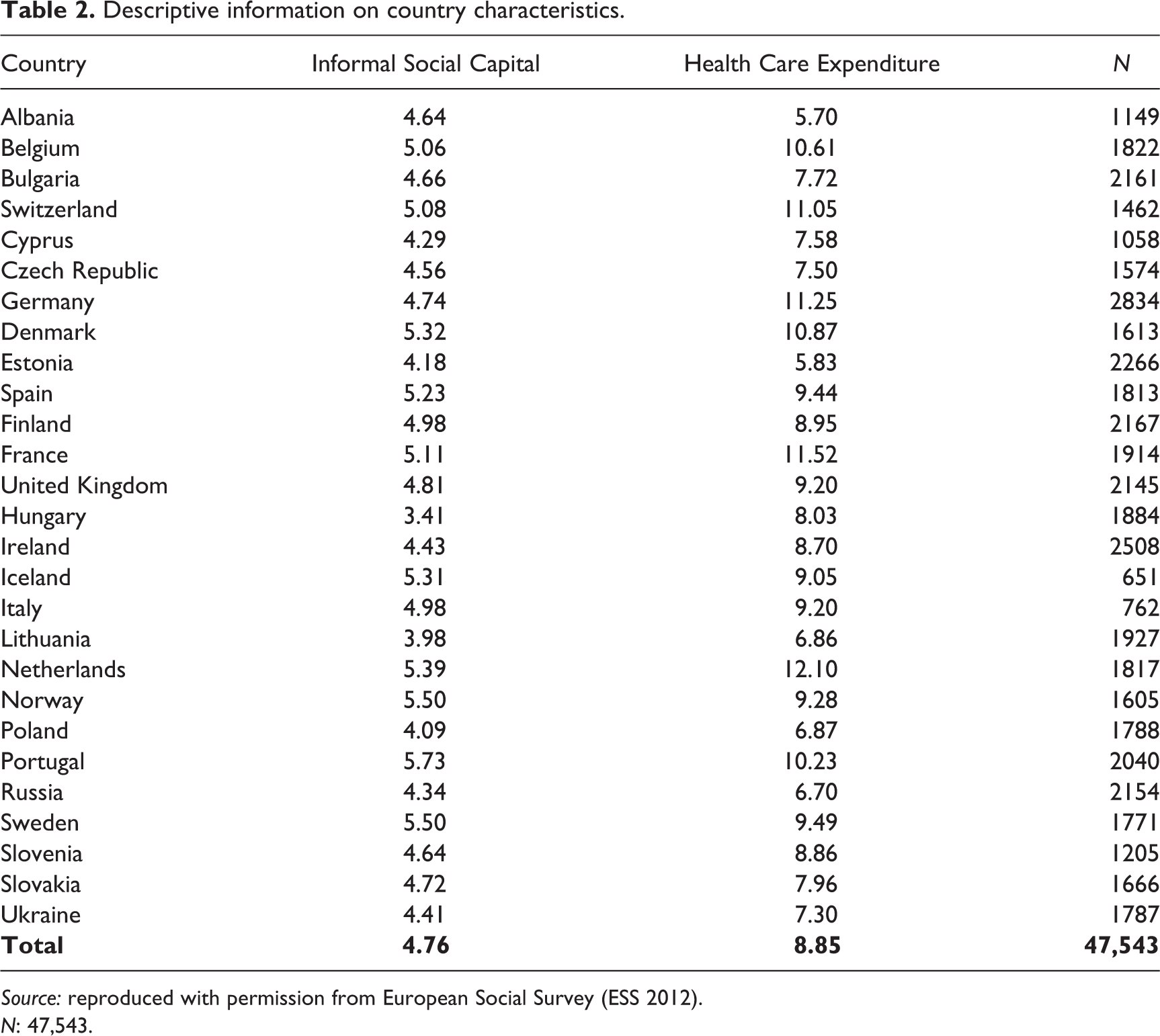
Source: reproduced with permission from European Social Survey (ESS 2012).
N: 47,543.
Strategies for analyses
First, we tested the bivariate relationship between chronic illness and informal social capital in the different countries with analysis of variance. Results (Table 3) showed that there was a significant amount of variation between countries in social capital. We also found that in most countries, the more people are hampered by a chronic illness, the less informal social capital people have. This indicated a robust relationship between chronic illness and informal social capital.
Differences in informal social capital per country.
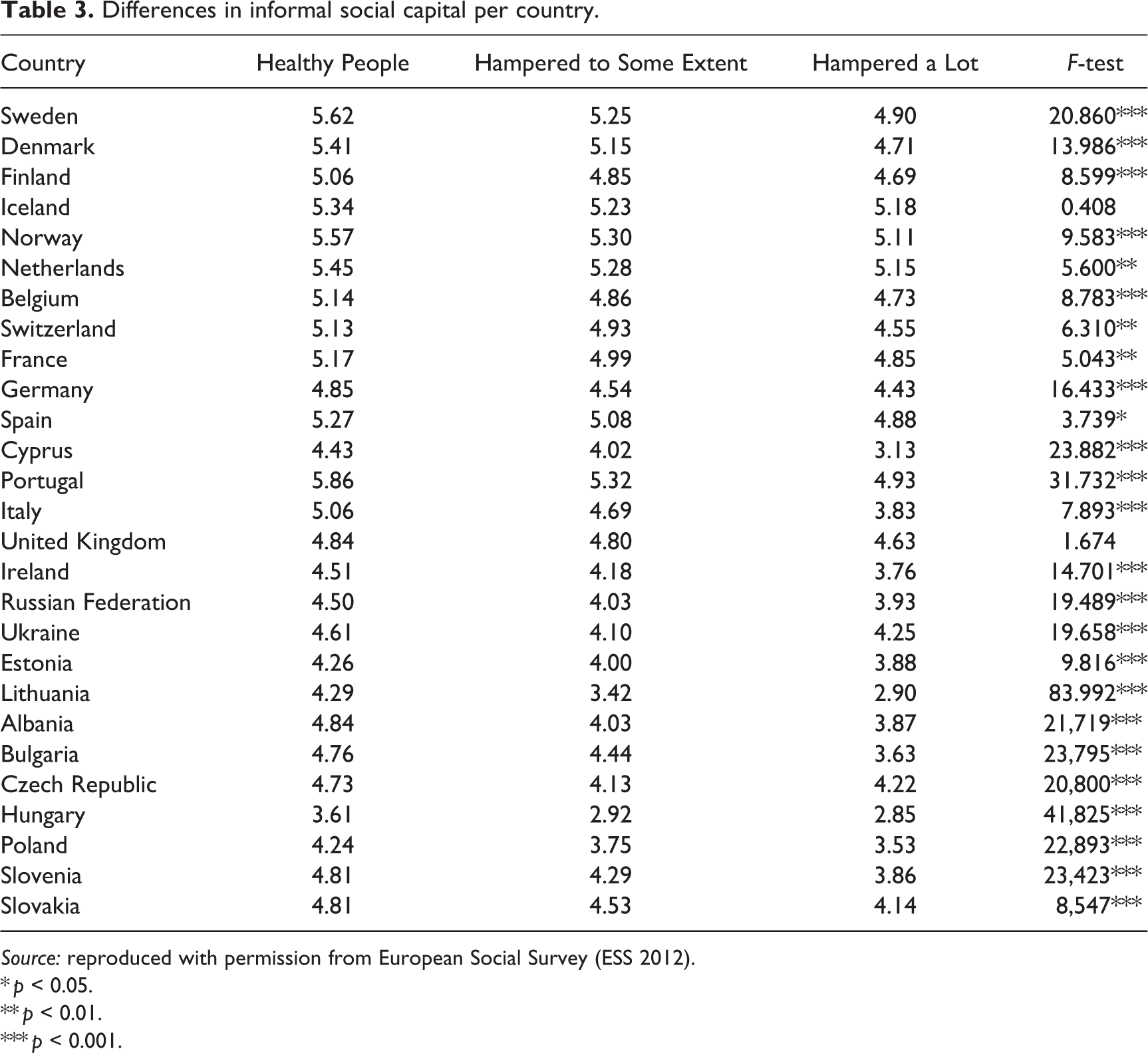
Source: reproduced with permission from European Social Survey (ESS 2012).
* p < 0.05.
** p < 0.01.
*** p < 0.001.
Subsequently, we carried out random-intercept multilevel regression analyses to test our hypotheses. Multilevel analysis takes into account that individuals are nested in countries and random-intercept models take into account possible country differences. Bryan and Jenkins (2016) suggested that the use of multilevel logit models for analysing international comparative data, which include fewer than 30 countries, is problematic. Therefore, a multilevel regression model was determined to be the better choice for analysing the data used in this study. All models are shown in Tables 4 and 5. Additionally, Chi-squared tests demonstrated that random-intercept models fit the data significantly better than fixed-intercept models. The intraclass correlation in the empty model shows that 11% of the variation in informal social capital can be attributed to differences between countries.
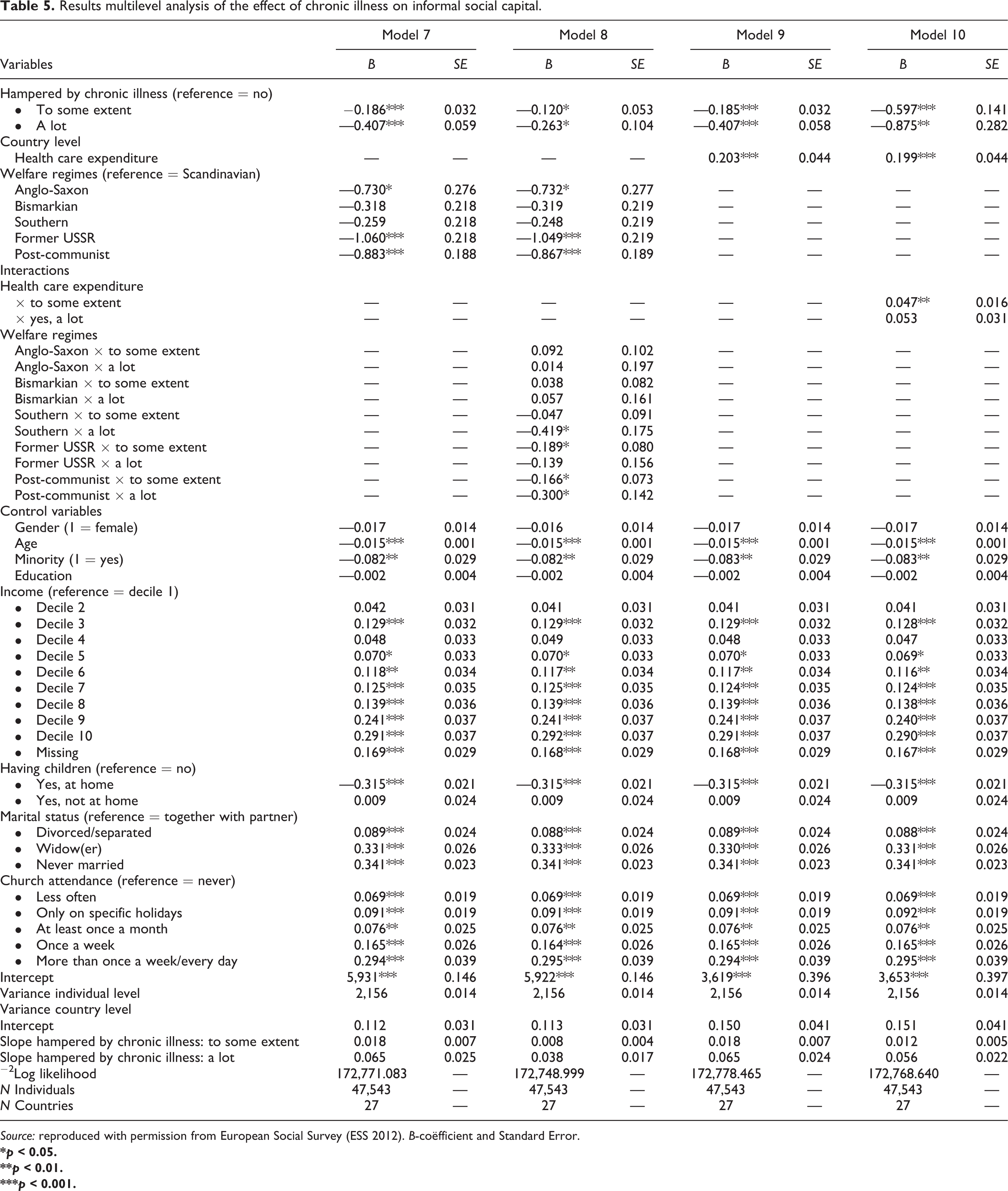
Results multilevel analysis of the effect of chronic illness on informal social capital.
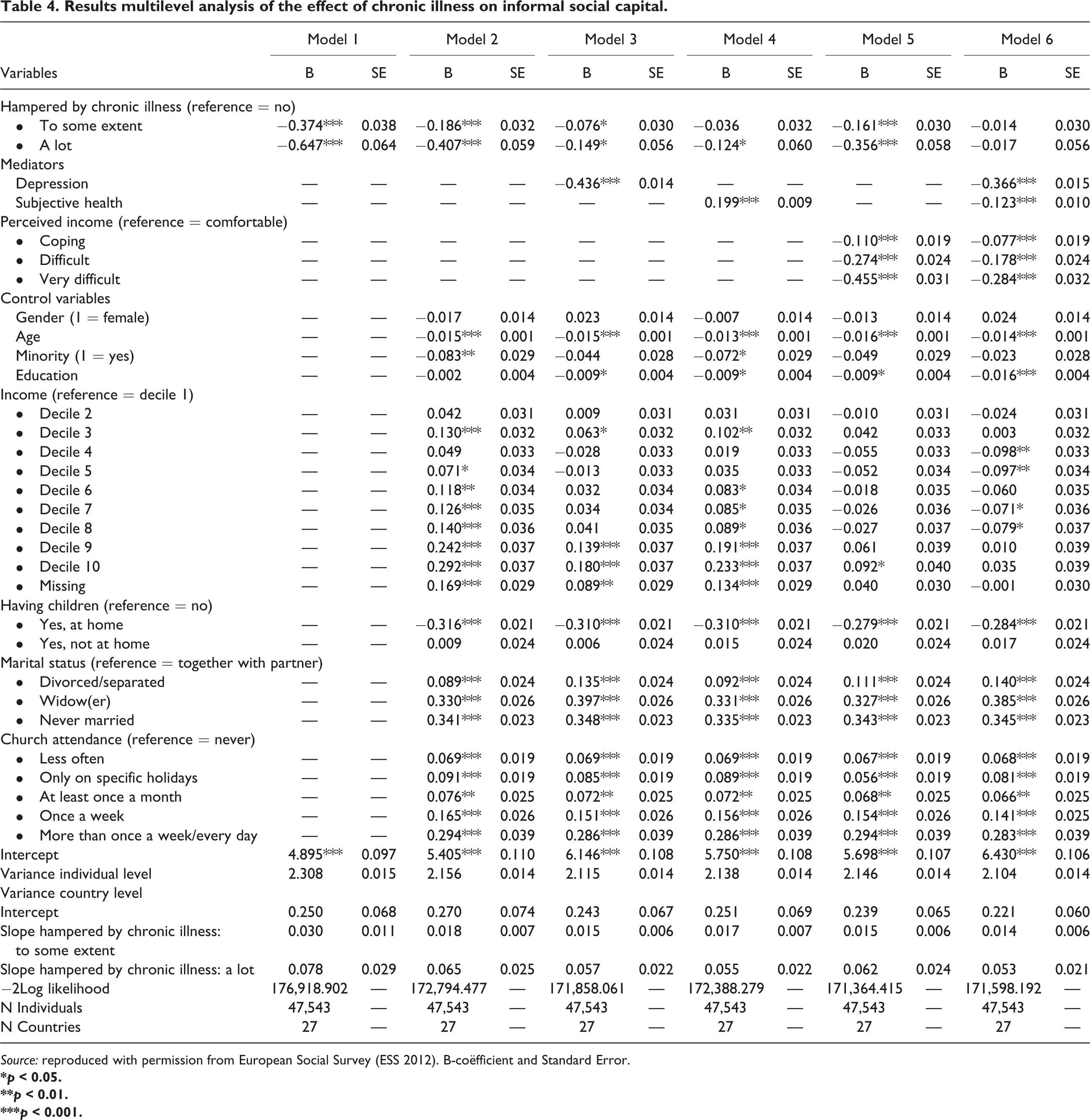
Source: reproduced with permission from European Social Survey (ESS 2012). B-coëfficient and Standard Error.
Results multilevel analysis of the effect of chronic illness on informal social capital.
Source: reproduced with permission from European Social Survey (ESS 2012). B-coëfficient and Standard Error.
*p < 0.05.
**p < 0.01.
***p < 0.001.
Model 1 only includes our main independent variable, chronic illness. The second model, Model 2, tests the significance of the bivariate relationships while taking into account our control variables in order to test for spurious relationships. In Models 3–5, we tested our mediating hypotheses by adding the mediators, one by one. Thereafter, we added all mediating variables simultaneously in Model 6. Models 7–10 analyzed our cross-level interaction hypotheses. We investigated the main effect of welfare regimes on informal social capital in Model 7. Subsequently, we added relevant cross-level interaction terms concerning welfare regimes in Model 8. The same procedure was followed for health-care expenditure in Models 9 and 10. In Model 11, all country-level characteristics (main effects and interaction effects) were added simultaneously. All analyses were performed with the use of IBM SPSS Statistics 19.
Results
Model 1 shows that people with a chronic illness have significantly less informal social capital. Those who are hampered a lot (b = −0.647) have even less social capital than those who are hampered to some extent (b = −0.374) as compared to healthy people. When we control for several individual level characteristics in Model 2, this relationship still holds (b = −0.186 and −0.407), confirming Hypothesis 1 (see above).
On the basis of Models 3–5, we can state that depression, subjective health, and perceived income in each model explain a large part of the initial relationship between chronic illness and informal social capital; all these mediators have the expected effects on chronic illness and, moreover, reduce the original differences in Models 1 and 2, respectively.
It is, moreover, interesting to note that Model 6 shows that the initial relationship in Model 1 is almost fully explained by depression, subjective general health, and perceived income. For people who are impeded to some extent in their daily activities, 92.5% 2 can be explained by a lack in these resources. For people who are impeded a lot in their daily activities, this is 95.8% 3 . We tested whether the mediations are significant, with the method of Preacher and Hayes (2008). Figure 1 presents the path diagram, in which it can be seen that all mediating effects are significant, hence supporting hypotheses 2, 3, and 4 (see above).
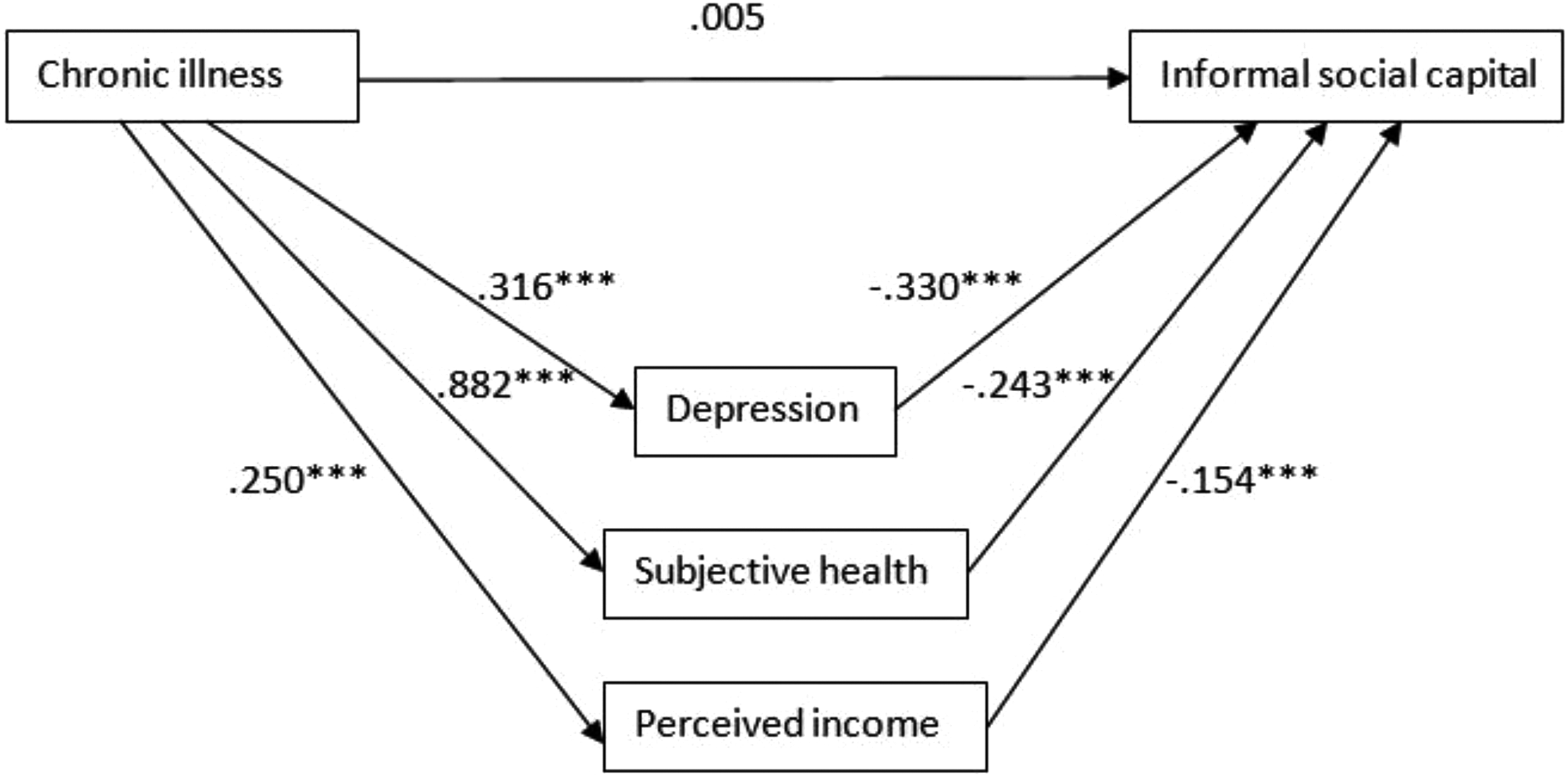
Mediators for the original relationship between chronic illness and informal social capital.
Regarding the country-level characteristics 4 , Model 7 shows that there are differences in informal social capital between welfare regimes. People in Anglo-Saxon regimes have less informal social capital (b = −0.730) than people in Scandinavian countries. The Bismarkian and Southern regimes also differ, but not significantly from Scandinavian states in terms of the amount of informal social capital. Compared to the Scandinavian regime, post-communist and former USSR countries differ the most in the amount of informal social capital (b = −0.883 and −1.060). Thus, inhabitants of former USSR states differ most from the Scandinavians.
We expected that the relationship between chronic illness and informal social capital would be different in various welfare regimes. Model 8 shows that few interaction terms are significant. In post-communist regimes, the relationship between chronic illness and informal social capital is significantly negative (b = −0.867). For those who are hindered ‘to some extent’ and ‘a lot’, this relationship is even more negative (b = −0.166 and −0.300, respectively). As stated before, former USSR states have the least informal social capital (b = −1.049) of all welfare regimes. People who are only hampered ‘to some extent’ by their illness (b = −0.189) have even less social capital. The negative effect for people who are hampered ‘a lot’ is not significant (b = −0.139); however, the negative effect for those who are hampered ‘to some extent’ is significant (b = −0.189). Although Southern countries do not differ significantly from the Scandinavian regime in the amount of informal social capital (b = −0.248), people in these countries who are hampered ‘a lot’, do have significantly less informal social capital (b = −0.419). The other regimes do not differ significantly from Scandinavian countries in the relationship between chronic illness and informal social capital. Hypothesis 5 is thus only partly confirmed, particularly for the chronically ill in former USSR and post-communist countries.
Model 9 shows that people who live in countries that spend more on health care have more contact with friends, family and colleagues (b = −0.203). This can be seen in Model 10 as well (b = −0.199). Chronically ill people in countries that spend a lot on health care, have more informal social capital than these people in countries with a lower health-care expenditure, but this relationship is only significant for people who are hindered ‘to some extent’ by a chronic illness (b = −0.047) and not for people who are hampered ‘a lot’ (b = −0.053). Hence, we can conclude that Hypothesis 6 is partly confirmed as well.
Considering our control variables, Model 2 shows that the elderly, minority groups, people with children who live at home, and lower-income groups have less informal social capital. People who attend church regularly and people who are not together with a partner (divorced, never married, and widowed) see friends, family and colleagues more often. This is consistent with prior research findings (Huijts, 2011; Lin, 2000; Van Oorschot et al., 2006; Savelkoul et al., 2011).
Discussion
In this contribution we aimed to gain insight into the relationships between chronic illness and informal social capital. Research on this particular relationship is rather scarce, and hence we set out to fill this gap in our knowledge. We enriched existing knowledge by describing and explaining the relationship between chronic illness and informal social capital with individual and contextual level characteristics. We used representative and high-quality data on 27 European countries from the ESS (2012). Moreover, we applied multilevel regression analyses to test our hypotheses.
Previous research demonstrated that certain resources, such as income and education, have positive relationships with social capital (Berkman and Kawachi, 2000; Gesthuizen et al., 2008). Health can also be considered a resource fostering social capital. Our research showed that people who are hampered ‘to some extent’ by a chronic illness actually have less informal social capital than healthy people. Additionally, we found that people who are hampered ‘a lot’ have even fewer contacts with friends, family and colleagues. We found this pattern in most European countries. In line with our expectations, health is positively related to social capital, which could imply that health can be seen as a resource. We attempted to explain this relationship with several individual level mediators that indicate a lack of other resources, namely depression, subjective health, and perceived income. Results showed that these characteristics explained the initial relationship between chronic illness and informal social capital almost fully, when included simultaneously. These results support our reasonings that certain resources are important in explaining the relation between chronic illness and social capital.
Subsequently, we tested whether the initial relationship between chronic illness and social capital differed between European societies and how these differences could be explained. First of all, we found that, in accordance with our expectations, social capital differs across welfare regimes. Scandinavian countries seem to have the highest level of social capital, followed by Southern, Bismarkian, Anglo-Saxon, and post-Communist countries. Social capital was lowest in former USSR countries. Only the difference between Scandinavian countries and Bismarkian, post-communist, and USSR countries was significant, thereby partly confirming our hypothesis on differences in social capital across welfare regimes. Subsequently, we proposed hypotheses about the moderating influence of welfare regimes; these findings provide innovative insights. We expected that welfare regimes differ in their ability to compensate for the lack of resources of the chronically ill. The findings suggest that post-communist and former USSR regimes compensate people with a chronic illness poorly to maintain informal social capital. As expected, people in this regime who suffer (‘a lot’) from a chronic illness, have even less social capital than the healthy people in these countries.
An interesting finding is that Southern countries also seem to compensate the chronically ill less than Scandinavian countries. However, only people who are hampered ‘a lot’ differ significantly from healthy people in their amount of informal social capital. In Southern European countries, there is a high degree of familialism (Trifiletti, 1999). We suspect that, when people are impeded to some extent, family members can still take care of their relatives. When the need for help becomes more severe, help from family may become insufficient. Thus, people who are hampered ‘a lot’ by their chronic illness in the Southern regime ‘lose’ more informal social capital.
Regarding health-care expenditure, we found that the more countries spend on health care, the more informal social capital its inhabitants have. This relationship is even stronger for people who are hampered ‘to some extent’ by a chronic illness. This finding underlines the importance of taking into account health-care expenditure. For people who are hampered ‘a lot’, this effect does not reach significance. We suspect that for people who are hampered ‘a lot’, health limitations are so severe that health-care expenditure can no longer sufficiently compensate.
The theoretical framework of this study proposed a relationship between chronic illness and informal social capital. Yet, there are also studies that examined the positive and negative effects of social relations on health (Cohen, 2004; Kawachi et al., 1996). Hence, these studies proposed a reversed causal relationship in their theoretical framework. To the best of our knowledge, there are no studies that tested the direction of the relationship more thoroughly. Future research should improve on this by using panel data.
It should be acknowledged that our measurement of social capital relies on one item only. Although this measurement has been used frequently in previous research and has been proven to be a valid indicator of informal social capital (e.g. Savelkoul et al., 2011), future research would benefit from a more comprehensive measurement in order to cover multiple aspects of informal social capital. Furthermore, it should be acknowledged that cross-national studies like ours can entail difficulties, such as problems concerning comparability or socio-cultural biases. Yet, our results on the relationship between chronic illness and social capital are robust. Differences in social capital between healthy and chronically ill people show the same pattern in every country (except Ukraine); healthy people have the highest level of social capital and people who are hampered ‘a lot’ by a chronic illness have the least social capital.
To answer our initial research questions, we found that the relationship between chronic illness and informal social capital can be mediated almost fully by depression, subjective health, and perceived income. Moreover, we showed that country characteristics play a role in this relationship. Countries differ in their ability to compensate for the lack of resources that affects people with chronic illness to continue their social contacts, as shown by significant moderators. The combination of explanatory individual characteristics and country-level features has thus been proven to be fruitful, and should be taken into account in future research.
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Notes
Appendix
Classification of Welfare Regimes.
| Welfare Regime | Countries |
|---|---|
| Scandinavian | Denmark, Sweden, Finland, Iceland, Norway, the Netherlands* |
| Anglo-Saxon | United Kingdom, Ireland |
| Bismarkian | Belgium, Germany, Switzerland, France |
| Southern | Spain, Cyprus, Portugal, Italy |
| Former USSR | Russian Federation, Ukraine, Estonia, Lithuania |
| Post-communist | Albania, Bulgaria, Czech Republic, Hungary, Poland, Slovakia, Slovenia |
*There has been a debate about in which regime the Netherlands should be placed. The Netherlands are sometimes refered to as an ‘anomaly’ (Arts and Gelissen, 2002) because it can be placed within both the Bismarkian (Bambra and Eikemo, 2008) and the Scandinavian regimes (Scheepers et al., 2002). It is thus more a hybrid case than a prototype of a specific ideal-type. We chose to categorize the Netherlands in the Scandinavic regime in line with Wildeboer et al. (2000), who based their decision on an analysis that includes 58 characteristics in 11 welfare state regimes.