
Abstract
This article investigates how macro-level structures condition the sources of socioeconomic inequalities in health. Drawing on multiple social science disciplines, the authors develop theoretically grounded propositions about how different types of welfare states, varieties of capitalism, and social structures give rise to cross-national variations in the sources of health inequalities. They consider how these macro-level structures affect the distribution of five key resources important to health, estimate the relative contribution that each resource makes to health inequalities, and compare those contributions in 21 developed democracies. Moving beyond a current literature focused on welfare states, the authors show how different types of political economies and social structures also condition the health gradient. This research carries implications for policy and suggests agendas for further investigation into the relationship between macro-level structures and inequalities in health.
In all societies, there is a socioeconomic gradient in health: people in higher socioeconomic classes tend to have lower rates of mortality and better health than those in lower socioeconomic classes (for reviews, see Bartley 2016; Mackenbach 2019). But the steepness of this health gradient and its sources vary dramatically across countries. Rates of mortality for manual workers are a little more than 1.5 times higher than they are for upper level nonmanual workers in Italy, for instance, but they are more than 2.5 times higher in Finland (Mackenbach 2019:26). How can cross-national variations in health inequalities and their sources be explained? Those are the problems taken up in this article.
Some significant efforts have been made to address these issues. One school of thought ascribes differences in the health gradient to cross-national variation in income inequality on the premise that class-based differences in health turn on disparities in material resources and related status anxieties (Lynch et al. 2000; Marmot 2015; Van Doorslaer and Koolman 2004), although the evidence for that view is mixed (Truesdale and Jencks 2016). Another approach, prominent in social epidemiology, associates poor health outcomes with exposure to risk factors, and examines the extent to which people in different socioeconomic positions are exposed to various risks or prone to risky behaviors (Aldabe et al. 2011; Balaj et al. 2017; Moor, Spallek, and Richter 2017; Schutte et al. 2013). Both approaches yield important insights, but the first tends to focus on income inequality at the expense of considering other types of resources that affect health; and the second stops short of explaining why national risk profiles differ.
Accordingly, we bring to the problem of explaining cross-national variation in the sources of the health gradient an approach that emphasizes the importance of the macro-level structures of society, embedded in varieties of capitalism, welfare states and systems of social relations. As Beckfield, Olafsdottir, and Bakhtiari (2013) noted, there are reasons to believe that macro-level structures such as these generate cross-national variations in health inequality, but there are relatively few studies about how they do so. To explore this issue, we bring interdisciplinary perspectives in sociology and comparative political economy developed for other purposes to bear on the problem of explaining health inequalities. We ask, How might the structural features of specific types of political economies, welfare regimes and social structures contribute to class-based inequalities in health? We then examine whether they do so in predictable ways.
The body of research most closely related to this inquiry examines the relationship between health inequalities and national political or policy regimes. Some analyses focus on political variables, such as the partisan composition of governance or the extent of neoliberal reform (for reviews, see Beckfield and Krieger 2009; McAllister et al. 2018; Muntaner et al. 2011). Others focus on the relationship between social policy regimes and inequalities in health (for reviews, see Bergqvist, Yngwe, and Lundberg 2013; Brennenstuhl, Quesnel-Vallée, and McDonough 2012; Lynch 2020). These have been fruitful lines of research, but our intuition is that, to explain cross-national variation in health inequality and its sources, we need to look beyond specific policy regimes or welfare states at a larger set of macro-level structures conditioning economic and social relations.
We begin by developing a theoretical perspective on why various macro-level structures might affect inequalities in health, which emphasizes how access to a wide range of economic and social resources conditions health, and how those structures distribute these resources. We then consider the implications of prominent theories about welfare regimes, varieties of capitalism, and comparative social structures for cross-national variation in the distribution of such resources. In an empirical analysis of 21 developed democracies, we compare the contributions that inequalities in access to five key resources—income, education, social connectedness, workplace autonomy, and social status—make to health inequality, measured here as the difference between the health of professional and managerial employees and the health of low-skill manual workers. Although other studies point to the importance of these resources for health, we know of none that compares the relative contribution that each resource makes to the health gradient. Second, we examine cross-national variation in the distribution of these resources and estimate how much inequalities in access to each resource contribute to the national gaps in health found between these two occupational groups. On the basis of this analysis, we draw conclusions about how macro-level structures affect inequalities in health and consider some implications for policies designed to address those inequalities.
A Resource-Based Approach to Explaining Health Inequalities
Our theoretical starting point is a literature on the social determinants of health which establishes that the health of individuals is conditioned by access to a relatively wide range of economic and social resources. Some are the material resources that supply healthy living conditions. Others are social resources with psychosocial effects on health. Although factors beyond the scope of this study such as genetic make-up and early life experiences also matter to health, there is a strong basis for believing that access to economic and social resources make crucial contributions to people’s health (for overviews, see Bartley 2016; Berkman et al. 2014; Siddiqi et al. 2013).
Each type of resource has some specific effects: money can be used to purchase healthier housing conditions, for instance, and social connections can supply the emotional support needed to ward off depression. But in developed societies, there is also a general channel through which access to resources impinges on health. In these societies, the principal sources of morbidity and mortality are chronic illnesses, such as cancer and cardiovascular diseases, which have been associated with persistent experiences of stress. Multiple studies show that repeated levels of stress associated with the “wear and tear” of daily life adversely affect a person’s health (Matthews and Gallo 2011; Seeman et al. 2014; Steptoe and Kivimaki 2013). To put the problem in general terms, most people face a common set of life challenges, ranging from finding housing or employment to caring for children; and to meet those challenges people draw on the resources available to them, such as their savings or supportive networks. Where people lack such resources, coping with life challenges is likely to entail the higher levels of anxiety and stress associated with adverse health outcomes. In short, access to a range of economic and social resources can condition people’s health by virtue of how it enhances their capabilities for coping with life challenges (Hall and Taylor 2009).
We focus on five types of resources, chosen to meet several criteria. First, there is good evidence linking each of these resources to individual health outcomes. Second, the distribution of these resources is likely to be conditioned by the macro-structures of a society. Third, these resources parallel the five “flexible resources” that Link and Phelan (1995) identified as fundamental mechanisms linking socioeconomic inequality to inequalities in health, namely, money, knowledge, social connectedness, power and prestige (Clouston and Link 2021). 1
The first of these resources is income. It is especially important because income is a multipurpose instrument for securing many of the conditions central to good health, such as decent housing, nutritious food, and high-quality health care. The second is education. Access to education is important to health because it is a gateway to less onerous occupations and often associated with the avoidance of risky behaviors (Mirowsky and Ross 2003). The third resource is social connectedness, understood as the extent to which people are embedded in supportive social networks. Social networks provide the logistical and emotional support that enhance people’s capacities for coping with life challenges, and they are closely associated with health (Berkman et al. 2000). The fourth resource we consider is autonomy at work, understood as the level of control people exercise over the pace and direction of their work. Higher levels of autonomy at work reduce the work-related stresses that often take a toll on health (Bambra 2011b). Finally, we contend that a person’s social status can contribute to their health. We construe social status as the subjective level of social worth that people ascribe to themselves. Higher levels of social status are associated with higher levels of self-esteem, which reduce the anxieties associated with ill health, and higher social status makes it easier for people to elicit the cooperation of others in the resolution of life challenges (Marmot 2004; Prag, Mills, and Wittek 2016). Although other resources can be relevant to health, these five resources constitute an appropriate set for considering how cross-national variation in economic and social structures condition inequalities in health. 2
Such resources are distributed unequally in every country, but cross-national variation in that distribution is not random. Our core contention is that it is shaped by specific macro-level structures, namely, regularities in economic and social relations, which may be conventional or generated by formal institutions and backed by sanctions. These structures are both economic and social. The general character of the relevant economic structures is well established. In Williamson’s (1975) famous formulation, the economy is made up of competitive markets and firm hierarchies. Their institutional shape carries implications for the distribution of income and of control over the work process; and we draw on research in comparative political economy indicating that the shape of markets and firm hierarchies varies systematically across countries in ways that affect the distribution of such resources (cf. Hall and Soskice 2001; Amable 2003).
Alongside these economic structures, of course, every country also has a distinctive social structure, with horizontal dimensions present in the social networks connecting people to their family, friends, and acquaintances, and vertical dimensions constituted by the social hierarchies that confer status or social prestige (Grusky 2018). We draw on a sociological literature which suggests that there are systematic variations across countries in the shape of social networks and social hierarchies that lead to cross-national variations in how social connectedness and social status are distributed across people in different socioeconomic positions
In sum, there are good reasons for thinking that access to economic and social resources affects people’s health, that inequalities in the distribution of these resources contribute to socioeconomic inequalities in health, and that the distribution of such resources varies with the macro-level structures of nations.
Cross-National Variation in Economic and Social Structures
We focus on cross-national variation in three sets of macro-level structures—those associated with welfare regimes, varieties of capitalism, and systems of social relations—and ask how differences in them contribute to cross-national variation in the sources of health inequalities by virtue of how they distribute the resources important to health.
If we had a much larger universe of developed democracies in which these three sets of macro-structures varied independently of one another, we might be able to use a correlational analysis to separate out the effects of each. But the available of countries is a relatively small one in which these macro-structures overlap—various types of welfare regimes, for example, accompany specific types of capitalism—and it is often in combination that they distribute the resources affecting health (Kelly-Irving et al. 2023). Hence, it is difficult to account for national variations in the health gradient by reference to a single type of macro-structure or to arrive at precise estimates for the effects of one macro-structure compared with another. 3
For these reasons, we take an inferential approach to the analysis in which we draw predictions from prevailing theories about welfare regimes, varieties of capitalism and social structures about how each can be expected to affect the distribution of resources pertinent to health in the relevant groups of countries, expressed as hypotheses about the variation we should see between groups of countries. We then inspect data about how these resources are distributed within each group of countries to consider whether those distributions correspond to the predictions. Finally, using estimates for the relationship between each resource and health, we draw conclusions about how these macro-structures give rise to cross-national variations in the sources and extent of health inequality between people in upper level and lower level occupational positions.
Each of these macro-structures is the subject of large literatures which we cannot review in detail but, in this section, we draw from research in several subfields to explain how key dimensions of each can be expected to affect the distribution of economic and social resources in the countries included in this study. 4 As background material, Table 1 provides summary measures for how some of the features covered in this analysis vary across these countries.
Summary Indicators for National Differences in Macro-structures.

Note: For measures and sources, see the Appendix.
Welfare Regimes
We begin with welfare regimes, the macro-level institution most often associated with health. There is considerable debate about how to construe and classify welfare regimes, including debates about their boundaries and how to assess their effects that we do not have space to discuss here (see Bambra 2007; Dahl et al. 2006; Kelly-Irving et al. 2023). 5 Despite some differences in the criteria used to distinguish them, however, there is considerable overlap in how most studies of welfare regimes classify the countries in our study. In general, they distinguish among (what we will call) Nordic welfare regimes (Denmark, Finland, Norway, and Sweden), continental welfare regimes (Belgium, France, Germany, Switzerland, and the Netherlands), liberal welfare regimes (Australia, Britain, Canada, Ireland, and the United States) and southern European welfare regimes (Greece, Italy, Portugal, and Spain), and that is the typology we will use here (eg, Eikmo et al. 2008).
Construed in broad terms, welfare regimes condition health inequalities in multiple ways (Bambra 2011a; Beckfield et al. 2015). We concentrate here on how they distribute the economic and social resources that we have identified as important to health. First, they redistribute income. As social benefits flow disproportionately to people in the lower rungs of the income distribution, in countries where those benefits are more generous, inequalities in household income should be a less important source of inequalities in health than in countries with more restrictive welfare regimes. Accordingly, we expect income inequality to contribute less to health inequality in the relatively generous Nordic welfare regimes and more in the liberal welfare regimes that offer fewer benefits (hypothesis 1).
Second, as Esping-Andersen (1990, 2015) has observed, welfare regimes do not simply redistribute income. By reinforcing or undermining existing status orders, they also promote distinctive systems of social stratification (Birkelund 2006). He noted that continental welfare regimes tend to allocate benefits in terms that reinforce existing status hierarchies, whereas the Nordic regimes tend to equalize social status by allocating more benefits on the basis of citizenship. This implies that differences in social status between socioeconomic groups may be higher and contribute more to health inequalities in countries with continental welfare states than in those with Nordic welfare regimes (hypothesis 2).
Third, welfare regimes affect social connectedness. It is well known that people in lower socioeconomic positions tend to depend more heavily on their families for social connectedness than people in higher positions, who often have wider networks of connections (Ajrouch, Blandon, and Antonucci 2005; Bianchi and Vohs 2016; Carey and Markus 2017). The welfare regimes of southern Europe accord families especially important roles in the provision of care (Ferrera 1996; Scheepers, Grotenhuis, and Gelissen 2002; Naldini 2016). Therefore, by reinforcing family-based social networks, southern European welfare regimes may improve the social connectedness of people in lower socioeconomic positions, reducing the contribution that class-based differences in social connectedness make to inequalities in health in these nations (hypothesis 3).
Varieties of Capitalism
However, welfare regimes are not the only source of structural factors affecting health. An influential literature on comparative capitalism identifies other features of the political economy likely to affect the distribution of resources important to health (Amable 2003; Hall and Soskice 2001; Hancké et al. 2007; Thelen 2014; Witt et al. 2018). Although there is some debate about how to classify political economies, there is widespread agreement on the importance of differences among four types of political economies (which we call): social democratic economies (Denmark, Finland, Norway, and Sweden), continental economies (Belgium, France, Germany, Switzerland, and the Netherlands), liberal market economies (Australia, Canada, Ireland, the United Kingdom, and the United States) and southern European economies (Greece, Italy, Portugal, and Spain). These categories overlap with those used to distinguish welfare regimes, partly because social policies are often configured in response to the organization of the political economy (Estevez-Abe, Iversen, and Soskice 2001; Hassel and Palier 2020).
We can summarize the salient differences in these political economies only briefly. Hall and Soskice (2001) distinguished liberal market economies, where firms rely mainly on competitive markets to coordinate their endeavors and favor workers equipped with general skills, from continental economies, where trade unions are stronger and firms rely more heavily on corporatist mechanisms for strategic coordination among producer groups to manage their endeavors. They also favor employees with industry-specific skills acquired through extensive vocational training schemes. Social democratic economies are similar but distinguished by encompassing trade unions committed to more egalitarian wage structures and social benefit systems more oriented to worker mobility (Pontusson 2005). In the southern European economies, vocational training is also important, but trade unions are weaker, strategic coordination is more reliant on the state, and the incidence of small firms and self-employment is higher (Burroni, Pavolini, and Regini 2022).
Structural variations across these types of political economies carry implications for the distribution of at least three resources central to health. The first is income. Because their trade unions are weak and their firms rely on competitive markets to compensate labor, liberal market economies tend to have high levels of income inequality. In Europe stronger trade unions and coordinated wage bargaining depress levels of income inequality, especially in social democratic economies whose encompassing trade unions are more committed to wage compression (Thelen 2014). Accordingly, we expect income inequality to make the largest contribution to inequalities in health in liberal market economies and the smallest contribution in social democratic political economies (hypothesis 4).
The distinctive skill systems of political economies also distribute access to education in terms that may feed into inequalities in health. Where access to good jobs and the material perquisites that promote good health depends on educational credentials that are widely available to the populace, we should expect class-based differences in educational credentials to contribute less to inequalities in health. Conversely, where access to a good job is dependent on attaining specialized credentials in stratified educational systems that track people from a young age, inequalities in educational attainment should be larger, more closely linked to class origins, and hence more strongly associated with socioeconomic inequalities in health.
These differences correspond to those found between the skill systems of liberal market economies and the more coordinated economies of Europe. In liberal market economies, firms rely on the general skills conferred by formal education at the secondary or tertiary level to which large proportions of the population have access. In Europe, by contrast, securing a good job is highly dependent on acquiring the credentials conferred by specialized training regimes that people enter at a young age (Busemeyer and Trampusch 2012). Hence, we expect inequalities in educational attainment to be more closely associated with health inequality in the coordinated political economies of Europe than in liberal market economies (hypothesis 5).
Finally, differences in the managerial systems of these political economies affect how much control people in lower level positions are likely to have over the pace and direction of their work. Because firms in liberal market economies tend to rely on employees applying general skills to multiple tasks, a larger proportion of lower level employees in these economies have significant levels of discretion over their work (Guillén 1994; House et al. 2004). In the continental political economies, by contrast, many firms retain elements of hierarchical systems of management that limit the autonomy of lower level employees (Maurice, Sellier, and Silvestre 1984). Hierarchical management systems are also prominent in southern Europe, but larger numbers of workers there enjoy more autonomy because so many work for small firms or in self-employment (Cetrulo, Guarascio, and Virgillito 2020). In the Nordic political economies, where many firms have embraced team-based approaches to management, employees should also have more autonomy in the workplace than those in continental political economies (Dickmann, Brewster, and Sparrow 2016). These considerations suggest that inequalities in the distribution of autonomy at work should contribute less to health inequality in liberal market economies and more in continental political economies, with the Nordic and southern European political economies somewhere in between (hypothesis 6).
The Structure of Social Relations
Alongside this structure of economic relations, a structure of social relations also distributes resources important to health. Construed in broad terms, of course, the structure of social relations bears on health in many ways, including through the patterns of gender and race relations it embodies (Cockerham 2007; Read and Gorman 2012; Williams 2012). However, to delimit the inquiry, we concentrate here on two dimensions of social structure that have often been associated with health, are likely to vary between occupational classes, and for which there is measurable cross-national data, namely, the distribution of social connectedness and social status. More research is needed into how variations in social structure condition inequalities in health, but this component of our analysis can be read as an indication that there is promise in such research.
In contrast to the literatures on welfare regimes and varieties of capitalism, scholarly research on social structure does not yield clear-cut national typologies. But cross-national studies of social networks carry implications for how social connections are distributed across socioeconomic groups. Pichler and Wallace (2009) observed, for instance, that class-based differences in the strength of social connections are smaller in countries where income inequality is lower (see also Letki and Mierina 2015). This suggests that class-based differences in social connectedness may contribute relatively less to health inequality in the Nordic countries, where generous welfare states and coordinated wage bargaining reduce income inequality, than they do in liberal market economics where we expect income inequality to be higher (hypothesis 7).
Cross-national differences in kinship relations may also affect class-based difference in social connectedness. Hollinger and Haller (1990) found, for instance, that people in Italy, Hungary, and Austria have much closer family connections than people in the United States, Australia, and Britain. Because people in lower socioeconomic groups tend to depend on their families for social connectedness more than people in upper groups do, it follows that, where kinship ties are stronger, class-based differences in levels of social connectedness may be smaller than they are elsewhere (Carey and Markus 2017). Some of these differences are visible in indicators for the strength of family ties in Table 1 (see also Alesina and Giuliano 2014). The implication is that inequalities in social connectedness may contribute less to socioeconomic inequality in health in the southern European countries where kinship relations are stronger and reinforced by the welfare regime (hypothesis 8).
Social status is also a resource associated with health. Thus, cross-national variations in the shape of the status hierarchy should affect the health gradient (Marmot 2004). In countries where a steep hierarchy ascribes substantially more prestige to people in upper socioeconomic groups than to those in lower groups, inequalities in status should contribute more to socioeconomic inequalities in health than in countries where the status hierarchy is flatter; and there is evidence that the status hierarchy varies across countries (Brashears 2008; Fiske et al. 2016; Ravlin and Thomas 2005). Once again, the literature does not yield national typologies. But the status hierarchy is likely to be affected by ideas about who deserves to be seen as full members of the national community of the sort embodied in national citizenship regimes and collective narratives about a nation’s past and future (Hall and Lamont 2009; Kunovich 2009).
Therefore, we expect that social status will be distributed more equally in countries with more inclusive citizenship regimes. There are few good measures for assessing the inclusiveness of such regimes, especially with respect to race, but citizenship regimes emphasizing “civic” as opposed to “ethnic” nationalism are generally deemed more inclusive of immigrants, and they may be more inclusive in general. On this criterion, the measures drawn from the analysis of Vink and Bauböck (2013) and reported in Table 1 indicate that the citizenship regimes of the Anglo-American democracies are the most inclusive (see also Banting and Kymlicka 2017; Reeskens and Hooghe 2010). Similarly, we expect the status hierarchy to be flatter in the settler societies of Canada, Australia and the United States, whose national narratives emphasize a “melting pot” or “multiculturalism” in contrast to the narratives of European societies, where the legacies of older status hierarchies remain stronger (Bouchard 2013; Claybourn 2019). The implication is that class-based differences in social status should contribute less to health inequalities in the Anglo-American democracies than they do in many European countries (hypothesis 9).
Data, Measures, and Estimation Strategy
We have focused on five types of resources—income, education, social connectedness, autonomy at work, and social status—that are both important to health and distributed unequally across socioeconomic groups. This theoretical discussion raises three empirical questions. First, how much does inequality in access to each type of resource contribute to inequality in health? Second, how does the contribution of each resource to health inequality vary across countries? Third, to what extent do cross-national variations in the sources of health inequality reflect macro-level differences in welfare states, varieties of capitalism and the structure of social relations?
Data and Measures
To answer these questions, we use data from the World Values Survey and European Values Survey data sets (Inglehart et al. 2014) that others have used to assess the determinants of inequalities in health (e.g., Beckfield et al. 2013; Jen, Jones, and Johnston 2009). We use all waves with the relevant measures, including six from the World Values Survey and four from the European Values Survey running from 1981 to 2020. Each national survey includes responses from at least 1000 adults, and our analyses use calibration weights (on the basis of age, gender, education, and region within each country) to reduce bias due to differential nonresponse and missing data. Because our analysis requires more variation in welfare states and types of capitalism than Europe offers, this is the only source of relevant cross-national data we have found. We focus on developed societies where chronic diseases associated with the resources examined here, rather than infectious diseases, are usually the most important causes of mortality, and we consider only western democracies to rule out the effects of communism and transition from it which, in contrast to regime change in southern Europe, had dramatic effects on health (Siddiqi, Bobak, and Hertzman 2009). We restrict the analysis to the working age population (25–64 years) because our focus is on differences between occupational classes. This yields a data set of approximately 70,000 individuals with health and occupational group data, across 21 Organisation for Economic Co-operation and Development countries. Our substantive covariates differ in their country coverage, as well as item nonresponse, yielding samples in the subsequent analyses of between around 26,000 and 60,000 respondents. Measures for social status are available only in some countries, and the data for it are drawn primarily from the 2005–2009 and 2017–2020 waves.
We measure health with a question about the state of the respondent’s health, counting responses of “very good” and “good” as good health, and “fair,” “poor” or “very poor” as poor health, as many other studies do. Self-reported health has been found to be a good proxy for general health (Balaj 2022; Idler and Benyamini 1997), and following the practice of most studies using this variable, we dichotomize it to reduce measurement error (Aldabe et al. 2011; Balaj et al. 2017; Schutte et al. 2013). Although cultural differences can yield cross-national variations in how people with similar levels of health report the state of their health, those should have little effect on our results because our principal comparisons are between groups within individual countries; and, although women generally rate the state of their health lower than men, this should not affect our results because they are based on representative samples of both men and women. Our estimates for the occupational health gap may be biased upward because people with lower levels of education tend to report poorer levels of health for the same health status; but this should not affect our analysis of the contribution that various resources make to the health gap. For our purposes, perceived health may also be a superior measure of health because it better reflects the lived experiences of individuals (see Balaj 2022).
Because we are especially interested in class-based differences in health, we focus on difference in average health between people in different occupational classes. Although some studies use levels of income or education to assess the health gradient, we think that income does not capture class position as well as occupation; and, in contemporary economies where tertiary enrollments have expanded, recent research reveals substantial variations in the quality of jobs and incomes secured by people with higher education (Ansell and Gingrich 2021; Kitschelt and Rehm 2022). Thus, we believe that occupational position provides a better measure for class-based differences in health, and we treat it as an exposure variable. In this context, because the levels of education or income secured by people in similar occupations vary across countries, they can be construed as separate types of resources available to people in those occupations.
Our indicator for occupational position is the occupation of the respondent, divided into five categories paralleling those used by Erikson and Goldthorpe (1992) to identify social classes: professional or managerial, high-skill nonmanual workers, low-skill nonmanual workers, high-skill manual, and low-skill manual workers (see also Galobardes, Lynch, and Smith 2007). For details, see Table A2 in the Appendix. We measure health inequalities by comparing the average health of a “lower occupational group” composed of low-skill manual workers to an “upper occupational group” of professional or managerial workers, constituting 17 percent and 26 percent of the pooled sample, respectively. Robustness tests indicate that, measured in these terms, inequalities in health do not vary significantly over time in this data set.
Our measures for the five resources of interest are as follows. Income is measured by the decile of the national income distribution into which the respondent’s household income falls. The respondent’s level of education is their highest level of educational attainment divided into three categories corresponding to tertiary education (age 21 or above), completion of secondary education (ages 17–20), and less than complete secondary education (ages 16 and younger). 6 To capture the extent of a respondent’s social connections, we use a modified version of the “social network index” devised by Berkman et al. (2004:168), which combines marital status, ties to family and friends, and membership in voluntary associations into a composite indicator reflecting four levels of social connectedness. We measure how much autonomy or control a person has over the pace and direction of their work with responses on a 10-point scale to a question asking how much independence the respondent has in performing tasks at work (for details of these measures, see Table A1).
We assess a person’s social status with a question asking whether they would describe themselves as belonging to the upper, upper middle, lower middle, working, or lower class. This is a relatively crude measure, but it prompts respondents to place themselves on a familiar social pyramid, and in ancillary tests it performs as expected for a variable measuring social status (i.e., it is correlated at modest levels with income and education but varies independently of both). Using data from the 1987 wave of the International Social Survey Program, because it includes this measure and one for self-placement on a social ladder (a variable commonly used to measure subjective social status), we find that the two measures are closely correlated (details in Table A7).
Estimation Strategy
There are two stages to our empirical analysis. To assess the relative contribution that inequalities in the distribution of each resource generally make to inequality in health, we begin with a mediation analysis on the full pooled sample of a type widely employed in such research (Aldabe et al. 2011; Balaj et al. 2017; Moor et al. 2014). Although other studies point to the importance of these resources for health, we know of none comparing the relative contribution that each makes to health inequality.
Two features of our analysis deserve note. Because we lack panel data, we do not model any time lags between access to these resources and a person’s health. In this approach we follow most other studies of such issues (e.g., Lynch et al. 2004); and, because we focus on differences in the levels of resources available to individuals in two occupational groups that are likely to have been present in broad terms over their life course, the cross-class differences in health that they yield are not likely to depend heavily on such time lags. Similarly, we think it reasonable to assume that the relationship between access to each resource and health is generally stable over the period covered by our data.
The mediation analysis is conducted as follows. After confirming that our measures for each resource are significantly associated with self-reported health and occupation, we conduct logistic regressions for the relationship between self-reported good health and both occupational group and these resources, with fixed effects for country and survey year, age, and gender. Conceptually, the contribution of each resource to occupational inequalities in health is the degree to which the health advantage of the professional or managerial group is decreased by accounting for the resource. Operationally, we calculate this as the percentage change in the coefficient on professional or managerial occupation (with low-skill manual workers as the reference category). We decompose the contribution each resource makes into its direct contribution and its indirect contribution through other resources. To exploit the full data set, we omit social status from this part of the analysis but bring it in later when we consider cross-national variation. The noncategorical variables are rescaled to vary between 0 and 1 and estimates are y-standardized to account for variation in unobserved heterogeneity across models, making comparison across models possible (Mood 2010:74).
In the second stage of the analysis, we are interested in establishing whether inequalities in the distribution of specific types of resources contribute more to health inequality in some countries than in other countries. For this purpose, we need to consider both how unequal the distribution of a given resource is and how important that resource is to securing good health there. Where the national distribution of a key resource, such as income, is more unequal, it will contribute more to health inequality. But any one resource might be more useful for securing good health in some countries than in others. For instance, a person’s income might matter more to their health in countries where people must purchase health care than in countries where health care is publicly provided.
Therefore, we take a three-step approach to estimating the contribution that each type of resource makes to national health inequality. First, for each national sample, we estimate a coefficient indicating how much the probability of reporting good health changes with a one-unit change in possession of the relevant resource, such as income or social status. We do this for each resource in nationally specific linear probability models conditioned on age, gender and survey wave. Virtually all the coefficients in this estimation are statistically significant at the .05 level (results in Figure A1). Robustness tests in which we also condition on the respondent’s employment status yield only slightly different estimates that do not change the substantive interpretation of the results.
Second, we estimate how unequal the distribution of each resource is in each country, expressed as the ratio between the average level of that resource available to professional or managerial workers and the average level available to low-skill manual workers. Third, using our country-specific estimates for how the probability of reporting good health changes with a unit change in each resource and our knowledge of the levels at which each resource is available to low-skilled manual and professional employees in each country, we calculate a measure that we label the “resource-predicted health gap” for each resource in each country. This measure indicates, in percentage terms, how many more low-skilled manual workers could be expected to report good health if they had the relevant resource at the average levels at which professional or managerial workers in that country do. It allows us to compare how much inequalities in access to specific types of resources contribute to inequalities in health between people in upper and lower occupational positions, both within nations and across them.
Empirical Results
The Relative Contribution of Different Resources to Health Inequalities
We report, first, on the results of the mediation analysis on the full sample, which compares in cross-national terms the relative contribution that inequalities in the distribution of different economic and social resources make to the occupational health gap. Figure 1 shows how much of the difference in good health found between people in an upper occupational class of professional or managerial workers and a lower occupational class of low-skill manual workers can be attributed to differences in their access to four key resources (full estimation in Table A4). Since income is a multipurpose instrument for securing many of the material requisites for good health, as might be expected, inequalities in income contribute the most to occupational inequality in health. However, class-based differences in how much control people have over their work and in their levels of education also make significant contributions. Differences between the two occupational groups in levels of social connectedness account for less, but they suggest that inequalities in social, as well as economic, resources can be important to inequalities in health.

Contributions of economic and social resources to socioeconomic inequality in health (full sample).
Cross-National Analysis
Because we expect the macro-structures of each nation to distribute economic and social resources differently, we also expect to see cross-national variation in how much inequalities in each resource contribute to inequalities in health. We assess that variation by estimating “resource-predicted health gaps” for each resource in each country with the procedures we have noted.
These gaps are reported in Table 2. In the first row, for instance, under “Income” for Australia, the figure of 10.15 indicates that if low-skill manual workers in Australia had the same average income as professionals and managers there, we could expect the percentage of low-skill workers in Australia reporting good health to increase by about 10 percentage points (from a level of 65 percent to about 75 percent). Similarly, the figure 2.0 in the first row of the fourth column indicates that if low-skilled Australian workers had the same level of autonomy at work as professionals and managers do, we would expect the proportion of low-skill Australian workers reporting good health to rise by 2 percentage points. Column 1 of this table also provides a measure for the overall level of health inequality between people in the upper and lower occupational groups in these national samples, on the basis of adjusted risk ratios calculated from predicted probabilities conditioned on age and gender (as in Beckfield et al. 2013; McNamara et al. 2017). See Table A5 for separate results for men and women.
Resource-Predicted Health Gaps, by Country.
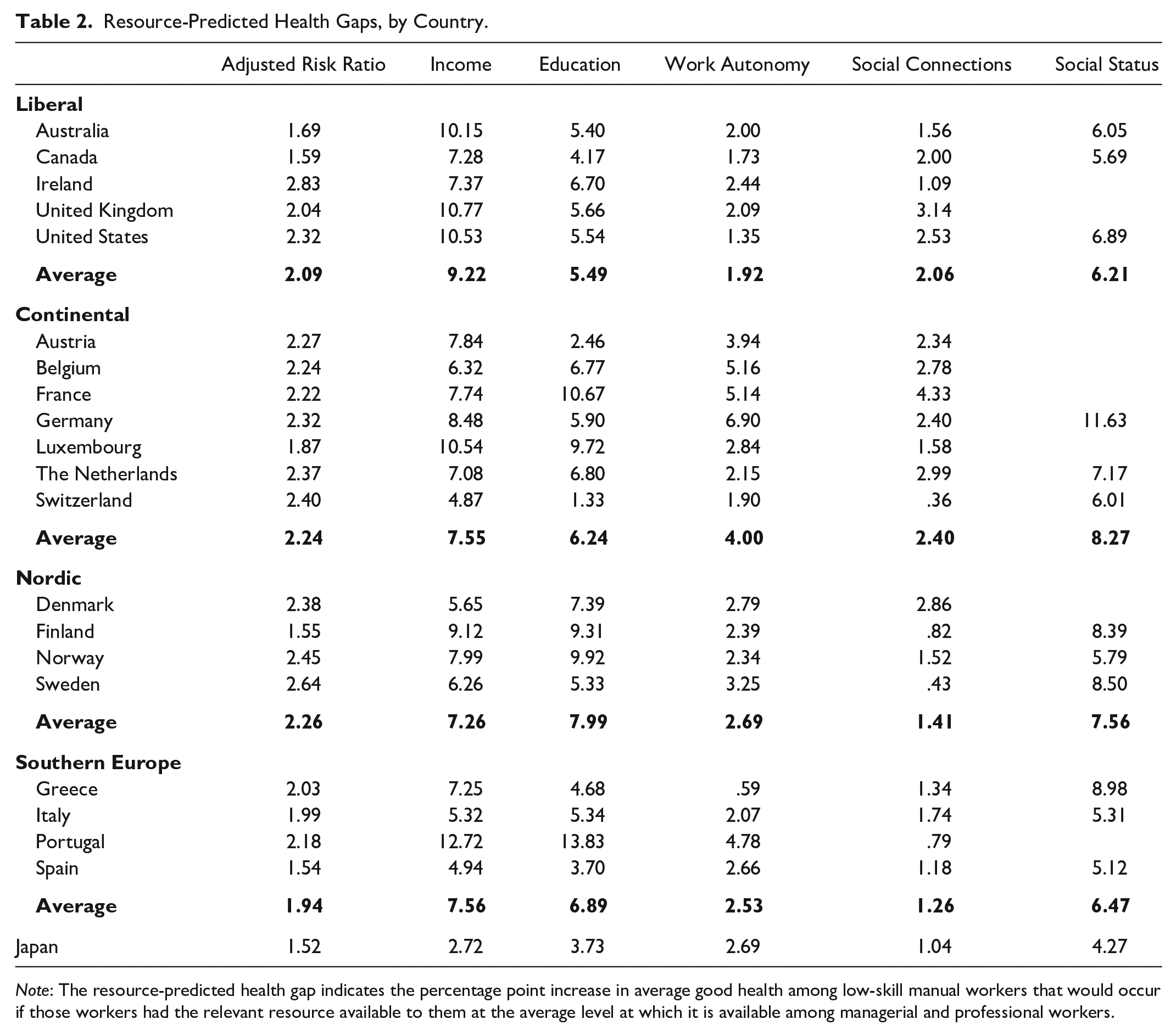
Note: The resource-predicted health gap indicates the percentage point increase in average good health among low-skill manual workers that would occur if those workers had the relevant resource available to them at the average level at which it is available among managerial and professional workers.
Several conclusions follow from the estimates in Table 2. First, they indicate that the sources of socioeconomic inequality in health vary substantially across countries. Differences across occupational classes in social connectedness and autonomy at work, for instance, contribute more than three times as much to health inequality in some countries as in others. Second, as the mediation analysis indicated, income inequality makes especially large contributions to the health gradient in all countries. However, inequalities in access to education and social resources such as social connectedness and social status are also important sources of it. Cross-national variation in how much any given resource contributes to health inequality (reading down the columns) is driven largely by how unequal the distribution of that resource is in each country. Within countries, the relative contribution of each resource to health inequality (reading across the rows) is driven both by how unequal the distribution of the resource is in that country and by our estimates for how closely each type of resource is associated with good health in that nation.
Because other factors beyond the scope of this study also condition the health gradient, we are not trying to provide a full explanation for variations in its steepness. But these results suggest that the socioeconomic gradient in health is not generated primarily by one type of inequality, such as income inequality, but by how the economic and social structures of a society distribute multiple kinds of resources. All the resources examined here are correlates of social class in that they are distributed unequally across upper and lower occupational groups (Link and Phelan 1995). But this analysis reveals significant national differences in the extent to which access to any given resource varies by occupational class, and hence how much that resource contributes to health inequality there. It also suggests that within countries, a more equal distribution of some types of resources, such as social connectedness, may offset the adverse health effects of more unequal distributions of other resources.
Macro-level Structures and Health Inequalities
We turn now to the question of how differences in welfare states, varieties of capitalism, and social structures contribute to cross-national variation in the sources of health inequality. Do the national patterns in resource-predicted health gaps reported in Table 2 conform to the expectations outlined our discussion of under “Cross-National Variation in Economic and Social Structures”?
For ease of interpretation, Table 2 groups the countries in this study into four categories corresponding to the broad classifications found in prominent theories of welfare regimes and comparative capitalism (see also Figure 2). The first point to note is that, within each group of countries, there is still considerable cross-national variation in the magnitudes of the resource-predicted health gaps. This finding indicates that the macro-level structures associated with welfare regimes and varieties of capitalism cannot fully explain cross-national variation in the sources of the health gradient. That is to be expected, as distinctive features of each nation beyond the scope of this analysis condition the distribution of these resources. However, the cross-national patterns in these resource-predicted health gaps are congruent with many of the predictions we have drawn from prevailing theories about the effects of macro-structures on the distribution of resources.

Resource-predicted health gaps within each group of countries.
Welfare Regimes
We begin with the anticipated effects of welfare regimes. As expected, on average, income inequality makes the largest contribution to the occupational health gap in countries with liberal welfare regimes, and the smallest in the Nordic countries with generous welfare regimes (hypothesis 1). Class-based differences in social status also contribute more to health inequalities in the European countries with continental welfare regimes, which tend to reinforce existing status hierarchies, than they do elsewhere (hypothesis 2). Class-based differences in social connectedness contribute the least to the occupational health gap in southern Europe, where we expect family-oriented welfare regimes to reduce the differences between people in different occupational classes in social connectedness (hypothesis 3).
Varieties of Capitalism
Moving to effects that might be associated with varieties of capitalism, income inequality contributes considerably more to inequalities in health in liberal market economies than it does in the coordinated economies of Europe (hypothesis 4). In liberal market economies, where large proportions of the population acquire similar educational credentials conferring general skills, class-based differences in levels of education are also less closely associated with these inequalities in health than they are in the coordinated economies of Europe, where securing a good job is more dependent on acquiring specialized educational credentials at a young age (hypothesis 5). But there is also notable variation among European countries on this measure, which may reflect important differences in their educational systems not considered here. As expected, class-based differences in autonomy at work contribute less to inequalities in health in liberal market economies, where managerial practices usually accord more discretion to lower level workers, than they do in the continental economies with more rigid managerial hierarchies (hypothesis 6). Differences in autonomy at work also contribute somewhat less to health inequality in the Nordic political economies, which have more flexible management systems, and in most countries of southern Europe, where large numbers of people are self-employed or work in small firms, although Portugal is a major outlier.
Social Structure
There is also evidence that health inequality is affected by variations in social structure. Inequalities in social connectedness make only modest contributions to health inequality in the Nordic countries, where generous welfare regimes and social democratic economies reduce the levels of income inequality associated with class-based differences in social connectedness (hypothesis 7). Class-based differences in social connectedness also make especially small contributions to these occupational inequalities in health in the countries of southern Europe, where close kinship ties are a prominent feature of the social structure (hypothesis 8).
Our findings about the contribution of the status hierarchy to health inequality must be treated with caution because our measure of social status is imperfect, and we have it only for a smaller sample of countries. The results conform to our expectation that inequalities in social status will contribute less to inequalities in health in settler societies with inclusive citizenship regimes. On average, class-based differences in social status contribute less to the occupational gap in health in Canada, the United States, and Australia than they do in the other groups of countries (hypothesis 9). However, the contribution of social status to health inequality is also notably low in Italy and Spain, two countries that do not have especially inclusive citizenship regimes. This suggests, not surprisingly, that other factors also affect the shape of a nation’s status hierarchy.
Of course, this is an observational analysis that cannot identify causation, and there is national variation in these results that the broad macro-level structures on which we focus cannot explain. In those respects, this should be read as an exploratory analysis designed to open up new avenues of research. However, it is striking how many of the aggregate patterns in Table 2 are congruent with what we would expect from prevailing theories about welfare regimes, varieties of capitalism and comparative social structure. These findings suggest that cross-national variations in such macro-level structures condition both the shape and sources of the socioeconomic gradient in health.
Conclusion
In this article we explore cross-national variation in the sources of socioeconomic inequalities in health. To a body of work often focused on the effects of income inequality, we bring a perspective that emphasizes how inequalities in access to a wider range of economic and social resources bear on health outcomes. We ask how the macro-level structures associated with welfare regimes, varieties of capitalism and national social structures might condition the health gradient by virtue of how they distribute those resources. In so doing, we bring social science frameworks developed for other purposes to bear on inequalities in health, with a view to moving issues of health inequality into a more central position on the interdisciplinary agendas of social science.
Our premise is that five key resources—income, access to education, social connections, autonomy at work, and social status—contribute to a person’s health but are distributed unequally across socioeconomic groups. That is widely accepted, but the relative contribution that each makes to health inequality is rarely examined. Using mediation analysis on a large cross-national sample of people from 21 developed democracies, we compare the relative contributions that access to different types of resources makes to socioeconomic inequality in health. We find that income inequality matters most, followed by autonomy at work and access to education, but that various features of social structure also matter.
We also consider how the macro-level structures associated with distinctive welfare regimes, varieties of capitalism and social structures give rise to cross-national variation in the sources of the health gradient by distributing these resources in different ways. To investigate this, we draw from prevailing theories about these macro-level structures a set of expectations about how they might condition the sources of socioeconomic inequalities in health, and then compare those expectations with estimates for cross-national variation in the sources of health inequality. The results provide presumptive evidence that these macro-level structures condition the sources of the health gradient. By looking beyond welfare regimes, on which most of the related literature focuses, to varieties of capitalism and comparative social structures, we point to promising lines of further research. Our results invite political economists, who often study income inequality, to devote more attention to inequalities in health, and social epidemiologists, who often emphasize the behavioral correlates of health, to devote more attention to the macro-structures of societies.
There are several ways in which this research can be extended. We consider cross-national variation in the distribution of resources in terms that aggregate over time. We think that this approach is the best way to assess the effects associated with durable macro-level structures because it discounts short-term fluctuations in resource distributions in order to focus on persistent cross-national differences in them. However, if the distribution of any one resource, such as income, becomes more unequal over time, our analysis suggests that this resource will then contribute more to the health gap between the affected occupational groups.
Income inequality did increase over this period, but with limited implications for our comparative conclusions because it increased the most in liberal market economies, where it was already a major determinant of health inequalities, and the increases were concentrated at the top end of the income distribution, where changes are generally less consequential for health inequality than at its bottom end (Laporte 2002). Nevertheless, welfare regimes and varieties of capitalism are gradually changing in response to secular shifts associated with globalization and the transition to a knowledge economy (cf. Hassel and Palier 2020; Hemerijck 2013), and on some measures, health inequalities in Europe are also changing (Mackenbach et al. 2016). Therefore, there is a case for following up this analysis with others that examine how changes over time in macro-level structures may be inspiring shifts in the distribution of resources that impinge on inequalities in health.
This analysis might also be extended to other parts of the world with different welfare regimes or varieties of capitalism, as in Asia or Latin America (Schneider 2013; Witt and Redding 2014), although the “capabilities” logic underpinning our analysis implies that the relevant effects may be more difficult to identify in regions where infectious diseases are more prominent causes of morbidity. A wider comparative ambit would also provide more variation on dimensions of social structure that we have not been able to assess. As we have noted, alongside social networks and social hierarchies, there are other dimensions of social relations, including gender relations and racial divisions, that can impinge on health inequalities. These factors may not only contribute to inequalities in health between occupational groups; as recent arguments about “social determination” suggest, they may also be the basis for deep-seated inequalities in health rooted in differences other than occupation (Williams 2012; Waitzkin, Pérez, and Anderson 2021).
This investigation also carries some lessons for policy makers. Following the Black report (Black 1980), policy makers became more attentive to the social determinants of health, but their initiatives usually focused on redistributing income or discouraging risky behaviors (Lynch 2020). The perspective advanced here suggests that inequalities in health depend, not only on such factors, but also on how social resources, such as connectedness and social status, are distributed (see also Klinenberg 2019).
These social resources are rarely the direct objects of public policy, but they are often inadvertently affected by policies designed for other purposes. Zoning regulations that limit the number of small eating places, for instance, or the closing of libraries and old age centers to secure budgetary economies can foreclose opportunities for people to meet and form social connections. Attaching stigmatizing eligibility requirements to social benefits may save money but reduce the social status of the recipients, with adverse effects on their health (Hall and Taylor 2009). Accordingly, this study suggests that policy makers concerned about inequalities in health should be attentive, not only to the distribution of economic resources, but to the conservation of social resources, as well as economic ones. Just as there are multiple sources of the health gradient, there are multiple ways in which policy makers can address it.
Supplemental Material
sj-pdf-1-srd-10.1177_23780231231174832 – Supplemental material for The Structural Sources of Socioeconomic Inequalities in Health: A Cross-National Perspective
Supplemental material, sj-pdf-1-srd-10.1177_23780231231174832 for The Structural Sources of Socioeconomic Inequalities in Health: A Cross-National Perspective by Lucy Barnes, Peter A. Hall and Rosemary C. R. Taylor in Socius
Footnotes
Acknowledgements
All authors contributed equally to this article and their names are listed in alphabetical order. We want to thank Susan Bell, Sandy Jencks, and two reviewers for Socius for their helpful comments on earlier versions of this article.
Supplemental Material
Supplemental material for this article is available online.
1
Note that their concepts of “knowledge” and “power” are more encompassing than our concepts of “access to education” and “autonomy at work,” but our formulations capture some features of the mechanisms that Link and Phelan had in mind.
2
Wealth can also be an important resource for health, operating much as income does, especially for older people on retirement incomes (Semyonov, Lewin-Epstein, and Maskileyson 2013). As we lack measures for it, we restrict this inquiry to people in the working age population.
3
Some efforts to identify the effects of welfare states on inequalities in health, for instance, may be picking up the effects of a specific variety of capitalism rather than of the welfare state.
4
For reviews of these large literatures, see, on varieties of capitalism, Clift (2014:199–229), Hancké, Rhodes, and Thatcher (2007), and Witt et al. (2018); on welfare regimes, Powell, Yöruk, and Bargu (2020), Morel, Palier, and Palme (2012), and Hemerijck (2013); and on systems of social stratification, ![]() .
.
5
These include debates about how welfare regimes are gendered, whether they encompass more than standard social policies, and whether to emphasize their effects on inequalities measured in relative or absolute terms or on specific social groups–many of them inspired by the paradox that health inequalities are not especially low in the generous Nordic welfare regimes (for reviews, see Bambra 2011a; Bambra et al. 2009; ![]() ).
).
6
We use these three categories to provide a standardized measure of educational attainment because the World Values Survey does not provide consistent International Standard Classification of Education categories, and the meanings of their educational categories vary with national educational systems.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.