
Abstract
Most developed countries hold significant quantities of medical supplies in reserve for emergency response. Due to high handling costs and remote storage locations, such stocks are typically not used for day‐to‐day operations. In consequence, the expiry of reserve supplies (without use) is a significant problem. One possible remedy for such wastage is to donate large batches of dated supplies to developing nations, which often do without adequate medical supplies in their health systems. Here, we focus on personal protective equipment (PPE) and similar products, which have low risks associated with aging and safety. However, the international community is cautious about donating dated medical supplies, with the World Health Organization explicitly recommending against it. Issues of safety, while important, are not the primary concern as recent studies have shown expiration dates to be conservative. Instead, most concerns relate to macrolevel effects on the recipient country. Taking safety as given, we carefully model the incentives in the medical supplies donation supply chain, providing insights into the likely effects of corruption and impacts on the local industry. Overall, we find that the impact of donation is not monotone in the quality of donated products. In particular, dated donations whose quality is slightly lower than the quality of products in the local market are likely to be more beneficial than fresh donations; thus, we suggest that the international community reconsiders its stand on banning donations from dated reserves. We provide concrete guidelines for such donations and suggest a possible path for implementation of a donation program.
INTRODUCTION
A large portion of the world's population suffers from scarce healthcare resources, which can lead to unsafe practices including reusing normally disposable items such as surgical gloves and masks, and using diluted hand‐wash, and so forth (Ider et al., 2012; Okwen et al., 2011). It is estimated that up to 70% of injections in developing countries are administered with reused and unsterilized syringes and needles (Khamassi, 2012). This situation is in sharp contrast to the advanced health systems in developed countries. The U.S. healthcare system wastes a large quantity of medical supplies that are in usable condition; for example, Wan et al. (2015) estimated that just 4% of all hospitals nationwide waste at least $15.4 million of supplies annually. The large gap between deprived areas and developed countries suggests the possibility of donations. In this paper, motivated by the huge waste of medical products in developed countries, we focus on donations of PPE‐type (personal protective equipment) products.
A key source for such donations could be the medical reserve stocks in developed countries. Medical reserve refers to the back‐up medical supplies held by a government to prepare for emergencies. Encouraged by the World Health Organization (WHO), most developed countries hold such reserves, which typically consist of antiviral drugs, vaccines, syringes, disposable gloves, masks, and gowns. Because these products usually have a fixed use‐by date and the likelihood of using them for emergencies during that shelf‐life is relatively small, these reserves face severe issues with expiration (see below). Further, because some of these reserves have proved inadequate in the face of COVID‐19, we would expect to see many countries rebuild their stocks after the pandemic has passed, and likely to even greater levels than seen previously (Dyer, 2020). This will further exacerbate issues of expiry in a few years' time.
Our focus in this paper is PPE (such as protective clothing, gloves, masks, and respirators) and similar products (like hand sanitizers and syringes). These products share similar features: They are protective, disposable, typically not for repeat use, and are usually labeled with a long fixed shelf life. They have fewer risks associated with aging as the WHO suggests PPE beyond the labeled expiration date “can still be effective at protecting health care providers” subject to the product being inspected before use (WHO, 2020), whereas drugs and vaccines may become unstable and dangerous with age. Further, there are no hazardous waste disposal issues for unused PPE, so there is no concern that the products are being donated to avoid disposal costs, as there can be with other types of medical supplies (e.g., Pinheiro, 2008).
PPE and similar products need to be replaced after a number of years of sitting in a reserve because eventually their seals are considered nonsterile. An inspection of the U.S. Department of Homeland Security (DHS') reserve stock reported 84% of examined hand sanitizer was expired with some by up to 4 years, and 200,000 respirators were beyond the 5‐year manufacturer's guaranteed usability (US DHS, 2014). In preparation for the COVID‐19 pandemic, Ontario, Canada, found roughly 55 million N95 masks and other medical equipment had passed their expiration date (Martell & Warburton, 2020). However, old sanitizer is likely more effective than diluted sanitizer and an old respirator will be more effective than no respirator. These reserve products, if used for a population that lacks adequate medical resources, could greatly improve healthcare outcomes.
Nevertheless, despite the huge potential social benefits, the option of donating aged reserve is not adopted in practice and dated reserve products are typically sent to landfill. The international community has been cautious, yet with inconsistent guidelines and regulations. In a prudential guideline, the WHO discourages donating expiring products, and requires that all donations “should have a remaining shelf‐life of at least one year” when arriving in the recipient country (WHO, 2011). Meanwhile, although acknowledging the WHO's guideline, the American Food and Drug Administration (FDA) states that it is willing to donate expired medicine supplies on “a case‐by‐case basis” (FDA, 2011).
These seemingly contradictory stances do not deny the potential benefits of donation, especially when the recipient areas are extremely short of medical products. Caution regarding donating dated medical supplies can be attributed to four aspects: namely, efficacy—whether it is safe to use products close or past the labeled shelf life (e.g., Saha & Galper, 2013); ethics/fairness—whether such donations sufficiently consider the “rights and worth of different populations” (Pinheiro, 2008); corruption—corrupt bureaus may take advantage of donation to line their own pockets (e.g., Shelley, 2014); and adverse effects on the local industry—donations can fail to help the recipient areas by pushing local suppliers out (e.g., Moyo, 2009).
Efficacy arguments against using dated products are based on the assumption that expiring or expired products, as defined by the “expiry date” label, lose their potency and could be harmful. However, a product does not become unsafe immediately after the labeled expiry date. The labeled date is usually much shorter than the true shelf life, which is typically unknown and is estimated quite conservatively (Pomerantz, 2004). Convincing evidence has been produced by the Shelf Life Extension Program (SLEP), which found 88% of the tested product lots could be extended at least 1 year beyond their original expiration date for an average extension of 66 months (Lyon et al., 2006). To address the efficacy concern, we assume that the donated products will be used within a short enough time span (relative to the long lifetime of the products) that further in‐country degradation is a second‐order effect (and not modeled).
We do not consider the ethical issue of whether it is “fair” for a population to use dated medical supplies, that is, whether it treats people with sufficient dignity (e.g., Tomasini & Van Wassenhove, 2009). Comprehensively studying the fairness aspects would require discussions from a sociological perspective, which is beyond the scope of this study. Instead, we take a more pragmatic approach that currently we have large quantities of usable supplies being dumped in developed countries and large populations doing without suitable supplies in developing nations. We therefore ask whether the recipient nation would be materially better off with these supplies.
From the recipient's perspective, this paper investigates whether dated donation is beneficial when there is the potential for corruption and impacts on the local industry. In particular, we formulate a Stackelberg game between an official who is in charge of the donated supply and a local monopoly supplier who responds to the official's actions (i.e., whether the donation is provided free) and sets the market price. If the market price is forced too low, the supplier cannot cover the overhead cost and will exit the market. The official can be noncorrupt or corrupt, which could lead to different objectives: A noncorrupt official looks to maximize the region's healthcare welfare, which is modeled as a Cobb–Douglas function, whereas a corrupt official aims to maximize his own interests by pocketing the money from selling the donation. To focus on the impact of corruption resulting from the donation, we look at donation‐related corruption, which emerges only when donation stocks are made available. We analyze and compare the region's healthcare welfare and the supplier's decision in three cases: the base case when there is no donation, a noncorrupt official with donation, and a corrupt official with donation.
We find that the value of the donations is not monotonic in their quality, and so dated donations could be more beneficial for the recipient country than fresh donations. Specifically, while very dated donations are certainly not beneficial, fresh donations could make the whole recipient country reliant on donation by driving out the local industry; and further, when coupled with corrupt officials, fresh donations could make the recipient country worse off compared to the case without donation. This is because donation products serve as an alternative to the local products and compete with the supplier. Whether the official is corrupt or not, donation forces the local supplier to lower the market price, and a high quality of donation could drive the supplier's price too low to maintain its operations and cause the supplier to exit the market, which could discourage any further attempts to develop local supply capacity. Our analysis suggests that dated donations of an appropriate quality could alleviate these problems and so provide a viable solution, reducing the adverse impact on the local industry and constraining the negative impact from corruption.
Overall, we recommend reconsidering the bans on donating dated medical products: Such bans may be relaxed if there are no additional safety and ethical issues, for example, when the products (such as PPE) pose low risks of harm and when such donations are well stored (e.g., in the reserve) and are not being donated to avoid disposal costs. There need to be strict requirements on the donation product: The product efficacy needs to be proven; and it is also important that the product quality is lower than that of the fresh product from local suppliers, otherwise the effect on the local market will be too detrimental. This could be achieved through rigorous testing and clear labeling of the product. Although our work shows that donation of slightly dated products can be beneficial, this must be accompanied by safeguards to ensure that other factors not explicitly modeled in the work, such as medical safety, ethical issues, and environmental concerns, are not compromised. For example, donation of dated products with adequate efficacy should be agreed upon by the recipient before these products are made available; otherwise, it could lead to a higher distrust between the recipient and the donor.
The rest of this paper is organized as follows. Section 2 reviews the literature. Section 3 presents our base model of the healthcare supply chain for the product being considered, and Section 4 models two cases where dated donation is provided with a noncorrupt manager and a corrupt manager, respectively. Then, Section 5 compares the three modeled cases and discusses the results. Finally, Section 6 concludes the paper and makes concrete recommendations for implementation of donation programs of dated reserve products.
LITERATURE REVIEW
Our work relates to three broad streams of literature: donation‐related operations, the impact of donation, and corruption. In this section, we review the relevant work and discuss our contributions to the literature.
First, our work contributes to the growing literature on donation‐related operations, particularly for medical supplies donation from the recipient's perspective. One growing topic in donation of medical supplies is medical surplus recovery and allocation; see Zhang et al. (2020) for an overview. With known recipient valuations, Atasu et al. (2017) suggest that a provider‐driven model can improve value provision to recipients, where the donor selects recipients and decides the type and quantity of donations. Zhang et al. (2020) consider private recipient valuations and design a mechanism to enable the donor to select the recipients to serve at each shipping opportunity. Essentially, research on medical surplus recovery studies a resource allocation problem without monetary transfer, where the main focus is matching uncertain supply of medical donations with recipients from a waiting list. In these studies, the matching problem is studied from the donor's perspective, yet the outcomes for donation recipients are not discussed. We take a different perspective and investigate the impact of providing medical supplies donations on the recipient, in line with the call for donations to take the recipient's actual needs into account (e.g., Berenguer & Shen, 2020).
A few studies of donation operations explicitly consider the decision or the outcome on the donation recipient's side. Natarajan and Swaminathan (2014) study the recipient's optimal procurement policy with funding constraints, where the timing of the receipt of previously promised funding from donor agencies is uncertain and constrained. Taylor and Xiao (2014) consider the subsidizing strategy in the distribution channel and investigate the impact of donor subsidy on recipients' access to malaria drugs, and find that the donor should subsidize purchases but not sales. Further, Taylor and Xiao (2019) look at consumer awareness changes in a donation program implemented through a commercial channel, and examine how the donor's optimal subsidy and utility should change with the loss of price control and the level of consumer awareness. While these studies provide important insights informing donor decisions to better help less developed areas, donation quality is not considered and bureaucratic corruption is not discussed. Different from these studies, our work investigates the impact of donation quality from the recipient's perspective, and looks at how donation can affect recipient welfare and the local supplier when confronted with noncorrupt versus corrupt officials.
Our work also contributes to the broader literature on the impact of donation on the recipients. While studies on this topic are relatively limited in the operations management literature, there are extensive discussions in development economics and public health. This body of literature has found that, despite the potential benefits, in‐kind donations can pose a negative price effect, that is, large volumes of donations may shift the supply curve and put pressure on local producers to reduce prices (cf. Awokuse, 2011). Originating from food aid (Schultz, 1960), the price effect has been studied in several empirical investigations of donations of food (e.g., Tadesse & Shively, 2009), used clothing (Frazer, 2008), and shoes (Wydick et al., 2014), but not yet medical donations. While a negative price effect has been found in apparel and shoe donations, mixed findings have been reported for food donations, with the price effect supported in some but not other studies. The varying conclusions from these studies suggest the impact on the local market and the recipient's economy depends on the context and the type of aid. Tadesse and Shively (2009) find that the quantity of food donation influences the extent of the price effect. Specifically, the effect on local prices and local food production is detrimental when the donation shipments exceed the 10% threshold of local production; below this level the impacts appeared to be benign.
Compared to the work on the price effect, discussions about the impact of in‐kind medical donations (new or dated) are more qualitative and narrative. Igoumenidis et al. (2013) discuss the impact of in‐kind drug donations (as opposed to cash) on the recipient and suggest a localized and decentralized approach to manage the aid, so donations can bypass unnecessary procedures and encounter less corruption. Despite the concerns raised regarding dated donations, other voices support the donation of subpar medical supplies. From a medical ethics perspective, Saha and Galper (2013) suggest donations of products that are known to be stable past their expiry date can be made per recipient's request. Overall, though these studies touch the impact of donation quality, they use a qualitative rather than a quantitative approach, and the negative price effect has not been well studied for medical donations. As such, our work contributes by quantifying the price effect for one type of medical donation while looking into the impact of donation quality.
Finally, this work sits within the literature on corruption as we explicitly consider that corrupt members of the supply chain may divert the donated products for their own gains. Underdeveloped countries are particularly vulnerable to corruption and fraud in their healthcare sectors. Partly because the administrative systems are neither well developed nor transparent, leakages of public resources and misuse of medical supplies for private gain are common in these countries (Musau & Vian, 2008). There is evidence that donation provides a chance for corrupt bureaucrats in recipient countries to divert the products for repackaging and resale. For example, the Uganda Minister of Health estimated that half of the medicines accessed by the government for public healthcare were siphoned off (MeTA, 2009). Media reports also claim that medical supplies donated to North Korea are diverted by corrupt officials and sold at local markets (Kim et al., 2013) and that officials in Africa divert and sell donated medicines for their personal profit (Shelley, 2014).
Modeling the role of an official in the donation supply chain, we contribute to corruption studies related to government officials and public products. Due to the difficulties of incorporating all the cost, demand, and supply functions, it is challenging to build a model of bureaucratic corruption (Jain, 2001). Looking at government officials selling government property for personal gain, Sheiffer and Vishny (1993) find that weak governments usually experience high levels of corruption, which is very distortionary and costly. Though bureaucratic corruption is commonly perceived as bad practice, some suggest that corruption may improve efficiency and help growth, given the preexisting distortions in underdeveloped countries (cf. Bardhan, 1997; Mèon & Weill, 2010). Corruption is typically modeled as a principal–agent model in which the government or the citizens act as the principals and aim to reduce the corrupt behaviors of officials (e.g., Acemoglu & Verdier, 2000). Different from the principal–agent setting, Popa (2014) takes the view that corruption can benefit both the corrupt officials and individual citizens, and models corrupt interactions as markets in which public goods are sold. Our results suggest that, depending on the donation quality, corruption can hurt or benefit a recipient's healthcare welfare as well as the local supplier's profitability, and we characterize these conditions. As such, we extend the modeling of corruption to the donation supply chain setting, analyze the impact on the recipient, and obtain managerial insights from the structural results.
MODEL DESCRIPTION
We consider an overall impoverished area/country where there is a shortage of medical products. Donations could help the area improve healthcare, but could also influence the local market and induce corrupt behaviors by officials processing the donated products. In this work, we model the impacts associated with donations of one type of medical product (e.g., PPE), which has a long shelf life and whose properties are deemed to be stable.
The product can continue to be useful after the initial labeled dates, especially if it is well stored. For example, after being in storage for a long time, the strap and nose foam of a respirator may become less elastic, which can reduce the fit and seal and make the respirator less effective in keeping outside air from leaking around the edges of the respirator; but this just means the respirator is less likely to perform at its full potential (3M, 2016), not that it is totally ineffective. While such dated products are inappropriate to use in a setting where respirators are mandated, such respirators will improve health welfare in settings where they are not typically used. Indeed, PPE products past expiration dates are distributed and used for prolonged hours in developed countries under situations of desperate shortage (e.g., BBC News, 2020; Martha, 2020), and recently the CDC (Centers for Disease Control and Prevention) issued guidance explicitly endorsing the use of certain respirators from the reserve past their labeled shelf life when responding to the COVID‐19 pandemic (CDC, 2020).
Motivated by the above, we assume that the quality/effectiveness degrades as the product ages but at a very slow rate (Saha & Galper, 2013); thus, the quality of donated products is no higher than that of fresh products but does not change during the decision horizon. Another example of donated product fitting our assumptions is where new models are more effective than older models. If the donation quality is higher than the equivalent available the local market, then donation will surely outperform the local supplies and the potential supplier effects discussed in this paper will be even more than if quality is equal, though this is not explicitly modeled. The quality of the product indicates its healthcare value, and a higher quality will lead to higher healthcare welfare (if everything else is held equal), as detailed in Equation (1) below.
Several regions are contained in the impoverished area, and they can get the product from two different sources. One source is to buy from the supplier in the local market. Yet, the amount to purchase is subject to a budget constraint, so it is possible these regions cannot afford enough product to fulfill their healthcare needs. An alternative source is from donation, which is expected to ease the need for the product and improve healthcare; this humanitarian purpose motivates donations to these regions.
However, donations could be taken advantage of by corrupt officials, possibly undermining the expected positive effects. Meanwhile, the local supplier could react to donations and change the affordability of the product. As corrupt officials and the strategic supplier change the dynamics associated with donation, it is necessary to investigate if donation can fulfill the humanitarian purpose as expected. Though belonging to the same area/country, each regional administration oversees its regional healthcare issues and is able to secure donations from independent sources; as a result, the type and the amount of donations received by each region are relatively independent (Shaw et al., 2015). Thus, we can look at a typical region as a donation recipient and analyze the impacts of donation. While the region could receive donations intermittently, we consider the time span for a large donation to be used in the region (if freely available); the length of the time span will depend on the donation size but is generally sufficient for the local supplier to react and adjust prices accordingly.
The model and notation
Over the considered time span, the region has a healthcare budget T, which can be used to procure the product considered in this work as well as other healthcare products. With budget T, and subject to the market price p set by the supplier, the region decides how much product to buy from the market, in order to maximize the healthcare welfare of the population served by the region. Due to the budget constraint and/or high market price, the region may not be able to afford all necessary healthcare products.
Denote the region's purchasing amount as





While the region decides the purchase quantity







On top of budget T, the region may receive an external donation of products, though the donated products could be dated, that is, if they come from the medical reserve. Let q denote the quality of dated donation, then



As the donation provides extra resources for the region and thus changes the dynamics of the local market, the supplier will react by adjusting market price p, which will be discussed later in corresponding scenarios. In this aspect we assume complete information, such that the supplier can anticipate the response functions of the region and the manager; this standard modeling practice allows us to derive the supplier's decision and obtain meaningful insights.





The base case
We first consider the base case when donation is not available, and take this as a benchmark. When there is no donation, the manager cannot conduct donation‐related corruption, and the region only needs to make one decision about 








The solution is straightforward: Whether and how much to buy depends on the region's budget level T, and the price p depends on the budget distribution, as per Proposition 1. A superscript b is used to indicate the results for the base case, and a superscript * indicates the optimal solution.
The market price The quantity of product purchased with budget T is The healthcare welfare with budget T is



It is not surprising that the amount of product purchased, 



Setting price 



MODEL ANALYSIS
In this section, we consider situations when donation products are provided. If the manager is corrupt (as is discussed in Section 4.2), donated products may be diverted into the black market and generate a charge for the region to receive them: In that case, the unit price of the donated product is denoted by w. Compared to the base case, the total amount obtained by the region is 
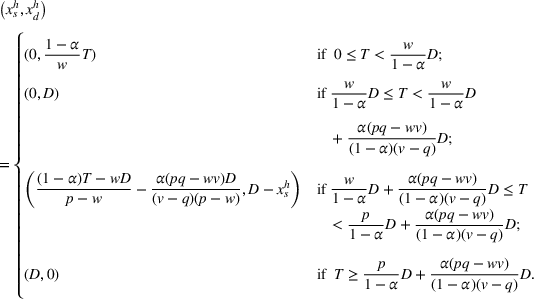
Before investigating the impact of donation, it is helpful to understand how the region should make purchasing decisions from a healthcare welfare perspective. Putting aside whether the manager is corrupt or not, to maximize the region's healthcare welfare is to solve the following problem:
Let The region's response functions depend on the market price p, donation price w, and budget T as follows: For For For 











With the region's response functions in Proposition 2, the supplier and the manager will respond by setting p and w, respectively, based on their objectives. Next we discuss two scenarios: when the manager is noncorrupt and when the manager is corrupt. These results will assume no constraint for the local supplier's capacity. Intuitively, one would expect having a supply constraint to both decrease the healthcare welfare and increase the pressure on the local industry. Therefore, the results give an upper bound for a region's welfare and a lower bound for the adverse effect on the local industry.
Noncorrupt manager
In this section, we consider how donation could impact the region by putting the possibility of corruption aside. While the region's purchasing decision follows Proposition 2, a noncorrupt manager will decide w so as to maximize the region's healthcare welfare 


Let 

When there are free and sufficient donations, the region will top up the total quantity of products to its demand D, since free donated products can always improve the healthcare welfare. Accordingly, the supplier's revenue function is different from when no donation is available, which motivates her to adjust the market price p. Specifically, in the case where the equilibrium price 



To derive the pricing decision for the supplier, we make a further assumption so that the model is more tractable. Assume that the budget level T follows a uniform distribution between 0 and If the manager is noncorrupt, then: the donation price if donation quality 







One important observation from Proposition 3 is that the supplier could be driven out of market by high‐quality donation products. This is due to the supplier's reaction to the donation: As shown in Proposition 4, the supplier lowers her price for fresh products as donation quality q increases, because donation breaks her monopoly power. A donation quality
The threshold If donation quality The supplier's price For a given budget T, the healthcare welfare function The welfare function Regarding the continuity of the welfare function For all For all 























If the supplier is out of the market, then regions intending to purchase from the supplier will have to turn to donation. As indicated by the expression of the product composition 

As such, the analysis indicates donation could be a double‐edged sword. While donation seemingly improves access to the product, it could drive out the local supplier and fail to improve healthcare welfare as expected. The results confirm the fear that free donations can hurt the local industry and make the recipient country too reliant on foreign aid (Moyo, 2009; Oxfam, 2005). Having donations drive out the local supplier could discourage the development of local production capacity and distribution network, and thus hinder the long‐term development of the local community. This is in line with the impression that many underdeveloped countries do not appear to make much headway, even when they receive massive amounts of donations and assistance. In line with the views Moyo outlines in her book (Moyo, 2009), we provide a model‐based analysis showing that free donations of a good quality may well be the reason for that.
Due to the adverse effect on the local supplier, the recipient region's healthcare welfare is not continuously increasing with donation quality, and donations of a very high quality do not necessarily improve welfare more than donations of a lower quality. This leads to our key observation for this section. Donations of an average quality, which is somewhat lower than the fresh quality but still reasonably good, could ease the adverse effect on the supplier but also significantly improve healthcare welfare.
This observation follows from two results in Proposition 4. (1) The threshold quality for the supplier to remain in the market, 













While the above is derived when the noncorrupt manager's objective coincides with the healthcare welfare function, some may argue that a noncorrupt manager should care about overall social welfare, including for the supplier who contributes to the local economy. The solution of donation quality being slightly lower than the fresh quality provides a viable and practical approach for a noncorrupt manager who cares about both the supplier's revenue and the healthcare welfare. The ideal level for donation quality could be determined by jointly considering the supplier's price and the impact on the healthcare welfare.
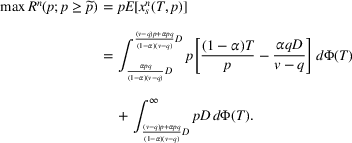
Corrupt manager
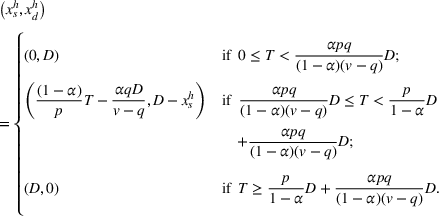
In this section, we consider the case when the manager is corrupt. The corrupt manager would divert the donation for sale on the black market (e.g., Kim et al., 2013; Shelley, 2014), and thus would seek to maximize his personal earnings by setting price w for the donation product. Since Proposition 2 shows the donation cannot be sold if If the manager is corrupt, let The threshold The supplier's price The donation price The donation price For a given budget T, the healthcare welfare function The welfare function 

























Proposition 5 shows that the supplier will leave the market if the donation quality q is high (i.e., 


The case when quality 

It appears surprising that when 

The decrease in donation price stops once donation quality q becomes higher than the threshold 



The above discussion indicates that the healthcare welfare achieved in the corrupt case becomes equal to that achieved in the base case when donation quality 







While these results are derived with the model setup so that the supplier and the corrupt manager compete for the product market, another possibility is that they collude, set a nonzero price that they both agree on, and then split the earnings in some fashion, particularly when Donations of a reasonable quality (below fresh but still of significant value) continue to be a viable solution when the manager is corrupt; mitigation measures are of use to ensure an appropriate quality level for donated products.
The corrupt manager will have a preference for donation quality since it affects his earnings. Not surprisingly, the corrupt manager will want donations of a high quality, that is, 








Since donation quality plays a key role in the studied effects, preventative mitigation measures are necessary to ensure the quality level is appropriate. To make the quality lower than the threshold quality, the donation products can be clearly labeled with the approaching or passed expiry dates and the projected effectiveness. Yet, due to the possibility that a corrupt manager waits for donation products to degrade, it is not clear whether any other regulatory actions taken by the donors, such as clearly labeling when the donation should be distributed by, can mitigate this form of corruption. In‐country studies would need to be carried out to examine whether this corruption effect is likely to occur in practice, which is clearly beyond the scope of this paper.
COMPARISONS AND DISCUSSIONS
In this section, we compare the results of the three cases: base case, noncorrupt manager, and corrupt manager, and summarize the results in Proposition EC.3 in the Supporting Information. We then discuss how the three cases compare with each other in terms of the supplier's price and the healthcare welfare, and summarize the results for low‐priority products, for example, PPE, as considered in this paper.
The market price
In this subsection, we discuss how the supplier's price compares across the three cases, as in Proposition EC.3, Item 1, in the Supporting Information, and in Figure 1. When donation is available, the supplier sets the market price lower than the base case, no matter whether the manager is corrupt or not, that is, 

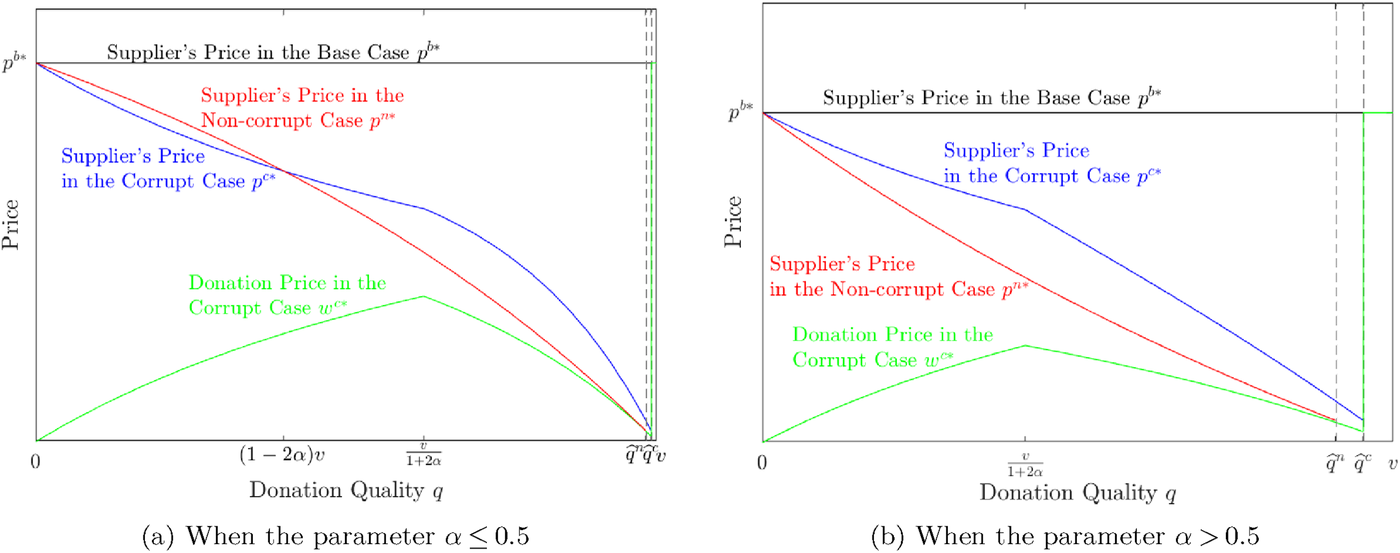
Comparison of prices in different scenarios
The comparison between the noncorrupt and the corrupt case is not intuitive as it depends on donation quality q. If 
Yet, if donation quality 


The healthcare welfare
The comparison of the healthcare welfare is illustrated in Figure 2. We first compare the noncorrupt case with the base case, which shows the same pattern in both Figure 2a,b. If the donation quality q is smaller than the threshold 


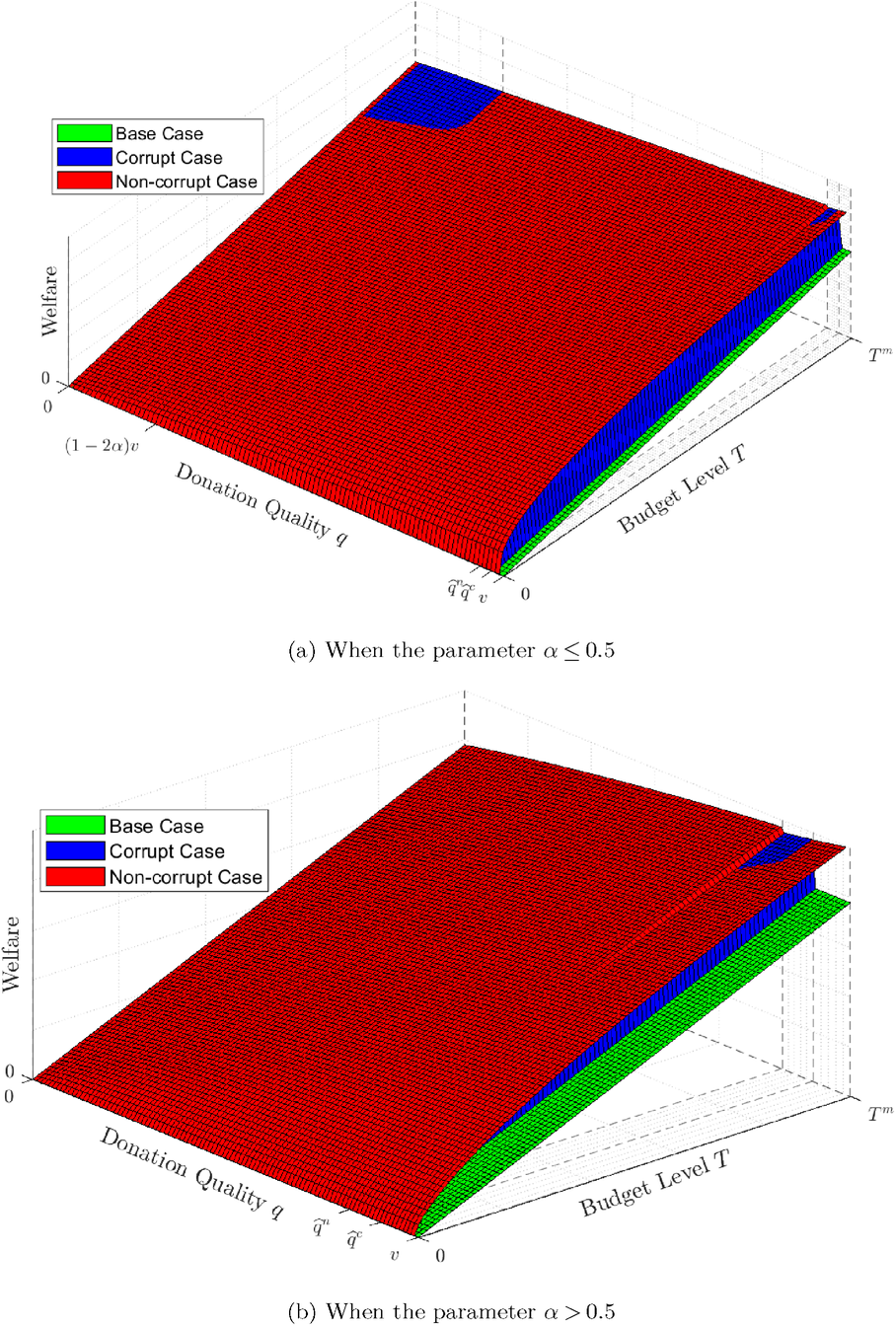
Comparison of welfare in different scenarios
It is interesting to observe from Proposition EC.3, Item 3, in the Supporting Information, that donation could make a high‐budget region's healthcare welfare lower than that in the base case when the supplier is driven out. This happens for regions with budget 



The comparison between the corrupt manager case and the base case also depends on the donation quality q. Similar to the noncorrupt manager case, donation under a corrupt manager improves healthcare welfare for all regions if donation quality Compared to the base case, donation improves a region's healthcare welfare if the supplier remains in the market; but could reduce healthcare welfare when donation quality is high enough that the supplier is driven out of the market, especially if the manager is corrupt.
When comparing the corrupt and noncorrupt cases, as in Proposition EC.3, Item 5, in the Supporting Information, it is not surprising that corruption is harmful, with healthcare welfare in the corrupt case being lower than that in the noncorrupt case for most regions. However, it is unexpected that some high‐budget regions can have a higher welfare in the corrupt case. This happens when the donation quality is in two ranges, but for different reasons. (1) If the donation quality 



While a high‐budget region's welfare can be higher in the corrupt case, the corrupt manager always makes a low‐budget region's welfare lower than in the noncorrupt case. This further confirms the harm caused by corruption: Diverting and selling donation products hurt poor regions that need help the most; the inequality of resources in the recipient country is deepened, as it enables rich regions to take advantage of poor regions. This is summarized in the next key observation. Compared to the noncorrupt manager, the corrupt manager reduces the healthcare welfare in most cases, but could cause an increase in the healthcare welfare for some high‐budget regions if donation quality q is within certain ranges.
Note that if the parameter α is small, then a high donation quality could satisfy the condition 
For low‐priority products
For typical low‐priority products where the parameter α is high, that is, 




Meanwhile, while Proposition EC.3, Item 3, in the Supporting Information, indicates the noncorrupt case could lead to lower welfare than the base case, this is less likely to happen for low‐priority products. This is because 


As such, for low‐priority products with the parameter α larger than 0.5, a pragmatic solution could be donations of a quality lower than the quality threshold in the noncorrupt case (and thus lower than the fresh quality). There are at least three benefits. The first is improved healthcare outcomes: The recipient's healthcare welfare is higher than when there is no donation, no matter whether the manager is corrupt or not. The second is alleviating the adverse effects on the local industry: The supplier can remain in the market no matter whether the manager is corrupt or not, and the corrupt manager does not make the adverse effect on the local supplier worse. The third benefit is constraining the negative consequences from corruption: Though the corrupt case leads to lower healthcare welfare than the noncorrupt case, all regions suffer, thus eliminating the chance that high‐budget regions take advantage of low‐budget regions when the manager is corrupt.
CONCLUSIONS AND IMPLEMENTATION
This paper models the impact of donating dated PPE‐type medical supplies from a developed country's medical reserve. We find that donation quality plays a key role in the healthcare welfare, the effect on the local supplier, and the impact of corruption. In particular, we find that the value of donation is not monotone in quality. The healthcare outcome does not always increase with the donation quality: Recipient regions could experience a sharp decrease in healthcare welfare if donation quality goes above certain threshold where the supplier is driven out of the market; and this happens no matter whether the manager is corrupt or not.
As such, our results suggest it helps to provide donations of a quality that is slightly lower than the quality threshold determined when the manager is noncorrupt (and thus lower than the fresh quality). Dated stocks that are proved to be stable with rigorous testing can and should be donated when they are close to or just past the labeled shelf life, while donations of dated stocks that are unstable or whose quality deteriorates quickly with time should be avoided. Low‐quality donation does not help with the healthcare welfare when the manager is noncorrupt, and can produce more harm than good when coupled with a corrupt manager by hurting both poor regions and the local supplier. However, donating products that are of a quality higher than the quality threshold or even higher than the quality of the local supplies, while possibly good for short‐term health outcomes when the manager is noncorrupt, is likely to be detrimental in the long run by driving the local supplier out of business. This argues for making donation available that are clearly stamped as dated, in order to indicate their quality is lower than the fresh.
Given these results we recommend that the WHO reconsiders its stance on such donations. In situations with no additional concerns about safety and ethics, they could ease their strict policy of totally abandoning dated donations, especially for products confirmed to be stable long after the initial shelf life. It would, of course, be prudent to run a pilot program with a single product first to see if there are any unanticipated adverse effects. Given that 84% of the DHS' reserve stock of hand sanitizer has previously been reported to have passed its expiry date (US DHS, 2014) and impoverished countries are experiencing shortages of the product and using diluted hand‐wash (Ider et al., 2012), this might be an obvious product to start with. Masks, needles, and syringes are other obvious candidates for donation.
As these donations come from the reserve, it would also help avoid expiration and dumping of the reserve stock. Two other ways to reduce expiration in the reserve are stock rotation (e.g., Zhou & Olsen, 2017) and shelf life extension (Courtney et al., 2009). However, such solutions are not always effective. Routinely rotating old reserve supply to regular daily operational use in the healthcare system (and then replacing with new stocks) may be uneconomic due to high handling costs and the possible remote location of the reserve. The SLEP in the United States, which extends the shelf life of the reserve products so they can be stored for a longer period, is a reactive way to delay expiration: Products still need to be replaced when they reach the extended shelf life. Instead, donating these stocks would use them effectively for the vast population in need of medical resources. When it comes to implementation, it is important to prevent dumping and making inappropriate donations, and the donor needs to discuss and seek consent from the recipient nation prior to making any dated donations.
While we have discussed the negative effects of donation on local suppliers, we have not specifically explored how to alleviate this side effect. As our results highlight the influence of donation quality, it is left for future research to explore other mechanisms to constrain the side effects and support local suppliers. Also, we have not discussed what lobbying medical supply companies might engage in if such a program was suggested. One possibility to avoid such lobbying would be to ask a large medical supplies company to actually run the program. They would undoubtedly be quite diligent in replacing dated supplies in the host country's reserve (since that is direct income), and therefore might be willing to donate the funds available to distribute the dated supplies. As mentioned earlier, they would be in the best position to ensure that the donations go to regions that are doing without the product (and therefore reduce issues of local supply replacement). Further, in the long run, this may improve demand from the impoverished country as using this product becomes the expected norm. Finally, eliminating local middlemen from the process would also reduce the opportunities for corruption.
While our models are relatively simple, we believe they capture the key trade‐offs faced in these scenarios. One limitation is that our model assumes full information. While this assumption is relative standard and allows us to derive meaningful results, future work considering partial information could enrich the story. We frame quality as age dependent, and it is left for future research to capture more dimensions of the quality variable. Our model considers a particular type of medical supplies, such as PPE and similar products, which are purchased and used by regions to fulfill their healthcare needs, and thus is not applicable to general donation items bought by end‐user consumers. As our model focuses on a typical region, considering other forms of corruption before donation reaches the region could make an interesting separate study in the future, as would the consideration of donation of products for emergency (rather than routine) healthcare needs.
Footnotes
ACKNOWLEDGMENTS
The authors are very grateful to the senior editor and the anonymous reviewers for their in‐depth reading and valuable comments, which helped us improve the quality of this contribution.
Open access publishing facilitated by The University of Auckland, as part of the Wiley ‐ The University of Auckland agreement via the Council of Australian University Librarians.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.