
Abstract
Summary
The aim of this study was to measure differences in occipital cortex excitability in migraineurs before and after administration of topiramate. We have previously demonstrated occipital cortex hyperexcitability in migraine using an objective technique of magnetic suppression of perceptual accuracy (MSPA). We hypothesized that a neuromodulator such as topiramate would demonstrate differences in MSPA in migraine compared with baseline. Ten migraine patients were recruited. To assess inhibitory function MSPA was measured using the following protocol. Timed transcranial magnetic stimulation were delivered at interstimulus intervals (ISI) varying from 40 to 190 ms (eight stimulations at each ISI) at 60% stimulus intensity. Subjects were asked to report letters projected at a fixed luminance on the screen. Visual suppression was calculated based on the number of errors the subjects made using automated analysis. This procedure was repeated at a minimum of two different dosages of topiramate when it was titrated for optimal migraine control. The interim dose was that at which an improvement in headache frequency was first observed, and the optimal dose was that at which the patient had a ≥ 50% reduction in headache frequency, or had reached a 100-mg dose. The mean [standard error (
Introduction
Migraine is a disabling primary headache disorder that includes episodic and chronic variants. The underlying mechanisms of chronic migraine are not well known. In the past, medication overuse was implicit in the popular term ‘transformed migraine’ (1); however, chronic migraine may occur without medication overuse. Outside the USA, where medication overuse is not as common, migraine transformation and chronic migraine are just as prevalent (2,3).
Routine clinical imaging for typical chronic headache is usually normal, with no evidence for structural abnormality in the presence of a normal neurological examination (4,5). White matter lesions have been reported to be present in migraineurs and were found to be more prevalent in migraine with aura and also associated with an increase in migraine frequency of more than one headache per month (6,7). Neurophysiological techniques appear to provide an excellent opportunity to study migraine since it is characterized by physiological rather than structural pathology. In studying standard episodic migraine, we (8) and others (9,10) have used a variety of transcranial magnetic stimulation (TMS) protocols to adduce converging evidence for functional cortical hyperexcitability in migraine. One technique, termed magnetic suppression of perceptual accuracy (MSPA), is an objective and reliable way of demonstrating excitability differences in the visual cortex between migraine patients and controls (11).
In the MSPA protocol, subjects see a series of three-letter trigrams flashed briefly on a computer screen. Each trigram is followed by a short interval of 40–190 ms, then a single magnetic pulse is delivered by a stimulation coil held against the occipital skull. In normal subjects, plots of MSPA data (henceforth MSPA profiles) exhibit a characteristic U-shaped function; accuracy of reporting the letters is good at short (40 ms) and long (190 ms) intervals, but no better than chance at medium (100 ms) intervals. The cellular basis for suppression of perception at the 100-ms interval is likely to be preferential activation of inhibitory neurons by a high-intensity TMS stimulus (12). In subjects with episodic migraine, MSPA profiles are characteristically shallower; it is harder to suppress perception at the medium intervals. We argue that this difference arises because of increased baseline cortical excitability, caused in turn by impaired intracortical inhibitory mechanisms in these patients (11). We have previously published a study where we had demonstrated MSPA profiles over a spectrum of migraine frequency, and subjects with chronic migraine had the least amount of inhibition based on their MSPA profiles (13).
According to a practice parameter published by the Quality Standards Subcommittee of the American Academy of Neurology, preventive treatment for migraine should be considered for individuals whose migraines substantially affect their lives and who have not responded to acute care or where migraines are frequent enough that treating them with acute medications risks development of drug-induced headache (14). Medications for the acute treatment of migraine are administered after an attack begins with a goal of eliminating migraine symptoms and reducing attack duration. Triptans, for example, target the trigeminal sensory system and their associated vasculature to reduce neurogenic inflammation and dilation of cranial vessels. On the other hand, medications for the preventive treatment of migraine are administered daily with a goal of reducing attack frequency and duration.
The mechanisms by which these preventive migraine medications exert their pharmacological effects remain unclear. Preventive medications may function through a variety of potential mechanisms that are believed to increase the threshold for migraine activation and/or stabilize a hyperexcitable nervous system. In the current study, we chose to examine the effects of topiramate; although the pharmacological mechanisms of action for topiramate's efficacy in migraine are not well understood, it has demonstrated efficacy for migraine prevention in several large, well-designed, controlled trials (15–17). The pharmacological actions that might provide its migraine-preventive efficacy have been postulated to include the blockade of voltage-gated sodium (Na+) channels, enhancement of γ-aminobutyric acid (GABA)-mediated neurotransmission, block of L-type calcium (Ca2+) channels, inhibition of carbonic anhydrase, activation of potassium (K+) currents and negative modulation of the excitatory neurotransmitter glutamate through kainate and α-amino-3-hydroxy-5-methyl-4-isoxazole propionic acid receptors (18).
TMS has been used to study the effect of migraine-preventive treatment on the threshold for inducing visual phosphenes (9, 19). However, the measurement of phosphenes in migraine is controversial. Therefore, in this study we used MSPA as a model to study the effect of topiramate on visual cortical inhibition in patients with chronic migraine.
Method
Subjects
The study was approved by Western Institution Review Board. Ten subjects were recruited from clinic patients of the Swedish Headache Clinic who were diagnosed with chronic migraine without medication overuse (CM) using the International Classification of Headache Disorders, 2nd edn (International Headache Society 2004) (20). Patients kept a prospective 30-day baseline paper diary that confirmed the diagnosis of migraine. All subjects had a normal neurological examination at the time of study. In all subjects the study was performed in the interictal period between acute migraine attacks and subjects must have been migraine attack-free for at least 72 h before and after participation. Subjects did not take migraine-preventive medications at least 4 weeks prior to the study and none had been exposed to topiramate prior to their involvement in the study. Analgesic and abortive medications were permitted during this 4-week period and during the course of the study. Subjects were asked to keep a paper diary throughout the study to monitor frequency of headache and response to topiramate. All subjects were given topiramate in an open-label fashion starting at 25 mg and titrating using additional doses of 25 mg at an interval of 2 weeks until an improvement in headache frequency was seen (the ‘interim dose’) and then titrating again until at least a 50% reduction in headache frequency was noted compared with prospective baseline or a dose of 100 mg was reached (the ‘optimum dose’). Headache frequency was determined by review of the patients' headache diaries. More than one headache could be reported within the same 24 h as long as each headache lasted at least 4 h and met criteria for migraine or was treated with a triptan or ergotamine. Patients were asked at follow-up visits whether they had any changes in symptoms and thus adverse events were captured in this manner. Subjects were seen at monthly intervals or sooner if they felt that they were having side-effects.
Apparatus
All eligible participants underwent occipital cortex stimulation using the Magstim 200 (The MagStim Company Ltd, Whitland, UK). A 90-mm circular coil was used that has 14 turns giving a peak magnetic field strength of 2 T and 530 V/m of peak electric field strength.
Procedure: MSPA
Stimuli
Visual target stimuli consisted of low-contrast letter trigrams (random letters presented in groups of three; see Fig. 1). The letters were presented in upper case Arial 48-point font. The presence of a frame helped to equalize any crowding effect on the letters and therefore also improve their legibility (21). The letters used were chosen from a subset of letters of approximately equal legibility (22). The letter trigrams, within the frame, subtended 1.21° × 0.55° of visual angle when viewed from a distance of 175 cm. There was no colour contrast between the trigrams and the background; they differed only on a grey scale. Visual stimuli were presented for short durations (30–250 ms) on a Gateway 2000 monitor and PC, running SuperLab (Cedrus Corp., Phoenix, AZ, USA) software. For each trigram presented, participants were asked to report verbally the letters in the correct order, which were then recorded by the investigator (participants were asked to say ‘blank’ or ‘don't know’ if they were unaware of a letter at a specific position).
Trigram: random letters presented in groups of three.
Phase 1—practice
Before magnetic stimulation began, participants completed a series of practice trials. The first three trigrams were presented for 250 ms to familiarize participants with the stimuli. Participants then completed 10 practice trials in which the trigrams were presented for 30 ms. If participants were unable to report the letters accurately by the end of this session, the practice trials were rerun to ensure that they were familiar with the procedures and were able to perceive the stimuli accurately.
Phase 2—time course of suppression
In Phase 2, participants were presented with 54 trials in which the letter trigrams were followed at a variable interval [the stimulus onset asynchrony (SOA)] by the magnetic pulse. Six SOAs were tested: 40, 70, 100, 130, 160 and 190 ms, with participants completing nine trials at each SOA. The order of presentation of trials was randomized for each participant. The intensity of the TMS pulse was set at 60% of maximum stimulator output for this phase of testing. Throughout, an interval of at least 5 s between successive magnetic pulses was observed. Participants responded verbally by trying to name the letters in the order in which they were presented.
Procedure
MSPA after pharmaceutical intervention. MSPA profiles were obtained when subjects were taking an interim dose of topiramate at least 28 days from the previous MSPA measurement. The MSPA procedure was repeated after subjects had been taking an optimal maintenance dose of topiramate for at least 28 days.
Statistical methods
Distributions of both visual suppression (percentage of letters reported correctly) and headache frequency were approximately normal. Thus, we calculated means and standard errors of these outcomes at each dose. We performed paired t-tests to compare headache frequencies and visual suppression across dose groups. We primarily report results for visual suppression at 100-ms intervals because relevance of surround inhibition has been documented at this ISI. We calculated Spearman correlations to quantify the relation between change in headache frequency and change in visual suppression at 100 ms from baseline to optimal dose. P < 0.05 was considered statistically significant.
Results
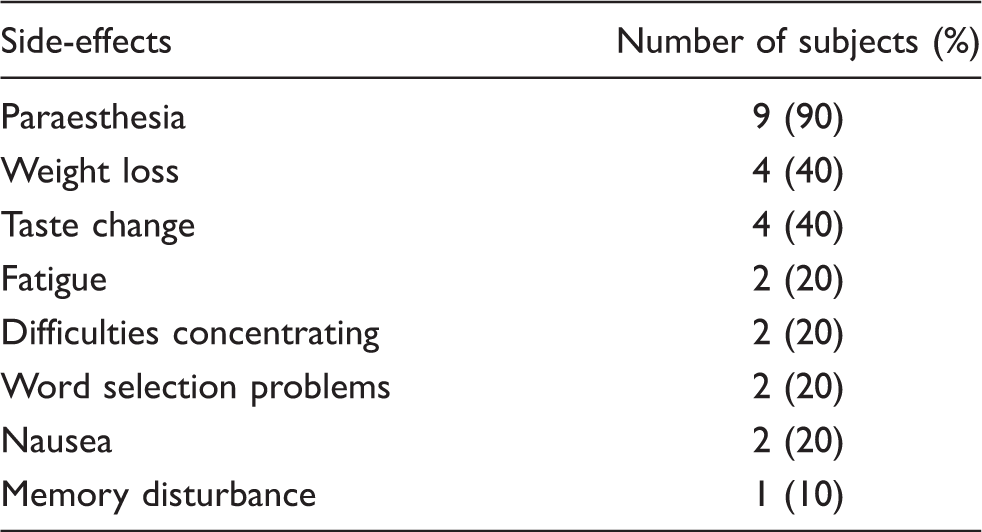
Topiramate daily dose was inversely related to headache frequency. At baseline, participants reported a mean ( Frequency of headache at baseline and after topiramate. Most common adverse effects experienced by patients
Topiramate daily dose was also inversely related to visual suppression scores. Figure 3 shows the mean ( Magnetic suppression of perceptual accuracy (MSPA) profiles by topiramate dose. SOA is stimulus onset asyncrony, the time in milliseconds between the appearance of the letter trigram and the delivery of the transcranial magnetic stimulation pulse. Standard errors are shown as bars.
There was not a strong relationship between decrease in headache frequency and decrease in visual suppression associated with topiramate dose (Fig. 4). From baseline to interim dose, the correlation between change in headache frequency and change in visual suppression was −0.43 (P = 0.21). The correlation between changes in headache frequency and visual suppression from baseline to optimal dose was −0.05 (P = 0.89).
Correlation figure. It is percent correct correlated to the number of headaches at baseline, interim dose and optimal dose, respectively.
Discussion
Previous research has shown a decrease in visual suppression in chronic migraine (13). In the current study we examined the effect of topiramate, a migraine prevention medication, on visual suppression in subjects with chronic migraine using MSPA, an objective validated technique. At baseline, subjects with chronic migraine had the pattern of deficient visual suppression seen in a previous study of chronic migraine (13) (see Fig. 2). Topiramate was seen to increase inhibition of the visual cortex as demonstrated by normalization of the baseline deficient visual suppression. We tested the MSPA at two different doses of topiramate (interim and optimal) and found that at an SOA of 100 ms there was a relationship between the dose and the degree of visual suppression. The greatest degree of visual suppression was seen at the optimal dose, and the interim dose was greater than baseline.
MSPA has been demonstrated in animal models to be a function of surround inhibition and thus GABA driven (10). In this study topiramate altered the curves of MSPA demonstrating increased inhibition at interim and optimal doses at 100 ms. This can therefore be interpreted as evidence for modulation of GABA-mediated neurotransmission by topiramate. In healthy volunteers, using double-pulse TMS, topiramate modulated intracortical inhibition, which is a function of GABAAergic neurotransmission (23).
Our results are similar to a study in which increased visual suppression was seen after treatment with valproate, another migraine prevention medication in patients with episodic migraine (19). In that study, the increase in phosphene thresholds was found after treatment in patients with migraine with aura, but not in patients with migraine without aura, and only in one subset of subjects stimulated with a figure 8 TMS coil, not in those stimulated with a circular coil. Despite the differences between their study and ours, both confirm that the neuromodulators topiramate and valproate alter the excitability of the visual cortex in migraine. The current study was in subjects with chronic migraine and used the more objective technique of MSPA.
We found no correlation between the degree of visual suppression and frequency of migraine. This is similar to a recent study using TMS of the motor cortex in migraine (24), and implies that topiramate enhances visual suppression and therefore increases the disturbed inhibitory tone in migraine independent of migraine frequency. Another theory is that topiramate modulates visual suppression and decreases migraine frequency but the time-lines may be different. Nevertheless, this study has substantiated the fact that the effect of topiramate is modulating cortical excitability, and the differences in visual suppression seen at optimal and mid-dose compared with baseline are not related to disease state alone.
Whereas visual suppression was observed only at the optimal dose of topiramate, clinical efficacy was seen at both the interim and optimal doses. Our data also confirm that topiramate's efficacy in migraine prevention may be observed at the first month of treatment (15–18), and with the titration method used it was generally well tolerated.
Interpretation of the results of this study is limited by the lack of a placebo arm. Future studies are planned to validate the technique and replicate results with inclusion of placebo treatment. This will help determine more specifically whether or not this is a specific drug effect or is related to disease state.