
Abstract
We present a 58-year-old man with neurological manifestations indicating increased intracranial pressure in association with hyperthyroidism. Hyperthyroidism due to a hyperfunctioning solitary thyroid nodule was the underlying cause, since all the symptoms disappeared after the treatment of hyperthyroidism. Our aim is to emphasize that hyperthyroidism should be suspected in a patient with progressive symptoms of increased intracranial pressure.
Hyperthyroidism is a disease that has many symptoms and can present in different ways. The typical manifestations of hyperthyroidism are consistent with a hypermetabolic state, including nervousness, weight loss, heat intolerance, palpitations, irritability and tremor (1). Also, individual case reports have suggested an infrequent association between hyperthyroidism and many neurological disorders such as depression, mania, schizophrenia, seizure, headache, sleep disturbances, myopathy, neuropathy and hydrocephalus or increased intracranial pressure (2–4). To our knowledge, this is the only case reported with progressive symptoms of increased intracranial pressure associated with hyperthyroidism due to a hyperfunctioning solitary thyroid nodule.
Case report
A 58-year-old man was admitted with complaints of severe headache, nausea, persistent vomiting and difficulty in walking lasting for 2 months. His disability had begun with headache that was not relieved by analgesics. Gradually, blurring of consciousness and difficulty in walking were added to his complaints. His legs had become so weak that they felt tired if he walked > 5 m and the patient had lately begun to stumble all the time while standing. His consciousness was unstable. He rarely felt awake, most of the time he was sleepy. He had hypertension, diabetes mellitus and had had a prostatectomy operation.
On initial examination his arterial blood pressure was 110/60 mmHg, respiratory rate was 24/min, pulse rate was 116/min, body temperature was 36°C. There was a 4 × 5 cm mass lesion at the right side of the anterior cervical region on physical examination. His chest and abdominal examination were normal, but there was a 2/6 systolic murmur on his cardiovascular system examination. Neurological examination showed that the patient was lethargic, had dysphasia and was generally in poor health. There was bilateral papilloedema (Fig. 1), proximally prominent four-sided muscle weakness (grade of muscle weakness in proximal parts of upper and lower extremities was 4/5, distal parts of upper and lower extremities 4–5/5), hypoactive deep tendon reflexes, bilateral Babinski's sign. The patient's gait was unsteady and it was impossible for him to put one step forward even with support. There was no stiffness of the neck or facial asymmetry. The pupils were symmetric and light reflexes were both positive. Even though the muscle strength was not so impaired, because of gait ataxia his ambulation was extremely affected.
Fundus photography of the patient's (a) right eye and (b) left eye (before treatment).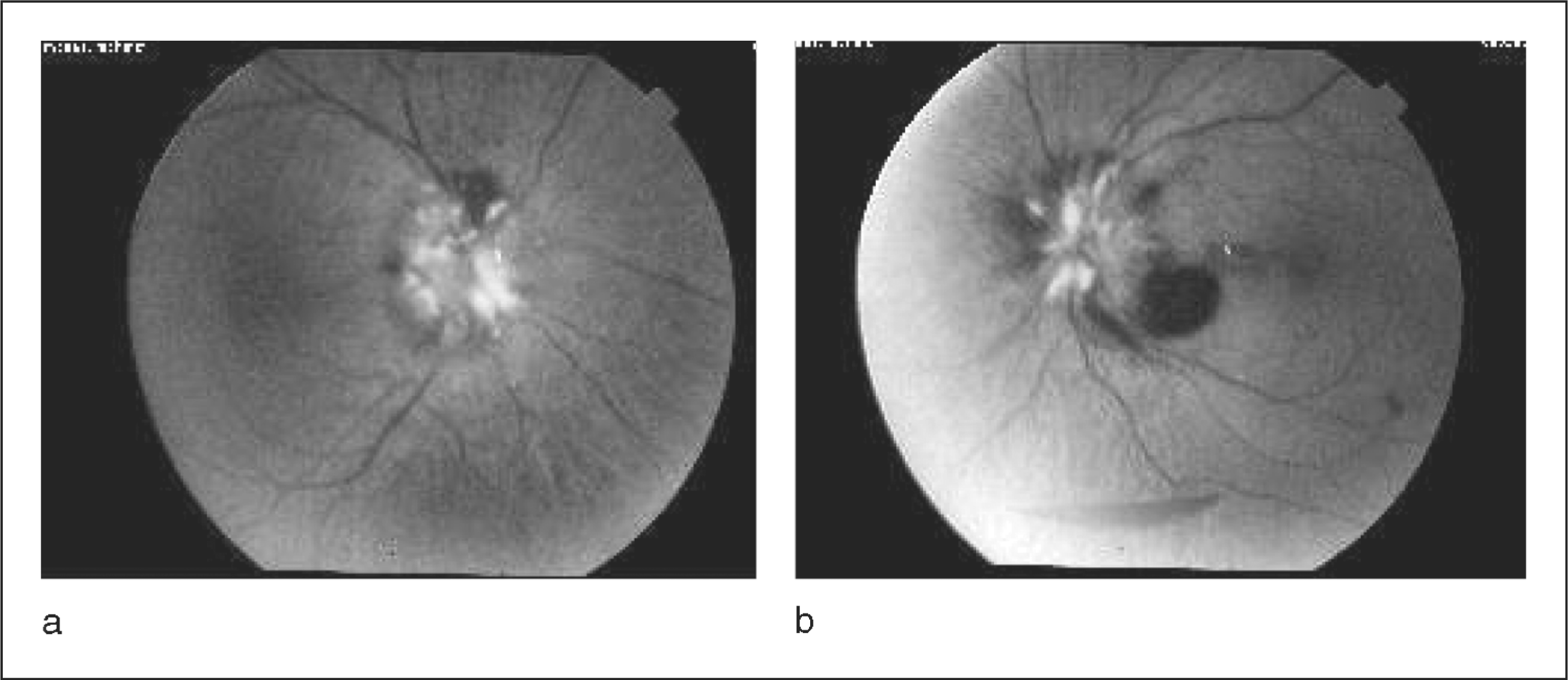
Lumber puncture findings showed opening pressure of 450 mm water [normal values (nv) 60–200 mm water] and closing pressure of 170 mm water; protein 51.3 mg/dl (nv15–45 mg/dl); glucose 58 mg/dl, no leucocytes or erythrocytes. Cerebrospinal fluid (CSF) IgG index was 0.70. Complete blood count was normal and biochemical parameters were normal except for slight elevation of blood urea nitrogen. Neither ethanol nor other drugs were detected in his blood. Thyroid function analysis revealed elevations in thyroxine [4.58 ng/dl (nv 0.8–1.9 ng/dl)] and triiodothyronine [7.71 pg/dl (nv 1.8–4.2 pg/dl)] levels with suppressed thyrotrophin [thyroid-stimulating hormone 0.068 µIU/ml (nv 0.4–5 µIU/ml)]. Thyroid-stimulating immunoglobulin [2.9 U/l (nv 0–9 U/l)], anti-thyroglobulin antibodies [< 20 IU/ml (nv 0–50 IU/ml)] and anti-thyroid peroxidase antibodies [< 10 IU/ml (nv 0–50 IU/ml)] were normal.
Electrocardiography and chest X-ray were normal. Brain magnetic resonance imaging (MRI) revealed lipoma at the vermis, non-specific gliotic lesions at the level of corono radiata and centrum semiovale and slightly dilation of ventricles. Thyroid ultrasonography revealed a multicystic nodule at the right lobe, deviation of trachea to the left side. Computed tomography of the thyroid gland revealed a nodule at the right lobe 3.5 × 5 × 5.5 cm in size. Hyperfunctioning solitary thyroid nodule was the underlying cause of the hyperthyroidism.
Increased intracranial pressure was sustained by high opening CSF pressure (450 mm of water) and clinical findings. Dexamethasone (24 mg/day) was started intravenously. After 2 days, his headache was relieved, the patient's general appearance was better and had improved day by day.
Propylthiouracil 300 mg/day and propranolol 40 mg/day were started orally. The patient recovered a short time after the thyroid hormone-lowering medication was added to the existing therapy. Dexamethasone therapy had been applied to the patient for 3 weeks.
The patient came for control after 45 days. He was conscious, very well oriented and cooperated. There was no papilloedema (Fig. 2) nor any other neurological abnormality. One year after discharge he had a subtotal thyroidectomy operation. During his follow-up in our outpatient clinic he has not experienced these complaints for 5 years and is well with thyroxine medication, although still with slightly enlarged ventricles.
Fundus photography of the patient's (a) right eye and (b) left eye (after treatment).
Discussion
In the patient discussed here, severe headache, persistent vomiting, papilloedema, gait disturbance, lethargy and high opening pressure in lumber puncture were compatible with decompensating increased intracranial pressure. It was thought appropriate to investigate possible causes of increased intracranial pressure. For that reason MRI of the head was done, which revealed slight dilation of ventricles. The most probable cause was idiopathic intracranial hypertension (IIH). IIH is a poorly understood syndrome that is a disease of CSF pressure regulation. This disease has also been associated with endocrine disorders such as Addison's disease, Cushing's disease, hypoparathyroidism, hypothyroidism and hyperthyroidism (5, 6), and it can be triggered by certain drugs (e.g. nalidixic acid, acute withdrawal of corticosteroid therapy) (7). When we evaluated the patient with the perspective of these facts, we decided to investigate hyperthyroidism, and discovered hyperthyroidism due to hyperfunctioning solitary thyroid nodule.
Even though chronic headache is a relatively well-known feature of hyperthyroidism (3), increased intracranial pressure due to hyperthyroidism is rare in the literature. Individual case reports have suggested an infrequent association between hyperthyroidism and IIH (4,8–10). A patient with hyperthyroidism mimicking clinical features of increased intracranial pressure, without evidence of hydrocephalus on neuroimaging and normal CSF pressure cured by serum thyroid hormone-lowering medication, has also been mentioned in a paper (11).
Even though the exact mechanism of how hyperthyroidism causes increased intracranial pressure is not known, cerebral blood flow increase due to hyperthyroidism has been shown. If the patient suffered subclinical disturbance of CSF circulation, hyperthyroidism might trigger some mechanisms that increase cerebral pressure, making the patient's disturbance clinical.
Most patients with hyperthyroidism are readily diagnosed clinically. Infrequent manifestations lead to a delay in diagnosis. Our case highlights the need to exclude hyperthyroidism in patients with increased intracranial pressure even though it is rare. Awareness of these atypical presentations will assist doctors in making a timely diagnosis.