
Abstract
Reversible cerebral vasoconstriction syndromes (RCVS) occur predominantly in middle-aged women. Only one child with RCVS has ever been reported. We report three boys (aged 10, 16 and 10 years) who had multiple thunderclap headaches, including one boy with bath-related attacks. None of them had secondary causes. All their magnetic resonance angiography demonstrated reversible cerebral vasoconstrictions of the major arteries with increased cerebral blood flow velocities on transcranial colour-coded sonography studies. Two of the three had hypertensive surges during headache attacks. None of the three boys had seizure, stroke or other neurological deficits. However, a left occipital subcortical lesion of unknown nature was noted in one boy. The efficacy of calcium channel blockers was variable in these three boys. This report suggests that, although rare, RCVS should be considered in paediatric patients if they present with a history of multiple attacks of thunderclap headache.
Introduction
Reversible cerebral vasoconstriction syndromes (RCVS) are defined as a group of disorders characterized by reversible vasoconstriction of the cerebral arteries as well as recurrent acute and severe headaches resolving spontaneously within 3 months (1,2). It can lead to various complications, such as cortical subarachnoid haemorrhage (SAH), intracerebral haemorrhage, seizures, posterior reversible encephalopathy syndromes and ischaemic infarctions (1–3). Calcium channel blockers (CCBs) were frequently used in patients with RCVS; however, no double-blind placebo-controlled studies have been published (3–5).
There is a female preponderance for this syndrome, especially in middle-aged women (1,3). Bathing is a common trigger of thunderclap headache and in one study all the reported patients with bath-related thunderclap headache were women (6). RCVS has rarely been described in children; only one Canadian boy aged 13 years has been reported (7). In this report, we presented three paediatric patients with RCVS, one of whom had headache attacks triggered by bathing.
Case report
Patient 1
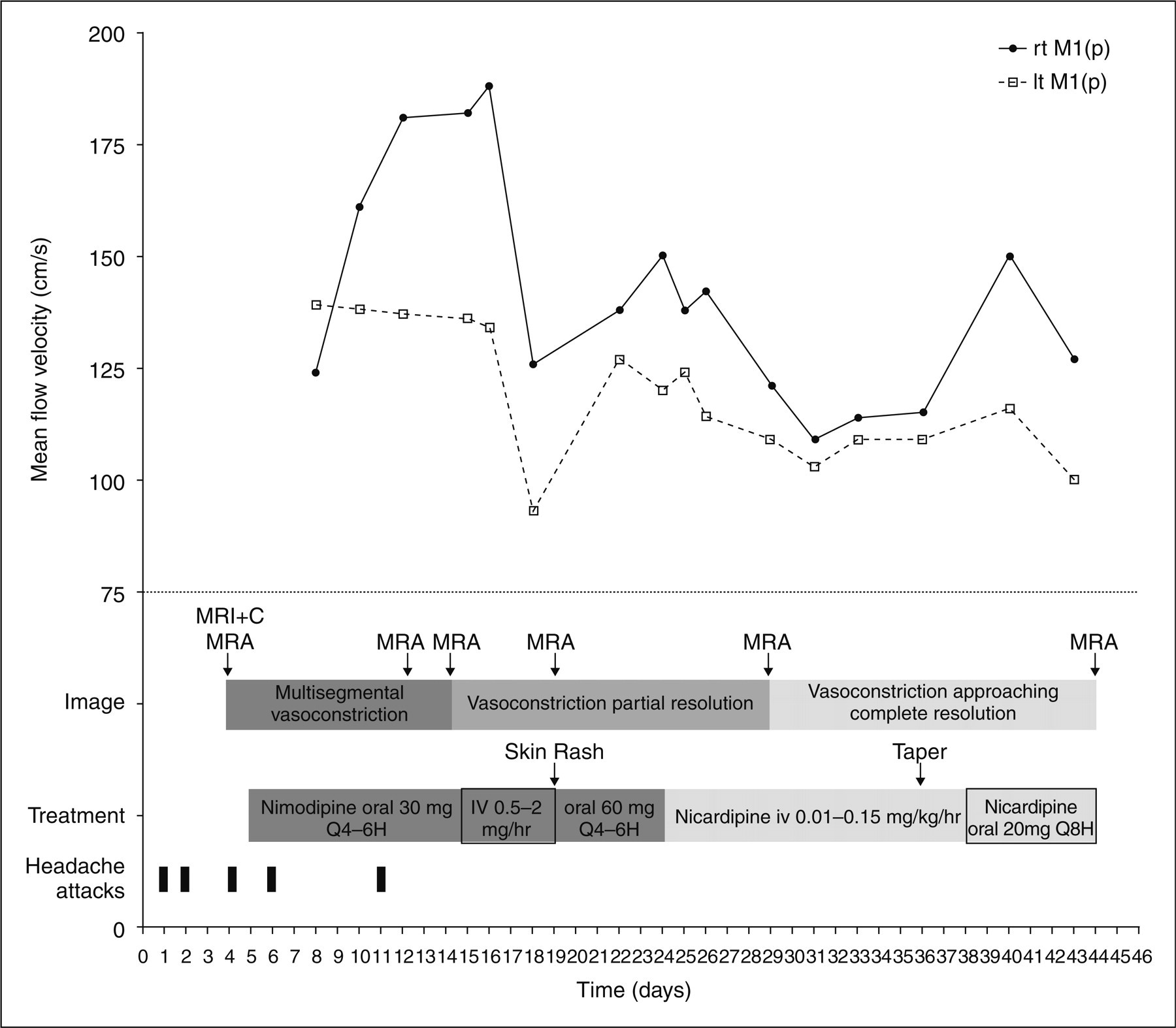
A 10-year-old boy [body mass index (BMI) 23 kg/m2], who denied a prior headache history, was admitted to our hospital after three severe thunderclap headaches, i.e. reaching maximum intensity in seconds, in the past week. His mother, aunts and cousins all had a history of migraine. He had been on H1-antihistamine (levocetirizine 5 mg per day) and corticosteroid-containing nasal spray (fluticasone propionate 1 puff twice a day) for allergic rhinitis until his first headache occurred. He was awoken around 03.00 h during sleep by a sudden-onset, non-throbbing, intense headache (day 1) with a verbal numeric pain scale of 10/10 intensity. He described the headache as ‘like a stick hitting the back of my head continuously’. He did not have nausea, photophobia or phonophobia, but had vomited once. His blood pressure was 130/92 mmHg (average blood pressure 105/65 mmHg) on arrival at the emergency department (ED) of our hospital. The headache lasted for 1.5 h with a peak intensity lasting for 15 min, and was gradually relieved after treatment with oral diclofenac (25 mg). The second and third headaches abruptly occurred over the same region when he poured hot water over his chest during a shower on day 2 and day 4 with duration of 30 and 5 min and severity 8/10 and 5/10, respectively. He denied having had baseline headaches between these severe attacks. His neck was supple. Neurological examination was unremarkable. Laboratory findings, including blood cell counts and screening blood chemistries, were normal. Brain magnetic resonance angiography (MRA) (Fig. 1a) on day 4 showed multiple, short-segmental, mild to moderate narrowing in bilateral middle cerebral arteries (MCA) and posterior cerebral arteries (PCA). Transcranial colour-coded sonography (TCCS) (day 8) demonstrated markedly increased flow velocity with turbulence over bilateral intracranial internal carotid arteries, anterior cerebral arteries (ACA), MCA (mean blood flow velocity: right MCA 124 cm/s, left MCA 139 cm/s) and PCA. The patient was given 30 mg nimodipine orally starting on day 5 every 4–6 h, and only two mild headaches occurred transiently when he was doing his homework on day 6 and day 11. He changed his bathing habit to a scrubbing bath from day 5 to day 8, and resumed taking showers on day 9 without recurrence of bath-related headache. Nevertheless, follow-up MRA on day 12 showed no improvement of the vasoconstrictions, and the blood flow velocities on TCCS became even higher (mean blood flow velocity: right MCA 181 cm/s, left MCA 137 cm/s). In addition, a small hyperintense lesion was noted on fluid-attenuated inversion recovery (FLAIR) MR images in the white matter of the left occipital region of the brain (Fig. 2a) without obvious change in apparent diffusion coefficient values. FLAIR magnetic resonance imaging (MRI) also revealed hyperintensities in the sulci of bilateral occipital and posterior temporal regions of the brain (Fig. 2a), but these sulcal hyperintensities were not hypointense on gradient-echo (T2*) MRI. We then switched from oral to intravenous (i.v.) nimodipine treatment on day 15, titrating from 0.5 to 2 mg/h. No hypotension was noted during i.v. nimodipine treatment. Multisegmental vasoconstrictions on MRA improved on day 14 and the blood flow velocities on TCCS improved on day 18 (mean blood flow velocity: right MCA 126 cm/s, left MCA 93 cm/s). However, because of an allergic skin rash, i.v. nimodipine was terminated on day 19 and the oral form was resumed using 60 mg every 4–6 h. However, TCCS on day 22 again showed deterioration. The treatment profile was adjusted to i.v. nicardipine (day 24), titrating slowly from 0.01 to 0.15 mg kg–1 h–1. Transient dizziness was complained of once during titration. Improvement of blood flow velocity was shown on follow-up TCCS. On day 36, i.v. nicardipine was tapered and replaced by oral form nicardipine 20 mg three times per day. He was discharged on day 44 with his medication continued. Follow-up MRA at discharge showed much improvement (Fig. 1b). He had been headache free for > 3 months. Brain MRI performed 4 months after disease onset showed resolution of the FLAIR sulcal hyperintensities, but the left occipital hyperintense lesion persisted. The clinical course, treatment, image findings and TCCS studies are summarized in Fig. 3.
(a) Three-dimensional (3D) time-of-flight (TOF) magnetic resonance angiography (MRA) obtained on day 4 after the onset of symptoms shows multiple short-segmental narrowing over bilateral middle cerebral arteries (arrows). (b) 3D TOF MRA obtained on day 44 shows resolution of vasoconstrictions (arrows). (a) Fluid-attenuated inversion recovery (FLAIR) magnetic resonance image obtained on day 12 shows a small hyperintense lesion in left occipital white matter (arrow) and hyperintensities in the sucli of bilateral posterior temporal and occipital regions of the brain (arrowheads). (b) Magnified view of the hyperintensities over left posterior temporal sulci (arrowhead). Summary of the clinical course, treatment, neuroimaging findings and transcranial colour-coded sonography studies of patient 1 (rt M1(p), proximal M1 segment of right middle cerebral artery; lt M1(p), proximal M1 segment of left middle cerebral artery).

Patient 2
Transcranial colour-coded sonography results of our three male paediatric patients during ictal stage and remission in comparison with healthy boys

VMCA denotes the mean blood flow velocities of bilateral proximal middle cerebral arteries (MCA).
Patient 3
A 10-year-old boy (BMI 18.6 kg/m2) was admitted due to episodic thunderclap headaches for 1 month. He had allergic rhinitis without medical treatment. He suffered from a sudden-onset, severe, non-throbbing headache over bilateral frontal and temporal areas after being hit by a soccer ball over his right cheek (day 1). He complained of phonophobia but no nausea, vomiting or photophobia. The headache gradually improved after usage of paracetamol, but a mild to moderate baseline headache persisted. He was admitted to one hospital after another severe attack on day 3 and was treated with pain killers and glycerol (days 4–9) under the suspicion of increased intracranial pressure. However, thunderclap headaches with a similar pattern lasting from 10 min to 3 h recurred intermittently after discharge. Sneezing was the only trigger he noticed. He was then admitted to our hospital and MRA on day 21 showed multisegmental narrowing over bilateral MCAs and PCAs. The TCCS (day 22) demonstrated high flow velocities with turbulence over bilateral carotid siphon, MCA and PCA. Nimodipine 15 mg was given orally every 4 h starting on day 24, but was stopped on day 26 because his headache did not improve. A spinal tap on day 26 showed a high opening pressure (235 mmH2O), but the CSF studies, including cell counts, levels of glucose and protein, as well as cultures were negative. The MR venography on the same day showed patent cerebral venous sinuses. No papilloedema was found. Oral form nimodipine treatment was restarted with the same dosage on day 28, and headaches have not recurred since day 29. Follow-up MRA on day 31 showed improvement of vasospasm, but the blood flow velocities on TCCS did not improve as well. Throughout the whole course of illness, no hypertension was detected. He has remained headache-free for 2 years ever since, but increased blood flow velocities were still noted on TCCS at the 2-year follow-up (Table 1).
Discussion
All three boys' headache profiles were similar to those described in adults with RCVS, i.e. multiple thunderclap headaches (1,2). The associated symptoms such as nausea, vomiting, photophobia and phonophobia were variable. The duration of recurrent thunderclap headaches ranged from 9 to 30 days with three to 16 attacks. All of them had a history of allergic rhinitis, but none had migraine or developmental problems. Two patients had hypertensive episodes during headache attacks, with systolic blood pressure greater than 95 percentile of children of the same age (8). Fortunately, none of them developed neurological deficits or seizures.
RCVS can be idiopathic or related to various secondary causes (1,3). It mainly affects middle-aged women (1), whereas in men it is characterized by a younger age of onset, multiple-substance exposure and more frequent cannabis use (3). Many precipitating factors, such as vasoactive substances including cannabis, selective serotonin reuptake inhibitors, over-the-counter nasal decongestants containing pseudoephedrine, and postpartum status, have been identified to be associated with RCVS in adults (3). Sexual intercourse, defecation, emotional change, physical exertion, urination with effort, coughing, sneezing, bathing, and sudden head movement are commonly reported triggers of RCVS (1,3). In four reported paediatric cases to date (three in the current study and one in a previous study (7)), no precipitating factors demonstrated in adults were noted, but all our cases had triggers of their thunderclap headaches.
In all three patients, the initial MRA (range 4–21 days after the first headache onset) demonstrated multiple segmental arterial constriction. No SAH or arterial dissection was noted. MRA improvement was demonstrated within 10 days to 2 months at follow-up. Notably, a small hyperintensity over the left occipital white matter which persisted over 4 months was noted on the MR FLAIR image of patient 1 without any clinical correlates. A longer follow-up is warranted to delineate the occipital lesion. Additionally, we speculated that the hyperintensities over his cortical sulci were possibly hyperintense vessels (9,10) contributed by very low flow velocities of distal branches of MCA and PCA or their leptomeningeal anastomotic collateral vessels. Though not the gold standard technique, findings of gradient-echo (T2*) MRI made cortical SAH less likely (11). The possibility of proteins, cells or artefacts should also be considered, but current imaging techniques did not allow any conclusions to be drawn (12). CSF study was not performed because no other indications including clinical symptoms or signs were sufficient.
All the initial TCCS showed remarkably increased blood flow velocities over the major cerebral arteries in our paediatric cases (Table 1) compared with healthy children (13). In our previous study of RCVS in an adult group, patients with a mean flow velocity of MCA > 120 cm/s had a greater risk of ischaemic complications than those without (14). Even though all three patients in this study did well clinically without neurological deficits, we empirically administered CCBs to prevent ischaemic complications because their cerebral blood flow velocities were high. However, we could not explain the lack of correlation between MRA and TCCS in patient 1 during treatment.
The most common adverse event of nimodipine or nicardipine is hypotension (15). Other less frequent adverse effects include headache, oedema, nausea, diarrhoea, hepatitis, gastrointestinal haemorrhage, rash, thrombocytopenia and hyponatraemia (15). All of our patients received CCBs, and the thunderclap headaches were eliminated or remarkably reduced in two of the three. None of them developed hypotensive events during treatment. However, the variable duration, dose, route, the potential of spontaneous recovery and development of occipital hyperintensity lesion despite treatment in one patient make it difficult to draw any conclusion on the efficacy of CCBs in treatment of our patients.
In conclusion, although rare, RCVS should be considered in paediatric patients with multiple thunderclap headache attacks. Further studies of such cases in this age group are mandatory to delineate the treatment strategy and disease outcome.
Footnotes
Acknowledgment
This study was supported in part by a grant from the National Science Council (97-2628-B-010-007-MY3).