
Abstract
The aim of this study was to asses the clinical features, pattern of healthcare and drug utilization of migraine patients attending 10 Italian headache centres (HC). Migraine is underdiagnosed and undertreated everywhere throughout the world, despite its considerable burden. Migraine sufferers often deal with their problem alone using self-prescribing drugs, whereas triptans are used by a small proportion of patients. All patients attending for the first time 10 Italian HCs over a 3-month period were screened for migraine. Migraine patients underwent a structured direct interview about previous migraine diagnosis, comorbidity, headache treatments and their side-effects and healthcare utilization for migraine. Patient satisfaction with their usual therapy for the migraine attack was evaluated with the Migraine-Assessment of Current Therapy (ACT) questionnaire. The quality of life of migraine patients was assessed by mean of Short Form (SF)-12 and Migraine-Specific Quality of life (MSQ) version 2.1 questionnaires. Of the 2675 patients who attended HCs for the first time during the study period, 71% received a diagnosis of migraine and the first 953 subjects completed the study out of 1025 patients enrolled. Only 26.8% of migraine patients had a previous diagnosis of migraine; 62.4% of them visited their general practitioner (GP) in the last year, 38.2% saw a specialist for headache, 23% attended an Emergency Department and 4.5% were admitted to hospital for migraine; 82.8% of patients used non-specific drugs for migraine attacks, whereas 17.2% used triptans and only 4.8% used a preventive migraine medication. Triptans were used by 46.4% of patients with a previous diagnosis of migraine. About 80% of migraine patients took over-the-counter medications. The Migraine-ACT revealed that 60% of patients needed a change in their treatment of migraine attacks, 85% of whom took non-specific drugs. Both the MSQ version 2.1 and the SF-12 questionnaires indicated a poor quality of life of most patients. Migraine represents the prevalent headache diagnosis in Italian HCs. Migraine is still underdiagnosed in Italy and migraine patients receive a suboptimal medical approach in our country, despite the healthcare utilization of migraine subjects being noteworthy. A cooperative network involving GPs, neurologists and headache specialists is strongly desirable in order to improve long-term migraine management in Italy.
Introduction
Migraine affects 11% of the general population worldwide (1), with a prevalence of 18% in women and 9% in men in Italy (2). It is estimated that 6363 000 Italians suffer from current migraine. Migraine leads to severe disability with negative effects on quality of life and an obvious impact on direct and indirect social costs and work productivity. Data from general population surveys showed that approximately 90% of migraineurs have moderate or severe pain, three-quarters have a reduced ability to function during headache attacks, and one-third require bed rest during their attacks (3–6). The negative effects on ability to perform daily activities and on the sense of well-being may be more relevant in those patients attending Headache Centres (HC) (7).
According to the World Health Organization, disability and functioning are relevant parameters for monitoring the health of nations, and migraine is in the top 20 causes of disability worldwide. The burden of migraine on individuals and on society as a whole is even greater if we consider that migraine has a peak of prevalence at the age of an individual's greatest productivity (8). Moreover, epidemiological studies have indicated that about 5% of women and 2% of men suffer from chronic headache forms, i.e. headache for > 180 days (9, 10). Chronicity is very often the result of transformation of an episodic migraine not properly treated to a daily headache that leads to overuse of symptomatic drugs, which in turn can be the cause of resistance to preventive treatment and of serious side-effects (7, 11). Overall, these epidemiological data strongly suggest that migraine should have the best treatment possible at disease onset. However, migraine is underdiagnosed and undertreated everywhere throughout the world (1, 12). One possible explanation is that migraine sufferers often deal with their problem alone using self-prescribing drugs. In the USA, for example, even if a significant improvement was recorded in comparison with data obtained in 1989 and 1999 (12, 13), only 56.2% of migraineurs reported that they received a diagnosis of migraine in 2007 (14). Moreover, the same study showed that 49% of migraine patients in USA treat acute attacks of migraine with over-the-counter (OTC) medication; 20% usually use prescribed medications and 29% use both (14).
Unrecognized migraine remains an important health problem also in Europe. FRAMIG 2000, a population-based study of management of migraine in France, showed that 80% of migraineurs were aware that they had migraine, but only 18% had medical follow-up for migraine, and that migraine-preventive medication was used by only 6% of patients (15). In the UK, 86% of migraine patients had consulted a doctor for their headache at least once in their life, but only 67% received a diagnosis of migraine (16). Important disability was found in a high proportion of those who never consulted, never received a correct medical diagnosis, and treated only with OTC medications (16). Thus, it seems that migraine does not receive early diagnosis and the appropriate treatment, regardless of the type of health system organization. In Italy, despite the fact that the National Health Service provides all citizens with a free visit to a general practitioner (GP) and specific antimigraine drugs such as triptans, the situation is no different from other countries: the Migraine Epidemiology—Therapy and Economics: an Outcome Research Study, conducted in Italy during the first trimester of 1996, showed that migraine prevalence in a large sample of the population presenting to their GPs for any reason was 11.6%, although < 3% of them sought medical advice specifically for headache. Among the drugs used for acute attacks, most patients in this study took non-steroidal anti-inflammatory drugs (NSAIDs) (89.1%), 21.9% took no medication whatsoever, whereas triptans were reserved for a small proportion of attacks (2.4%) (17). A more recent study, conducted nearly 10 years later, confirmed that triptan medications are used by only 6% of migraine patients in Italy (18). These are probably the reasons why migraine patients seek an answer to their problems by crowding dedicated HCs with qualified staff specifically trained in the diagnosis and treatment of headache, but few data exist about the outcome of patients referred to HCs. Only one Italian survey has shown an increment of the proportion of migraine patients taking prescription drugs (from 49.4 to 81.3%), triptans (from 9.1 to 31.8%) and prophylactic drugs (from 16.8 to 58.2%) after HC access (19).
Furthermore, based on the selection criteria of the US evidence-based guidelines (20), around 38–50% of patients with migraine should be considered candidates for preventive therapy (21, 22), which may reduce resource utilization (23) and improve ability to function and quality of life of patients (24). Despite these possible benefits, only 12.4% of migraineurs use a daily preventive migraine medication in USA (21). It must be noted also that adequate acute treatment can minimize the negative effects on patients as well as on society, and published evidence indicates that the use of triptans may in fact have significant effects on the quality of life of migraineurs and on migraine-related costs (25–29).
The aim of this study was to evaluate the clinical features, pattern of healthcare and drugs utilization of migraine patients attending 10 HCs in Italy. We conducted an observational, multicentre, cross-sectional study.
Patients and methods
All patients consecutively attending for the first time 10 Italian HCs over a 3-month period (September 2006 to March 2007) were screened for migraine by a headache specialist. The HCs were selected in order to represent all the geographical area of the country (six in General Hospitals, four in Teaching Hospitals). The diagnosis of migraine was made according to the second edition of the International Classification of Headache Disorders criteria (30). Informed consent for sensitive data treatment was obtained from all migraineurs recruited in the study. Data from each patient were collected in a Case Reports Form that included demographic data, previous migraine diagnoses, current diagnoses, comorbidity, headache treatments and their side-effects; healthcare utilization in the last year was assessed if the patient was aware of suffering from migraine. Pharmacological therapies were classified as non-specific (NSAIDs, paracetamol, antiemetics, opiates) or specific for migraine (triptans), as prescribed by a doctor or self-prescribed and as off-label or not. Patient satisfaction with their usual therapy for the migraine attack was evaluated with the Migraine-Assessment of Current Therapy (ACT) questionnaire (31). Migraine-ACT is a specific tool that was developed and tested to identify migraine patients who require a change in their current acute medication treatment (32). Four clinically relevant domains of the migraine experience have been included in the questionnaire (consistency of response, global assessment of relief, headache impact and emotional response), each corresponding to a single question with a no/yes answer. Migraine-ACT has an intuitive scoring: an increasing number of ‘no’ answers indicates increasing treatment needs. When the total score is ≤ 2 patients need a change in their treatment of the migraine attack (31). Health-related quality of life was assessed using both a generic and a disease-specific tool. Patients were asked to complete the Short Form (SF)-12 (33) and the Migraine-Specific Quality of life (MSQ version 2.1) (34), two well-known tools that have been extensively used in headache research. The scores in all three dimensions of MSQ (Role Restrictive, Role Preventive, Emotional Functioning) and the scores of the two summary scales of the SF-12 (Physical Component and Mental Component) were calculated.
A descriptive statistical analysis was performed. For qualitative data the χ2 test was used.
Results
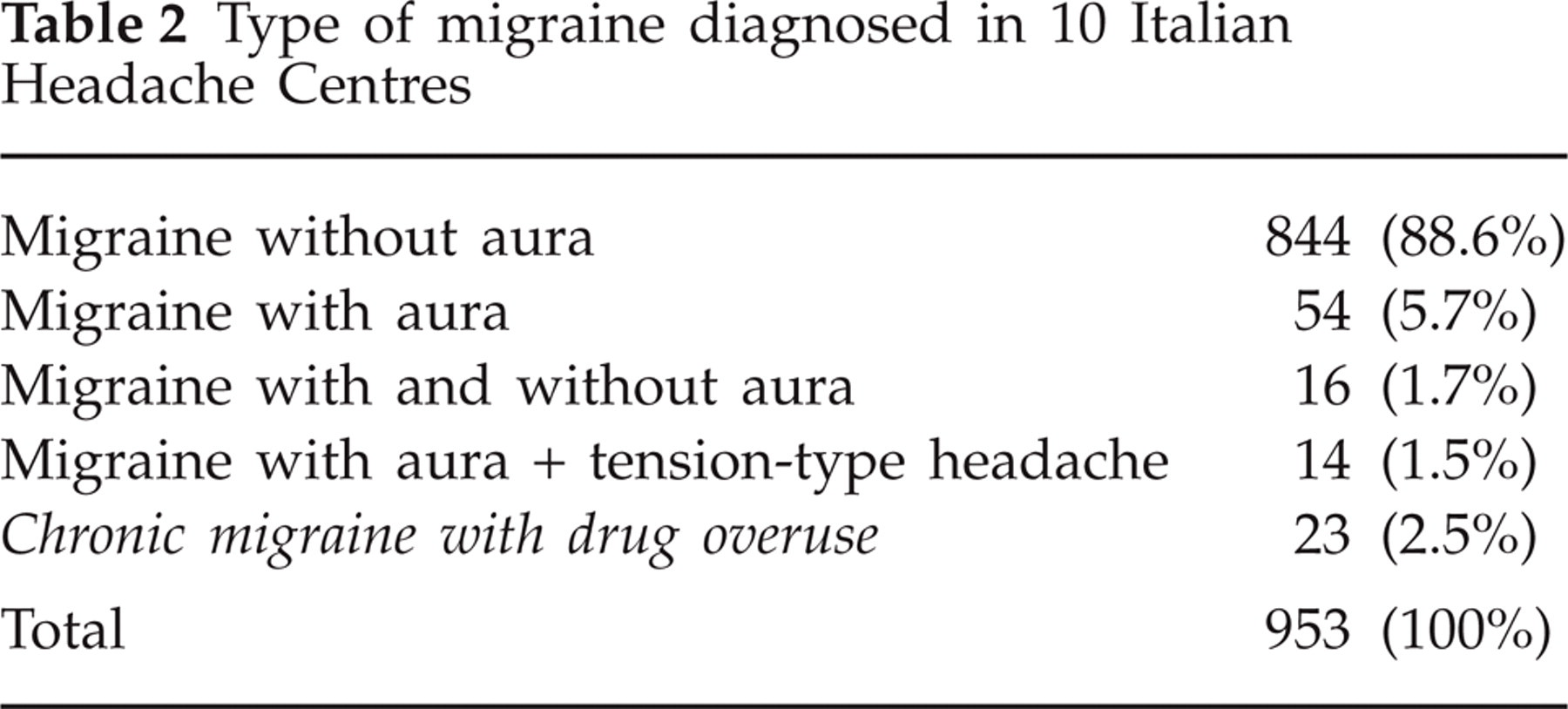
A total of 5158 patients attended HCs during the study period; 2675 were visiting for the first time. Of those visiting a HC for the first time, 71% (n = 1910, 438 M, 1472 F) received a diagnosis of migraine, and the first 1025 consecutive subjects (54% of the migraine group) were enrolled in the survey. Nine hundred and fifty-three patients completed the study (775 F, 178 M) and 72 patients (8%) were excluded from the analysis because of missing data. However per-protocol results did not differ from those of the intention-to-treat population. Demographic characteristics are summarized in Table 1. Migraine without aura was the more frequent diagnosis (88.6%), followed by migraine with aura (5.7%) and by patients who received multiple diagnoses (Table 2).
Demographic characteristics and habits of 953 migraine patients enrolled
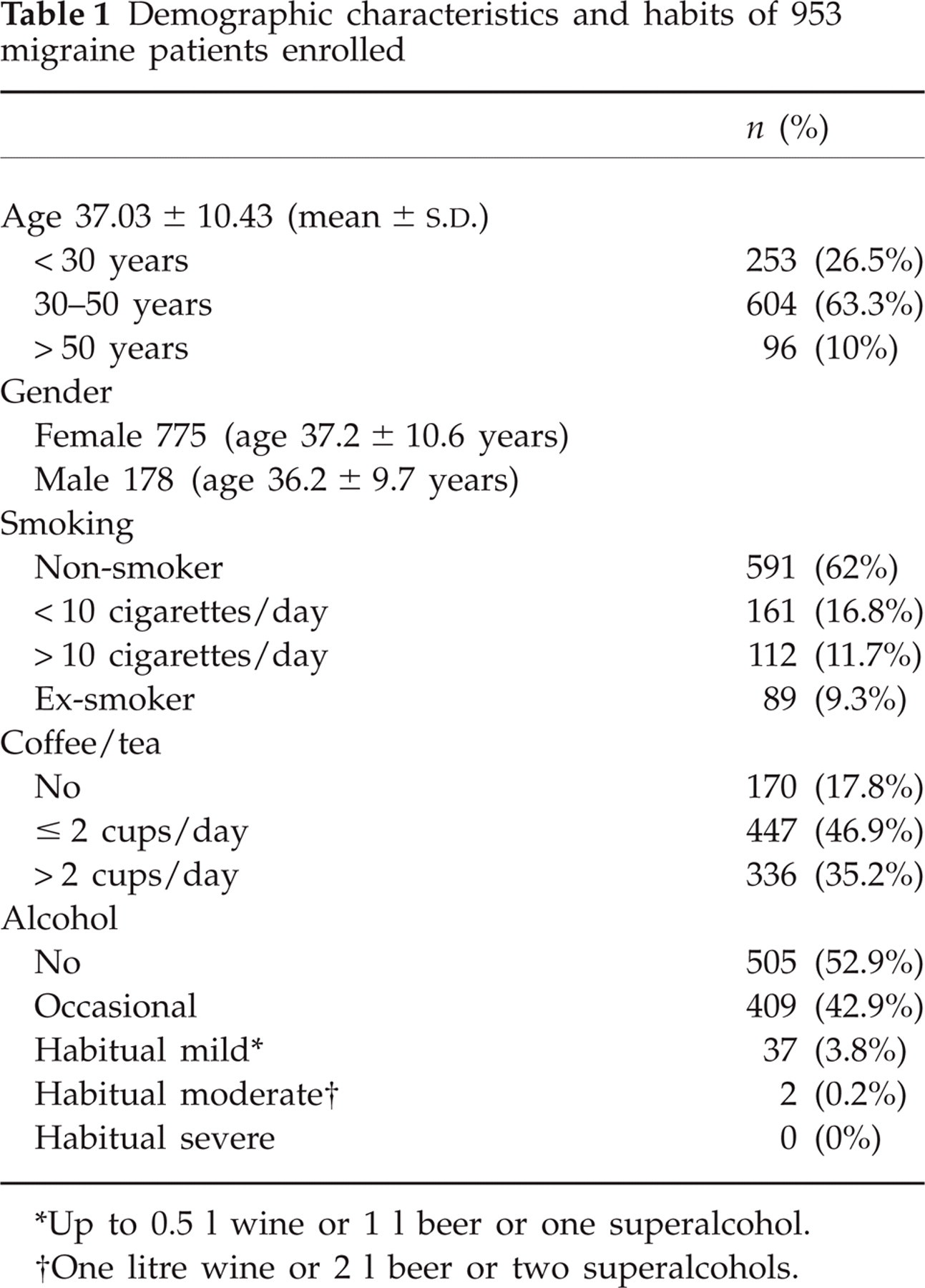
Up to 0.5 l wine or 1 l beer or one superalcohol.
One litre wine or 2 l beer or two superalcohols.
Type of migraine diagnosed in 10 Italian Headache Centres
Only 26.8% (256) of migraine patients had a previous diagnosis of migraine and they reported a duration of the disease of 7.9 ± 8.3 years (mean and
The healthcare utilization for migraine in the last year of this cohort is noteworthy: 160 subjects (62.4%) visited their GP; 98 patients (38.2%) saw a specialist for headache; 62 (23%) attended an Emergency Department (ED) for migraine and 12 (4.5%) were admitted to hospital (Table 3). Migraineurs attended an ED or were admitted to hospital for headache regardless of whether they had previously consulted a doctor or not (P = 0.8044).
Healthcare utilization for migraine in the last year by 256 patients with a previous diagnosis of migraine

Of patients who completed the study, 335 (35.1%) reported disorders other than migraine in their history and 250 (26.2%) referred current medical problems other than headache (Table 4).
Previous and current health problems in 953 migraine patients

The great majority of patients (909; 95.3%) used drugs for migraine headache: most of them (82.8%) used non-specific drugs for acute attacks of migraine, 17.2% used triptans to treat their attacks and only 4.8% used a preventive migraine medication. Drugs used for acute and preventive treatment of migraine by our sample of migraine patients are specified in Table 5.
Drugs for acute and preventive treatment of migraine consumed by 953 migraine patients before headache centre access

The total number of drugs was greater than the number of patients because some patients consumed more than one type of drug.
Off-label.
Not recommended for migraine in current guidelines.
SSRI, selective serotonin reuptake inhibitor.
Of 953 patients, 300 (31.5%) used more than one type of non-specific medication for acute migraine attacks, and 130 (13.65%) more than one triptan.
Of the 256 patients with a previous diagnosis of migraine, 203 (79.3%) used non-specific drugs to treat their attacks, 119 (46.4%) used triptans and 35 (13.6%) were on prophylaxis.
Among patients without a previous diagnosis of migraine, 98 of 697 (14%) used triptans as acute treatment and 11 (1.5%) were on prophylaxis.
Six hundred and eleven patients (67.2%) used self medication only (OTCs), 186 (20.4%) used drugs prescribed by their GP and 112 used both (12.3%).
Among patients who used preventive medications for migraine, 14 (26.4%) were taking drugs not recommended by evidence-based guidelines and 22 (41.5%) used off-label medications (Table 5). Of the total of 953 patients, 84 (8.8%) reported adverse events due to migraine medications: 54.3% of them reported gastrointestinal disturbance, 17.2% asthenia, 15.1% central nervous system problems, 8.6% cardiovascular symptoms, 2.5% weight gain and 2% cutaneous rush.
The great majority (93.6%) of subjects with gastrointestinal problems were on treatment with non-specific medications. Among patients that used triptans, four (1.8%) referred chest tightness and one tachycardia. Only one hypertensive patient reported an increase of hypertension with NSAID use, but none with triptan. Dizziness, asthenia and somnolence were more reported by triptans users than by NSAID users.
Migraine-ACT questionnaire revealed that many patients were not satisfied with the current acute treatment, with ‘no’ answers to the four questions ranging from 45.5 to 54.6%. The reasons for incomplete satisfactions are shown in Table 6.
Migraine-ACT questionnaire results

Furthermore, 574 (60%) out of 953 patients needed a change in their treatment for the migraine attack (Migraine-ACT score ≤ 2), 488 (85.0%) of whom took non-specific drugs and 117 (20.3%) triptans.
The MSQ version 2.1 scores showed how migraine affects health-related quality of life in three dimensions: Role Restrictive score, which measures the degree to which performance of normal activities is limited by migraine, was 50.8 ± 20.1 (mean and
The SF-12 questionnaire had low mean scores both for physical component (43.9 ± 8.4, mean and
Discussion
Our study has reported the clinical features, pattern of healthcare and drug utilization of 953 migraine patients attending for the first time 10 HCs in Italy and representing 71% of all subjects referred to HCs.
Two main results are evident from our survey: migraine is still underdiagnosed in Italy, and migraine patients receive a suboptimal medical approach in our country.
In fact, only 27% of migraineurs attending for the first time an Italian HC were aware of suffering from migraine, whereas the remaining 73% had never received a correct diagnosis. On the other hand, the vast majority of our migraine patients (in both the undiagnosed and the diagnosed groups) took non-specific drugs, and one-third of them more than one type.
These findings appear to be more relevant (and surprising) if we consider the following aspects: (i) the Italian Health System provides a free GP visit or a neurological consultation with little charge; (ii) healthcare utilization before the HC visit in our sample had been noteworthy; in fact, > 60% of patients had visited their GP for migraine several times in the last year, almost 40% of patients had consulted a neurologist, 23% of subjects went to an ED and 4.5% were admitted to hospital for their headaches; (iii) a substantial proportion of migraineurs were moderately or severely disabled, as suggested by average scores obtained using disease-specific as well as generic health-related quality of life questionnaires, confirming US and UK data (14, 23); (iv) illness duration without a diagnosis was rather long, with a mean value of 8 years in the studied cohort; and (v) more than half of our patients were not satisfied with their current acute treatment.
The above-reported data lead to other considerations. Even if we can not exclude that our patients may have failed to remember receiving a diagnosis, it is more likely that they did not receive such a diagnosis, or they did not seek medical care, or their GP underestimated the importance of diagnosing and treating migraine. The fact that resource utilization was high also in patients who had received a diagnosis of migraine suggests that migraine is poorly treated in Italy, even if correctly diagnosed. The important healthcare utilization of our migraine subjects, confirming previous US data of a progressive increment of the number of visits for the treatment of migraine from 1990 to 1998 (35), represents a substantial part of the direct costs for migraine in Italy, assessed to be €313 per patient per year in 1996 (17).
Migraine treatment proved suboptimal in Italy: the Migraine-ACT questionnaire revealed that 60% of migraineurs included in the study were not satisfied with their acute migraine treatment, particularly if they usually used OTC drugs (85.0%). Moreover, only 17.2% of patients attending an HC for the first time were treated with triptans that are well known to have better efficacy than non-specific painkillers (36). More than 80% of subjects were treated with non-specific acute medications, in both the undiagnosed and diagnosed groups. Although the proportion of patients receiving triptans was higher (more than double) than that reported in previous surveys on the general population or on patients followed by GPs (17–19), this was substantially low.
However, our data show that improving the rate of diagnosis of migraine may be the main route to follow in order to achieve better acute migraine management. In fact, the percentage of patients using triptans for migraine rises to 46.4% in the group who had a migraine diagnosis, and 43.5% of them were satisfied with current acute therapy by the Migraine-ACT questionnaire (score ≥ 3).
The majority of migraineurs (67%) treated their acute attacks with OTC medications exclusively, and only 20% used prescribed medications only. Thus, self medication seems to be another barrier to optimal migraine care also in Italy, a country where the use of OTCs in other fields is not so widespread (37, 38).
Furthermore, in our study only 4.8% of patients were treated with a preventive drug before attending the HC. This percentage is quite low considering that it has been demonstrated that > 30% of migraineurs are good candidates for preventive therapy (16). Moreover, among patients who used preventive medications, many were using drugs not recommended by current evidence-based guidelines, and > 40% were taking off-label medications. Off-label drug prescriptions are a controversial issue in migraine management, as some drugs used in headache treatment are not recommended for this use in Italy, although their efficacy and safety have been demonstrated in clinical trials (e.g. valproate). In our country physicians may prescribe off-label treatment on their own responsibility and only after receiving the patient's informed consent (39). Administration of drugs without evidence of efficacy for migraine prophylaxis strongly suggests the need for educational programmes on evidence-based medicine in Italy (40), but it might also be the expression of a selection of severe cases of non-responders to usual treatments. The complex comorbidity of our patients, which appears to be important for a population with a mean age of 37 years, might be an expression of this selection.
Only 9% of our patients reported adverse events due to migraine medication: more than half reported gastrointestinal disturbances due to non-specific medications, whereas one-third referred asthenia or other minor central nervous system problems, especially in the triptan group. Only few subjects reported cardiovascular symptoms: among patients that used triptans, four referred chest tightness and one tachycardia; only one high blood pressure sufferer reported an increase of hypertension in the NSAID group, but none with triptans. Gain of weight was complained of in a few patients who took prophylaxis. Data on adverse events have shown that OTCs might be dangerous drugs (38), whereas treatment with triptans appears to be well tolerated if correctly prescribed.
Surprisingly, psychiatric comorbidity in our sample was very low compared with other published Italian surveys (41). This result might be explained by the fact that psychiatric problems need a good patient–physician relationship, a relationship that requires more time than that scheduled for a standard first visit, and the use of standardized tools/interview to obtain a correct diagnosis.
A limitation of our study was that it was performed in secondary and tertiary headache clinics, thus the investigated sample may not represent the whole spectrum of migraine patients present in the general population. Moreover, the observed population probably represents a selection of severe or complicated cases that do not respond to specific medications as do pure migraine patients. A prospective survey of new migraine-only patients from the general population would be very useful to highlight the real pattern of healthcare and drug utilization due to migraine.
In conclusion, our survey has confirmed that, although migraine causes significant disability, deterioration in quality of life, and substantial economic consequences, most people with migraine do not receive a correct diagnosis and are likely to be inadequately treated before attending an HC in Italy. It is important to note that inappropriate treatment leads to poor patient satisfaction, which in turn may result in lapses from care and may enhance the risk of self-medication and, eventually, headache chronification and medication overuse.
These results strongly indicate that physicians, GPs above all, must be encouraged to make a diagnosis of migraine, and to treat patients accordingly. A consequent improvement in the use of effective treatment of migraine attacks with specific drugs such as triptans, and of appropriate prophylaxis when is needed, is strongly desirable in Italy in order to improve the quality of life of patients and to reduce direct and indirect costs of migraine (29, 42). In our opinion, increased communication and coordination between primary care and ED physicians, neurologists and headache specialists could improve long-term migraine management in Italy.
Acknowledgements
The authors thank all the participants involved in this study: Dr M. Abbate, Dr G. Coloprisco, Dr F. De Cesaris, Dr S. De Filippis, Dr S. Gangemi, Dr D. Grimaldi, Dr U. Pietrini, Dr P. Mantegazza, Professor F. Monaco, Dr G. Pierangeli, Dr N. Rocca, Dr M. Viana and Dr D. Bettucci. (Diego Bettucci, MD, director of the Headache Centre and distinguished physician at the Neurological Department of Novara Hospital, esteemed member of the SISC (Italian Society for the Study of Headaches), died suddenly on 26 May 2008. He was 56 years old.) This study was sponsored by Merck & Co. Inc.