
Abstract
A series of 22 patients was consecutively diagnosed with hypnic headache (HH) from June 2007 to June 2008 in two headache specialty centres participating in the French Observatory of Migraine and Headaches. Patients and headache characteristics were compared with the 2004 International Classification of Headache Disorders, 2nd edn (ICHD-II) criteria for HH and published series of HH patients. One-third of HH patients reported migraine-like headaches (pulsating/unilateral/stabbing) and > 20% were aged < 50 years at symptom onset. Of note, HH patients displayed typical motor activities during the headache (getting up, eating/drinking especially a cup of coffee, reading/ watching television) that differentiate HH from migraine and suggest relationships between HH and trigeminal autonomic cephalalgias. The functional and emotional impact of HH appears low and similar to that of migraine in patients consulting in primary care practice. Improvements in ICHD-II criteria are suggested, especially to introduce the typical motor behaviour acted out by HH patients.
Introduction
In 1988, Raskin reported for the first time six closely similar cases of aged patients encountered during the years 1977–1986 who reported short-lasting diffuse headaches occurring exclusively during sleep, at the same time usually every night, and associated with nausea but no autonomic symptoms. He named this syndrome ‘hypnic headache’ (HH) (1). Since then, individual new cases or short series of cases of HH have been reported in the literature (2–6). HH is a rare syndrome: in 1998 its frequency was estimated at 0.07% on the basis of one HH diagnosis for every 1400 headaches evaluated at the Mayo Clinic annually, and at 0.09% of all headache patients seen from 1998 to 2002 in an Italian specialty headache centre (2, 4). Thus far, approximately 90 patients with HH have been reported in the literature (6, 7). The first suggested diagnostic criteria for HH were defined by Goadsby and Lipton in 1997 (8). However, it was not until 2004 that the International Classification of Headache Disorders, 2nd edn (ICHD-II) adopted HH as a primary headache disorder (code 4.5) (9).
We report here a series of 22 consecutive patients diagnosed with HH over 5 years in two tertiary care headache centres in the South of France. These cases were identified amongst patients participating in the French ‘Observatory of Migraine and Headaches’ (OMH), which is a national clinical research network on headache and facial pain set up in 2002 by the French Headache Society (10). Characteristics of these HH patients are analysed below in relation to the ICHD-II diagnostic criteria and compared with those of previously published series of HH patients.
Methods
The national OMH network involves 16 tertiary care headache clinics and one specialized headache emergency department and overall covers approximately two-thirds of the French metropolitan territory. The setting up of the OMH database was declared to and approved by the French Commission on Data Processing and Liberties. During the period June 2007 to June 2008, neurologists from two OMH centres (in Marseilles and Nice) contacted known HH patients for a face-to-face interview during which patients were administered a standardized 28-item questionnaire. New consulting patients diagnosed with HH were also interviewed. All patients participating in the study were interviewed during a consultation by the same physician in each centre. HH diagnosis was first established based on clinical symptoms and discussed afterwards according to the ICHD-II criteria (code 4.5).
The study questionnaire captured information on patients' demographics, age at time of first consultation at a tertiary care centre, existence of a diagnosis of HH before entering the OMH network, age at time of HH onset, headache characteristics (headache quality, location and variability, intensity, time of occurrence and duration, usual frequency in a day and a month and variability, episodic or chronic evolution), associated signs and symptoms [nausea/vomiting, photo-/phonophobia, autonomic symptoms, patients' purposefully getting up during the attacks (to eat or drink, read or watch television, stroll, …), agitated behaviour, intense thirst, urination, alimentary behaviour, thymic disorders], existence of other types of headache [migraine, tension-type headache (TTH) …], comorbidities (sleep disorders, hypertension …), personal or family history of headaches, acute treatment(s) of attacks, use of hypnotics, acute and/or prophylactic treatments of headaches, and possible medication overuse. The presence of abnormalities on neurological examination and neuroradiological investigations was looked for. No polysomnographic recording was performed. Blood pressure was measured.
The functional and emotional impact of headaches was assessed using French versions of the Headache Impact Test (HIT)-6 and Hospital Anxiety and Depression (HAD) scales, respectively (11–14). Substantial or severe functional impact was considered when the HIT-6 score was > 55. Emotional impact was considered when HAD score for anxiety (HAD-A) or depression (HAD-D) was ≥ 8.
Results are analysed only descriptively. Quantitative variables are described by the mean and standard deviation (
Results
Patients
Patients' characteristics are displayed in Table 1. Of the 22 patients diagnosed with HH over 5 years and seen in consultation from June 2007 to June 2008 in the two participating OMH centres, 54.5% were women. Median patient age at the time of consulting was 60.5 years, with one patient aged < 50 years (45 years). Median age at the time of disease onset was 54 years, with five patients (22.7%) aged < 50 years at that time. Median time interval between symptom onset and diagnosis was 7 years. Only one patient (male, presenting with daily severe symptoms) had been diagnosed with HH before consulting in the OMH headache speciality centre.
Main characteristics and headache profile of the 22 hypnic headache patients of our series

HAD, Hospital Anxiety and Depression; HIT, Headache Impact Test.
Thirteen HH patients (59.1%) gave a personal history of other types of headache, either migraine without aura (MoA) or TTH. Ten HH patients (45.5%) gave a family history of probable MoA. Both personal and family histories of MoA were reported by nine patients (40.9%), only a personal history of MoA by three patients, and only a family history of MoA by one patient, who complained of concurrent undiagnosed headaches (Table 1).
Hypnic headache profile
All patients reported only nocturnal headache attacks. Time of pain occurrence was 00.00–02.00 h for six patients, 02.00–04.00 h for 13 and 04.00–06.00 h for three. Two patients had additional nocturnal attacks at 05.00–06.00 h. None reported any variability in the time of occurrence of headaches or any influence of the time of retiring to bed. Median duration of attacks was 60 min (range 0.25–3 h). Mean frequency of attacks was 23 days per month (range 5–30) (Table 1) and described as variable by 12 patients (variability concerned the occurrence of a second nocturnal attack for one patient). The attacks were episodic for 10 patients (at least initially for two). No evolution in periods was reported.
Sixteen HH patients described their headaches as diffuse, of whom three reported preferential headache location on one side (right side, n = 2; left side, n = 1) and one on either side alternately. Six patients reported headaches as exclusively unilateral (right side, n = 3; left side, n = 3). Pain topography was only frontal in three patients, only temporal in two, only orbital (at least initially) in four, fronto-temporal in one, orbito-cervical in two, occipital initially in one, occipito-parietal in one, located in vertex in one patient, and extending to the whole left side in one patient. Only three patients reported variability in pain location.
Headache intensity was rated as severe by seven patients, moderate by 13 and mild by two. Headache quality was described as pressing by 13 patients, pulsating (throbbing) by seven, ‘like a stake’ by one, and ‘like a vice’ by one patient.
Associated signs and symptoms
Nausea was constantly reported by two patients and on some occasions by three, but none reported vomiting. Photophobia was reported by three patients and phonophobia by none. Moderate autonomic symptoms (tearing, rhinorrhoea/nasal congestion) were reported by three patients (Table 1). One patient reported systematic nightmares before waking up with HH.
During the headaches, HH patients acted out a specific stereotyped motor behaviour characterized by a feeling of being compelled to get up (all patients) and undertake purposeful activities, i.e. reading or watching television, eating or having a drink (mainly a coffee), or urinating (note: no male patient suffered from prostatic hypertrophy and more than half of patients were women) (Table 1). No HH patient exhibited a state of agitation, however. This behaviour during the attacks differed typically from that of migraine sufferers (who tend to stay in bed) or cluster headache (CH) patients (who often wander stamping their feet in marked agitation). One HH patient reported a feeling of intense thirst during the headaches.
HH diagnosis according to ICHD-II criteria
Eleven patients (50%) fulfilled all five ICHD-II criteria for HH (code 4.5). Criterion A (dull headache) was missing in eight patients, criterion C (at least two HH typical characteristics) in two, and criterion D (no autonomic symptoms, no more than one of nausea, photophobia or phonophobia) in four, whereas all patients met criteria B (headache developing during sleep and awakening the patient) and E (not attributed to another disorder) (Fig. 1).
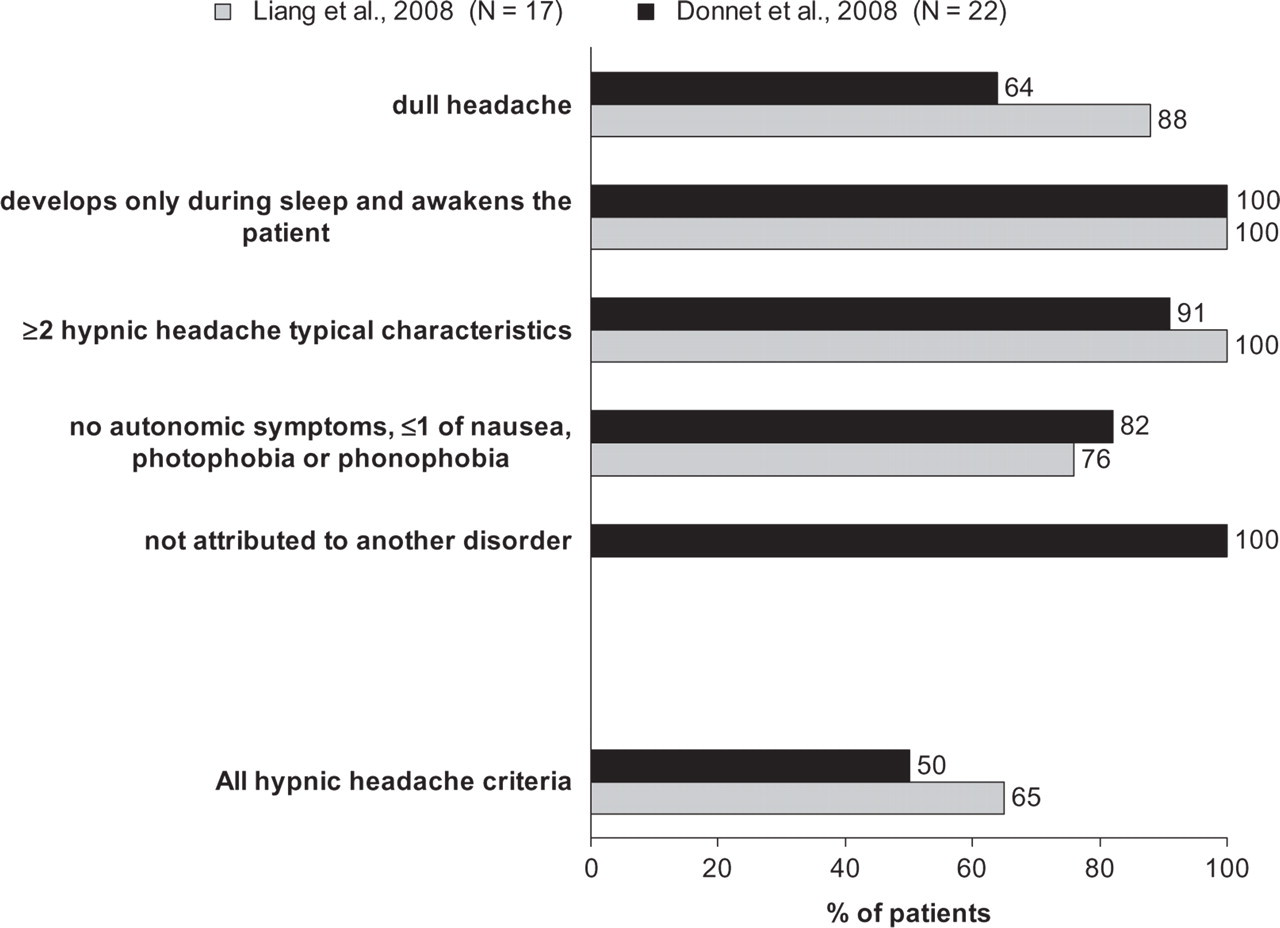
Fulfilment of individual International Classification of Headache Disorders, 2nd edn criteria for hypnic headache by patients in our series and those in the series reported by Liang et al. (6).
Comorbidities
Other headache disorders included MoA in four patients and TTH in one. Neurological examination was normal in all patients. Magnetic resonance imaging was performed in 17 patients and computed tomography in four. One patient declined neuroradiological investigations. These examinations revealed no abnormality in 18 patients, an arachnoidocoele in one female patient, remaining signs of a cerebral trauma in one male patient, and a microprolactinoma in a female patient. One patient had diabetes insipidus that arose at the same time as HH.
Mean systolic blood pressure was 130.2 ± 9.8 mmHg (range 110–150). Mean diastolic blood pressure was 74.8 ± 8.8 mmHg (range 60–95). Seven patients were considered to have hypertension.
Functional and emotional impact of hypnic headaches
Functional impact on daily living was assessed by the HIT-6 scale in 17 patients. The mean HIT-6 score was 58.4 ± 6.9 (range 45–70). Patient distribution according to the HIT-6 score is shown in Fig. 2. Eleven HH (64.7%) patients had a HIT-6 score of > 55.
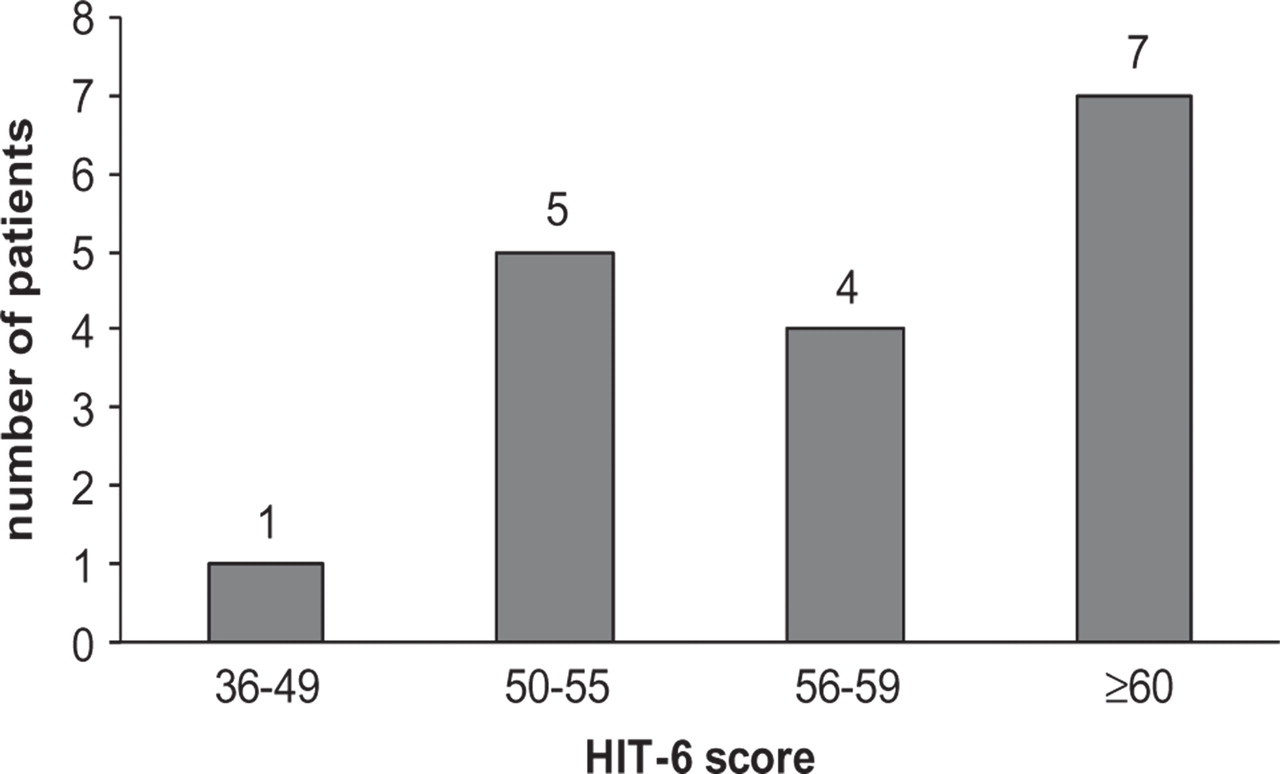
Distribution of hypnic headache patients as a function of headache-related disability score in the Headache Impact Test-6 scale (11).
Anxiety and depression were evaluated by the HAD-A and HAD-D scores, respectively, in 18 patients. The mean HAD-A score was 8.8 ± 4.4 (range 3–18). The mean HAD-D score was 5.4 ± 3.4 (range 0–11). Eleven HH (61.1%) patients had a HAD-A score of ≥ 8 and five (27.8%) a HAD-D score of ≥ 8.
Acute and prophylactic treatments of HH attacks
Five patients took no acute treatment for attacks. Three patients only drank a cup of coffee. Other patients frequently used an acute treatment (sometimes as the combination caffeine–paracetamol–dextropropoxyphene). Nonetheless, medication overuse was detected in only one patient. In addition, one patient used hypnotics and three used anxiolytics (meprobamate, n = 1; bromazepam, n = 2).
The majority of patients used no prophylactic treatment for their HH attacks. Only one patient received lithium, whereas eight were treated with oxetorone. No patient received flunarizine, verapamil or indomethacin.
Discussion
This series of 22 HH patients diagnosed over 5 years in two speciality headache centres in the South of France is the largest yet reported. Only one of the patients had been referred to the centre with a pre-established diagnosis of HH. The low rate of disease diagnosis, besides the long time elapsing between symptom onset and diagnosis, highlights the poor recognition of HH despite the stereotypical character of symptoms.
Further to the first description by Raskin in 1988 of aged patients regularly awakened by headaches of short duration associated with nausea but without other autonomic symptoms (1), different sets of diagnostic criteria for this syndrome have successively been proposed. Those first suggested by Goadsby and Lipton in 1997 (8) were then widened to include cases of unilateral pain and longer duration. The 2004 ICHD-II criteria now include dull quality of headaches but no obligatory lateralization, occurrence during sleep and awakening of patients, high frequency but no upper limit for duration of attacks, occurrence in ageing patients, absence of autonomic symptoms, and relative rarity of nausea, photophobia or phonophobia (9). Since then, however, several authors have again reported cases that somewhat depart from the ICHD-II criteria for HH.
Similar to the series reported by Liang et al. in 2008, our case series indicates that an appreciable proportion of HH patients do not meet the first ICHD-II criterion for HH, i.e. dull quality of headaches. Less than two-thirds of our patients (64%) fulfilled this criterion, compared with 88% according to patient recall and only 2/5 patients according to direct questioning in the series reported by Liang et al. (6). Similarly, Evers and Goadsby (2003) reviewing 71 cases of HH reported in the literature noted 38% of pulsating headaches (7). It thus appears that the ICHD-II A diagnostic criterion for HH should be revised to include headaches of other than dull quality.
Another classical hallmark of HH is its onset in patients aged ≥ 50 years (ICHD-II criterion C3). Most of our patients (95%) were actually aged ≥ 50 years at the time of diagnosis. In fact, unlike preceding series of HH patients (2, 6), at the time of symptom onset nearly one-quarter (23%) of our patients were aged < 50 years (41–47 years). More advanced age at the time of HH diagnosis usually results from the long time elapsing before diagnosis is established (≥ 10 years after symptom onset for 36% of patients in our case series).
Moreover, since the first criteria for the diagnosis of HH were suggested (8), frequency of headaches has been considered to be ≥ 15 times per month. Our patients' headache profile nevertheless indicates that headache frequency may be appreciably lower for a few HH patients (two patients with headache frequency < 15 days/month in our series). No case of HH evolving in periods was encountered in our series of 22 patients. Cases of episodic HH have been reported, however, in patients with prolonged active periods separated by periods of sustained remission, either spontaneous or following treatment-induced remission and subsequent treatment withdrawal (4).
In contrast, the duration of HH attacks in our patients conformed precisely to the usual duration of 15–180 min mentioned in the comments following the diagnostic criteria for HH (code 4.5) in ICHD-II, which admits that longer durations may be observed, however (9). In fact, the duration of attacks was ≤ 180 min in all HH patients in our series. Integration of this upper duration limit into the formal HH diagnostic criteria would probably enable exclusion of some other types of headache, e.g. TTH.
Evers and Goadsby have noted that nearly all HH patients in published series reported getting up during the headache and being active, because headache was worse when staying supine and, unlike migraine, there was no headache aggravation on physical activity (7). Dodick et al. also observed that HH patients started activities such as sitting in bed, walking or using ice packs (2). All four patients reported by Lisotto et al. also had to rise from bed and felt relief when walking (4). Since intermittent increases in intracranial pressure may occur during the rapid eye movement phases of sleep, De Simone et al. have suggested that orthostatism might alleviate episodes of intracranial hypertension (15). All patients in our series engaged in activities during the headaches: all systemically got up, most engaged in elaborate activities such as drinking (most often coffee), reading or watching television. This very typical behaviour should be considered as part of HH diagnostic criteria. It markedly differs from that of CH patients, who become restless and agitated during attacks. The ICHD-II B criterion could be appropriately modified to make it clear that the headache compels the patient to get out of bed.
The 1988 edition of the Classification and Diagnostic Criteria for Headache Disorders did not mention HH. In 1997 Goadsby and Lipton described HH amongst a group of primary headache disorders characterized by short-lived pain and prominent or sparse autonomic features that were assembled under the term ‘trigeminal autonomic cephalalgias’ (TACs) (8). In 2004, however, ICHD-II integrated HH not into Part 1, category 3 of the classification (‘Cluster headache and other TACs’), but into Part 1, category 4 (‘Other primary headaches’). In fact, HH positioning within headache disorders nosology appears difficult. In favour of ICHD-II Part 1, category 4 are the usual absence of autonomic signs or circannual rhythm. On the other hand, motor activity, circadian period, concomitant diabetes insipidus and intense thirst would be in favour of the implication of hypothalamic structures. This indeed raises the question of whether HH should be repositioned within the frame of TACs. However, there is very little in the literature that would permit in-depth discussion of this point: as yet, this is hampered by lack of endocrinological and functional neuroimaging studies on HH.
HH influence on mood and functioning in our series of patients was assessed using the HAD and HIT-6 scales. HAD anxiety and depression scores suggest that HH is generally associated with relatively moderate levels of anxiety and low levels of depression. Sixty-one per cent of our HH patients had a HAD-A score of ≥ 8, compared with 67% of migraine patients consulting in primary care and 76% of CH patients consulting in tertiary headache centres, in two previous studies carried out in France (16, 17). Slightly more than one-quarter (28%) of our HH patients had a HAD-D score of ≥ 8, compared with 59 and 43% of migraine and CH patients, respectively, in the two same French studies. Relatively low cut-off values were retained in all these surveys in order to secure detection of a maximum number of migraine subjects with anxiety and/or depression while retaining good levels of sensitivity and specificity (18, 19). HH impact on daily activities as assessed by the HIT-6 scale also seems comparable to that of migraine in primary care patients: the mean HIT-6 score was 58.4 in our HH patients, compared with 59.1 in a survey of migraine patients consulting in primary care in France (20), and 65% of HH patients had a HIT-6 score of > 55 (substantial or severe impact), compared with 64% in a population-based survey of consulting migraine patients in France (21). HH is indeed the only chronic daily headache associated with such a low level of medication overuse.
Concerning the prophylactic treatment of HH, most patients had no, or wanted to take no prophylactic treatment for their HH attacks. Although lithium is the therapy classically recommended for HH, it was prescribed to only one of our HH patients—and found ineffective. Eight patients were treated with oxetorone, an anti-serotonin drug recommended in France as a first-line treatment of migraine, with some efficacy. Since oxetorone has hypnotic properties, participation of a possible effect on sleep in oxetorone efficacy cannot be ruled out, however. On the other hand, good tolerability of oxetorone in this population of ageing patients may be a valuable advantage.
A strength of this study was the size of the series of HH patients identified over a relatively short time period. Comparison of our HH patients' characteristics and headache profile with the 2004 ICHD-II diagnostic criteria allowed the suggestion of some improvements in the current diagnostic criteria for HH, specifically to include headaches of any quality and introduce the typical motor activities displayed by HH patients during the headaches. Furthermore, endocrinological and neuroimaging studies would be desirable with a view to possibly reconsidering the place of HH in the nosology of headache disorders.