
Abstract
Nummular headache is proposed as a distinct type of headache in the Appendix of the second edition of the International Classification of Headache Disorders (ICHD-II). It is a chronic condition, with the following characteristics: pain is felt on a small circumscribed cranial area; pain is of mild to moderate intensity; there is no evidence of a structural abnormality. Herein, three cases fulfilling the ICHDII proposed criteria (code A13.7.1) for nummular headache are reported.
Introduction
Nummular headache (NH) is a term first coined by Pareja and colleagues in 2002 (1) for a distinct primary headache disorder. Its main feature is that the pain is felt in a small rounded or elliptical area of about 2–6 cm in diameter, usually with well-defined borders. NH is a chronic condition. The pain is of mild or moderate intensity and it may course with periods of exacerbation or remission. Herein, we report three cases of NH.
Case reports
Case 1
A 41-year-old woman reported, since she was 6 years old, a pressure-type pain in a rounded area of the vertex. The area was about 2.5 cm in diameter (Fig. 1). This pain was described as continuous, of mild intensity. She also reported exacerbations periods, lasting from 1 to 7 days, when the pain became severe. No triggers were reported. Associated symptoms, such as nausea, vomiting, photophobia, phonophobia, tearing, rhinorrhoea or conjunctival injection, were not reported. The only other remarkable factor from history was that she had systemic arterial hypertension controlled by low-salt diet.

Local and relative size of pain in three patients with nummular headache. The head is represented as an elliptical line. A, Anterior; P, posterior; L, left; R, right.
At examination, there were no signs or symptoms of sensory dysfunction in the symptomatic area and no tender pressure points were found. She had no cutaneous abnormalities on the painful area. No manoeuvre could trigger or bring relief to the pain.
Neuroimaging [computed tomographic (CT) scan] was normal. During exacerbation periods, intravenous (i.v.) metamisol had been used, providing some hours of pain relief, but the pain would reappear afterwards. Over time, the patient developed a clear-cut different sort of headache that met the criteria for chronic migraine. Control of this headache was obtained with monotherapy with amytriptiline (25 mg/day) or valproic acid (500 mg/day) or by a combination of propranolol (40 mg/day) and topiramate (50 mg/day).
Despite the successful treatment for chronic migraine, NH was completely refractory throughout her life. The following strategies were tried for NH: indomethacin 150 mg/day, local nerve block with lidocaine plus dexamethasone phosphate/acetate. No relief was obtained. On one occasion, during an exacerbation period, i.v. meperidine was tried, with only partial relief.
Case 2
A 29-year-old man suffered a mild brain and skull trauma on the left parietal area. Three months after the trauma, he reported the onset of continuous, mild intensity burning pain in the trauma site. Exacerbation periods lasting some hours and occurring two to three times a week were observed. During such periods, the pain was associated with bilateral tearing and rhinorrhoea. The pain had the peculiar characteristic of being felt in a circumscribed area of 2.5 cm in diameter (Fig. 1). No nausea, vomiting, photophobia or phonophobia were reported. He had no tender pressure points or cutaneous abnormalities, or signs or symptoms of sensory dysfunction in the painful area. A CT scan was normal. No response was obtained with amytriptiline 50 mg/day, indomethacin 150 mg/day or local nerve block with lidocaine plus dexamethasone phosphate/acetate.
Case 3
A 64-year-old man had been suffering right parietal pain since the age of 20 years. The pain was throbbing in nature, of moderate to severe intensity and worsened with physical activity. The pain was not associated with nausea, vomiting, photophobia, phonophobia or autonomic symptoms and had the peculiar characteristic of being felt in a circumscribed area of 4 cm in diameter (Fig. 1). During the previous 12 months the pain had been continuous. There was no history of analgesic overuse. He had Type 2 diabetes, arterial hypertension, dyslipidaemia and a history of smoking. Physical examination was unremarkable, including absence of signs and symptoms of sensory dysfunction in the symptomatic area. Magnetic resonance imaging showed discrete signs of subcortical vascular disorder. Indomethacin 200 mg/day, propranolol 40 mg/day and local nerve block with lidocaine plus dexamethasone phosphate/acetate brought no relief.
Further aspects observed may be seen in Fig. 1 and Table 1.
Clinical characteristics of three patients with nummular headache
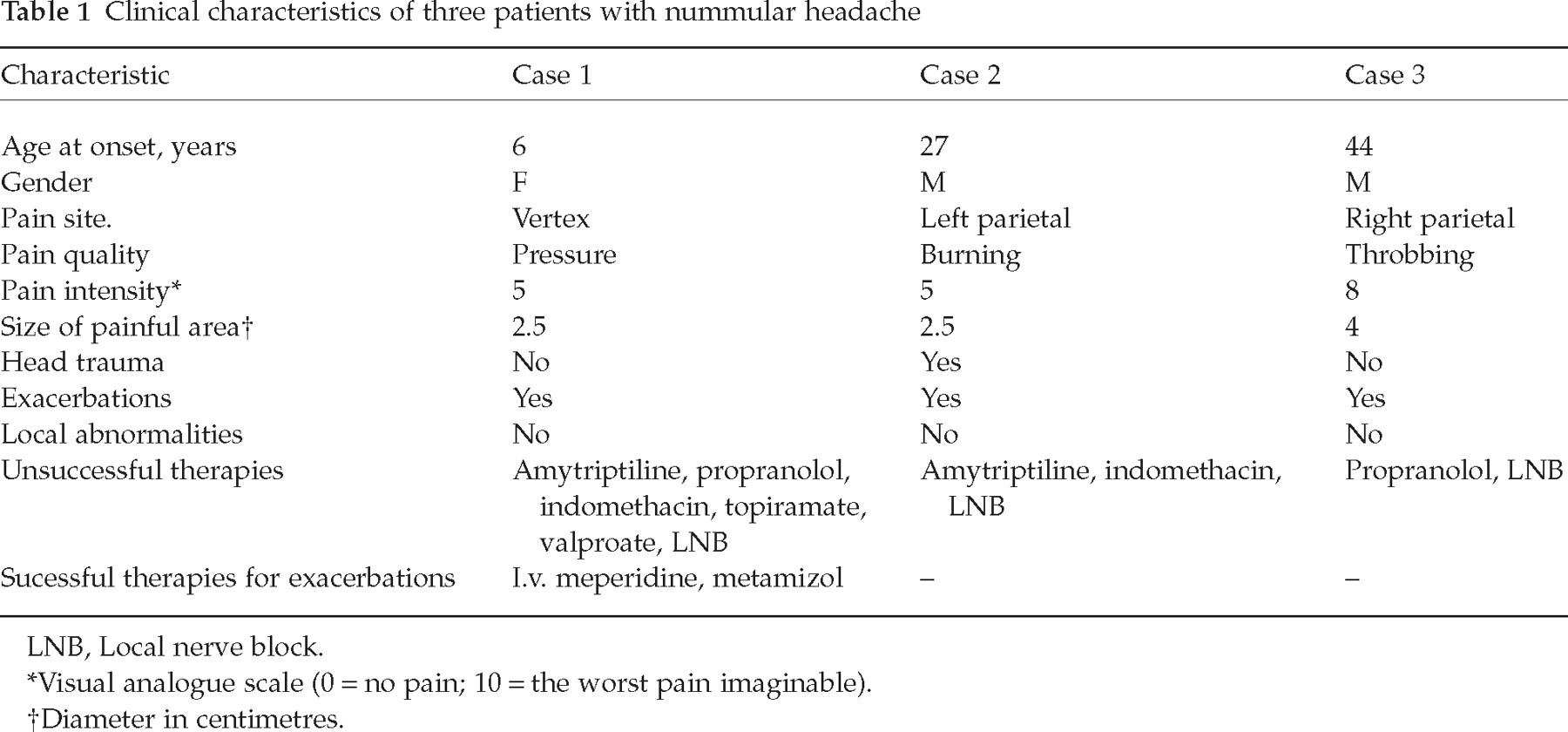
LNB, Local nerve block.
Visual analogue scale (0 = no pain; 10 = the worst pain imaginable).
Diameter in centimetres.
Discussion
Headache is a common disorder at all ages, with a prevalence as high as 80.8% in adults (2). During the last two decades, the 1988 classification of the International Headache Society (3) and more recently the International Classification of Headache Disorders (ICHD)-II (4) have provided standardized criteria for the full gamut of headache disorders. According to these classifications, headache disorders are subdivided into two main groups—primary headaches and secondary headaches. Migraine and tension-type headache are by far the commonest primary headaches (2, 5).
Furthermore, the ICHD-II presents criteria, in the Appendix, for some novel entities that have not been sufficiently validated by research studies. NH appears in the Appendix of ICHD-II coded as 13.7.1 (4). NH diagnostic criteria are shown in Table 2.
ICHD-II proposed diagnostic criteria for A13.7.1 nummular headache

ICHD-II, International Classification of Headache Disorders, 2nd Edition.
In Pareja’s series (1, 5), out of 27 patients, 19 presented with sensitive abnormalities on the painful area; in five, the pain started following a head trauma, even though a direct causal relationship was observed in only three of these cases. Six patients also presented with migraine and no patient had autonomic symptoms.
Pareja also reported that there were no effective treatments for NH (1). In a follow-up study (6), paracetamol has been shown to be beneficial as acute treatment. Gabapentin was an effective preventive therapy in two case reports (7, 8) and a case of NH was absolutely responsive to naproxen (9).
As for our series, in case 1 the pain, except for its peculiar localization, had characteristics of new daily persistent headache [ICHD-II, code 4.8 (4)]. Even though, during some periods, symptoms were compatible to chronic migraine [ICHD-II, code 1.5.1 (4)], the migraine headache was successfully treated, but NH persisted, being refractory even to opioids, suggesting that NH may be an entity of its own.
In case 2, the pain did not meet the criteria for chronic post-traumatic headache attributed to mild head injury [ICHD-II, code 5.2.2 (4)] because it did not meet criterion C (headache develops within 7 days after head trauma). On the other hand, the pain had aspects similar to those of constant pain caused by compression, irritation or distortion of cranial nerves or upper cervical roots by structural lesions [ICHD-II, code 13.12 (4)]. It is possible that the previous head trauma was the cause of the symptoms. Accordingly, this case did not meet the criteria for ICHD-II code 13.12, due to the difference in the putative causal mechanism and also the lack of anatomical or clinical sensitive abnormality. Moreover, another aspect in this case was the presence of bilateral tearing and rhinorrhoea during pain exacerbation periods. We could not prove that these signs were autonomic in origin. Since we did not observe a patient’s pain exacerbation, we prefer to explain it as simply a non-specific reaction to pain.
Case 3 presented a chronic head pain with some migrainous features: throbbing in nature, moderate to severe intensity, unilateral and worsening with physical activity. Although it could not be classified as chronic migraine [ICHD-II, code 1.5.1 (4)] because criterion A (headache meeting criteria for migraine without aura) was lacking, it did not even meet the criteria for probable chronic migraine either [ICHD-II, code 1.6.5 (4)] because criterion B (there is, or has been within the last 2 months, medication overuse). Moreover, no response to migraine prophylactic drugs was obtained.
We assigned a NH diagnosis based on the facts that: (i) the headaches did not fulfil diagnostic criteria for headache disorders from the main body of ICHD-II; and (ii) criteria for NH were fulfilled.
In our cases, as in most of those previously reported, the pain had a chronic–continuous character. Accordingly, differential diagnoses should be conditions such as chronic migraine, chronic tension-type headache, hemicrania continua and new daily persistent headache.
The variability of clinical presentations in our cases lead us to suppose that a localized headache of nummular type may represent many different underlying mechanisms and causes. In case 1, NH began during childhood, never disappeared and there was not related to any particular event. However, the behaviour of headache of nummular type was distinct from migraine as they had different features, clinical courses and responses to migraine treatment. In case 2, a previous local lesion might be related to the symptoms. Local, even though mild trauma, may lead to local demyelinization or injury in nerve endings with the ensuing neuromas, or even injury in cutaneous nociceptors triggering the mechanisms of neuropathic pain. The burning quality of the pain is suggestive of the latter mechanism. Against this possibility is the refractoriness of pain, even to local nerve blocks. Pareja (7, 10) has already suggested a peripheral mechanism for NH. Finally, case 3 may illustrate an idiopathic form of NH. Nevertheless, the characteristics of this case point to a central origin because of the presence of some migrainous features and the absence of pain relief with local nerve block.
Consistent with these hypotheses, we suggest cases 1 and 3 be regarded as central pain based on the absence of a peripheral mechanism of pain. We suggest case 2 be regarded as a neuralgia, using carbamazepine or phenitoin or lamotrigine or even clonazepan.
The present report on three cases of NH fulfilling ICHD-II (Appendix) proposed criteria shows the clinical polymorphism of a head pain of nummular type.
In some cases NH can be seen as a comorbid condition of migraine; in others, a kind of neuropathic pain associated with localized injury to nerves. However, in some instances NH is not attributable to any condition, and for this particular circumstance the term ‘primary’ NH is proposed.
Footnotes
Acknowledgements
The authors thank Dr Marcelo E. Bigal for critically reviewing the manuscript.