
Abstract
Whereas paroxysmal hemicrania (PH) is studied extensively in adults, even case reports of PH in children are rare. We present the first prospective follow-up study on PH in children. Our aim was to investigate whether differences exist between paediatric and adult patients. We assessed all children with chronic headache who were referred to our paediatric out-patient pain clinic within 3 years based on interviews and validated questionnaires. Among 628 patients we found five children with PH (0.8%) and three with probable PH (0.5%), in total 1.3%. Pain characteristics, autonomic symptoms and treatment response to indomethacin were similar to adult PH patients. Our results demonstrate that the International Headache Society classification of PH is also applicable to children. We suspect that PH has been underdiagnosed in children and therefore suboptimally treated thus far.
Introduction
Similar to other primary headaches (e.g. migraine), short-lasting headaches occur less frequently in children than in adults (1). According to the classification of the International Headache Society (IHS), short-lasting headaches include primary paroxysmal hemicrania (PH), cluster headache (CH) and sudden unilateral neuralgiform headache with conjunctival injection and tearing (SUNCT) (2–4). The classification of these so-called trigeminal autonomic cephalalgias (TACs) is based on clinical phenotype and response to pharmacological therapy. PH is characterized by multiple attacks of unilateral severe pain in the ophthalmic trigeminal nerve lasting from 2 to 45 min with a mean frequency of 12 attacks per day (range 2–40) (2, 3, 5–8). Attacks occur in association with at least one ipsilateral cranial autonomic dysfunction, such as ptosis, miosis, lacrimation, conjunctival injection, nasal obstruction or rhinorrhoea, indicating parasympathetic hyperactivity and sympathetic impairment (4). According to IHS criteria, the diagnosis of PH requires a rapid and complete therapeutic response to indomethacin treatment (2, 8, 9). In adults suffering from PH, 80% suffer from chronic paroxysmal hemicrania (CPH) without remissions, or remissions lasting for < 1 month. The remaining 20% are classified as episodic paroxysmal hemicrania (EPH) with remissions lasting for ≥ 1 month (10, 11). CPH mostly occurs in the third to fourth decade of life with a female preponderance (ratio female : male, 3 : 1) (7, 8, 12). In adults, CPH is rarely associated with various intra- or extracranial pathologies, e.g. head trauma, neoplastic or inflammatory disease (7, 13–16). Attack duration and response to pharmacological therapy help to distinguish PH from other TACs (7, 17). CH, the most common TAC, is characterized by a long attack duration (10–180 min) and a relatively low attack frequency (16, 18). Both children and adults with CH respond well to oxygen (19, 20). SUNCT is extremely rare and characterized by a very short attack duration (5–240 s) (21). It is assumed that the pathophysiology of all TACs has common pathways. Functional brain imaging studies have demonstrated activation of the posterior hypothalamus grey matter in all TACs (22–30). Furthermore, positron emission tomography has shown activation of the contralateral posterior hypothalamus and contralateral ventral midbrain in PH (26). The hypothalamus modulates nociceptive and autonomic pathways (31) of the trigeminal nerve, and the hypothalamus supposedly is the mediator of pain attacks (activation of the ophthalmic trigeminal nerve) and cranial autonomic symptoms (central disinhibition of the trigeminal-autonomic reflex) (2, 32–34). Variation in duration and frequency of attacks may depend on different disorders of the inferior posterior hypothalamic neurons (35).
Whereas PH is a well-known diagnosis among adult neurologists, awareness and knowledge of PH in children is scarce. Based on a Medline search we found only nine published case reports (36–45). Three of these nine children met IHS criteria (37, 40, 42). Few of the published reports specified duration and frequency of attacks, autonomic signs or response to indomethacin. Until now, it has not been known if PH in children follows similar patterns as in adults (36). We therefore present the first prospective follow-up study on PH in children. Our aim was to investigate potential differences between paediatric and adult patients with PH and to describe the therapeutic response to indomethacin.
Methods
Between January 2005 and December 2007 all children and adolescents aged 0.5–18 years who were referred to the out-patient clinic of the Vodafone Foundation Institute for Children's Pain Therapy and Paediatric Palliative Care due to chronic headache were included in a prospective study on out-patient treatment. Chronic headache was defined as persistence of headache symptoms for > 3 months according to McGrath et al. (46). Participants were divided into two age groups depending on their age on admission: children aged 2–10 years and adolescents aged 11–18 years. In the present study, results of patients with PH will be presented. The design of the study is demonstrated in Table 1.
Study design
Prior to their first visit, all children with chronic headache and their parents received four questionnaires by mail. On their first visit they were seen for at least 1 h by a paediatrician together with a clinical psychologist, both specialized in the treatment of pain disorders. Outcome measures were pain location, intensity, duration, frequency and quality within the last 7 days, accompanying autonomic symptoms and other somatic aspects, circadian periodicity, triggering factors, days absent from school, pain-related disability, pain-related coping strategies, treatment response to indomethacin and side-effects. All outcome measures were assessed at first consultation and during follow-up visits 3, 6 and 12 months following the first visit to our institute (see Table 1). All parameters were assessed either during the clinical interview, via self-report or a pain diary: (i) the German questionnaire for children with chronic pain (DSF-KJ) contains 10 items for children (age 4–10 years), 29 items for adolescents (age 11–18 years) and 48 items for their parents. The DSF-KJ was completed by children and parents separately; (ii) patients reported pain intensity on a numerical rating scale (NRS; 0 = no pain to 10 = maximal pain). This scale has been shown to be valid and sensitive in adult samples (47). NRS was categorized into four categories: 1–3 (mild pain), 4–6 (moderate pain), 7–9 (severe pain) and 10 (very severe pain) (48); (iii) pain-related disability in daily activities was assessed with the Pediatric Pain Disability Index (P-PDI) (49), which comprises 12 items such as attending school, doing homework, physical activity and sleeping habits, each rated on a five-point Likert scale (1 = never to 5 = always). P-PDI mean scores ranged between 1.0 and 5.0; high scores represent a high degree of disability; (iv) children's school absence was assessed by parents' report as missed days from school within the 4 weeks preceding the visit; and (v) pain-related coping strategies (passive pain coping, seeking social support and positive self-instruction) were assessed with the Pediatric Pain Coping Inventory-Revised (PPCI-R), consisting of 25 items rated on a three-point scale (0 = nearly always, 1 = sometimes, 2 = often) (47). PPCI-R mean values range between 0 and 2; the higher the value, the more the child used the respective coping strategy. It demonstrated good reliability with internal consistencies of the scales ranging between 0.71 and 0.80 (47). Patients underwent a physical and ophthalmological examination, cranial magnetic resonance imaging (MRI), electroencephalography and blood tests.
Descriptive statistics such as means, standard deviations and frequencies were computed for the relevant outcome measures. The analyses were calculated using
The Committee for Ethics in Medical Research of the Children's Hospital Datteln—Witten/Herdecke University approved the study.
Results
Classification according to diagnosis
Six hundred and twenty-eight children and adolescents with chronic headache visited the out-patient pain department in the study period of 3 years. Mean age of patients was 11 years (range 2.1–17.8), 48% were children (< 11 years) and 52% adolescents (≥ 11 years); 59% of patients were female, 41% were male (ratio 3 : 2). Most patients suffered from tension-type headache (TTH) or probable TTH (28%) and migraine or probable migraine (15%) or a combination of both (54%). Nine patients (1.4%) suffered from chronic daily headaches unspecified and two patients (0.3%) from medication-overuse headache. PH according to IHS diagnostic criteria was present in five of 628 patients (0.8%) and was probable in another three patients (0.5%) (Table 2).
Headache diagnoses of the sample (n = 628) within a 3-year period
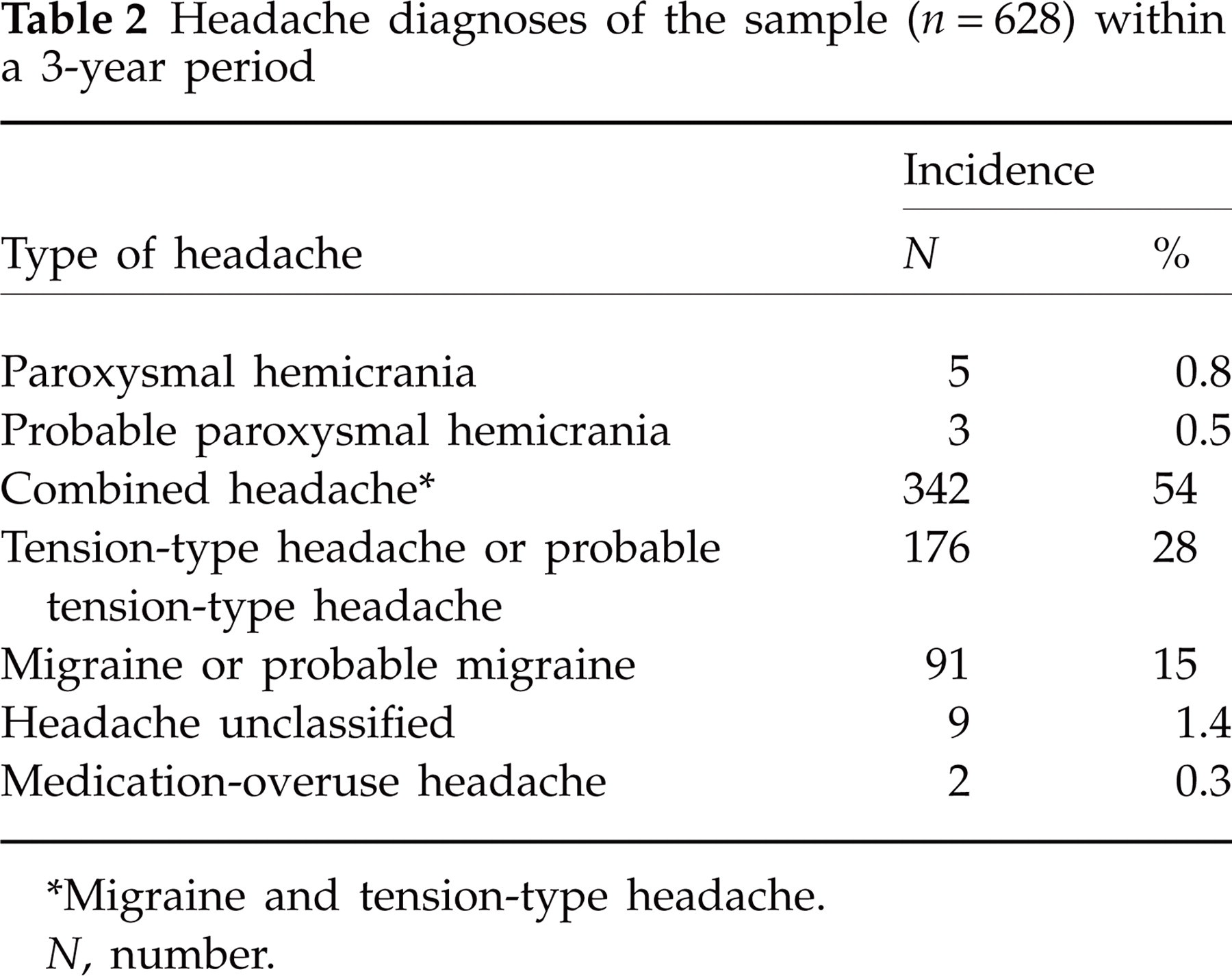
∗Migraine and tension-type headache.
N, number.
Sample characteristics, medical history and examination findings
Table 3 presents the clinical phenotype of each patient with PH according to IHS diagnostic criteria. Five children (nos 3 and 5–8, Table 3) clearly fulfilled diagnostic criteria for PH according to the IHS (0.8%). Three patients (nos 1, 2 and 4) had minor variations according to the IHS (0.5%). They could be classified as probable PH due to accompanying autonomic symptoms and responsiveness to indomethacin therapy (see below). Three of the eight patients were female and five were male. The mean age of headache onset was 5.9 years (range 2.6–12.11 years). The mean time from first symptoms to diagnosis of PH was 18 months (
Diagnostic criteria for paroxysmal hemicrania (PH) in the study patients

∗Facial paleness.
IHS, International Headache Society; M, male; F, female.
In a proper medical work-up of all patients with PH, we found no evidence of secondary cases of PH or coincidental MRI abnormalities.
Pain characteristics
Pain was paroxysmal and very severe (n = 3) or severe (n = 4) except for the youngest patient (no. 1) with moderate pain. Mean pain intensity was 8.4 (
Age at onset, time to diagnosis, duration and pain characteristics of the study patients with PH

∗Probable PH.
†Monitoring < 1 year.
PH, paroxysmal hemicrania; F, female; M, male; CPH, chronic paroxysmal hemicrania (no remission within 1 year); EPH, episodic paroxysmal hemicrania (remissions lasting ≥ 1 month); NRS, numerical rating scale.
Autonomic and accompanying symptoms according to IHS criteria
All patients had autonomic symptoms ipsilateral to pain as shown in Table 3. The most common autonomic symptoms were facial sweating (n = 6) and conjunctival injection (n = 3). Most patients (n = 5) showed a combination of these symptoms. Autonomic symptoms were different from the IHS classification in the youngest patient (no. 1), who had facial paleness only. Facial paleness was also present as an additional symptom in another patient. Phonophobia (nos 5, 6 and 8) and mild nausea (nos 3 and 5) were the only migrainous features. One patient (no. 3) felt exhausted.
Circadian and circannual periodicity and triggering factors of pain attacks
All patients had daytime attacks. Three patients also suffered from nocturnal attacks. The attacks occurred spontaneously without any regular preponderance throughout the circadian period. Most of the children (n = 5) suffered from chronic pain attacks without remission (CPH) and only two from episodic pain attacks (EPH) with remissions lasting for 2 months and 3 months within a period of 1 year. The last patient included in our study in September 2007 (no. 6; Table 4) could be monitored for only 6 months, in which he had no relapse. Triggering factors were physical effort (n = 5) rather than emotional stress. Lying down and relaxing led to pain relief (n = 6).
Pain-related disability and coping strategies
Impairment of everyday life activities due to pain was strong (P-PDI 2.8, mean ± 1.0) and increased with patient's age (see Table 5). For most children it was difficult or impossible to engage in their favourite activities, particular meeting friends (n = 5), watching television (n = 4), reading (n = 3), doing handicrafts (n = 2) and doing sports (2). Three patients no longer attended school or kindergarten and two patients missed 50% of school days. Patients had a mean of 9 days absent from school or kindergarten within the month preceding presentation to our out-patient clinic. Most children were exhausted and had a tendency to lie down during pain attacks. In the PH sample, children demonstrated a tendency to use passive pain coping strategies (2.1 ± 0.3 mean) and seeking social support while in pain (2.1 ± 0.4), as well as a tendency to demonstrate positive self-instruction (1.9 ± 0.5; see Table 5).
Pain-related disability and coping strategies

F, female; M, male.
Therapeutic response to indomethacin and adverse effects
Indomethacin therapy was effective in all patients at an average effective daily dose of 3 mg kg−1 day−1 (divided into three doses a day, see Table 6). Mean frequency of attacks was lowered from eight attacks per day to one attack per month at follow-up after 3 months, mean pain intensity of the remaining attacks was reduced from 8.4 to 1.9 on NRS and mean duration from 30 min to 8 min (see Table 6 and Fig. 1). Improvement of headache occurred within a few days of initiating the effective dose. Two of the three children with additional interictal TTH were free of headaches and one suffered less often from headaches. All patients attended school regularly and showed little impairment of everyday life activities due to pain [mean P-PDI reduced from high (2.8) to low scores (1.4)]. As shown in Fig. 1, the therapeutic effect of indomethacin persisted in all patients after 6 and 12 months' follow-up. After 3 months we reduced indomethacin to the lowest maintenance dose, which was 0.5 mg kg−1 day−1 on average (see Table 6). Reduction below this dosage resulted in aggravation of pain attacks. Re-increasing indomethacin doses was successful in all patients. One patient had a dramatic increase of pain attacks the day after omitting indomethacin intake at night. One patient (no. 1) was able to stop indomethacin after 6 months without recurrence of headaches. In one patient (no. 7) we had to discontinue indomethacin after 6 months due to adverse effects (see below), resulting in prompt recurrence of pain attacks. We switched therapy to topiramate (3 mg kg−1 day−1). Unfortunately, the patient developed the same adverse effects as before. With reduction of topiramate to 0.5 mg kg−1 day−1, adverse effects disappeared and the patient was still free of headaches.
Indomethacin dose and pain relief after 3 months

F, female; M, male; NRS, numerical rating scale; P-PDI, Pediatric Pain Disability Index.
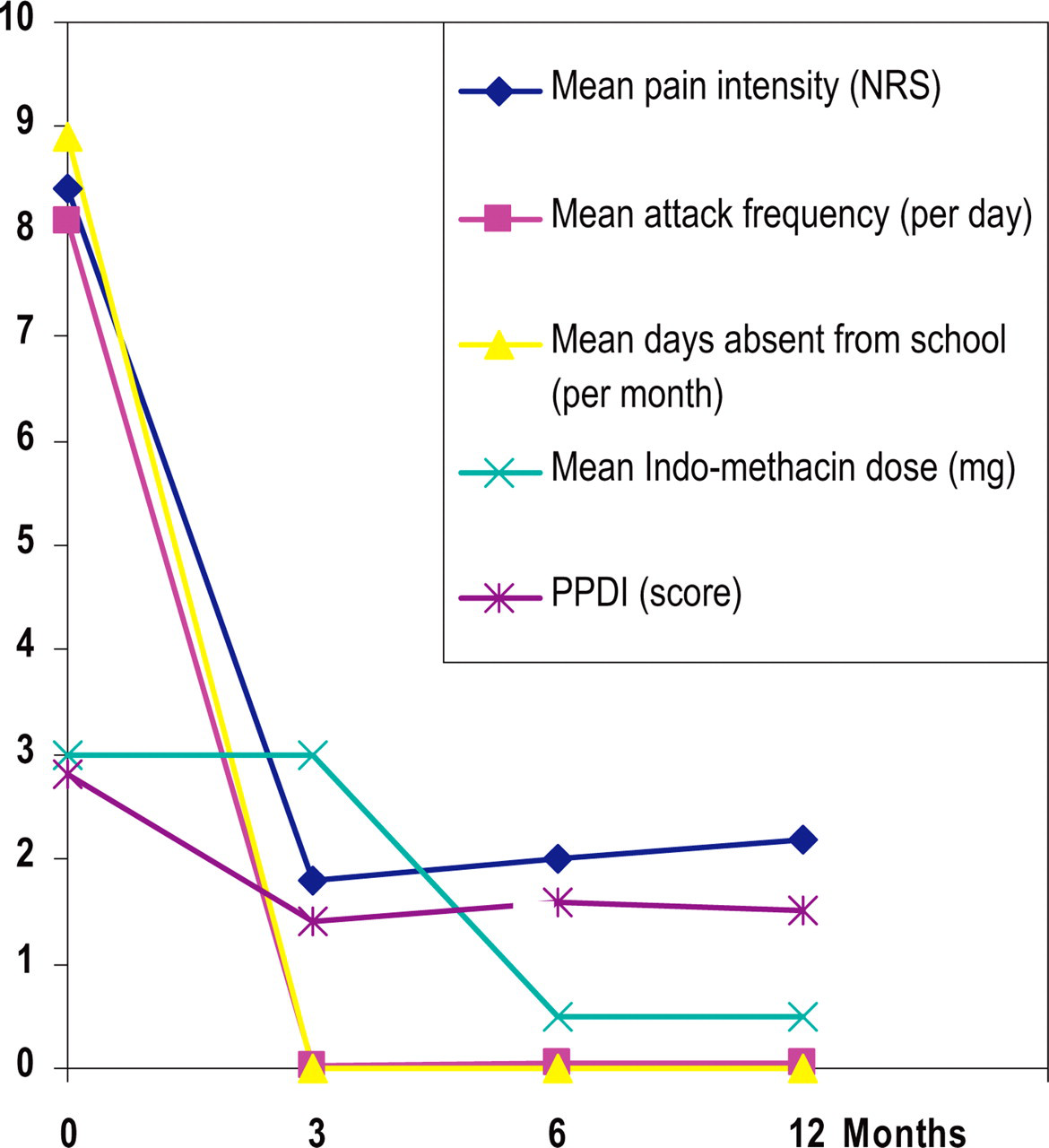
Indomethacin dose and pain relief after 3, 6 and 12 months. Units are given in parentheses for each parameter. NRS, numerical rating scale; PPDI, Pediatric Pain Disability Index.
Adverse effects were observed in one-half of our patients. At a high dose of 3 mg kg−1 day−1 one patient required treatment with proton pump inhibitors due to gastrointestinal side-effects. At a dose of 2 mg kg−1 day−1, two patients developed restlessness and aggressive behaviour, and one of them additionally suffered from sleep disturbances and sweating. In one patient adverse reaction disappeared with reduction of indomethacin to 1 mg kg−1 day−1. In the other patient indomethacin had to be discontinued after 6 months due to adverse effects, promptly resulting in recurrence of pain attacks (see above). Another patient developed transitory mild fatigue, lack of concentration and loss of appetite only during the first 3 weeks of therapy. Further adverse effects were not seen in long-term therapy. None of the patients developed tachyphylaxia.
Discussion
To our knowledge, this is the first study to address the question of whether PH in children follows a similar pattern as in adults (36). In the previous published nine case reports, only three of nine children met IHS criteria (37, 40, 42), and few authors specified the duration and frequency of attacks, autonomic signs and response to indomethacin. According to the IHS classification, five of our patients clearly fulfilled diagnostic criteria for PH and three patients (nos 1, 2 and 4) had minor variations, such as pain location in the forehead midline in the two youngest patients (nos 1 and 2). Perhaps their age accounts for the difficulty in locating their pain in accordance with the clinical knowledge that most young children describe pain in the midline of their body. There are also reports in which headaches with bilateral attacks were determined as PH due to prompt responsiveness to indomethacin therapy in adults (2, 7, 50–53). In addition, long attack durations were slightly too long for IHS in two patients (nos 2 and 4). However, reports in adults with even longer pain duration still defined their patients as suffering from PH (2, 3, 5–8). Furthermore, autonomic symptoms were different from IHS criteria in the youngest patient, who had facial paleness only. Facial paleness was present in one-quarter of our patients. Probably, this is a relevant sign in children that require attention. We believe that all three patients should be classified as probable PH due to accompanying autonomic features and prompt responsiveness to indomethacin therapy. Surprisingly, we found no patient with CH, which has a higher population-based prevalence than PH, and there are also more case reports on CH in children (16). As PH and CH share typical clinical features, the question arises of whether some of the children classified as PH may have suffered from CH. Compared with CH, our patients had short attack durations (45–90 min on average for CH) and no circadian or circannual cluster periods or predominant nocturnal attacks (54). Patients with CH are usually unable to lie down and characteristically ‘thrash around’ (54, 55). In contrast, most of our children had a tendency to lie down during pain attacks and remained exhausted for some time, as previously reported (6, 8, 12, 36, 56). None had a sense of restlessness, agitation or bizarre behaviour during attacks. However, good discrimination is possible by response to therapy. Oxygen inhalation had no benefit in the patient (no. 4) with a previous diagnosis of CH and two of our patients with long attack duration (nos 2 and 6). The response to indomethacin in our patients suggests that the children may have suffered from PH. For CH, indomethacin response has not been systematically evaluated (54). Sjaastad found indomethacin inactive in CH (57). Anecdotal evidence suggests that some CH patients respond to indomethacin, but the response rate appears to be less than seen in PH (54). However, it is striking that there were eight patients with PH but none with CH. Perhaps the prevalence of PH in childhood is underestimated. Based on a Medline search we found only nine case reports in children (36–45) (see Table 7). Our results suggest a higher prevalence of PH in children than estimated from case reports. Among 628 children with chronic headaches we found five children with PH (0.8%) and three with probable PH (0.5%), in total 1.3%. Numbers may have been overestimated due to the tertiary character of our institute. However, our study is one of the largest assessing children with chronic headache in an out-patient setting, even though is not epidemiological. We may speculate that the low rates of PH in children may have resulted in less attention to PH in clinical settings. This may result in failure to diagnose these children and subsequently administering inadequate treatment and underestimating its prevalence. In line with the above, time from first symptom to diagnosis was long in our study, consistent with other case reports in children (37, 39, 43). PH seems to be present in any age group. Two of our patients with probable PH were only 2 years old at pain attack onset. In the literature there is a report of one patient with pain onset at 1 year old (38).
Characteristics of patients with paroxysmal hemicrania in all case reports of children based on a systematic Medline search
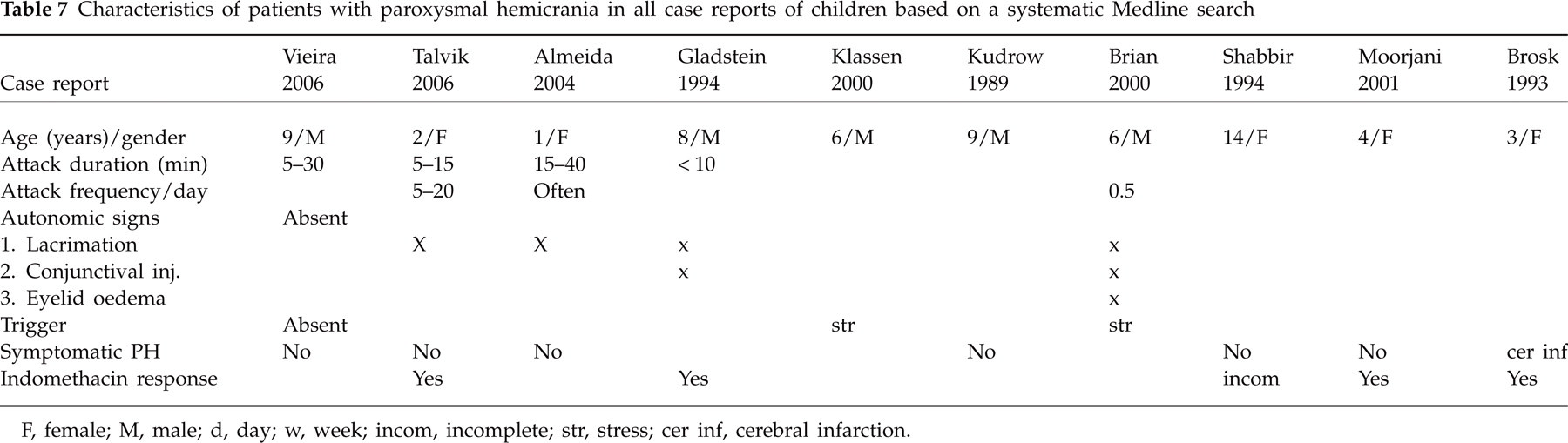
F, female; M, male; d, day; w, week; incom, incomplete; str, stress; cer inf, cerebral infarction.
According to the presentations in our study, clinical symptoms of PH in children resemble those of adults. Only the frequency of attacks and nocturnal attacks were lower (58), which is in line with other case reports in children (7, 37–40). The only migrainous features were phonophobia and mild nausea, similar to adults (8). We found no trigger factors apart from physical effort and emotional stress, as previously described in children (40). Interictal TTH was present in one-third of our patients in accordance with reports on adults (6, 58). We found no MRI abnormalities or symptomatic cases of PH according to most cases in adults.
It is noteworthy that the eight patients were highly impaired in their quality of life due to their pain. Similar to other chronic pain patients, they demonstrated severe pain-related disability and frequent absence from school. Given these characteristics and the significance of pain-related disability for children's development, adequate and effective treatment needs to be established for these children as soon as possible (59, 60). Our preliminary data suggest that indomethacin may be the treatment of choice demonstrated in a clear reduction in pain characteristics and lasting efficacy. The initial average effective daily dose of 3 mg kg−1 day−1 kept them nearly free of headaches. The very few remaining attacks were significantly reduced in intensity, duration and pain-related disability. Also, interictal TTH was gone in two patients and decreased in one. These results concur with adult patients. It is an issue for further research whether therapeutic response to indomethacin should be a diagnostic criterion for PH in children. To avoid side-effects, dosage adjustments of indomethacin to the lowest maintenance dose are necessary as soon as possible. It was 0.5 mg kg−1 day−1 in most of our patients, which is comparable to the adult maintenance dose (25–100 mg daily) (61). Long-term treatment is usually necessary. Nevertheless, one of our patients was able to stop indomethacin after 6 months without recurrence of headaches. Long-lasting remissions after indomethacin withdrawal have been reported in some patients with CPH (62). One of our patients who did not tolerate indomethacin was free of headaches with topiramate, as has been demonstrated in previous case reports on PH in adults (58, 63). Long-term therapy with indomethacin is generally well tolerated (2, 8, 9) in adults. In contrast to adults, we observed mild adverse effects at a moderate dose in one-third of our children, including restlessness, aggressive behaviour, sleep disturbance, sweating and gastrointestinal side-effects at a high dose. Most adverse effects disappeared by dose reduction (50%) and treatment with indomethacin suppositories.
Limitations
While this is the first comprehensive study to investigate PH in children, there are some noteworthy limitations. The number of children diagnosed with PH—albeit larger than in other studies—was small and did not allow for statistical comparisons. Future multicentre studies are needed to investigate treatment effectiveness properly from a statistically and clinically significant point of view. Results presented here stem from a tertiary institute, and frequency of PH diagnosis may have been overestimated. As already pointed out, the present study was not conceptualized as an epidemiological study. Future studies in primary, secondary and tertiary care are needed to investigate properly the prevalence and incidence in children and adolescents.
Conclusions
Our results demonstrate a higher prevalence of PH in children than previously expected from case reports. Although this analysis of PH in children is not epidemiological, we assume that PH may have been underdiagnosed in children and suboptimally treated in primary care. Pain characteristics, autonomic symptoms and treatment response to indomethacin were similar compared with adult PH patients. We therefore consider the IHS criteria of PH as applicable to children. Because of severe pain-related impairment of everyday life, it is crucial to diagnose children with this headache syndrome correctly as soon as possible. Suffering in children with PH can be significantly reduced with adequate treatment. According to our results, it is necessary to improve paediatricians' attention to PH in children. Future epidemiological studies are necessary to establish the incidence of PH in children and prospective studies to assess indomethacin long-term therapy and adverse effects.