
Abstract
The patients of this prospective study were analysed for headache as a sequela of surgery for acoustic neuroma (AN). Thirty-two per cent (30/95) of patients complained about a persisting headache syndrome with a severity of at least 6/10 on the nominal analogue scale 6 months after surgery. The occurrence of headache was significantly correlated with the prospectively evaluated parameters preoperative headache and the number of perioperative complications. Postoperative failure to return to the preoperative level of activity was also associated with the occurrence of headache, but also with the risk of retirement after successful surgery of the AN. Headache is therefore, like postoperative ataxia, dysgeusia and probably facial paresis, an important factor for the overall outcome of patients after AN surgery. Hypacusis is not as important. The symptoms and course of each individual patient were analysed. The attempt to categorize the headaches according to the second edition of the International Classification of Headache Disorders revealed five headache syndromes, the most prevalent being tension-type-like headache (46.7%), followed by neuralgia of the occipital nerve (16.6%), trigeminal neuropathy (16.6%), neuropathy of the intermedian nerve (10.0%) and cervicogenic headache (10.0%). The respective pathophysiological mechanisms are discussed and treatment options based on the clinical picture are presented.
Introduction
Headache is a well-known sequela after surgery for acoustic neuroma (AN) with a prevalence of up to 75% (1). Its frequency depends, among other things, on the surgical approach (translabyrinthine, suboccipital, cranioplasty, intradural drilling) and the time of survey after the operation. Based on mainly retrospective studies, it has been characterized as tension-type-like (2–4) or as headache occurring in severe and short-lasting attacks (5). In the latter study, a small subgroup was shown to meet the criteria for the primary headache syndromes tension-type headache and migraine. Hearing problems, facial paresis and gait ataxia are also cited in the literature as the most significant postoperative symptoms.
In the present study, 113 consecutive patients suffering from AN were analysed prospectively in order to characterize this subgroup of post-craniotomy headache further. First, we were interested in pre-, intra- and postoperative risk factors for the occurrence of headache after surgery. Second, the impact of AN surgery-associated headache on the patient's life was analysed by assessing private and professional outcome and subsequent correlation with the occurrence of headache. Finally, we tried to classify the headache of every individual patient according to the International Classification of Headache Disorders, 2nd edn (ICHD-II) (6) and grouped them into headache syndromes. We present interpretations of these entities with respect to pathophysiology and treatment options.
Patients and methods
Study population
All patients undergoing AN surgery between March 1993 and May 1999 in a large neurosurgical department in a university hospital in Southern Germany were recruited. One hundred and thirteen in-patients agreed to participate and gave their written informed consent. They were interviewed about personal details (age, sex, family history of AN) and asked to fill in a standardized questionnaire, which included information on pre- and postoperative symptoms with a focus on headache and cranial nerve function. Facial paresis was classified semiquantitatively as none, moderate or severe according to House and Brackmann (7). The presence and classification of pre-existing headache were recorded, if recalled by the patient. The short form of the German version of the Prime MD Patient Health Questionnaire was used to assess psychiatric comorbidity (present or not present) with a focus on depression and anxiety disorder (8). The entity acoustic neuroma surgery-associated headache was distinguished from a pre-existing headache by a change in the location, intensity or character and from regular postoperative headache due to wound healing by a duration of > 6 months. To be particularly specific in identifying pain instead of an unspecific strange feeling of the head or face, only relevant headache of an intensity of at least 6/10 on the numerical analogue scale (NAS) was considered. Current headache was categorized according to location, character, periodicity, radiation, associated symptoms, alteration over time and treatment (oral medication, diagnostic blockade or surgical neurolysis). Each patient underwent a standardized neurological examination on the day of admission, prior to discharge and 3 and 12 months later. After this 1-year visit, follow-up of the individual patient was discontinued.
Tumour characteristics
Preoperative classification of the tumours was done according to Matthies (9) using gadolinium-enhanced magnetic resonance imaging or, if this was contraindicated, computed tomography: T1, intrameatal; T2, intra- and extrameatal growth; T3, tumour reaches the brainstem; and T4, tumour compresses the brainstem. The images were analysed independently by one of the authors (C.G.), the surgeon and a neuroradiologist: if two or more of them were of the same opinion, this was assigned to the subject; if there were three different opinions, the middle one was chosen. All tumours were histologically classified by our Neuropathology Department.
Surgical procedure
Surgery was performed using a suboccipital osteoplastic approach with internal debulking and microsurgical tumour removal. The integrity of the facial nerve was monitored intraoperatively by continuous electromyography and that of the acoustic nerve by acoustic evoked potentials. The degree of tumour removal was classified (complete resection, remaining capsula and subtotal resection) and the microscopic continuity of the facial and vestibulocochlear nerves was recorded according to the surgeon's estimation before wound closure.
Outcome classification
Surgical outcome was classified according to the Glasgow outcome score (GOS; 5, good recovery with resumption of normal life despite minor deficits; 4, moderate disability with independent life despite disability; 3, severe disability and dependence for daily support; 2, persistent vegetative state; and 1, death). The consequences of surgery on quality of life were assessed qualitatively by collecting data using a modified short version of the SF-36 (Medical Outcomes Study-36, Item Short Form Health Survey) with a focus on the resumption of occupation, retirement within the first postoperative year and subjective return to the preoperative level of activity (10). New postoperative facial paresis was classified in the same way as preoperative facial paresis and according to the time of its occurrence (early, after surgery and prior to discharge; late, at the 3-month follow-up).
Statistical analysis
Statistical analysis was performed using
Results
Study population
Of the 113 study patients, 50.4% were female (Table 1). The mean age of all patients was 51.3 years (± 12.8) and was significantly higher than that of the subgroup with neurofibromatosis type 2 (26.4 years ± 10.9; P < 0.001). The ANs were located more often on the left than on the right, and tumour size was generally larger than T1. Preoperative symptoms included hearing problems (hypacusis and tinnitus) and other cranial nerve dysfunctions (vertigo, trigeminal hypaesthesia, facial paresis and dysarthria). On admission, a pre-existing headache or facial pain was described by nine patients: four (3.5%) had trigeminal neuralgia, three (2.7%) episodic tension-type headache and two (1.8%) migraine (Table 1).
Characteristics of the study population, including demographic parameters (gender and age), information on the tumour and preoperative symptoms including headache

NA, not available; NF-2, neurofibromatosis type 2; TTH, tension-type headache; TN, trigeminal neuralgia.
Of the preoperative symptoms, hypacusis (P < 0.001), dysarthria (P = 0.042) and trigeminal hypaesthesia (P < 0.001), but not trigeminal neuralgia, were significantly correlated with tumour size (Table 2).
Correlations between tumour size and clinical parameters

TN, trigeminal neuralgia; GOS, Glasgow outcome score.
The drop-out rate was as follows: GOS could be assessed from 105 patients prior to discharge. After 1 year, 107 patients filled in the questionnaire concerning resumption of occupation. One hundred and one answered questions on the return to preoperative levels of activity, and an evaluation of headache was possible in 95 cases.
Surgical outcome
In 83.2% of patients, the AN could be completely resected. Subtotal removal was documented in 12.4% and a remaining capsula in 4.4%. The main perioperative adverse effects were early (none to moderate in 71, severe in 40 cases) and late (none to moderate in 84, severe in 15 cases) facial paresis, hypacusis (81.3%) and in 30 cases (26.5%) surgical (liquorrhoea, infection, neurological deficit) or in 6.2% anaesthesiological problems. A second revisional operation was necessary in 18 patients (15.9%). GOS could be assessed in 105 patients (Table 3): 89% of these were able to at least lead an independent life. One patient died due to intraoperative haemorrhagic cerebellar infarction. Tumour size and postoperative facial paresis, but not GOS, were significantly correlated with each other (early P < 0.001, late P = 0.005; Table 2).
Outcome of acoustic neuroma surgery assessed by Glasgow outcome score and its impact on the ability to work

Assessment of private and vocational activity
After 1 year, 107 patients could be evaluated for the resumption of occupation and retirement. Of these, 26 (24.3%) had been retired prior to surgery and three were still receiving medical treatment for other diseases. Fifty-seven (73.1%) of the remaining 78 returned to work after a mean of 6.6 ± 4.3 months. Sixteen (20.5% of 78) of those who did not return to work retired during the year of study. A subjective return to the preoperative level of activity was declared by 76 of 101 (75.2%) patients.
GOS and the ability to return to work were significantly correlated with each other (P < 0.001). Table 4 shows that the risk factors for retiring after surgery were the number of complications (P = 0.004) and subjective failure to return to preoperative levels of activity (P < 0.001), but not tumour size or age.
Risk factors for postoperative retirement, failure to return to the preoperative level of activity and headache

For retirement, only relevant data are shown. The occurrence of headache is significantly correlated with the presence of preoperative headache, the number of perioperative complications and with the return to the preoperative level of activity.
Patients who did not return to their preoperative level of activity had significantly more perioperative complications (P < 0.001), operative revisions (P = 0.003) and suffered postoperatively from facial paresis (P = 0.05), dysgeusia (P = 0.046) and ataxia (P < 0.001). They retired significantly more often (P < 0.001, Table 4). A correlation with preoperative parameters could not be formulated. Four out of five patients with psychiatric comorbidity (depression or anxiety disorder) stated that they could not return to their preoperative level of activity (P = 0.013).
Acoustic neuroma surgery-associated headache
Statistics
Thirty (32%) of 95 patients described a headache reaching at least 6 on the NAS and persisting for ≥ 6 months after surgery. In six (20%) of these, pain intensity was ≥ 8. Table 4 demonstrates correlations between pre-, peri- and postoperative parameters and the occurrence of post-surgery headache. The presence of a preoperative headache syndrome (P = 0.026), the number of perioperative complications (P = 0.042) and the postoperative return to preoperative levels of activity (P = 0.023) were significantly correlated with headache after surgery. For the remaining preoperative variables (age, gender, tumour size, neurological deficit) no association or tendency (P < 0.15) could be found. According to binary logistic regression analysis using the parameter pre-existing headache, this variable predicts the occurrence of headache after AN surgery (P = 0.028) correctly in 71.6% with a sensitivity of 20.0% and a specificity of 95.4%. Patients with pre-existing headache and postoperative headache stated a marked difference between both with respect to the location and quality of the pain (data not shown). Within the subgroup good recovery/moderate disability (GOS 5 and 4) the probability of retirement was significantly correlated with the development of headache after AN surgery (P = 0.011). No correlation was found between psychiatric comorbidity and the occurrence of headache.
Figure 1 is based on Table 4 and depicts the correlations between comorbidity (psychiatric and positive history of headache) and surgery (intra- or postoperative events) on the one hand and the consequences (postoperative headache, return to preoperative levels of activity and retirement after surgery within 1 year) on the other hand. It demonstrates that surgical adverse effects and psychiatric comorbidity are associated with retirement and failure to return to the preoperative level of activity. With respect to headache, only the subgroup of patients with initial good surgical outcome (GOS 4–5) shows a correlation between retirement and the occurrence of headache.

Depiction of the correlations between comorbidity, surgery and postoperative headache, retirement and failure to return to the preoperative level of activity as demonstrated in Table 4. Although no causative coherence can be drawn from the data, postoperative headache and the loss of activity are central consequences in addition to postoperative retirement. The solid lines indicate significant correlations. The dotted line indicates a tendency (P = 0.052) between postoperative headache and retirement, which is significant after analysis of the subgroup with Glasgow outcome score 4 and 5.
Characteristics
Five distinct headache syndromes could be identified based on the following characteristics: location, character, radiation of the pain, additional symptoms and treatment (Table 5). Most frequently [14 out of 30 patients with headache (46.7%)], a tension-type-like holocephalic headache was found of dull or drilling character, in two cases worse than 7/10 and responding well to over-the-counter pain medication. Pain-free intervals and the duration of attacks varied.
Five headache entities could be identified according to the characteristics of the pain (left half); the right half of the table lists the criteria of the headache syndromes in the International Classification of Headache Disorders, 2nd edn, (ICHD-II) that were most similar to the respective postoperative headache

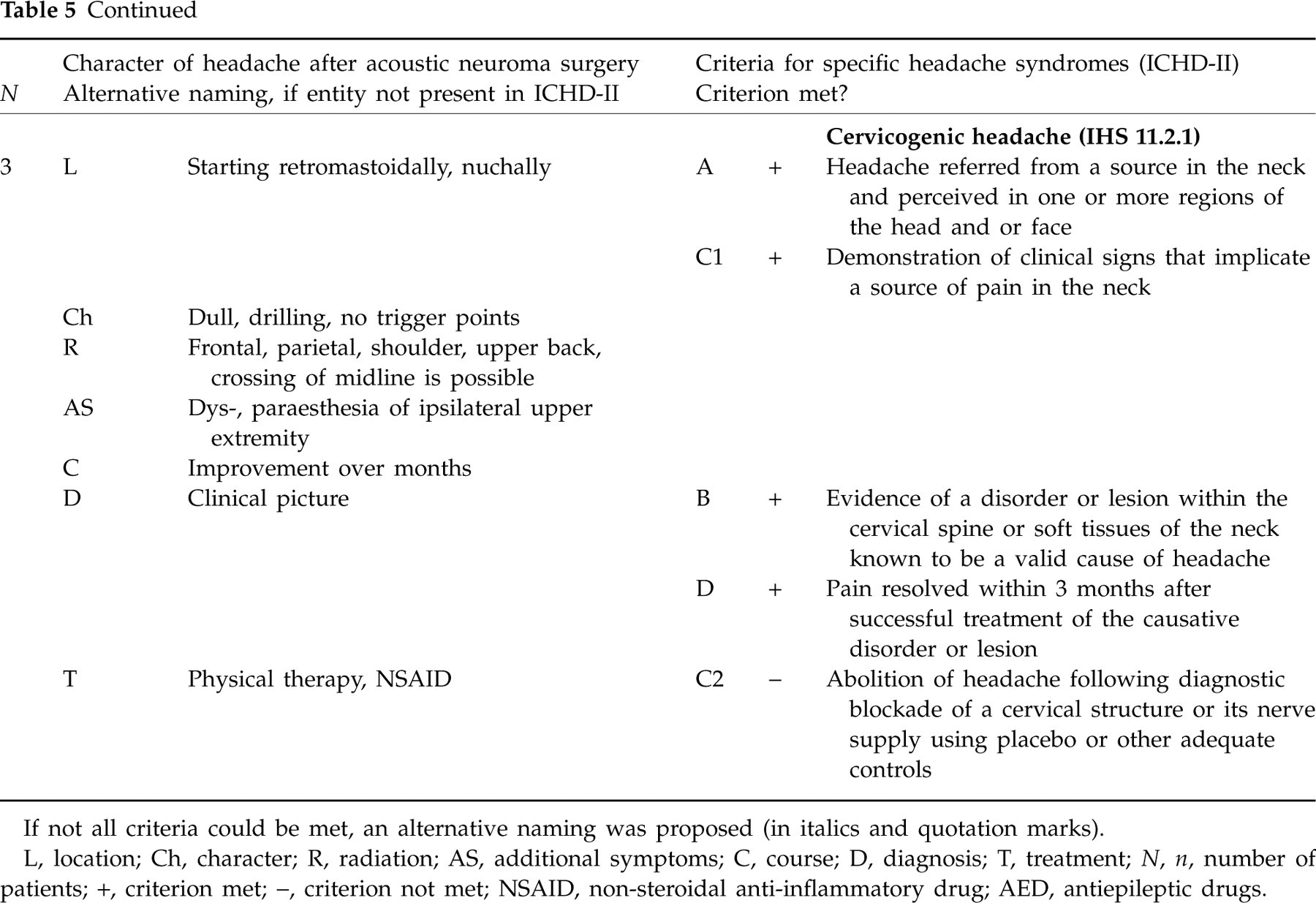
If not all criteria could be met, an alternative naming was proposed (in italics and quotation marks).
L, location; Ch, character; R, radiation; AS, additional symptoms; C, course; D, diagnosis; T, treatment; N, n, number of patients; +, criterion met; −, criterion not met; NSAID, non-steroidal anti-inflammatory drug; AED, antiepileptic drugs.
In five cases (16.6%) a paroxysmal stabbing pain starting from behind the mastoid and radiating cranially without crossing the midline was found with concomitant hypaesthesia of the respective skin region. The pain could be triggered by wound contact or head movement. It responded to a local anaesthetic block but not to oral anti-pain medication, including various antiepileptics such as carbamazepine. The patients reported that the pain tended to lose its neuropathic character and to become more and more permanent, dull and drilling.
Five other patients complained about neuropathic facial pain in the area innervated by the trigeminal nerve with V1 affected in one and V3 in four patients. The pain was dull, drilling and of moderate to severe intensity (< 8/10). Its duration was variable. A neuralgic character could not be documented. Dysgeusia and hypaesthesia were present in 80% and 100%, respectively. Some spontaneous relief was noticed within the year of study by three patients.
Neuropathic pain in the external acoustic meatus with radiation to the infra- and preauricular skin was present in three cases. Two of these also noticed sicca syndrome and dysgeusia. Treatment with antiepileptics and non-opioid analgetics was not successful. No trigger mechanism could be found. During the year of observation, pain-free intervals shortened, indicating a tendency to chronification, often associated with a depressive mood.
Three patients suffered from the fifth headache syndrome with a dull and drilling pain, starting in the neck and radiating cranially and to the ipsilateral shoulder and proximal upper extremity. The distribution of the pain did not correspond to a nerve root or peripheral nerve. It was accompanied regularly by an alteration of posture to achieve amelioration and by subsequent elevation of the muscle tone with a reduction in the range of neck movement. A specific trigger mechanism could not be described. However, physical or psychological stress was regularly associated with the occurrence of the pain. Non-opioid pain medication and physical therapy were found to be effective.
Headache syndromes and diagnostic criteria in the ICHD-II
Table 5 shows the categorization of the headache syndromes according to the ICHD-II (6). Criteria for neuralgia of the occipital nerve [International Headache Society (IHS) 13.8] and cervicogenic headache (IHS 11.2.1) were met. The remaining three syndromes were similar to tension-type headache (IHS 2), trigeminal neuralgia (IHS 13.1) and nervus intermedius neuralgia (IHS 13.3). However, due to the markedly higher intensity, ‘tension-type-like headache’ would be a better description of the first syndrome. The presence of a neuropathic pain component in the latter two syndromes and the missing neuralgic character with its paroxysmal stabbing pain and the presence of trigger factors would support naming these two syndromes ‘neuropathy of the trigeminal nerve’ and ‘neuropathy of the intermedian nerve’, respectively.
Discussion
Implications of headache for private and vocational activity
In recent years, AN surgery has become a routine procedure with improved results related to hearing and facial preservation and, subsequently, with good quality of life after surgery (11). In our study, short-term surgical outcome, assessed by GOS, was satisfactory in 89% (GOS 5 and 4), and was, as expected, correlated with the ability to return to work. The subjective failure to return to preoperative levels of activity was, together with the number of intra-operative complications, associated with postoperative retirement. This ability to resume daily activities was independent of the occurrence of hearing problems, in contrast to ataxia, dysgeusia and headache (as well as a tendency to facial paresis), although the former was the most relevant problem for the patients according to the literature (11–14). In these reports, headache is mainly ranked fourth of the problems after surgery (in 10.5–22%) behind hearing loss or tinnitus (in 25.8–61.3%), balance problems and facial paresis. In accordance with our data, a study on self-assessed quality of life using SF-36 has demonstrated, however, that only headache, and not age, sex, hearing or facial function after surgery, was associated with lower scores in any category (physical role limitations and bodily pain) (15). Headache and facial problems were furthermore the main reason for continuous medical consultation in about one-third of patients after surgery (12). As in our study with 75.2% of patients being able to return to their preoperative level of activity, Tos et al. (16) found that, socioeconomically seen, about four-fifths of patients suffering from AN were able to resume their daily activities irrespective of the strategy used (operation vs. observation). Ryzenman et al. (4) have stated that work ability was not affected in about 50% of patients after surgery, whereas 18% complained about substantial impairment.
The occurrence of headache after acoustic neuroma surgery
Headache is a common symptom after resection of AN. The literature reports a prevalence ranging from 0% (17) to 75% (1) depending on the time interval between operation and survey and the type of operation. In general, a low but variable frequency of headache is described if a translabyrinthine rather than occipital approach is used (0% in (17), 22% in (12), 53% in (3)). In one report, this difference was not present any more in a 1-year follow-up (18). Performance of an osteoplastic suboccipital craniotomy (19, 20) (but not in (21)) and avoidance of intradural drilling (22) also resulted in a reduction of post-surgery headache. Not surprisingly, postoperative headache was found to be more frequent if the investigation took place early (31% in (23), 61% in (24), 23% in (2), 54% in (25)) after surgery rather than late (4% after 2 years in (23), 6% after 1 year in (26), 27% after 1 year in (25), 16% after one and 9% after 2 years in (2)). Aside from some studies comparing different surgical techniques (19), incidence studies on postoperative headache suffer from a retrospective study design. In our prospective study, all patients were operated using a suboccipital approach and 32% experienced a headache of at least 6/10 on the NAS for > 6 months. A positive history of preoperative headache was a risk factor for the occurrence of headache after surgery. This correlates with results published by Levo et al. (24), but contradicts data collected by Mosek et al. (27). Our finding is in accordance with studies describing a pre-existing primary headache as the main risk factor for secondary headache due to brain tumour (28, 29) or lumbar puncture (30), raising the question of an overlap of the pathophysiological mechanisms involved in primary and secondary headaches. To the best of our knowledge, the correlation of postoperative headache with the number of intra-operative complications, but not the number of operative revisions, is presented here for the first time. Its significance remains unclear. However, we speculate that the mechanism of headache induction by posterior fossa surgery is the first, greatest trauma during an operation in a patient with susceptibility to headache. A second trauma by a revisional operation would thus not constitute a significant additional factor for the occurrence of headache. The failure to return to preoperative levels of activity and the occurrence of postoperative headache were significantly correlated with each other. The number of complications is significantly associated with the long-term consequences of postoperative retirement and the failure to return to the preoperative level of activity.
The correlations visualized in Fig. 1 do not account for a causative relationship, however. In our speculative interpretation, postoperative reduction of physical activity, one of the main non-pharmacological approaches for prevention of headache (31, 32), might result in increased susceptibility to headache. This is supported by the finding that the failure to return to preoperative levels of activity (not psychiatric comorbidity) is the only postoperative parameter that correlates with postoperative headache. Failure to return to preoperative levels of activity is additionally associated with psychiatric comorbidity. The impact of headache after AN surgery on quality of life is demonstrated by the finding that headache is significantly associated with the probability of retirement in the subgroup with good recovery/moderate disability (GOS 5 and 4).
Headache entities
In contrast to prevalence and risk factors, only scant information is found in the literature on the clinical manifestation of headache after AN surgery. Early studies have described the pain most often as tension-type-like (2, 3) with a dull aching or pressure quality (27), with an additional neuralgic or vascular component (1). Ryzenman et al. (4) also found a moderate intensity with frequent episodes occurring daily and lasting 1–4 h. Others describe severe, short-lasting attacks provoked by stress, and a subgroup with headache meeting the IHS criteria (6) for tension-type headache (5/89) and migraine with (n = 3) or without (n = 12) aura (5). To the best of our knowledge, the attempt to categorize all secondary post-surgery headache types according to the classification of the IHS is presented here for the first time.
Most frequently, a tension-type-like headache syndrome was found, differing from tension-type headache by its more severe intensity. Less common were headache syndromes meeting the criteria for neuralgia of the occipital nerve and cervicogenic headache and most probably the criteria for trigeminal neuralgia (‘neuropathy of the trigeminal nerve’) and nervus intermedius neuralgia (‘neuropathy of the intermedian nerve’). We speculate that the differences in these headache entities are of importance for the management of patients. As shown, patients with the tension-type-like or cervicogenic headache responded well to treatment with non-steroidal anti-inflammatory drugs (NSAIDs) and physical therapy. In accordance with neuralgia of the occipital nerve (IHS 13.8), pain could be temporarily eased by local anaesthetic block. A tendency to transformation of the neuralgic character to a dull and drilling permanent pain was found. Neuropathy of the trigeminal nerve—differing from classic trigeminal neuralgia by the lack of trigger areas and pain paroxysms of stabbing pain—showed spontaneous amelioration in 60%, but without responding to treatment with antiepileptic drugs. The neuropathic pain in the area of the intermedian nerve was also not responsive to treatment with NSAIDs or antiepileptic drugs and showed a worse prognosis if chronification occurred, with shortening of the pain-free intervals and development of a depressive mood disorder. In summary, treatment was initially mainly based on the clinical picture and followed the corresponding headache syndrome of the IHS. This was successful particularly in the case of tension-type-like headache, cervicogenic headache and neuralgia of the occipital nerve, but unfortunately less useful for neuropathies of the trigeminal and intermedian nerve.
Based on the differences in the clinical picture, the existence of different pathophysiological mechanisms has to be discussed.
Cervicogenic headache
At least three pathophysiological mechanisms could be considered for cervicogenic headache in our patients. Surgery of the posterior fossa, including incision of skin, muscles and dura mater, might result in irritation of sensory neurons of the upper three cervical spinal nerves. These are thought to converge with trigeminal afferents, resulting in the perception of headache (trigeminal nerve) by irritation of cervical spinal nerves (33). This would be supported by the efficacy of a local diagnostic blockade which, however, was not necessary in our patients due to good pain control by physical therapy and NSAIDs. Alternatively, posterior fossa surgery might result in connective tissue bridges between the dura and bone or muscle depending on the surgical procedure, with irritation of trigeminal afferents on posture or head movement (34). It could be speculated that headache thus might be reduced by insertion of bone or similar material between the muscle and the dura or by performing duraplastic instead of direct dura closure (to prevent dural tension). The third mechanism might simply be the result of an upper cervical spine degenerative disease and aggravation of the symptoms due to head position during surgery.
Neuralgia of the occipital nerve
Although the exact pathophysiology of occipital neuralgia is unclear, we speculate that direct compression of the occipital nerve by scars or connective tissue or the development of post-traumatic scar neuroma may induce segmental demyelination of the nerve with expression of sodium channels that becomes spontaneously active, as has also been discussed for trigeminal neuralgia (35). The ineffectiveness of treatment with carbamazepine remains unexplained. As the patients were followed postoperatively outside of our clinic, low dosage of the drug or inconsistent treatment cannot be ruled out.
Neuropathy of the trigeminal or intermedian nerve
Neuropathic pain is defined as pain after nerve injury and characterized by pain in the absence of a stimulus or caused by normally innocuous stimuli due to a reduced nociceptive threshold (e.g. (36)). The dull, drilling pain in the region supplied by the intermedian nerve (external acoustic meatus) or branches of the trigeminal nerve (V1, V3) indicates that the corresponding nerve was affected during surgery. The exact causative event remains uncertain: the intermedian nerve might be irritated during removal of the tumour with drilling of the internal acoustic meatus, the trigeminal nerve during mobilization of the tumour.
Tension-type-like headache
Tension-type headache in its episodic form is the most prevalent type of headache (37). A combination of genetic (38), endo- and paracrine (39), vascular (40), muscular (37, 41) and central mechanisms (37, 42) has been discussed for the pathophysiology of primary tension-type headache. The actual mechanism remains unclear. The symptomatic tension-type-like headache of our patients is probably due to the manipulation or removal of structures in the posterior fossa. This would be supported by the finding that the retrosigmoid approach results more often in headache than the translabyrinthine one (24). Schaller and Baumann (21) speculate about aseptic meningitis caused by fibrin glue used for dura closure or intradural drilling of the posterior aspect of the internal acoustic meatus. The latter was shown to be associated with a higher frequency of postoperative headache (22). Catalano et al. (43) furthermore found that residue trapping of free circulating bone dust results in significant reduction of headache, possibly preventing aseptic meningitis. Furthermore, Levo et al. (24) have shown that a postoperative gait problem was a risk factor for headache. Our data could not confirm this (no correlation of headache with ataxia) in accordance with another study by Levo et al. (44), who could detect no influence of vestibular function on the occurrence of headache after AN surgery.
Conclusion
Outcome after surgery for AN is generally very satisfactory, with most patients being able to live independently. In this study, we have characterized headache after AN surgery further: headache prevalence in our prospective study was 32% and possible risk factors were preoperatively pre-existing headache and the number of perioperative adverse effects. The occurrence of post-craniotomy headache and the failure of patients to return to their preoperative level of activity were furthermore associated with each other. They were significantly correlated with the risk of postoperative retirement, thus indicating an important socioeconomic impact of headache in these patients. In addition to the known similarity of post-craniotomy headache with tension-type headache, our attempt to categorize the headache of each patient according to the IHS classification resulted in the construction of four other headache syndromes with individual pathophysiological mechanisms and therapeutic consequences.
Footnotes
Acknowledgements
We thank Ms K. Ogston for her help in preparing the manuscript and Mrs S. Ehrentraut for statistical analysis. The study was supported by a grant of the BMBF (Chronic headache, project D1), and the Förderprogramm für Forschung und Lehre (FöFoLe, reg.-no. 561) of the University of Munich.