
Abstract
The aim of this pilot study was to add weight to a hypothesis according to which patients presenting with chronic neck pain could have a predisposition towards respiratory dysfunction. Twelve patients with chronic neck pain and 12 matched controls participated in this study. Spirometric values, maximal static pressures, forward head posture and functional tests were examined in all subjects. According to the results, chronic neck patients presented with a statistically significant decreased maximal voluntary ventilation (P = 0.042) and respiratory muscle strength (Pimax and Pemax), (P = 0.001 and P = 0.002, respectively). Furthermore, the current study demonstrated a strong association between an increased forward head posture and decreased respiratory muscle strength in neck pateits. The connection of neck pain and respiratory function could be an important consideration in relation to patient assessment, rehabilitation and consumption of pharmacological agents.
Keywords
Introduction
Neck pain is considered to be one of the most costly musculoskeletal problems with tremendous impact on health and quality of life of the individual and on society as a whole. Although chronic neck pain syndrome has received considerable clinical research attention, many different relevant aspects of its consequences are still under investigation. Previous research on chronic neck pain syndrome has demonstrated the existence of: (i) decreased strength of deep neck flexors and extensors (1–6), (ii) hyperactivity and increased fatigability of superficial neck flexors (especially sternocleidomastoids and anterior scalene) (7–11), (iii) limitation of range of motion (12–16), (iv) increased forward head position (FHP) (17–20), (v) decrease in proprioception and neuromuscular disturbances (21, 22), (vi) existence of pain, and (vii) psychosocial dysfunction (23–27). According to a hypothesis previously published by Kapreli et al. (28), patients presenting with some or all of these factors associated with chronic neck pain could have a predisposition towards respiratory dysfunction. This disclosure presents a totally different and previously unreported feature of chronic neck pain syndrome (28).
Perry et al. (29) examined the existence of a correlation between faulty breathing and musculoskeletal pain patterns. Abdominal and chest breathing was assessed by observation only, and results showed that 83% of patients with neck pain, in a population of different chronic musculoskeletal pain syndromes, experienced a changed breathing pattern indicating a relationship between neck pain and respiration. No other research has examined this relationship, and urgent research is required to explore and add weight to the hypothesis of Kapreli et al. (28). Therefore, the aim of the present pilot study was to investigate the effects of chronic neck pain on respiratory function. In particular, consideration was given to spirometric measures and assessment of respiratory muscle strength in these patients. A further aim was to examine whether an alteration of normal cervical posture such as FHP, commonly found in chronic neck patients, could correlate with respiratory dysfunction.
Methods
Subjects
Twelve patients (five male, seven female) with chronic neck pain and 12 healthy subjects (five male, seven female) participated in this study. Subjects in the control group were individually matched to the patients for age, height, weight and activity level. The Baecke Questionnaire was used to assess the activity level of subjects in both groups (30, 31). The selected subjects were invited to participate on the basis of written informed consent, approved in accordance with the requirements of the Ethical Committee of TEI Lamias, Department of Physiotherapy, Greece. Patients were included if they had a history of neck pain with or without headache for ≥ 6 months that was associated with cervical joint dysfunction and experienced incidence of pain at least once a week. Subjects were excluded if they had undergone cervical spine, abdominal or chest surgery, had participated in a neck exercise programme in the past 12 months, were cigarette smokers or tobacco chewers, had any occupational industrial exposure, were obese (body mass index > 40), had clinical abnormalities of the vertebral column or thoracic cage, neuromuscular diseases, known cases of gross anaemia, diabetes mellitus, pulmonary tuberculosis, bronchial asthma, chronic bronchitis, bronchiectasis, emphysema or malignancy.
The cervical spine was examined by a trained physiotherapist to confirm the presence of cervical segmental pain and dysfunction (32). The Neck Disability Index (NDI) (33) (score out of 50) was used to measure the subject's perceived disability resulting from their neck pain. Furthermore, patients indicated their average weekly intensity of neck pain and their intensity of neck pain on the day of examination on a 10-cm visual analogue scale anchored on ‘no pain’ and ‘the worst possible pain imaginable’ (34).
Spirometry
Spirometry was performed on an electronic Spirometer (Spirolab II; SDI Diagnostics Inc., Easton, MA, USA). All pulmonary function tests were carried out at a fixed time of the day (09:00–13:00 h) to minimize diurnal variation (35). The apparatus was calibrated daily and operated within the ambient temperature range of 20–25 °C. The precise technique in executing various lung function tests for the present study was based on the operation manual of the instrument with special reference to the official statement of the American Thoracic Society of Standardization of Spirometry (36). After taking a detailed history and anthropometric data, subjects were informed about the whole manoeuvre. They were encouraged to practise this manoeuvre before doing the pulmonary function test. The test was performed with the subject in the sitting position using a nose clip. The test was repeated three times after a 3-min rest, and results were obtained from the Spirometer. These parameters were forced vital capacity (FVC), vital capacity (VC), peak expiratory flow, forced expiratory volume in 1 s (FEV1), forced expiratory ratio (FEV1/ FVC), forced expiratory flow (FEF25–75%; FEF25%, FEF50%, FEF75%) and maximum voluntary ventilation (MVV).
Maximal static respiratory pressures
Maximal inspiratory pressure (Pimax) and maximal expiratory pressure (Pemax) were measured in random order to avoid the measurement order effect. They were both obtained from residual volume (RV) and total lung capacity (TLC), with the subjects seated wearing nose clips and with a rigid, plastic flanged mouthpiece in place. Pimax is the maximal negative pressure measured at the mouth after complete exhalation to RV followed by a single sustained maximal inspiratory effort from that lung volume against an occluded airway. Pemax is the maximal positive pressure measured at the mouth after inhalation to TLC followed by a maximal expiratory effort from that lung volume against an occluded airway. These measurements reflect the strength of the inspiratory and expiratory muscles, respectively (37).
Pimax and Pemax were measured using a digital mouth pressure meter (±300 cm H2O) (Micro RPM®; Micro Medical, Chatham, UK). A tube containing a unidirectional valve and a small air leak was coupled to a rigid mouthpiece. During the test, the individual remained seated with the nasal airflow impeded by a nose clip. The measurements were made by the examiner, who always explained and demonstrated the correct manoeuvre. Subjects performed five maximal manoeuvres, with an interval of 1 min, where the recorded value was taken as the highest value.
Forward head posture
For FHP assessment, a digital picture of the lateral view of each subject was taken (38, 39). All subjects were asked to sit comfortably on a high-backed chair with both feet flat on the floor, hips and knees positioned at 90° angles, and buttocks positioned against the back of the chair. They were requested to rest their hands on their laps, and to keep their shoulders against the back of the chair. They were also instructed to focus visually on a point directly ahead on the wall of the room. The visual focal point was confirmed by the examiner after subjects had assumed their comfortable sitting position. This minimized the tendency towards flexion or extension of the neck while maintaining a relaxed head position. The base of the camera was set at the height of the subject's shoulder. The tragus of the ear was clearly marked, and a plastic pointer was stuck onto the skin overlying the spinous process of the seventh cervical vertebra (C7). Once the picture was obtained, the angle between the horizontal line passing through C7 and the line extending from the tragus of the ear to C7 (cranio-vertebral angle) (38, 39) was calculated with the 3D drawing program (Auto-CAD 2000; Autodesk Inc., San Raphael, CA, USA) (Fig. 1). Raine and Twomey have reported the reliability of this procedure as high (intraclass correlation coefficient = 0.88) (39).
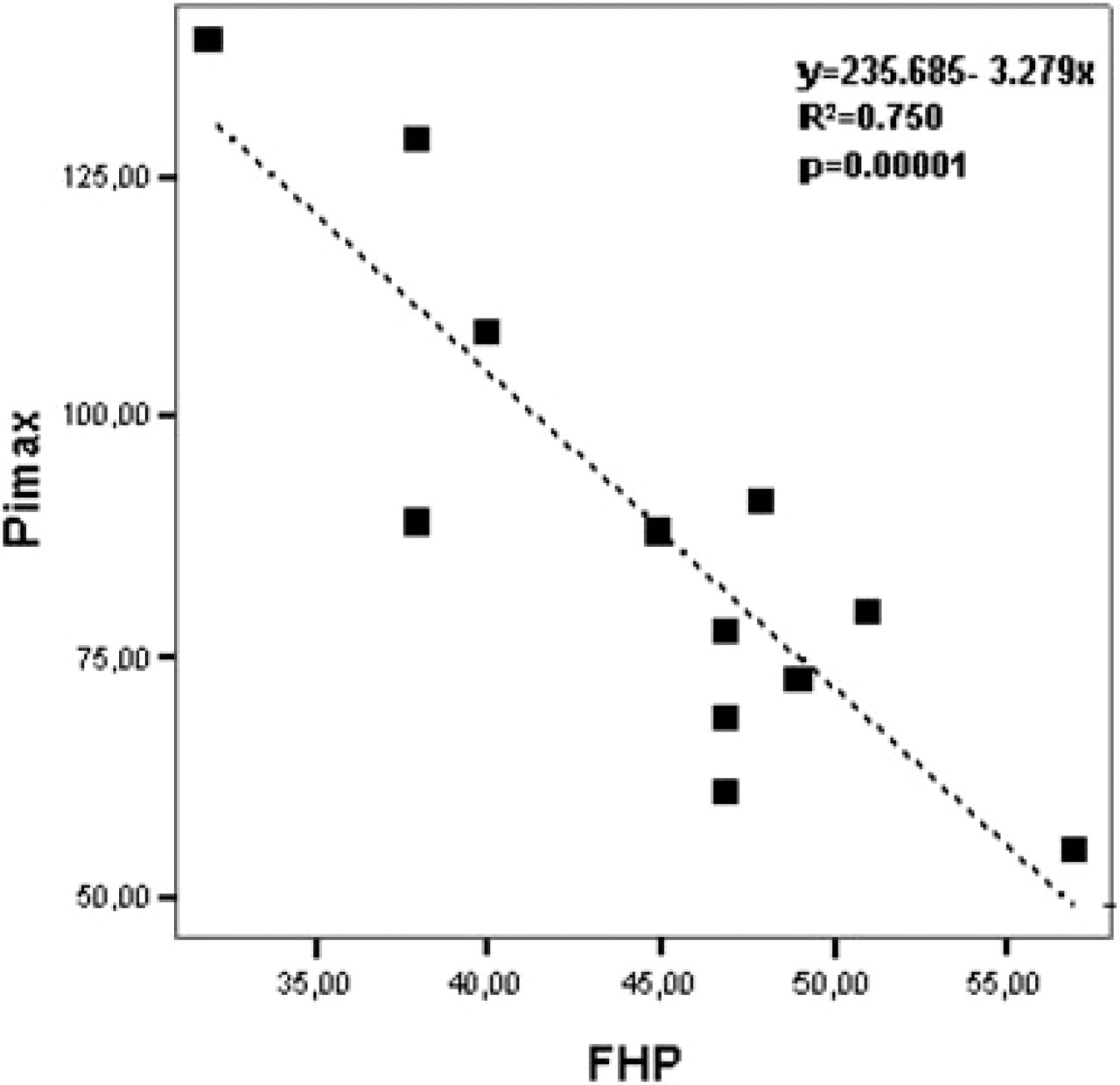
Regression analysis for individual differences in maximal inspiratory pressure (Pimax) between neck pain patients against forward head position (FHP). A significant negative correlation was found, indicating that increased FHP decreased Pimax.
Statistical analysis
All data were normally distributed (Kolmogorov–Smirnov test); therefore, parametric tests were employed for analysing the results. Differences in all variables between both study groups were assessed with paired Student's t-test. In addition, the effect size (r) was calculated and reported (40). The pulmonary function data were correlated against the FHP. Linear regression was applied on this correlation and the equation y = mx + c was derived with the correlation coefficient (r), where ‘y’ means pulmonary function value, ‘x’ indicates FHP and ‘c’ is a constant. For all comparisons, a level of P < 0.05 was considered to be statistically significant. The analysis was performed with
Results
Homogeneity was found between the two groups concerning anthropometric characteristics (age, height, weight) and activity level (Table 1). Patients were aged 18–47 years (mean 29.42,
Anthropometric and respiratory function values between neck pain patients and their matched controls

FHP, forward head position; FVC, forced vital capacity; FEV1, forced expiratory volume in 1 s; FEF, forced expiratory flow; PEF, peak expiratory flow; VC, vital capacity; MVV, maximum voluntary ventilation; Pimax, maximal inspiratory pressure; Pemax, maximal expiratory pressure.
Pulmonary function parameters of the patients and controls are compared in Table 2. Neck pain patients demonstrated a significant reduction in MVV (P < 0.05), Pimax (P = 0.01) and Pemax (P < 0.05) in comparison with controls. More precisely, neck pain patients were found to have a mean reduction of 14% in MVV, 21.4% in Pimax and 16.5% in Pemax (Table 1) compared with controls. In addition, regression analysis for Pimax and Pemax showed significant negative correlation with FHP, indicating that increased FHP may be associated with these lung function parameters in neck pain patients (Figs 1 and 2).
Paired samples t-test
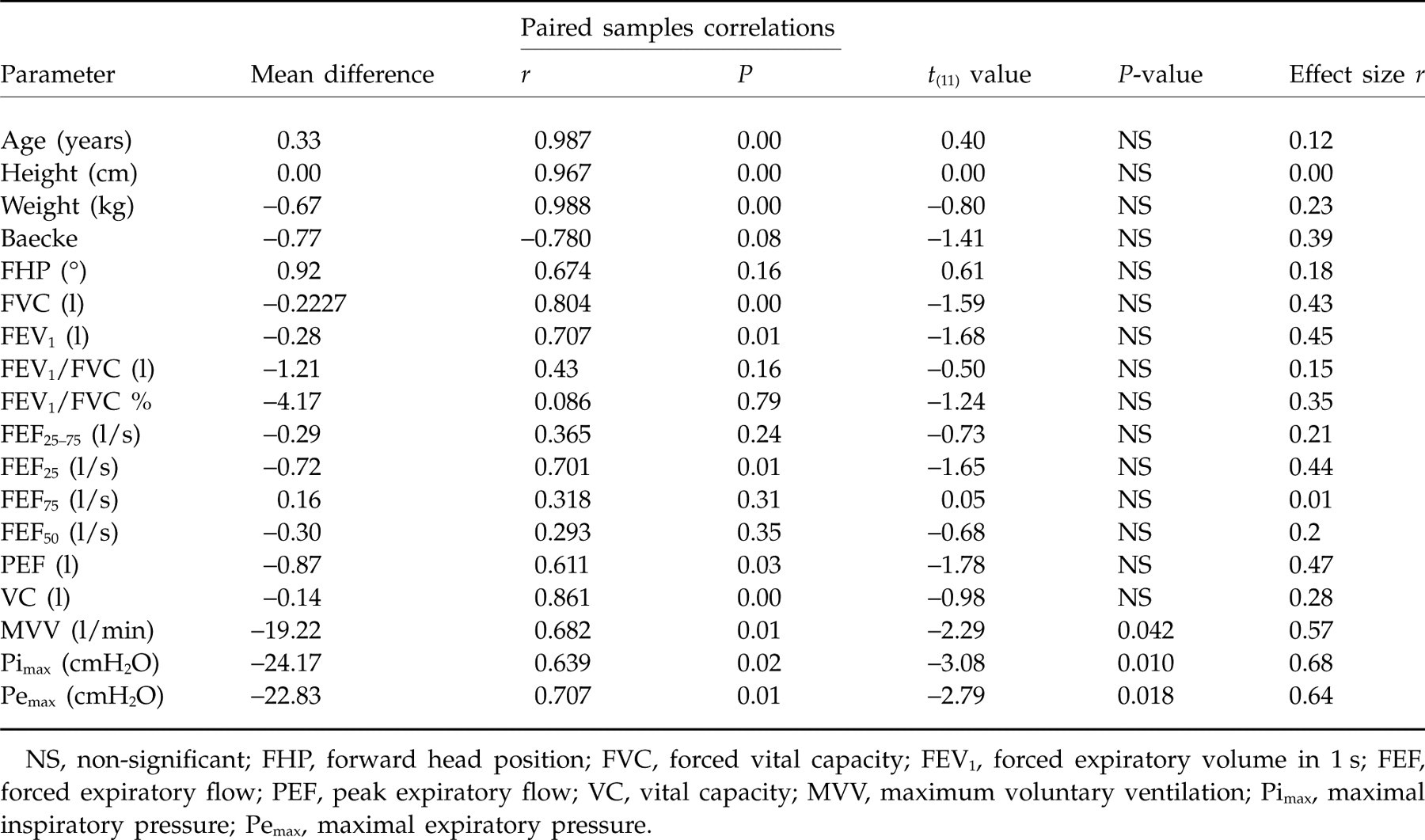
NS, non-significant; FHP, forward head position; FVC, forced vital capacity; FEV1, forced expiratory volume in 1 s; FEF, forced expiratory flow; PEF, peak expiratory flow; VC, vital capacity; MVV, maximum voluntary ventilation; Pimax, maximal inspiratory pressure; Pemax, maximal expiratory pressure.

Regression analysis for individual differences in maximal expiratory pressure (Pemax) between neck pain patients against forward head position (FHP). A significant negative correlation was found, indicating that increased FHP decreased Pemax.
Discussion
According to the present results, chronic neck patients present with a respiration dysfunction attributed to decreased MVV and respiratory muscle strength (Pimax and Pemax). Furthermore, the current study has demonstrated a strong association between increased FHP and decreased respiratory muscle strength in neck pain patients. These findings seem to support the hypothesis that a common disorder like chronic neck pain syndrome can present with problems beyond the musculoskeletal. It seems that this kind of pathology has further implications, closely correlated with the respiratory system (28).
In the current study, a statistically significant deterioration of MVV, Pimax and Pemax was found in neck patients. Maximum static respiratory pressures (Pimax and Pemax) and MVV are considered to be the most sensitive indices of respiratory muscle weakness, with MVV being a sensitive indicator of neuromuscular disorders. Those pulmonary function parameters have been found to be decreased in chronic neuromuscular diseases such as Parkinson's disease (41, 42) or multiple sclerosis (43, 44). It is believed that significant and great impairment in MVV could indicate impaired performance of repetitive respiratory motor acts as a result of bradykinesia and rigidity of the respiratory muscles (45). The reduction of those parameters in neck patients in comparison with healthy controls could be ascribed to the connection that exists between neck pathology and respiratory muscles, supporting the hypothesis.
On the other hand, there was no evidence from the results of this study of any other significant alterations in spirometric values in neck patients. In patients with neuromuscular diseases, the most regularly noted abnormality of lung volumes is a reduction in VC. The pattern of abnormality of other subdivisions of lung volume is considered to be less consistent. RV is usually unchanged or increased, the latter particularly with marked expiratory weakness. As a result, TLC is less noticeably reduced than VC, and the RV/TLC and functional residual capacity/TLC ratios are often increased without necessarily implying airway obstruction (37, 46) Even airway resistance has been found to be normal in mild respiratory muscle weakness (47), whereas the airway function may appear to be even supernormal when volume-corrected indices such as FEV/VC or specific airway conductance are used (37).
Nevertheless, the neck patients of the present study did not differ in VC with healthy subjects. This finding could be attributed to the following reasons. It is believed that VC is less sensitive than maximum respiratory pressures in mild respiratory muscle weakness (37). Furthermore, VC has shown a marked fall mainly in supine compared with erect posture, especially in patients with isolated or disproportionate bilateral diaphragmatic weakness or paralysis (48). In case of neck patients, with no apparent respiratory symptoms or diaphragmatic weakness, VC is not probably subject to change. However further research with a larger sample size is needed in order to investigate the respiratory pattern in chronic neck patients, in detail, using subgroup analysis or other outcome measures (e.g. plethysmography or arterial blood gases).
The connection that exists between chronic neck pain syndrome and respiratory dysfunction, found in the present study, could be explained by a multifunctional model (Fig. 3). According to previous research, chronic neck pain patients present with decreased strength of deep neck flexors and extensors (1–6), hyperactivity and increased fatigability of superficial neck flexors (especially sternocleidomastoids and anterior scalene) (7–11), and limitation of cervical range of motion (12–16). These functional alterations can cause biomechanical modifications in the thoracic spine and consequently on respiratory muscle function (28).

Neck pain and respiratory dysfunction (with permission) (Kapreli et al., 2008) (28).
The deep flexors and extensors of the cervical spine, although they do not play a direct role in respiration, are important dynamic elements for correct posture, muscle balance and segmental stability. Known as ‘active ligaments’ (49), these muscles could have an impact on kinetic control, not only on the specific area but also on articulations related to it such as in the shoulder or thoracic spine (50). During respiration, there is a need for stability within the cervical and thoracic spine in order for the muscles to act in moving the ribs up or down. Poor cervical muscle control and restricted range of motion could present with mechanical adjustments and adapted contraction patterns, due to the alteration in the muscles' force–length curve relationship, thereby altering movement of the rib cage. This could lead to insufficient respiratory function, including all muscles involved such as diaphragmatic, intercostals or abdominals (28) (Fig. 3).
Furthermore, although sternocleidomastoids and scalene used to be considered as accessory respiratory muscles, their respiratory role has recently proved to be essential (51), influencing dorsoventral rib diameter and lung volume (52). It is further believed that the topographic neural drive distribution among the intercostals during breathing is influenced by the inspiratory mechanical advantage that is subject to sternocleidomastoids and anterior scalene contraction (53). In the case of increased fatigability such as in neck pain patients, those muscles could either influence the respiration directly (especially inspiration) or indirectly, due to alterations in the functional length and recruitment, causing a change in rib cage mechanics (28) (Fig. 3). The above-mentioned elements provide an explanation for limited respiratory strength in chronic neck patients described through a biomechanical model.
Although, the cranio-vertebral angle did not differ between the two groups (patients 44.92°, controls 44°), surprisingly, respiratory muscle strength (Pimax and Pemax) showed significantly negative correlation with FHP in neck pain patients not in the control group. There are some possible explanations for these results. First, this finding could highlight the importance of the neurophysiological component in the explanatory model used to support the hypothesis against the forthright biomechanical component, a feature that will be interesting to explore in a future study. In addition, sitting vs. standing measurement for FHP may be another explanatory element. Fernández-de-las-Peñas et al. (18) have reported different cranio-vertebral angle values between neck patients and healthy subjects in the two positions, yielding statistically significant differences in the standing but not the sitting position. In the present study, all measurements were conducted in the sitting position, resulting in no differences for FHP between the two groups. In a future study, it may be valuable to include both positions for measuring FHP, as it seems this may influence the results. Lastly, the relatively small number of subjects in this pilot study is another factor that could explain these results. This could be solved in a future study by increasing the number of subjects.
Several studies have suggested that deficit in proprioception (21, 22) in chronic neck pain patients is another feature that contributes to dysfunction. The impairment of proprioception in patients with neck pain could lead to differentiated ascending afferent impulses towards the central nervous system (CNS), reorganization of cortical and subcortical regions of CNS and consequently decreased or altered activation of muscles described as arthrogenous joint de-efferentation (54). As a result, it could contribute to functional decline because of altered motor patterns causing rib cage mechanical alterations and respiratory dysfunction (55, 56) (Fig. 3). MVV is considered to be an indicator of neuromuscular control (37), and its limitation in neck patients may imply further interference of the nervous system. In the current study, MVV was found to be decreased in neck patients in comparison with controls, supporting the previously published hypothesis by Kapreli et al. (28).
Chronic neck patients, according to previous research, also present pain that can further support the examined hypothesis (28). Pain could lead to respiratory disturbances through the following two mechanisms. First, research has shown that acute pain results in an increase in minute ventilation (57) as noxious stimulation modulates the ventilatory control system, boosting respiratory drive. Furthermore, chronic pain seems to lead not only to hyperventilation, but also to long-term blood chemistry compensation similar to that experienced by chronic respiratory patients (58). Second, the pharmacological treatment (analgesics and anti-inflammatory drugs) that patients with neck pain follow has depressant effects on respiration (59). Both stimulatory effects of pain and the depressant effects of the agents may constitute factors sufficient to influence respiration by means of biochemical mechanisms, as they might have an impact on pH balance, resulting in alkalosis or acidosis (Fig. 3). The patients of the current study indicated that they had slight to moderate pain at least once a week, as that was a criterion for subjects' recruitment. Furthermore, all patients admitted that they were occasionally taking analgesics or anti-inflammatory drugs as a result of their pain and disability. Although there was no deterioration in lung volumes in neck pain patients, it might be useful in future to measure blood gases and record analgesics intake.
Finally, chronic neck pain patients frequently present with psychosocial symptoms as a result of their pathology (23–26). Research has shown that anxiety may have an influence on ventilation inducing hyperventilation and respiratory instability (27), resulting in accompanying biomechanical alterations. Additionally, kinesiophobia and depression could result in changes in physiological movement execution, resulting in limitation of cervical range of motion, consequent alterations in strength and resultant modified breathing pattern (28). Psychosocial symptoms were not examined in the current study, but may be important considerations in future research.
The present study had a number of limitations. A first limitation was the restricted number of examined subjects. However, even with this small number of subjects, effect sizes ranged from 0.57 to 0.68, for the statistically significant comparisons, sizes that are considered to represent a very large effect (it is > 0.5 the threshold for a large effect) (40). However, further research should be done using a larger number of subjects in order to have adequate statistical power in all parameters under investigation. Another limitation was the inability to find explanatory factors for the detected respiratory dysfunction, as the limited number of patients could not provide adequate sample size for further categorization. This could be solved in a future study by increasing the number of subjects and adding more outcomes (such as psychosocial examination, analgesic intake, etc.).
Finally, it could be argued that the deterioration of respiratory muscle strength in neck patients might be attributed to their general deconditioning rather than having a specific relationship to neck pain. However, it is difficult to attribute this decrease in respiratory muscle strength to general deconditioning of neck patients, as no statistically significant differences in Baecke scores (activity level) between the two groups were found. However, it will be an interesting feature to include a third comparator group (e.g. knee osteoarthritis) in the methodology of a future study, in order to examine this issue further.
In conclusion, in the current study chronic neck patients presented a respiration dysfunction attributed to deteriorated MVV and decreased respiratory muscle strength (Pimax and Pemax). Furthermore, the present study has demonstrated a strong association between increased FHP and decreased respiratory muscle strength in neck patients, providing evidence that the altered biomechanics in the cervico-thoracic area as well as changes in muscle force–length relationship are important factors that determine respiratory performance. These findings support the hypothesis previously published by Kapreli et al. (28) that a common musculoskeletal disorder like chronic neck pain syndrome may cause respiratory dysfunction. The connection of neck pain and respiratory operation could have a great impact on various clinical aspects, notably patient assessment, rehabilitation and consumption of pharmacological agents, and further research should therefore be performed.
Footnotes
Acknowledgements
We gratefully acknowledge the help from all the volunteers. We would like also to thank Dr Papachristos Athanasios, MD, for his help during patient recruitment and Ms Lambrini Komianou, PT, for her technical assistance during data collection.