
Abstract
Increased negative amplitudes and lack of habituation of contingent negative variation (CNV) in migraine are well established and are supposed to reflect an altered cortical excitability level. Migraine attacks occur less during pregnancy but often relapse after delivery. We investigated the effect of pregnancy on slow cortical potentials and reaction time in migraine patients and healthy controls. Four groups were examined: 14 pregnant migraine patients, 12 non-pregnant migraine patients, 15 pregnant healthy women and 16 non-pregnant healthy women aged 19-38 years. Two recordings were performed in the pregnant subjects: in the 36th week of gestation and 4 weeks after delivery. The nonpregnant subjects were recorded at the same time interval of 8 weeks. Pregnant migraine patients showed significantly fewer migraine days during the third trimester of pregnancy and returned to nearly the former level 4 weeks post delivery. Non-pregnant migraine patients demonstrated a significant reduction of migraine days at the second measurement. There was no effect of pregnancy on CNV amplitudes, but there was an effect of pregnancy on the habituation coefficient and reaction time of migraine patients. Faster habituation from a higher preactivation level was found. As an explanation for the changed habituation level we favour the model of correlation between preactivation level and habituation level, the so-called law of initial value. We found a correlation between preactivation level and habituation. Our study confirms a specific effect of pregnancy on slow cortical potentials in migraine patients.
Introduction
Migraine often improves during pregnancy, an observation confirmed by several epidemiological studies. Most of these studies have been made retrospectively (1–8). A few studies investigated patients prospectively (9–12). Diagnostic headache diaries during patients’ pregnancy until 1 month after delivery have been used (12). Migraine attacks have been shown to be reduced during pregnancy, but often reoccurring after delivery (12).
The pathophysiology of migraine has been widely examined with electrophysiological methods. The brain of the migraine patient is characterized by two different electrophysiological models related to interictal sensory information processing. The first model favours a high cortical preactivation level in combination with higher cortical excitability (13). The second model explains a low cortical preactivation level by reduced habituation of the cortical response due to hypofunctioning subcortico-cortical aminergic pathways (14, 15). A low cortical preactivation level would be due to low serotoninergic activity and a changed mitochondrial metabolism in migraine (16). Effects of repetitive transcranial magnetic stimulation on visual evoked potentials in migraine indicate that migraineurs could be characterized by reduced cortical excitability interictally (17).
A method to determine the interictal activation level and cortical excitability is to record the contingent negative variation (CNV) (18). The CNV is a slow event-related potential associated with the orienting response and reflects the allocation of processing resources to mental activities such as expectancy, attention and preparation of behaviour (19, 20).
Many studies have recorded increased amplitudes of the overall CNV (oCNV) as well as the initial CNV (iCNV) after the first stimulus and lack of habituation of iCNV between migraine attacks (21, 22). There is evidence that cortical preactivation levels change with a longer history of migraine (23).
The aim of the present study was to examine the effect of pregnancy on slow cortical potentials in migraineurs. Significant reduction of migraine attacks is often achieved by medical prophylaxis with β-blocking agents. The clinical effects manifest themselves with improved habituation of the iCNV (24). Pregnant migraineurs often reduce their frequency of migraine attacks during pregnancy (12). Therefore, we assume that pregnant migraineurs behave as patients after prophylactic treatment. We hypothesize that pregnant migraine patients tend to normalize iCNV amplitudes and habituation. We expect lower iCNV amplitudes and changed habituation level during pregnancy and a relapse after delivery.
Materials and methods
Patients and participants
Four groups of participants took part in the study: 14 pregnant migraine patients, 12 non-pregnant migraine patients and two control groups: 15 pregnant healthy women and 16 non-pregnant healthy women. One of the pregnant and one of the non-pregnant migraine patients were excluded because of missing data. For the pregnant women and patients two recordings were made: in the 36th week of gestation and 4 weeks after delivery. Non-pregnant women and patients participated in the recordings at the same time interval (8 weeks).
The non-pregnant healthy control participants without any history of primary headache or neuromuscular disease were recruited from students, whereas the pregnant healthy subjects were found through newspaper advertisements. Pregnant migraine patients were recruited from several gynaecological practices and through the newspaper, whereas non-pregnant migraine patients were acquired from a specialized neurological practice in Kiel, Germany. All migraine patients had a migraine diagnosis made by a neurologist according to the revised International Headache Society (IHS) criteria (25). They all filled out diagnostic headache diaries for 8 weeks, and none of them had received prophylactic treatment for at least 3 months. The pregnant migraine patients suffered from 2.9 migraine days per month over the last 12 months, 100% had regularly taken analgetics and 46.7% triptan medication before pregnancy. The non-pregnant migraine patients suffered from 3.2 migraine days per month over the last 12 months, 92.3% took analgesics and 30.8% triptan medication before measurement. According to the IHS criteria (25), the migraine patients had suffered from migraine with aura (MA) or migraine without aura (MoA) over at least 3 years with a minimum of one attack per month in the last 3 months before pregnancy and measurement. The clinical characteristics of the four groups are shown in Table 1. The patients’ symptomatology was classified as ‘improved’ if there was a reduction in the frequency of migraine days by ≥ 50% compared with the situation before pregnancy (26), as ‘worsened’ if the frequency of migraine days showed an increase of > 50%.
Clinical characteristics
Migraine characteristics averaged 3 months before pregnancy and measurement.
n, number of patients; MoA, migraine without aura; MA, migraine with aura.
EEG procedure
All EEG recordings were taken in a headache-free interval for at least 72 h before or after an attack. This was secured by an inquiry at the recording date and a telephone call 4 days after the recording. Patients kept headache diaries. A warning stimulus S1 (1000 Hz, 75 dB, duration 100 ms) was presented 3 s before an imperative stimulus S2 (2500 Hz, 75 dB, duration of maximum 1500 ms terminated by pressing a button as soon as possible) was presented. Forty CNV trials were presented as a choice reaction task with 32 GO and eight NO-GO trials. The NO-GO trials (200 Hz, 75 dB, duration 100 ms, no reaction required) were randomly presented to minimize adaptation effects during the recording session (27). NO-GO trials were not recorded or analysed in this study.
Reaction time was measured between S2 and pressing the button. EEG was averaged over 6 s (1 s before S1 until 2 s after S2). We used Ag/AgCl electrodes at Cz according to the International 10–20 System with linked mastoids as reference and with an electrode impedance of < 6 kΩ. The EEG was amplified with a bandpass of 0.03–35 Hz and digitized with a sampling rate of 100 Hz for each channel. The period before S1 was used as a baseline, and eye movements were recorded with an electrooculogram (EOG) using electrodes positioned above and below the right eye (bipolar recording). CNV was rejected if the peak activity of EOG exceeded 50 µV (time constant 0.3 s, frequency < 35 Hz). A protocol listed the number of rejected trials for each subject. In no case did this number exceed n = 5. For data analyses only GO trials were averaged, and reaction time, amplitudes of the oCNV, iCNV and terminal CNV (tCNV) were analysed. NO-GO trials were not analysed.
The iCNV was computed as the peak amplitude in a period of 200 ms within the maximum amplitude between 550 and 750 ms after S1 (28). The mean amplitude between 2800 and 3000 ms after S1 served to calculate tCNV, whereas oCNV was the mean amplitude between S1 and S2.
One block comprised four sequential GO trials, and the entire recording was composed of eight blocks. Habituation of iCNV (calculated with linear regression y = aX + b, where a is a habituation coefficient and b the constant) was also calculated. A positive habituation coefficient arose from decreased amplitudes and represented habituation, whereas a negative habituation coefficient represented increased amplitudes characterizing lack of habituation.
Statistical analysis
Statistical analysis was performed using SPSS (Statistical Package for the Social Sciences, version 10.1; SPSS Inc., Chicago, IL, USA). Initial two-way analyses of variance (
Results
Clinical data: course of migraine days before pregnancy, during the third trimester and 4 weeks after delivery
In the group of pregnant migraine patients, the number of migraine days per 4 weeks declined significantly (t 13 = 2.6; P = 0.023) during the third trimester of pregnancy, but increased again to nearly the former level within the first 4 weeks post delivery (t 13 = −3.1; P = 0.008). There were no migraine days in 53% (n = 8), an improvement of migraine days in 20% (n = 3), no one with unchanging migraine days and an increase of migraine days in 27% (n = 4) of the cases. Within the 4 weeks after delivery, the attacks reoccurred in 80% (n = 12) of all pregnant migraine patients, in four cases (33%) within the first week after delivery.
In the group of non-pregnant migraine patients, there was also a reduction of migraine days at the first measurement (t 11 = 2.2; P = 0.051), which became significant 8 weeks later at second measurement (t 11 = 3.9; P = 0.002). Table 2 and Fig. 1 show the results.

Frequency of migraine days in the 4 weeks before pregnancy, during the third trimester and 4 weeks post delivery in pregnant and non-pregnant migraine patients.
Migraine days per 4 weeks in pregnant and non-pregnant migraine patients

n, number of patients; M, mean value of migraine days per 4 weeks;
Electrophysiological data: effects of pregnancy and migraine on slow cortical potentials
Slow cortical potentials at the first measurement
We found no effect of pregnancy and migraine on oCNV, tCNV or iCNV amplitudes. The

Linear regressions [habituation coefficients and constants of initial contingent negative variation (iCNV) amplitudes] of the four groups in the 36th week of gestation and 4 weeks after delivery. One block comprises four sequential GO trials, each recording composed of eight blocks.
CNV components of the examined four groups at the first measurement
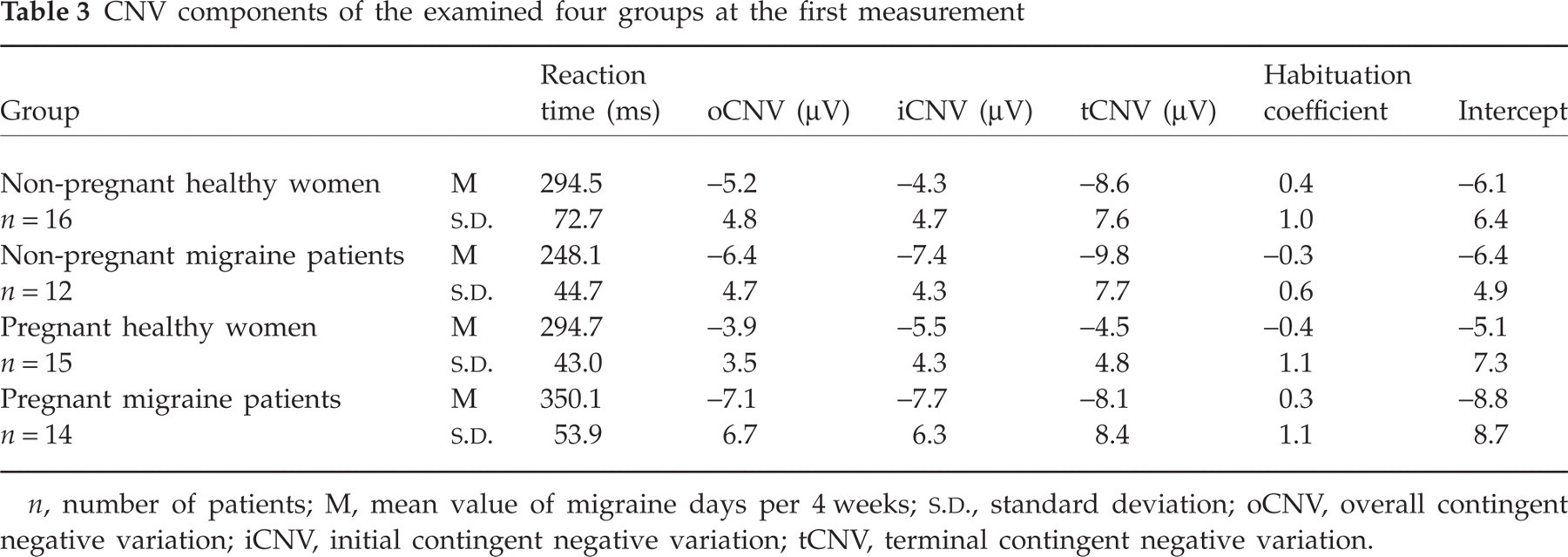
n, number of patients; M, mean value of migraine days per 4 weeks;
There was an interaction effect between pregnancy and migraine on reaction time (F 1,53 = 11.77, P = 0.001). Pregnant migraine patients showed a significantly slower reaction time compared with non-pregnant migraine patients (t 24 = 5.19; P = 0.000) as well as pregnant healthy women (t 27 = 3.09; P = 0.005).
Slow cortical potentials at the second measurement
The second measurement demonstrated an effect of migraine on iCNV amplitudes (F 1,53 = 5.51, P = 0.023). Migraine patients demonstrated more negative iCNV amplitudes than healthy women (t 26 = 3.05; P = 0.005). There was no effect on oCNV or tCNV amplitudes. For the habituation coefficient and the constant of iCNV amplitudes, we saw no effect of pregnancy on migraine at the second measurement. Table 4 shows the results of the CNV components of the four groups at the second measurement.
CNV components of the examined four groups at the second measurement
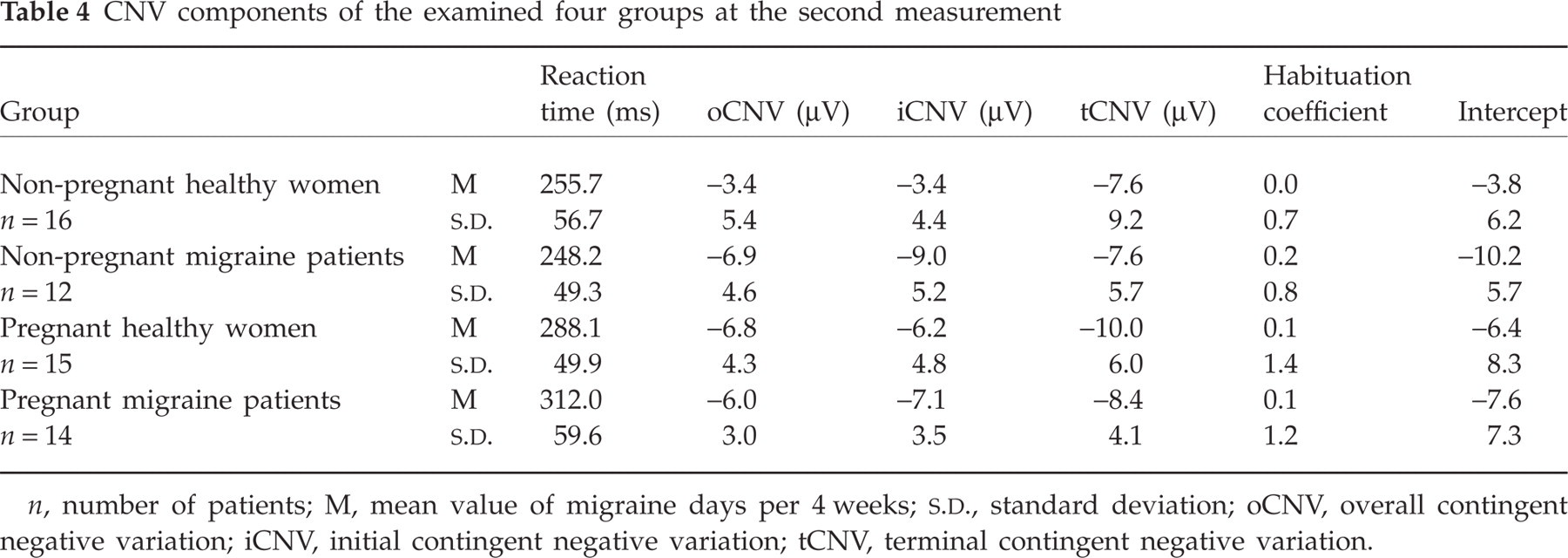
n, number of patients; M, mean value of migraine days per 4 weeks;
We observed an effect of pregnancy on reaction time at the second measurement (F 1,53 = 10.75, P = 0.002). There was a trend to a slower reaction time in migraine patients 4 weeks after delivery compared with migraine patients who where not pregnant (t 24 = 2.86; P = 0.009).
Discussion
Clinical findings
The number of migraine days per 4 weeks dropped significantly in the third trimester of pregnancy and rose to the former level 4 weeks after delivery. These results concur with previous findings (12). This might be the result of lack of hormonal fluctuation throughout pregnancy (3). In contrast, non-pregnant migraine patients also showed a reduction of migraine days at the second measurement. This unexpected effect may be due to effects of improvement of migraine as a result of using diagnostic headache diaries (29). The results suggest an effect of pregnancy on decreasing migraine days, which is probably stronger than the effect of headache diaries.
Electrophysiological findings
The electrophysiological findings show the well-known effect in migraine sufferers of more negative amplitudes of iCNV and a lack of habituation in iCNV amplitudes in non-pregnant migraine patients (22). As expected, migraine patients during the second recording demonstrated more negative iCNV amplitudes and an increased constant.
Furthermore, there are two main findings of our study. The first was an effect of pregnancy on a changed habituation level in migraine patients. Pregnant migraine patients are characterized by habituation compared with pregnant healthy women, who demonstrated a lack of habituation.
What may be the reason of the changed habituation level during pregnancy? There is evidence that the differences in memory, information processing and attention tasks could not be explained by the change of steroid hormones in pregnancy (30, 31). As an explanation for the changed habituation level we favour the model of correlation between preactivation level and habituation level, the so-called law of initial value (32, 33). This theory describes a psychophysiology mechanism of counterregulation dependent upon the preactivation level. The first block of the iCNV represents the cortical preactivation level. We observed a correlation between the first block of iCNV (preactivation level) and habituation coefficient. More negative iCNV amplitudes in the first block led to a more positive habituation coefficient (r = −0.44, P = 0.001). Pregnant migraine patients had high negative iCNV amplitudes in the first block, leading to a positive habituation coefficient. Pregnant healthy women had small negative iCNV amplitudes in the first block and therefore a negative habituation coefficient. This favours on initial value concept. A recent study has shown evidence that cortical preactivation level changes with longer history of migraine. Migraine patients with short-lasting migraine (< 121 months) show little preactivation, whereas long-lasting sufferers (> 120 months) show a higher preactivation level (23). The changed preactivation level seems to reflect long-lasting migraine disease and might result from different initial noradrenergic activity.
Additionally, there is an effect of pregnancy on reaction time, whereas pregnant migraine patients had dramatically slower reaction times than the other groups. Research has demonstrated a decrease in speed of information processing and attention in women in late pregnancy (30). However, in our study there was no effect of reaction time in healthy pregnant women. Only pregnant migraine patients showed slower reaction times. Decelerated reaction times were also found in the Stroop test comparing migraine patients and healthy controls (34). We hypothesize that pregnant migraine patients produce slower reaction times because of their higher preactivation level. According to the above-mentioned concept of initial value, we suppose an effect of preactivation level on reaction performance. A high preactivation level not only affected the habituation coefficient, but seemed also to influence the reaction time negatively. The correlation between preactivation level and tCNV amplitudes (r = 0.26, P = 0.050) and reaction time and tCNV amplitudes (r = 0.25, P = 0.057) was close to significant. The increased preactivation level of migraine patients is reflected in the tCNV amplitudes. The tCNV amplitude affects the reaction time. Further research has found this relationship between tCNV, which represents motor preparation, and reaction time (20, 35).
The study has confirmed an effect of pregnancy on slow cortical potentials and reaction time in migraine. In this context, the preactivation level seems to play an important role. Further research with blood samples, measurement of steroid hormones and psychological factors in pregnancy are needed.
Competing interests
None to declare.
Acknowledgements
The writing of this manuscript was improved by the assistance of one reviewer, N. Birbaumer. We also thank Dr Michael Siniatchkin for helpful discussion.