
Abstract
This prospective cohort study examined the risk of sickness absence among 27 127 female public-sector employees by status of migraine and co-existing conditions. A baseline survey was used to assess chronic disorders and demographic factors. Information on sickness absence in the 3 years following the survey was obtained from employers' registers. Migraine was related to 5.4 extra sickness absence days per person-year, with the corresponding figures being 14.6 and 6.1 for depression and respiratory disorders, respectively. After adjusting for age, marital status, socioeconomic status and presence of depression or respiratory disorders, employees with migraine had a 1.21 (95± confidence interval 1.18, 1.24) times higher risk of self-certified sickness absence episodes (≤ 3 days) than did those without migraine. The corresponding excess risk for medically certified absence episodes (≤ 3 days) was 1.15 (1.12, 1.19). Among employees with depression or respiratory disorders, secondary migraine was associated with an increased risk of sickness absence episode of 1.15 to 1.23. These findings suggest that migraine is associated with increased risk of recorded sickness absence independent of depression and respiratory disorders.
Introduction
Migraine is a common, chronic episodic headache syndrome which affects approximately one-tenth of the adult population in Western countries (1), with higher prevalence reported for women than for men (1, 2). Since migraine particularly affects adults in their most productive years between the ages of 25 and 55 years (3, 4), the related productivity loss inflicts a substantial economic burden on society (5–8). It has been estimated that in the USA the cost of workdays lost due to migraine is about $7.9 billion per year (7, 9).
Most previous research on migraine and work loss has evaluated self-reported sickness absence among migraine patients. These studies have relatively consistently found that female migraineurs report missing 1.1–4.1 workdays per year due to this disorder (6, 8, 10). However, studies using a comparative approach to examine whether sickness absence is higher among migraineurs compared with controls have yielded more inconsistent results (9, 11–14). Although retrospective studies using self-reported sickness absence data have found more sickness absence reported by migraineurs than by individuals without this condition, the few studies using register-based measures of sickness absence (13, 14) have not found clear evidence for incremental absenteeism among migraineurs. However, the sample sizes in these studies have been small.
The aim of this study was to examine the association between migraine and sickness absence in a large cohort of female public-sector employees using sickness absence data collected prospectively from employers' records. As there is an increased prevalence of depression and various respiratory disorders (asthma, hay fever and chronic bronchitis) in persons with migraine (15–20), the effects of these diseases were taken into account in the analyses.
Methods
Study population
The data used in this study were drawn from the ongoing Finnish Public Sector Study (21). Between 2000 and 2002, a questionnaire on health risk factors and morbidities was sent to all female employees working in 10 towns and 21 hospitals; 39 255 (74%) responded to the survey. Of these employees, 34 058 (86.8%) gave consent for their questionnaire responses to be linked to records on sickness absence, but 4117 were excluded because they had a job contract for < 6 months in the year following the survey, and 2814 were excluded because of missing information on variables of interest. Thus, the final study cohort consisted of 27 127 employees, who provided full information on demographic factors and on the presence or absence of migraine, depression and respiratory disorders (asthma, chronic bronchitis or hay fever).
There was no evidence of major selection bias, as the final study cohort corresponded well with all survey respondents in terms of age (means 44.5 vs. 44.5 years), marital status (proportion married or cohabiting 75.1 vs. 74.6%) and socioeconomic structure (proportions of manual, lower non-manual and higher non-manual workers 10.5, 64.1 and 25.4% vs. 11.2, 64.4 and 24.4%, respectively). However, the prevalence of migraine was slightly lower in the final study cohort than among all survey respondents (23.8 vs. 25.0%). This was also the case for depression (11.6 vs. 12.4%) and respiratory disorders (33.9 vs. 35.7%).
The Ethics Committee of the Finnish Institute of Occupational Health approved the study.
Assessment of migraine and other chronic diseases
Migraine, depression, asthma, chronic bronchitis and hay fever were defined on the basis of self-report on a check-list of common chronic diseases (22). For each disorder, participants were asked to report whether or not a physician had diagnosed them as having the disorder in question. Those employees with depression or respiratory disorders who also had migraine were referred to as having secondary migraine.
To examine the validity of self-reported physician-diagnosed migraine, we obtained records on triptan use from the National Prescription Register for the year of the survey. Triptan medication is used specifically to treat migraine, but it is not prescribed for every patient because low-severity migraine can often be treated with non-specific over-the-counter medication (23), and because not all patients respond satisfactorily to triptans (24). Triptan treatment is also expensive (25) and it is contraindicated in the presence of cardiovascular disease or major risk factors for it (26). Of the participants using triptan, 94% reported a history of physician-diagnosed migraine (507 reported migraine/538 used triptan): 0.1% of those not reporting a history of physician-diagnosed migraine used triptan (31/20 677).
Assessment of demographic characteristics
The demographic characteristics measured included age, marital status (married or cohabiting vs. other) and socioeconomic status (manual, lower non-manual or higher non-manual) defined by occupational title based on Statistics Finland's classification. Information on age and occupational title were obtained from the employers' registers. Information on marital status was based on self-reports.
Assessment of sickness absence
Participants' personal identification numbers (a unique number assigned to each Finnish citizen) were used to link the questionnaire data to the employers' sickness absence records for the 3 years following the survey. These records included the first and last days of absences. For episodes of ≤ 3 days, employees complete their own certificate explaining their absence. For episodes > 3 days, they must supply a medical certificate.
In Finnish public-sector organizations, each sickness absence taken by an employee is recorded, including the dates when each absence starts and ends. Employees are paid full salary during sickness absence. Absences due to a family member's funeral or due to caring for a sick child are not recorded as sick leave. Regulations allow absence from work for up to 3 days without loss of salary to care for acutely ill children < 10 years old. There are no limitations to the number of such 3-day periods per employee per year. Thus, the participants had no reason to report being ill falsely when caring for a sick child.
Data analysis
For each respondent, the number of self-certified (1–3 days) and medically certified (> 3 days) sickness absence episodes was calculated and the follow-up period was measured in person-years. Cox proportional hazards models were used to examine the association of migraine with subsequent sickness absence episodes. To take into account the fact that there might be a correlation between multiple events within each subject, a repeated measures survival analysis with a counting process model was applied (27). Sandwich estimates were used to obtain a robust standard error for the parameter estimates (27). As the risk factors for sickness absence (or the size of the effect) may differ for episodes of different duration, self-certified episodes and medically certified episodes were analysed separately. Results for two models are presented, the first of which includes adjustments for age, marital status and socioeconomic status, and the second an additional adjustment for the presence of doctor-diagnosed depression and respiratory disorders. To examine the effect of secondary migraine on sickness absence, separate Cox models were calculated using the status of depression and respiratory disorders. To describe the data in absolute terms, rates of sickness absence episodes were expressed as per 100 person-years, and total numbers of sickness absence days were expressed as per person-year adjusting for age, marital status and socioeconomic status. Comparisons between subgroups were done using Poisson regression analysis for sickness absence episodes, and using regression analysis based on a negative binomial distribution for total numbers of sickness absence days. Excess risk of sickness absence associated with migraine was calculated by subtracting the absolute absence rates of employees without migraine from the absolute rates of those with migraine.
All statistical analyses were carried out using the SAS 9.1.3 program package (SAS Institute Inc., Cary, NC, USA).
Results
Of the 27 127 respondents, 6450 (23.8%) reported doctor-diagnosed migraine. Prevalence of migraine was more common among older respondents, and among those who reported doctor-diagnosed depression or respiratory disorders. Lower non-manual workers had a lower prevalence of migraine than did higher non-manual workers. Marital status was not associated with migraine (Table 1).
Characteristics of the study sample by doctor-diagnosed migraine
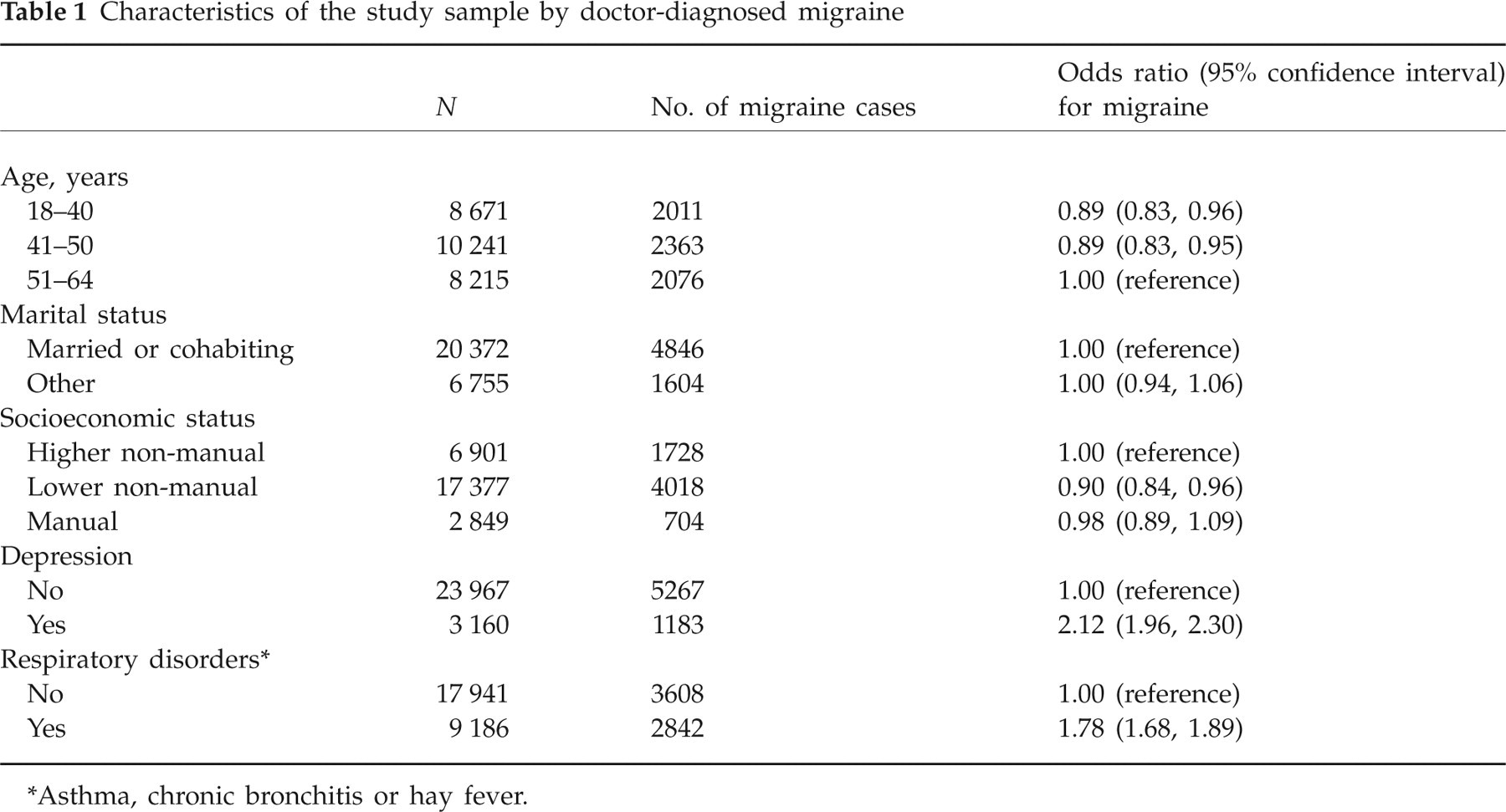
Asthma, chronic bronchitis or hay fever.
A total of 108 566 self-certified (≤ 3 days) and 56 859 medically certified (> 3 days) sickness absence episodes were recorded, resulting in 1201 563 sickness absence days (occurring in 75 403 person-years of follow-up). Both self-certified and medically certified sickness absence episodes were more common among employees who were not married or cohabiting, who had lower socioeconomic status and who reported doctor-diagnosed depression or respiratory disorders. Self-certified sickness absence episodes were more common among younger employees and medically certified sickness episodes were more common among older employees (Table 2).
Hazard ratios for sickness absence episodes by baseline characteristics
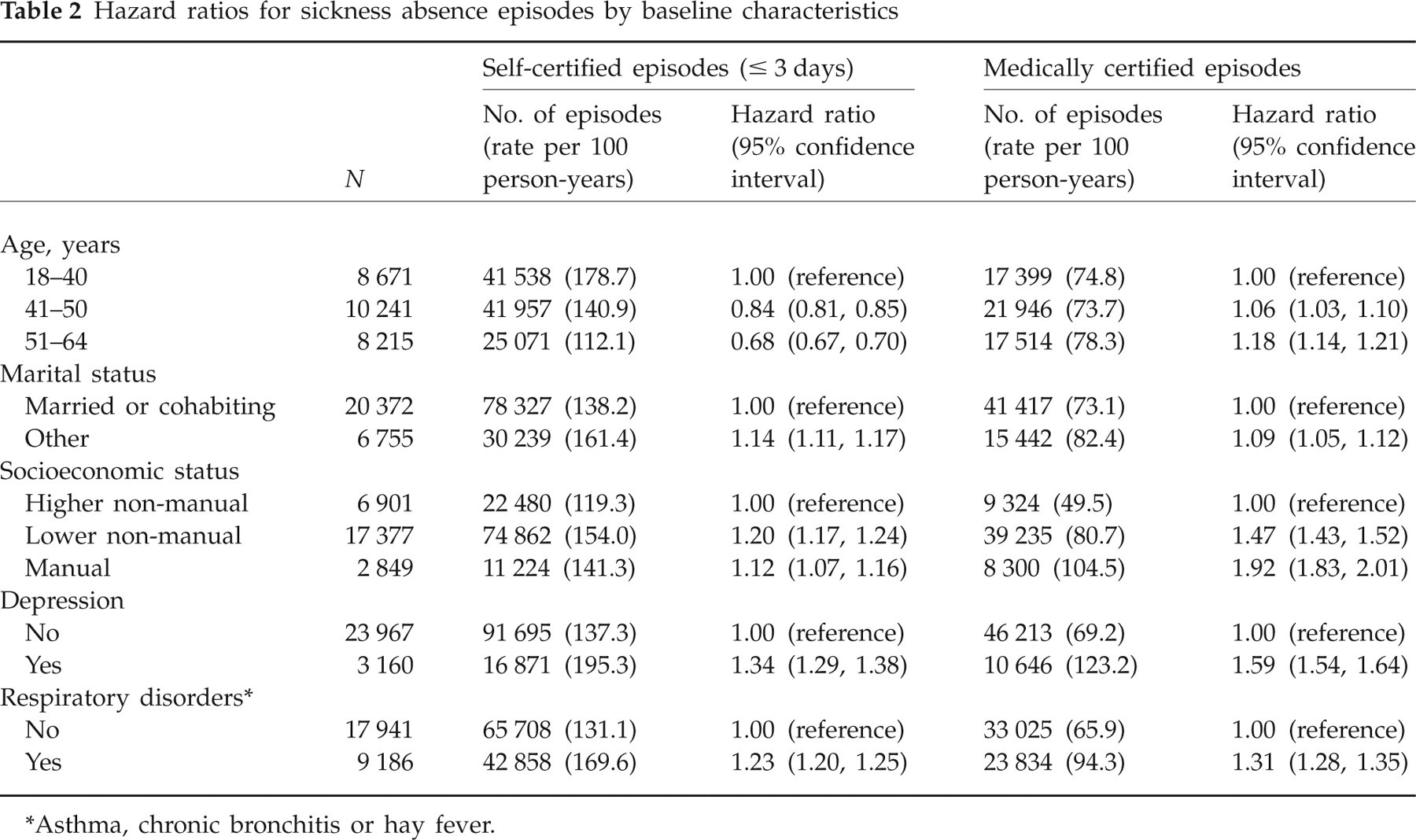
Asthma, chronic bronchitis or hay fever.
Association between migraine and sickness absence
After adjustment for age, marital and socioeconomic status, the total number of sickness absence days (combining self-certified and medically certified absence data) was 20.1 per person-year for participants reporting physician-diagnosed migraine and 14.7 for those not reporting migraine. For comparison, the corresponding figures were 28.8 for those with reported physician-diagnosed depression vs. 14.2 for those without depression and 20.0 for those with respiratory disorders vs. 13.9 for those without such disorders. Thus, migraine was related to 5.4 excess sickness absence days per person-year, whereas the corresponding figures were 14.6 and 6.1 for depression and respiratory disorders, respectively.
Table 3 shows the statistics for sickness absence according to migraine status. The crude levels of both self-certified and medically certified sickness absence episodes were higher for respondents with migraine compared with those without migraine, with the excess risk being 44.4 and 23.8 episodes per 100 person-years, respectively, for self-certified and medically certified episodes. After adjusting for age, marital and socioeconomic status, employees with migraine had a 1.26-fold [95% confidence interval (CI) 1.23, 1.29] risk of self-certified sickness absence compared with those without migraine. The corresponding risk for medically certified episodes was 1.25 (95% CI 1.21, 1.28). These associations were not explained by depression or respiratory disorders. The hazard ratios became slightly attenuated with further adjustment, but remained significant in the fully adjusted model.
Hazard ratios∗ for self- and medically certified absence episodes by migraine status

Adjusted for age, marital status and socioeconomic status.
Adjusted for (∗) and presence of doctor-diagnosed depression and respiratory disorders.
Effect of secondary migraine
Migraine was reported by 37.4% of employees with depression and by 30.9% of those with respiratory disorders. Compared with employees with depression or respiratory disorders only, those with co-occurring migraine had higher absolute rates of both self-certified and medically certified sickness absence episodes (Table 4). After adjustment for age, marital status and socioeconomic status, employees with depression and co-occurring migraine had a 1.15-fold to 1.18-fold risk of sickness absence compared with employees with depression only. Among employees with respiratory disorders and co-occurring migraine, the excess risk of both self-certified and medically certified sickness absence episodes was between 1.21 and 1.23.
Hazard ratios for self- and medically certified absence episodes by status of depression, respiratory disorders and co-existing migraine

Adjusted for age, marital status and socioeconomic status.
Adjusted chronic bronchitis, or hay fever.
Association between triptan medication and sickness absence
Based on prescription records, 358 (2.0%) participants were treated with triptan medication during the year of the survey. As shown in Fig. 1, the total numbers of sickness absence days were higher among both migraine sufferers using triptan and those not using triptan compared with those not reporting migraine; the rate ratios adjusted for age, marital status and socioeconomic status were 1.36 (95% CI 1.21, 1.53) and 1.37 (95% CI 1.32, 1.42) for migraineurs on triptan medication and those not on that medication, respectively. Triptan users had total numbers of sickness absence days similar to those of migraine patients using non-triptan medications (rate ratio 0.99; 95% CI 0.88, 1.12). Stratified analysis by length of sickness absence episodes showed that triptan users had a slightly higher rate of self-certified absence episodes (rate ratio 1.13; 95% CI 1.06, 1.22), but no difference was seen for medically certified absence episodes (rate ratio 0.95; 95% CI 0.86, 1.04).
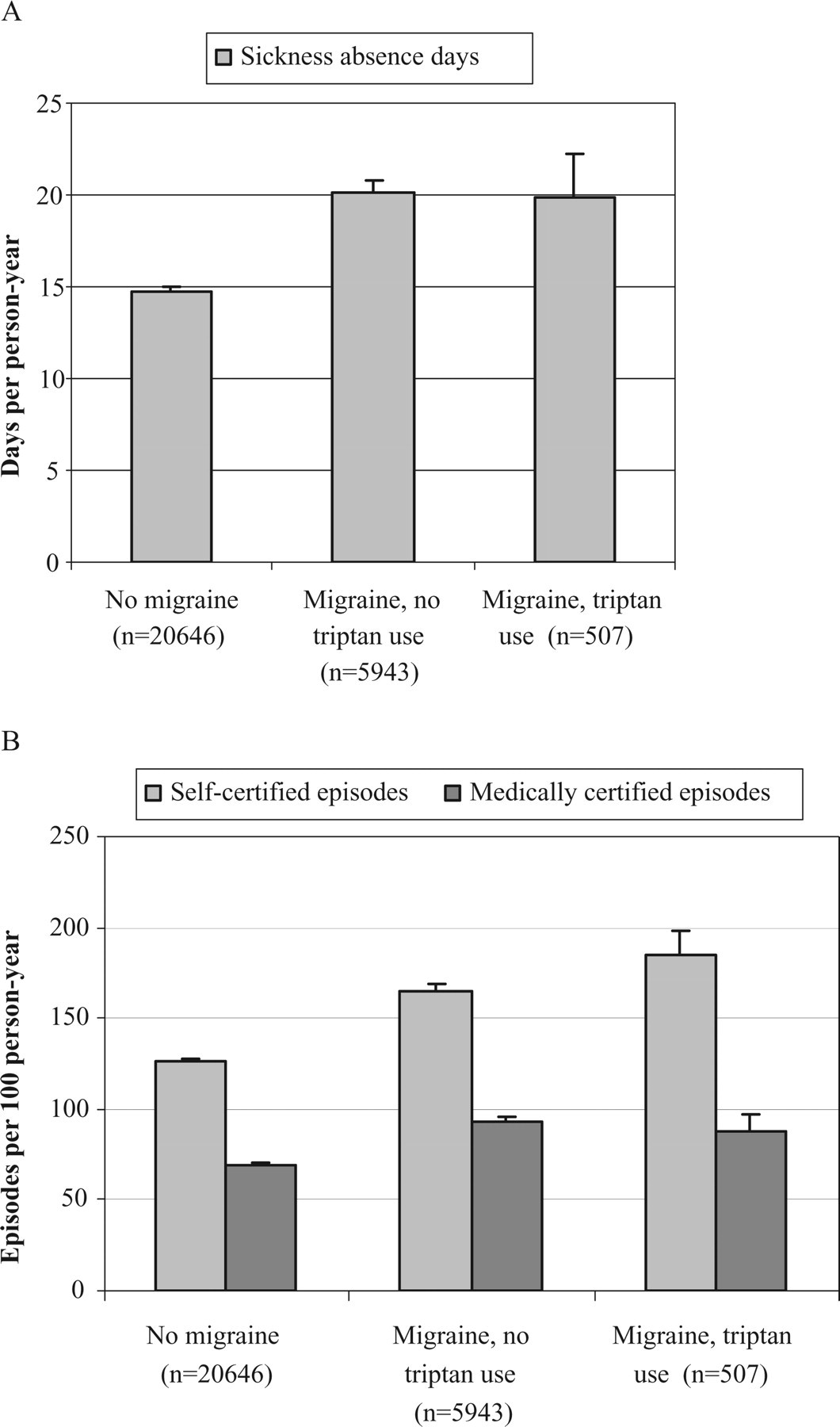
Total number of sickness absence days and rates of self-certified (≤ 3 days) and medically certified (> 3 days) sickness absence episodes by status of self-reported physician-diagnosed migraine and recorded triptan use. Adjustment for age, marital status and occupational status.
Discussion
In this large prospective study of female public-sector employees, those with migraine were at increased risk for both self-certified and medically certified sickness absence episodes, even after adjustments for age, marital status, socioeconomic status, and for the presence of co-occurring depression or respiratory disorders. Migraine was related to 44 extra self-certified absence episodes per 100 person-years, 24 extra medically certified absence episodes per 100 person-years and 5.4 extra sickness absence days per person-year. Among employees with depression or respiratory disorders, secondary migraine was associated with a 1.15-fold to 1.23-fold increased risk of sickness absence. Given that migraine is relatively common, these estimates suggest that migraine is associated with a considerable burden of sickness absence.
Whereas previous studies have typically been based on self-reports of sickness absence, we assessed sickness absence from employers' records to avoid reporting bias. Our results are in agreement with studies that have reported a relationship between migraine and incremental sickness absence (9, 11). The fact that some prior studies (13, 14) using register-based measures of sickness absence have failed to observe this association may be explained in part by differences in characteristics of the study populations, and because the relatively small sample sizes in these studies decreased the likelihood of detecting significant associations with moderate effect size.
In agreement with previous studies, we found an association between migraine and depression and respiratory disorders (15–20). Both depression and respiratory disorders predict sickness absence (28, 29), raising the question whether the excess risk of sickness absence related to migraine is attributable to these chronic conditions. Our analyses suggest that this is not the case, because the association between migraine and sickness absence survived adjustment for depression and respiratory disorders, and because secondary migraine was significantly associated with sickness absence also among participants with depression or respiratory disorders.
Study strengths and weaknesses
The specific strengths of this study were the use of a well-characterized cohort, large sample size, longitudinal study design and control for several potential confounding factors. In addition, our sickness absence measure obtained from employers' records is probably better in terms of coverage, accuracy and consistency over time than one attained through self-reports (30).
A limitation of our study is that the information on migraine status was based on self-report rather than on the diagnostic criteria of the International Headache Society (31, 32). Prior research (33) has shown self-report to be a sensitive measure of migraine, but its specificity is not optimal, as some headache patients are not able to identify correctly whether their headache is a migraine or some other type of headache. Although this could lead to overestimation of migraine prevalence, the fact that we requested only reports on physician-diagnosed migraine may contribute to underestimation. This is because many migraineurs are not physician-diagnosed. However, the prevalence of a history of doctor-diagnosed migraine of 23.8% observed in this study is well within the range of community prevalence estimates of between 3.3 and 32.6% given in prior studies (4).
Use of triptan is a reliable indicator of the presence of physician-diagnosed migraine. Our analyses using register-based information on triptan as a measure of migraine revealed associations between migraine and subsequent sickness absence days very similar to the associations found for self-reported doctor-diagnosed migraine. These findings further reinforce the results regarding the excess absenteeism among migraineurs. That triptan users compared with non-users had a slightly higher rate of self-certified absence episodes suggests a greater severity of migraine for triptan users (23), especially because prior studies have shown that triptans can reduce work absenteeism and improve productivity compared with standard of care or non-triptan medications (34).
Loss to follow-up was slightly greater among employees with migraine or other morbidities. This may have led to attenuation, rather than overestimation, of the association between migraine and sickness absence in our study. Furthermore, absenteeism related to migraine accounts for only part of the costs to employers, as migraine is also related to decreased work effectiveness (34–36).
Although the possibility of confounding by an unknown factor can never be excluded in observational studies, a major bias in our study seems unlikely, as various potential confounders (age, marital status, socioeconomic status and presence of doctor-diagnosed depression or respiratory disorders) were adjusted for in the analyses. In addition, as there is an association between migraine and stroke among women (37), the analyses were repeated in a subcohort from which stroke patients (n = 356) had been excluded. However, this did not substantially change our results.
The present cohort comprised Finnish female public-sector employees only, thus there is a need for replications to assess whether these findings are generalizable to other populations, other ethnic groups and men.
Conclusion
The present findings from a large contemporary cohort of female public-sector employees add to the evidence that migraine is associated with a considerable burden of sickness absence. Furthermore, we have shown that the association between migraine and sickness absence is not attributable to co-existing respiratory disorders or depression. As migraine is a fairly common condition, strategies aimed at better recognition and treatment of migraine could lead to substantial societal benefits by increasing the working capacity of the individuals affected.
Acknowledgements
This study was supported by the Academy of Finland (projects 105195, 117604, 124322 and 124271) and the Finnish Working Environment Foundation.