
Abstract
The trigeminal trophic syndrome is an unusual consequence of trigeminal nerve injury that results in facial anaesthesia, dysaesthesia and skin ulceration. Limited knowledge is available. The aim of this study was to increase the knowledge of this syndrome by performing a retrospective medical record review and case series report. Fourteen cases were identified. The female : male ratio was 6:1. Mean age of onset was 45 years (range 6-82). The cause was iatrogenic in most. Latent period to onset ranged from days to almost one decade. The majority (n = 12) had bothersome dysaesthesias. Most (n = 9) self-manipulated the face; a third (n = 5) did not. Most ulcers affected the second trigeminal division, mainly in the infraorbital nerve distribution. Neuropathic and/or neuralgic facial pain occurred in 50% (n = 7). Pain intensity was severe in most (n = 6). Gabapentin gave relief in two. To conclude, trigeminal trophic syndrome follows injury to the trigeminal nerve or its nuclei. For unclear reasons, most ulcerations follow infraorbital nerve distribution. Self-manipulation may contribute to ulcer development rather than being required. Gabapentin may help pain.
Keywords
Introduction
The trigeminal trophic syndrome (TTS) is an unusual consequence of trigeminal nerve pathway injury, which results in the classic clinical triad of unilateral trigeminal anaesthesia, facial paraesthesias and lateral nasal ala ulceration (1). A small number of patients, however, suffer skin lesions in other regions (non-nasal) (2). TTS may have been described as early as 1895 by Adolf Wallenberg while presenting his first patient with lateral medullary infarction (‘Wallenberg's syndrome’), which affects the spinal nucleus of the trigeminal nerve and its tract among other neural structures (3, 4). When referring to the 38-year-old man with hemifacial anaesthesia, Wallenberg wrote: ‘on the eight day, an herpetic eruption appeared on some of the analgesic areas’ (4). In 1933, TTS appeared in the English literature, when Loveman reported one case after resection of the sensory root of the Gasserian ganglion for trigeminal neuralgia (TN) treatment (5). Independently, that same year McKenzie reported two similar cases following TN surgery and one following trigeminal section during acoustic neuroma removal (6). Since then, multiple isolated case reports and small case series have appeared, mainly in the dermatological literature. The TTS symptoms can endure and last decades without significant relief, making life miserable (2).
Illustrative patient (case 13)
A 68-year-old woman presented with the following history. At age 55 years, she developed left TN (second distribution) and was placed on carbamazepine. Since she did not tolerate medication side-effects, left Gasserian ganglionectomy was performed. Immediately after surgery, she had left hemifacial anaesthesia, which resolved the neuralgia. Days later, she developed left hemifacial mild–moderate, constant, ‘difficult to describe’ pain and severe itching. Over the next years, she experienced erythematous lesions in her left forehead and periorbital region. A false sense of airflow obstruction developed (‘like a flap’) in her left nasal airway. Although Ear Nose and Throat examination failed to find anatomical obstruction, she admitted frequent and conscious self-manipulation attempting to relieve this ‘blockage’, which led to erosion of the nasal septum. By age 67 years her symptoms had not significantly changed and she started to feel intermittent, brief (seconds), painful ‘bug bites’ in the left nasolabial fold, intranasal cavity and periorbital region. If she pressed with her fingers, the intensity would diminish. A constant ocular foreign body sensation and severe neuralgic pain eventually developed too. Opiates, topiramate, pregabalin, nortriptyline, amitriptyline, clonazepam and oxcarbazepine failed to provide relief. Gabapentin 2400 mg/day gave partial relief. On examination, she had left hemifacial anaesthesia and absent corneal reflex. Her inferior nasal septum and complete nose columella were absent (Fig. 1). Multiple skin ulcerations and annular erosions were seen in her left scalp, lateral nose and medial eyebrow. The largest ulceration was at the left nasal ala (Fig. 2).

Absent nasal columella and inferior half of nasal septum. Partial absence of inferior turbinates.

Multiple skin ulcerations and annular erosions.
Methods
The Mayo Clinic's medical index database was queried to include the period from 1 January 1996 to 21 August 2007. Terminology sought for included: ‘trigeminal’ and ‘neurotrophic’ or ‘trophic’; ‘trigeminal neuralgia’, ‘trophic-neurotrophic ulcer’ and ‘ulcer nose’. Following counting, and with Institutional Review Board approval, a retrospective medical record review was performed to verify the diagnosis and collect data. The case series is here reported.
Results
Table 1 summarizes patient characteristics. Of 19 unique cases, 14 met diagnostic criteria, making this the largest TTS case series available. Women outnumbered men with a 6:1 ratio. Mean age of onset was 45 years (range 6–82 years). All cases were strictly unilateral, nine left- and five right-sided. The cause was iatrogenic and known in eight (cases 3, 4, 7, 8, 9, 11, 12 and 13); iatrogenic and unknown in one (case 5) since multiple procedures were done; primary neurological in two (cases 6 and 10); and uncertain if primary neurological or iatrogenic in three (cases 1, 2 and 14). The latent period from trigeminal injury to symptom onset ranged from days to almost one decade. The vast majority (n = 12) had bothersome dysaesthesias. Although most (n = 9) self-manipulated and injured the face, approximately one-third (n = 5) did not. Skin ulceration/soft tissue lesions were seen in all, predominantly in the second trigeminal division distribution (n = 10), followed by first (n = 4) and third (n = 2) division distribution. All had trigeminal neuropathy on examination manifested as facial hypo- or anaesthesia. Facial pain occurred in 50% (n = 7) of individuals and is summarized in Table 2. In those with pain, the intensity was severe in most (n = 6) and mild in only one (case 12). Five patients had constant, neuropathic pain features. Three patients had neuralgic components. High-dose gabapentin gave partial relief in two individuals.
Summary of cases
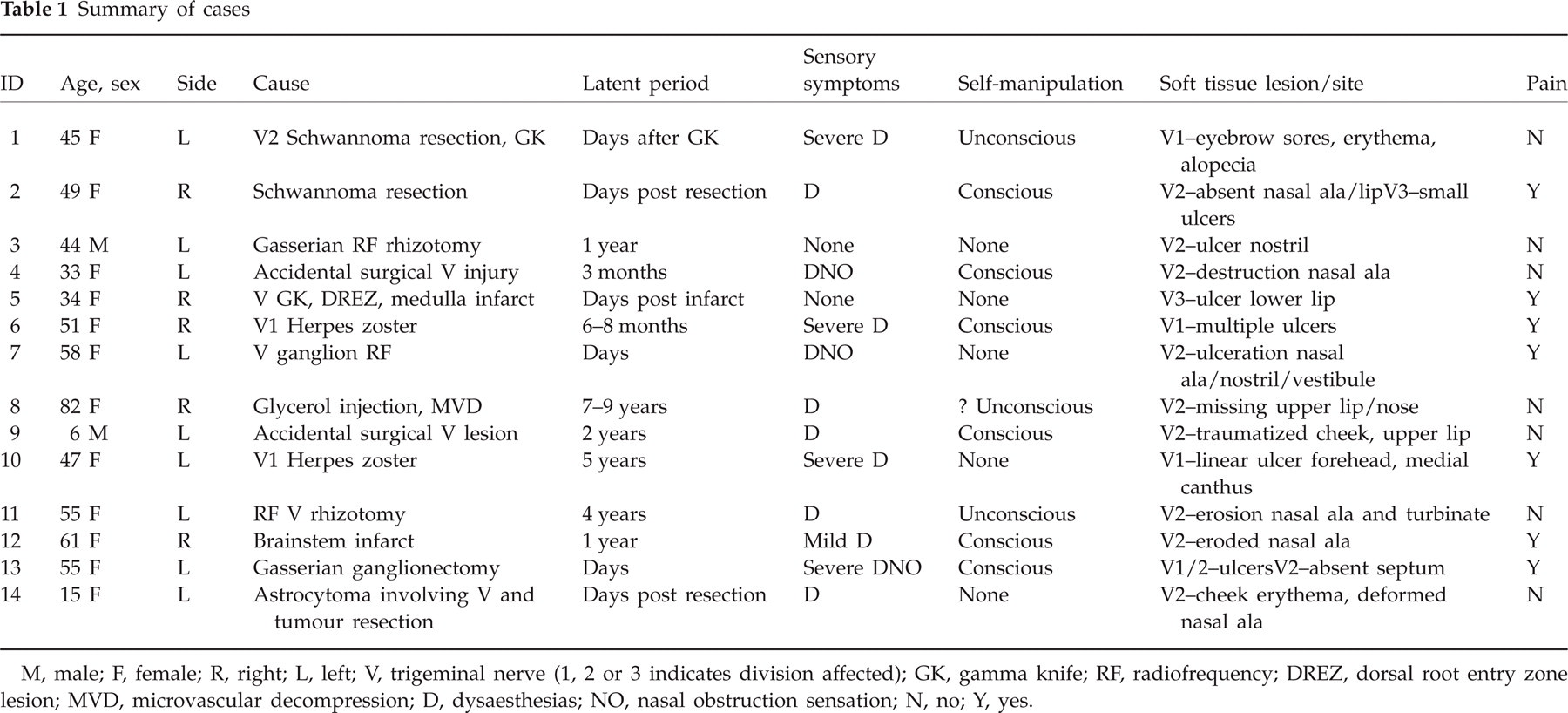
M, male; F, female; R, right; L, left; V, trigeminal nerve (1, 2 or 3 indicates division affected); GK, gamma knife; RF, radiofrequency; DREZ, dorsal root entry zone lesion; MVD, microvascular decompression; D, dysaesthesias; NO, nasal obstruction sensation; N, no; Y, yes.
Pain characteristics
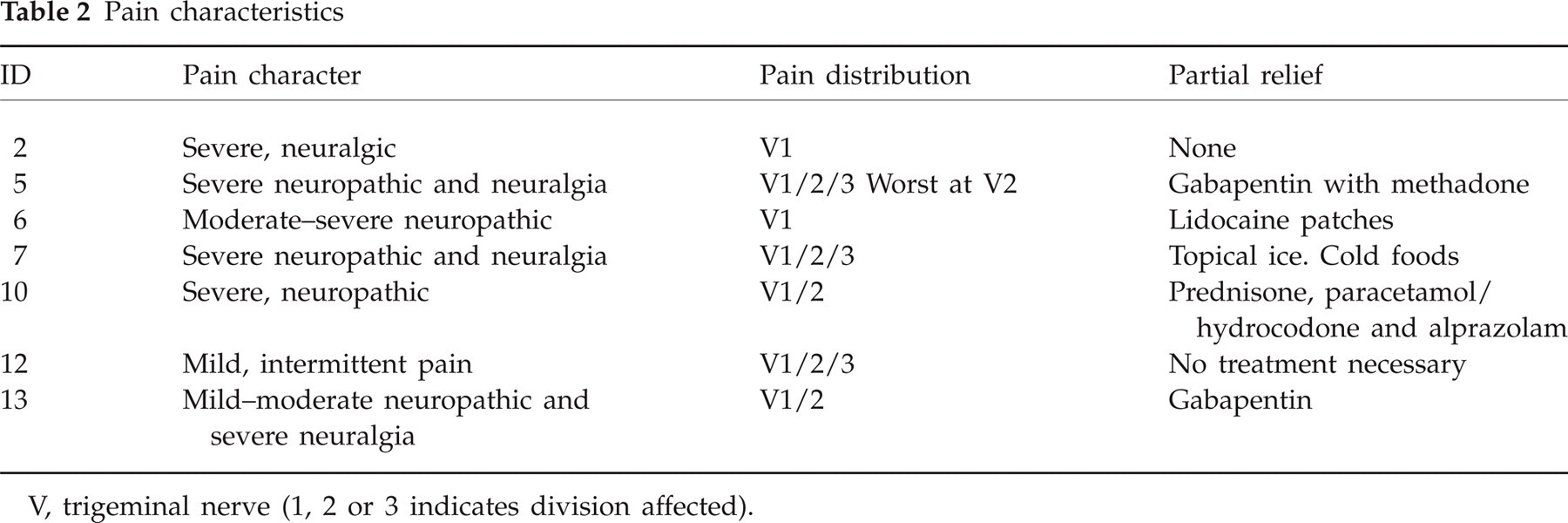
V, trigeminal nerve (1, 2 or 3 indicates division affected).
Discussion
In this series, TTS affected all age groups but clearly predominated in women. No clear side predilection was seen. A trigeminal pathway lesion was known in all cases, and by far the most common (more than 50%) causes of TTS were iatrogenic (whether intentional or accidental) trigeminal lesions occurring while treating TN, face pain, cluster headache, or neoplasms. The rest involved herpes zoster virus (HZV), and mixed primary and iatrogenic trigeminal insults. The time from trigeminal nerve injury to TTS symptoms ranged from days to years. That HZV and brainstem ischaemia may lead to TTS has previously been reported (7, 8). All patients here presented had an injury of the trigeminal nerve or its nuclei. None of them had higher trigeminal pathway injuries. I am not aware either of any TTS cases in the literature that are secondary to trigemino-thalamic or thalamo-cortical pathway lesions.
All patients had a dermatology evaluation, which is mandatory in these cases to rule out potential TTS mimics such as skin infections, neoplasms, vasculitis, granulomatous disease and other dermatitides (1). In general, it is currently accepted that the skin/soft tissue lesions are self-inflicted, probably secondary to paraesthesias (1, 2). In that sense, as pointed out by Shea, ‘trophic’ is a misnomer, since the term implies that denervation directly withdraws a putative ‘nourishing’ influence on the end organ (9). Although most patients here described had bothersome dysaesthesias, not all of them did. Furthermore, a significant proportion did not self-traumatize the anaesthetic side of the face. Westerhof has reported the successful treatment of chronic facial ulceration with transcutaneous electrical stimulation, possibly through enhancement of local blood supply with consequent improved wound healing (10). These observations suggest there is in fact a true trophic effect of normal trigeminal innervation on cutaneous vascular tone (9). Dysaesthesias and self-manipulation were not necessary for the development of skin ulceration in some of the cases described here. However, in those with more severe and bothersome dysaesthesias, self-manipulation may have contributed to more destructive and disfiguring skin/soft tissue lesions, probably from self-induced trauma to an already anaesthetic area. Therefore, self-manipulation seems to be a contributing factor for a worse cosmetic outcome, but not a requisite for TTS development. Dysaesthesias included itching, burning, tingling, crawling, ocular foreign body, pressure, and ‘bug bite’ sensations among others. In some, a sense of nasal airflow obstruction, ‘stuffiness’ or ‘dribbling’ developed.
With the exception of patient 8, who suffered from dementia, none of the others suffered from cognitive or psychiatric disorders. This is important to note, since TTS sufferers frequently self-manipulate their face, which could potentially lead to a wrongful diagnosis of dermatitis artefacta, a condition where patients have self-inflicted skin lesions that are solely produced by the patient's own actions, usually as a manifestation of psychological disturbances. In TTS, however, self-manipulation seems to be a ‘reflexive’ action in an attempt to relieve bothersome dysaesthesias. The absence of dysaesthesias decreased the incidence of self-manipulation in this series.
The facial skin/soft tissue lesions primarily affected the second trigeminal division distribution, particularly in the area of the nasal ala and its proximity. The preference for ulceration at the nasal ala is well described (1). Why this happens is unclear. Prior theories suggest that this happens because this zone overlaps between the first and second trigeminal division sensory innervation (11). Anatomically, this theory is inaccurate and does not explain the appearance of skin ulcers in other regions such as the scalp, forehead, eyelid and others reported in the literature (2) and in this series. It does appear, however, that the skin ulcerations occur in the distribution of individual terminal sensory cutaneous branches from either one of the three main trigeminal divisions. Cutaneous branches innervating the upper lip (superior labial branch), medial cheek (superior alveolar branch) and side of the nose (external nasal branch) all come from the infraorbital nerve, a second trigeminal division ramification (12). Similarly, eyebrow, scalp and forehead ulcers seem to follow the distribution of the infratrochlear branch of the nasociliary nerve, and to a lesser extent the supratrochlear and supraorbital cutaneous branches of the frontal nerve, all first division trigeminal nerve ramifications (Fig. 3).

Skin ulcerations occur in the distribution of terminal cutaneous sensory branches of the main trigeminal divisions. Illustration done by David Factor, Medical Illustrator.
Although pain is not considered part of the ‘classic’ presentation of TTS, in this series 50% had pain. In all but one, the intensity was very severe with either fixed/constant neuropathic (burning, throbbing, piercing, aching), intermittent neuralgic, or both pain characteristics. In all but one, the pain was extremely challenging to treat, intractable, and resistant to multiple drugs including opiates, tricyclic antidepressants, anticonvulsants, benzodiazepines, lidocaine patches and corticosteroids, among others. Two patients perceived high-dose gabapentin as helpful, providing partial relief. Whereas the neuralgic pain can be explained by the trigeminal nerve/nuclei lesion, the widespread neuropathic pain is likely to be secondary to deafferentation. With some encouraging results from primary motor cortex stimulation (13) used in similar settings, it is possible that some of the patients with TTS could benefit from similar interventions.
Conclusions
TTS primarily affects middle-aged women, but can affect all ages. It is a consequence of lesions through different mechanisms of the trigeminal nerve or its nuclei. Clinical manifestations include trigeminal neuropathy and trophic skin ulcerations. Cutaneous lesions occur in the distribution of terminal sensory cutaneous nerve ramifications of the trigeminal nerve divisions. For unclear reasons, the most common distribution of ulcerations was that of the infraorbital nerve. Most patients have bothersome dysaesthesias, and a significant proportion have pain as part of the syndrome. Self-manipulation does not appear to be a requisite for ulcer development, but rather may be a contributing factor. TTS management can be extremely challenging and should involve multiple specialists including neurologists, dermatologists and plastic surgeons among others, when appropriate. High-dose gabapentin may be of benefit for pain occurring in association with the TTS.