
Abstract
Migraine has been associated with an unfavourable cardiovascular risk profile and with increased risk of cardiovascular disease. In a cross-sectional analysis of 17 616 women aged ≥45 years, we evaluated the association of migraine and migraine aura status with elevated levels of total cholesterol, low- and high-density lipoprotein cholesterol (HDL-C), non-HDL-C, apolipoprotein (Apo) A-1 and B100, lipoprotein (a), C-reactive protein (CRP), fibrinogen, intercellular adhesion molecule-1, homocysteine and creatinine. A total of 5087 (18.4±) women reported any history of migraine. Compared with women with no migraine history, women who reported any history of migraine had modestly increased adjusted odds ratios (95± confidence interval) of 1.09 (1.01, 1.18) for elevated total cholesterol, 1.14 (1.05, 1.23) for non-HDL-C, 1.09 (1.01, 1.18) for Apo B100 and 1.13 (1.05, 1.22) for CRP. The increase did not meaningfully differ according to migraine aura status and migraine frequency. In this large cohort of women, only a modest association was found between migraine and adverse levels of certain cardiovascular biomarkers.
Introduction
Migraine is a common primary headache disorder affecting about 18% of the female and 6% of the male US population (1). It is characterized by severe, pulsating, mostly unilateral headache pain that is accompanied by nausea, vomiting and decreased toleration of light and sound. In some patients, transient neurological phenomena occur known as migraine aura. These include mostly visual sensations, such as the occurrence of flashlights and zigzag lines, but can also lead to unilateral sensible deficits in arm or leg, or in rare cases to unilateral weakness.
Migraine, and specifically migraine with aura (MA), has been associated with increased risk of ischaemic stroke in several observational studies (2–6). Recently, MA has also been associated with increased risk of major ischaemic cardiovascular disease (CVD), including coronary heart disease (7). Furthermore, migraine, and particularly MA, has been associated with a more unfavourable cardiovascular risk profile (8), increased levels of prothrombotic or vasoactive factors (9–13), as well as the C677T polymorphism in the methylenetetrahydrofolate reductase gene that has also been associated with increased homocysteine levels (13–15). However, the precise mechanisms by which migraine may lead to cardiovascular events remains unclear. Although it has been shown that migraine is associated with increased levels of total cholesterol and decreased levels of high-density lipoprotein cholesterol (HDL-C) (8), a comprehensive evaluation of the association between biomarkers of CVD and migraine is lacking.
We thus aimed to evaluate the association between traditional and novel biomarkers that have been related to increased risk of CVD and migraine as well as migraine aura status in a large cohort of apparently healthy, middle-aged women. Specifically, the following biomarkers were evaluated: total cholesterol, low-density lipoprotein cholesterol (LDL-C), HDL-C, non-HDL-C, apolipoprotein (Apo) A-1 and B100, lipoprotein (a), high-sensitive C-reactive protein (CRP), fibrinogen, soluble intercellular adhesion molecule-1 (ICAM-1), homocysteine and creatinine.
Methods
Study population
Study subjects were all participants in the Women's Health Study (WHS), a completed randomized, placebo-controlled trial designed to test the benefits and risks of low-dose aspirin and vitamin E in the primary prevention of CVD and cancer. The design, methods and results have been described in detail previously (16–18). Briefly, a total of 39 876 US female health professionals aged ≥ 45 years at study entry (1992–1995) and without a history of CVD, cancer or other major illnesses were randomly assigned to active aspirin (100 mg on alternate days), active vitamin E (600 IU on alternate days), both active agents, or both placebos. All participants provided written informed consent and the Institutional Review Board of Brigham and Women's Hospital, Boston, approved the WHS. Baseline information was self-reported and collected by a mailed questionnaire that asked about many cardiovascular risk factors and lifestyle variables.
Blood samples were collected from 28 345 participating women prior to randomization. Of those, a total of 640 samples could not be analysed for all evaluated biomarkers due to technical limitations. We further excluded 79 women with missing migraine information, leaving 27 626 for this study.
Assessment of migraine
Participants were asked on the baseline questionnaire: ‘Have you ever had a migraine headache?’ and ‘In the past year, have you had a migraine headache?’ From this information, women were categorized into ‘no migraine history’ and ‘any history of migraine’. Furthermore, we distinguished between ‘active migraine’, which includes women with self-reported migraine in the year prior to completing the baseline questionnaire, and ‘prior migraine’, which includes women who reported ever having had a migraine but none in the year prior to completing the questionnaire. Those participants who reported active migraine were asked details about their migraine attacks, including attack duration of 4–72 h; unilateral location of pain; pulsating quality; inhibition of daily activities; aggravation by routine physical activity; nausea or vomiting; sensitivity to light; and sensitivity to sound. In previous studies of the WHS (7, 19, 20), we have shown good agreement with modified 1988 International Headache Society (IHS) criteria for migraine (21). Specifically, we have shown that among WHS participants who provided a blood sample and reported active migraine, 83.5% fulfilled all but one modified IHS criteria (code 1.7, migrainous disorder) and 46.6% fulfilled all modified IHS criteria for migraine (code 1.1) (7).
Participants who reported active migraine were further asked whether they had an ‘aura or any indication a migraine is coming’. Responses were used to classify women who reported active migraine into active MA and active migraine without aura (MoA). In addition, women with active migraine reported the frequency of their attacks (daily, weekly, monthly, every other month, less than six times per year). We combined the answer categories daily (n = 16), weekly (n = 162) and monthly (n = 701) into one category due to the low number of participants in these categories.
Biomarker measurements
All blood samples were collected in tubes containing ethylenediamine tetraacetic acid and stored in vapour phase liquid nitrogen (−170 °C). In a core laboratory certified by the National Heart, Lung and Blood Institute/Centers for Disease Control and Prevention Lipid Standardization program, samples were analysed for lipids and a panel of inflammatory biomarkers. Total cholesterol, HDL-C and directly obtained LDL-C were assayed with the use of reagents from Roche Diagnostics (Basel, Switzerland) and Genzyme (Cambridge, MA, USA). Apo A-1 and B100 were measured using an immunoturbidimetric assay (Dia-Sorin, Stillwater, MN, USA). Lipoprotein (a) and high-sensitive CRP were measured using immunoturbidimetric assays on a Hitachi 917 analyser (Roche Diagnostics, Indianapolis, IN, USA) using reagents and calibrators from Denka Seiken (Tokyo, Japan). Fibrinogen was measured using immunoturbidimetric assay (Kamiya Biomedical, Seattle, WA, USA) and ICAM-1 using an enzyme-linked immunosorbent assay (R&D Systems, Minneapolis, MN, USA). An enzymatic assay was used to measure homocysteine (Catch Inc., Seattle, WA, USA). Creatinine was measured by a rate-blanked method that is based on the Jaffé reaction.
Statistical analyses
The mean biomarker levels were compared according to migraine status using analyses of covariance, adjusting for age. The biomarkers were then divided into quintiles based on the biomarker distribution among women who did not report taking postmenopausal hormone therapy, following the guidelines from the Department of Health and Human Services for lipid standardization (22). The cut-points for the highest quintiles were used to define elevated biomarkers for all participants. We used logistic regression to calculate prevalence odds ratios (ORs) and 95% confidence intervals (CIs) for elevated biomarkers according to migraine and migraine aura status as well as for migraine frequency categories. Logistic regression models were adjusted for age (continuous), body mass index (< 25, 25–29.9, ≥ 30 kg/m2), smoking (never, past, current < 15 cigarettes/day, current ≥ 15 cigarettes/day), systolic blood pressure (10-mmHg increments), antihypertensive medication use (yes, no), physical activity (rarely/never, < 1/week, 1–3/week, ≥ 4/week), alcohol consumption (rarely/never, 1–3 drinks/month, 1–6 drinks/week, ≥ 1 drink/day), history of diabetes (yes, no), postmenopausal status (yes, no), postmenopausal hormone use (never, past, current), history of oral contraceptive use (yes, no) and family history of myocardial infarction prior to age 60 (yes, no). We incorporated a missing value indicator if the number of women with missing information was > 100 or imputed a value otherwise. All analyses were performed using SAS version 9.1 (SAS Institute, Cary, NC, USA). All tests were two-tailed and a P-value < 0.05 was considered to be statistically significant.
Role of funding source
The funding agencies played no role in design, conduct, data management, analyses or the preparation of the manuscript of the study.
Results
Table 1 summarizes the baseline characteristics of the 27 626 participants. Mean age was 54.7 years (7.1 SD) and the mean body mass index was 25.9 kg/m2 (5.0 SD). A total of 5087 (18.4%) participants reported any history of migraine, of which 3585 (70.5%) reported active migraine (migraine within the last year) and 1502 (29.5%) reported prior migraine. Of the women with active migraine, 39.7% reported aura, 64.8% reported a migraine frequency of less than six times per year, 10.4% every other month and 24.8% at least monthly. The mean biomarker levels were as expected for this middle-aged cohort of apparently healthy women.
Baseline characteristics of participants in the Women's Health Study (n = 27 626)

Apo A-1, Apolipoprotein A-1; Apo B100, apolipoprotein B100; CRP, C-reactive protein; HDL-C, high-density lipoprotein cholesterol; ICAM-1, soluble intercellular adhesion molecule 1; LDL-C, low-density lipoprotein cholesterol; SD, standard deviation.
To convert cholesterol values to millimoles per litre, multiply by 0.02586.
Table 2 summarizes the age-adjusted mean biomarker levels according to migraine and migraine aura status. Compared with women who did not report a history of migraine, women with any history of migraine had statistically significantly increased levels of total cholesterol, LDL-C, non-HDL-C, Apo B100 and CRP, as well as ICAM-1, and decreased levels of HDL-C. However, the differences in the mean values were only modest with, for example, 3.0 mg/dl differences for non-HDL-C and 0.31 mg/l differences for CRP. When we further subdivided the women who reported any migraine into active MA, active MoA and prior migraine, we found statistically significantly different mean biomarker levels for total cholesterol, LDL-C, HDL-C, non-HDL-C, Apo B100, CRP and ICAM-1. The most unfavourable biomarker profile was noted for women who reported prior migraine, with the exception of CRP, which was slightly higher among women with active MA. However, the differences in the mean biomarker levels were small and unlikely to have meaningful biological relevance.
Age-adjusted mean biomarker levels according to migraine status in the Women's Health Study (n = 27 626)

Apo A-1, Apolipoprotein A-1; Apo B100, apolipoprotein B100; CRP, C-reactive protein; HDL-C, high-density lipoprotein cholesterol; ICAM-1, soluble intercellular adhesion molecule 1; LDL-C, low-density lipoprotein cholesterol.
To convert cholesterol values to millimoles per litre, multiply by 0.02586.
Table 3 summarizes the multivariable-adjusted prevalence ORs and 95% CIs for elevated biomarker levels according to migraine and migraine aura status. Compared with women with no history of migraine, women who reported any history of migraine had adjusted prevalence ORs (95% CI) of 1.09 (1.01, 1.18) for elevated total cholesterol, 1.14 (1.05, 1.23) for elevated non-HDL-C, 1.09 (1.01, 1.18) for elevated Apo B100 and 1.13 (1.05, 1.22) for elevated CRP. No other elevated biomarkers were significantly associated with any history of migraine. The highest significant associations between migraine status and elevated biomarkers were found for women who reported prior migraine ranging from an OR of 1.13 (95% CI 1.00, 1.29) for CRP to an OR of 1.24 (95% CI 1.09, 1.41) for non-HDL-C when compared with women who did not report any history of migraine.

Adjusted for age, body mass index, smoking, systolic blood pressure, antihypertensive treatment, physical activity, alcohol consumption, history of diabetes, menopausal status, postmenopausal hormone use, history of oral contraceptive use and family history of myocardial infarction prior to age 60.
Elevated biomarker level was defined as the highest quintile of that biomarker in women not taking postmenopausal hormone therapy, with values as follows: total cholesterol 242.0 mg/dl, LDL-C 154.0 mg/dl, HDL-C 61.6 mg/dl, non-HDL-C 191.1 mg/dl, Apo A-1 159.9 mg/dl, Apo B100 126.3 mg/dl, lipoprotein (a) 45.3 mg/dl, CRP 4.2 mg/l, fibrinogen 427.6 mg/dl, ICAM-1 411.5 ng/ml, homocysteine 14.0 μmol/l, creatinine 0.83 mg/dl.
P-value from a three-degree of freedom χ2 test.
Apo A-1, Apolipoprotein A-1; Apo B100, apolipoprotein B100; CRP, C-reactive protein; HDL-C, high-density lipoprotein cholesterol; ICAM-1, soluble intercellular adhesion molecule 1; LDL-C, low-density lipoprotein cholesterol.
To convert cholesterol values to millimoles per litre, multiply by 0.02586.
We did not find meaningfully differences of elevated biomarkers with regard to migraine frequency (Table 4). In general, women with a history of migraine who did not report active migraine within the last year (prior migraine) had highest ORs of elevated biomarkers with exception of CRP that was highest for women with a migraine frequency of at least monthly. Statistically significant differences for LDL-C, non-HDL-C and CRP were found. However, the increase in the ORs was again small.
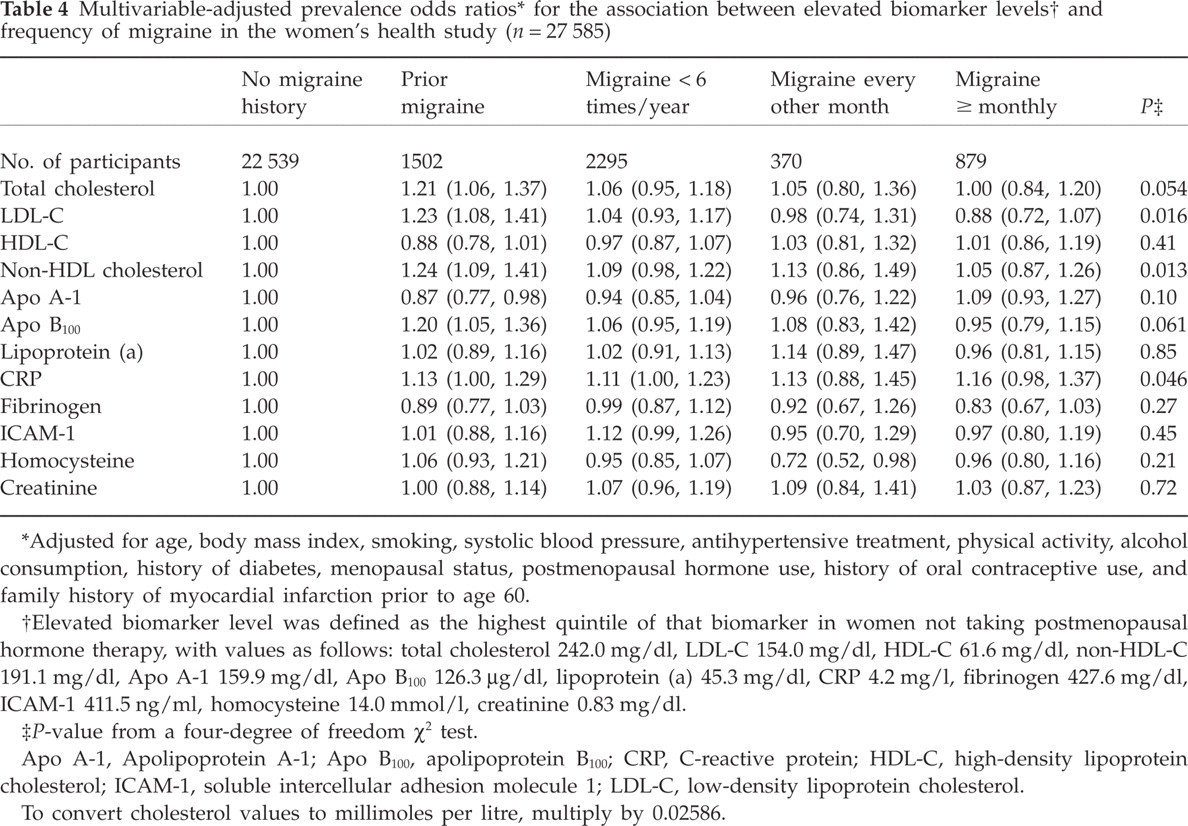
Adjusted for age, body mass index, smoking, systolic blood pressure, antihypertensive treatment, physical activity, alcohol consumption, history of diabetes, menopausal status, postmenopausal hormone use, history of oral contraceptive use, and family history of myocardial infarction prior to age 60.
Elevated biomarker level was defined as the highest quintile of that biomarker in women not taking postmenopausal hormone therapy, with values as follows: total cholesterol 242.0 mg/dl, LDL-C 154.0 mg/dl, HDL-C 61.6 mg/dl, non-HDL-C 191.1 mg/dl, Apo A-1 159.9 mg/dl, Apo B100 126.3 μg/dl, lipoprotein (a) 45.3 mg/dl, CRP 4.2 mg/l, fibrinogen 427.6 mg/dl, ICAM-1 411.5 ng/ml, homocysteine 14.0 mmol/l, creatinine 0.83 mg/dl.
P-value from a four-degree of freedom χ2 test.
Apo A-1, Apolipoprotein A-1; Apo B100, apolipoprotein B100; CRP, C-reactive protein; HDL-C, high-density lipoprotein cholesterol; ICAM-1, soluble intercellular adhesion molecule 1; LDL-C, low-density lipoprotein cholesterol.
To convert cholesterol values to millimoles per litre, multiply by 0.02586.
Discussion
In this large cohort of apparently healthy middle-aged women, we found only modest cross-sectional associations of migraine, migraine aura status, as well as migraine frequency, with elevated biomarkers of CVD. After adjusting for a large number of cardiovascular risk factors and compared with women with no history of migraine, statistically significantly increased prevalence ORs were observed for total cholesterol, non-HDLcholesterol, Apo B100 and CRP for women who reported any history of migraine. The magnitude of association, however, was only modest, with ORs ranging from 1.09 (95% CI 1.01, 1.18) for elevated total cholesterol to 1.14 (95% CI 1.05, 1.23) for non-HDL-C. With regard to migraine specifics, we observed the most unfavourable biomarker profile for women who reported prior migraine, but not for those who reported MA. We also did not find a pattern suggesting an association between migraine frequency and elevated biomarker levels.
Overall, our data do not support a strong biological relationship between biomarkers of CVD and migraine, migraine aura status or migraine frequency. More specifically, our results suggest that these biomarkers are an unlikely explanation for the observed association between MA and CVD in this cohort (7). In this previous report from the WHS, MA was associated with a significant approximately twofold increased relative risk of major CVD, including increased risks for ischaemic stroke, myocardial infarction, coronary revascularization, angina, and death from ischaemic cardiovascular cause. Migraineurs without aura did not have increased risk for any cardiovascular events (7).
The association between migraine and cholesterol as well as HDL-C levels has been previously evaluated in a population-based cross-sectional study from the Netherlands [Genetic Epidemiology of Migraine (GEM) Study] (8). In this study and compared with participants without migraine, the adjusted ORs for migraineurs with aura were 1.43 (95% CI 1.0, 2.1) for total cholesterol ≥ 240 mg/dl, 1.64 (95% CI 1.1, 2.4) for total cholesterol to HDL-C ratio > 5.0 and 1.19 (95% CI 0.8, 1.8) for HDL-C < 40 mg/l. In our study, we found a significantly increased OR for migraineurs with aura for total cholesterol to HDL-C ratio > 5 (OR 1.20; 95% CI 1.05, 1.38) and similar findings for HDL-C < 40 mg/dl (OR 1.10; 95% CI 0.95, 1.28), although our effect estimates were lower. With regard to total cholesterol, our results do not indicate an association with MA. Differences in study design and the fact that the GEM study used IHS-based criteria to confirm migraine and migraine aura cases may explain the divergent findings. However, our results were not meaningfully modified by IHS criteria for migraine (data not shown).
Although migraine has been associated with inflammatory mechanisms (23), the association between migraine and CRP, an indicator for inflammatory processes and a strong predictor for CVD (24), has not been comprehensively studied. In a small case series of 60 migraine patients with complex clinical features, elevated CRP levels of > 3.0 mg/l were found in 43% (25). In the WHS, the proportion of women with CRP > 3.0 among women who reported any history of migraine was 39.8% compared with 36.4% among women who did not indicate a history of migraine. The proportion was highest among women who reported prior migraine (40.2%) and did not differ with regard to migraine aura status.
The association between migraine and fibrinogen levels has been evaluated in a small study of 17 patients with MoA and 11 matched controls (26), in which migraineurs had slightly lower fibrinogen levels. Although in our data we also found statistically significant lower mean fibrinogen values among women who reported any history of migraine compared with those with no migraine history, the difference of 3.5 mg/dl is not biologically meaningful. With regard to ICAM-1, results from a study of 20 migraine patients, 10 patients with tension-type headache and 20 controls without any headache have indicated that ICAM-1 expression was decreased during experimentally induced migraine attacks (27). In our study, no association was found between ICAM-1 and migraine. However, in our study ICAM-1 was not measured conditional on a migraine attack.
Migraine, and specifically MA, has been associated with the C677T polymorphism in the methylenetetrahydrofolate reductase gene (13–15), which is also associated with moderately increased levels of homocysteine (28), a risk factor for CVD. Results from the GEM study have indicated that homocysteine levels were only increased in the subgroup of male T/T homozygote carriers of the polymorphism (13). In our study, neither migraine overall nor MA was associated with increased levels of homocysteine, a finding consistent with results from a small case–control study (29).
To the best of our knowledge, the association between migraine and Apo A-1 and B100, lipoprotein (a) and creatinine has never been evaluated. Other studies have evaluated the association between migraine and prothrombotic or vasoactive factors, including von Willebrand factor (30), factor V Leiden (10), prothrombin factor 1.2 (9), serotonin (11) and endothelin (31), for which we had no measurements available.
Our study has several strengths, including its large size, standardized migraine ascertainment and comprehensive measurements of traditional as well as novel biomarkers of CVD. In addition, information on a large number of other risk factors was available, allowing us to control for potential confounding effects.
Several limitations should be considered. First, information on migraine, migraine aura status and migraine frequency was self-reported and misclassification is possible. However, in previous studies on this cohort, good agreement between migraine classification and modified 1988 IHS criteria for migraine (21) was found (7, 19, 20). Second, our aura definition was broad and we had no further details to classify participants according the IHS criteria for migraine aura. However, our aura prevalence is close to that observed in other large population-based studies (32, 33). Since random misclassification tends to underestimate true associations, we cannot rule out, however, that part of the lack of association is related to this bias. Third, our study was cross-sectional, and thus we cannot say whether migraine influenced biomarkers or vice versa. However, our data do not indicate strong associations between migraine and the various biomarkers of CVD. Fourth, we classified women as having an elevated biomarker when they were in the highest quintile of a specific biomarker compared with all other women (i.e. evaluating a step function). However, when we used multinominal logistic regression models to evaluate a trend across biomarker quintiles, the results were not meaningfully different (data not shown). Fifth, the study cohort was composed of female health professionals, most of whom were White. Thus, generalizability may be limited. However, it is unlikely that a potential biological link between migraine and the evaluated biomarkers differs in the WHS compared with other female populations.
In summary, in this large cross-sectional study of middle-aged women, we observed significant but in strength very modest associations between migraine and total cholesterol, non-HDL-C cholesterol, Apo B100, and CRP. The most adverse biomarker profile was observed among women who reported prior migraine and did not differ substantially with regard to migraine aura status and migraine frequency.
Competing interests
P.M.R. is listed as coinvestigator on patents held by the Brigham and Women's Hospital that relate to the use of inflammatory biomarkers in cardiovascular disease. Full disclosures for each of the authors have been made available to the Editor.
Acknowledgements
The Women's Health Study is supported by grants from the National Heart, Lung, and Blood Institute (HL-43851) and the National Cancer Institute (CA-47988). The research for this work was supported by grants from the Donald W. Reynolds Foundation, the Leducq Foundation and the Doris Duke Charitable Foundation. The authors are indebted to the participants in the Women's Health Study for their outstanding commitment and cooperation, and to the entire Women's Health Study staff for their expert and unfailing assistance.