
Abstract
The aim of this study was to provide data on the prognosis and treatment options of headache associated with sexual activity (HSA). Sixty patients diagnosed with HSA between 1996 and 2004 were followed up between 2003 and 2006 at least 12 months after the first interview. The further course of the disease and their contentedness with therapy were requested. On average, the second interview was performed 35.9 months after the first examination. Of the 45 patients who had suffered from single attacks or bouts prior to baseline examination, 37 had no further attacks. Seven patients suffered from at least one further bout with an average duration of 2.1 months. One patient developed a chronic course of the disease after an episodic start. Of the 15 patients with chronic disease at the first examination, seven were in remission and five had ongoing attacks at follow-up. Ten patients received indomethacin for preemptive therapy, with good results in nine patients. Eighteen patients received β-blockers for prophylaxis, with good results in 15 patients. Episodic HSA occurs in approximately three-quarters and chronic HSA in approximately one-quarter of patients. Even in chronic HAS, the prognosis is favourable, with remission rates of 69% during an observation period of 3 years. For patients with longer-lasting bouts or with chronic HSA, prophylactic treatment with β-blockers or preemptive therapy with indomethacin are often successful.
Introduction
Even though in ancient times Hippocrates described a headache resulting from ‘immoderate venery’ (cited in (1)), it was not until the 1970s that attention was drawn to a benign form of headache occurring during sexual activity (HSA) (2–4). In the first systematic description of the disorder, 21 patients were reported (5). One subgroup had pain which evolved slowly, possibly due to excessive muscular contraction of the neck and jaw muscles. A second, larger group of patients experienced sudden onset of pain shortly before, at the moment of, or shortly after orgasm. Another publication described three patients with a third type whose pain resembled that of the headache following lumbar puncture, perhaps resulting from a tear of the dura during sexual intercourse leading to low cerebrospinal fluid pressure (4). The first edition of the International Headache Society (IHS) classification differentiated these three types of headache associated with sexual activity (HSA types 1–3, respectively) (6). However, the low-pressure type is very rare and must be regarded as a symptomatic headache, so in the second edition only the first two types are defined (Table 1) (7). The exact frequency of HSA is unknown. In the only population-based epidemiological study, the lifetime prevalence was about 1% with a wide confidence interval, similar to the frequency of benign cough headache and benign exertional headache (8). Subarachnoid haemorrhage and cervical arterial dissection must be ruled out when HSA occurs for the first time. Nevertheless, even benign HSA can be a frightening, distressing and disabling disease. Since the first systematic descriptions, several case series or case reports have been published. Patients with one single attack as well as with ongoing repeated attacks have been reported. However, little is known about the options for prognosis and treatment.
International Headache Society diagnostic criteria for primary headache associated with sexual activity

On first onset of orgasmic headache it is mandatory to exclude conditions such as subarachnoidal haemorrhage and arterial dissection.
Methods
We performed a clinical survey at the Department of Neurology of the University of Münster, Germany, which runs a supraregional headache out-patient clinic.
Baseline examination
Between 1996 and 2004, all patients diagnosed with HSA according to the IHS classification were subjected to a structured interview. HSA and coexistent headache disorders were diagnosed after taking the neurological and medical history and after a clinical examination conducted by physicians experienced in headache diagnosis. In all patients, after the first HSA attack or first bout of attacks, secondary headache was excluded by a computed tomography (CT) or magnetic resonance imaging (MRI) scan of the brain and by lumbar puncture. Additional CT or MRI angiography of the brain were performed in 11 patients because of a long interval (>2 weeks) between the last headache attack and the lumbar puncture (n = 8) or initially inconclusive results of the cerebrospinal fluid examination (n = 3). To define the HSA subtype, the patients had to choose among the following items. When the patient stated that the pain started mildly and intensified slowly and gradually with increasing sexual excitement, HSA type 1 was diagnosed. For HSA type 2, a severe headache occurring ‘all of a sudden’ had to be indicated. The patient had to select one of the given items depending on the predominant clinical feature. The previous course of the disease was determined in retrospect.
Follow-up examination
The patients were contacted by telephone between 2003 and 2006 at least 12 months after the first interview. They were interviewed about the further course of the disease and their contentedness with medical therapy applied in the meantime.
Quantitative data are presented as arithmetic means with 1 SD or as percentages. For comparing subgroups, non-parametric tests were used. Quantitative data were compared by Mann–Whitney U-test. qualitative data were compared by χ2 test or Fisher's exact test. The level of significance was set at P < 0.05.
Results
Out of 78 patients diagnosed with HSA between 1996 and 2004, 60 could be contacted by telephone 35.9 ± 21.0 months (12–108 months) later. Thirteen were female, 47 male. Eleven suffered from HSA type 1, 49 from HSA type 2. Fifteen patients were lost to follow-up, two refused a second interview and one had died from myocardial infarction.
Baseline examination
The mean age at baseline examination was 39.8 ± 12.3 years. The mean age at onset was 36.7 ± 11.7 years. Baseline examination took place after the first HSA attack in five patients, after the first bout of attacks in 31 patients and after the second bout of attacks in nine patients. A bout was defined as at least two attacks occurring in ≥50% of sexual activity and then no attack for ≥4 weeks despite continuing sexual activity. The mean duration of bouts was 3.3 ± 5.2 months. Fifteen patients had HSA for a duration of ≥12 months without remission (mean duration 5.9 ± 6.1 years). Of the latter patients, nine had infrequent atttacks (in <20% of sexual activity), three frequent attacks (20–50%) and three regular attacks during nearly all sexual activity. The medical history revealed arterial hypertension in 15 patients (25%). A total of 39 patients had other headache disorders. One additional headache disorder was diagnosed in 22 patients, two in nine patients, three in five patients and four other headache disorders in three patients. Other headache disorders were episodic tension-type headache (n = 18), benign exertional headache (n = 19), migraine (n = 16), chronic tension-type headache (n = 5), cervicogenic headache (n = 2), trigeminal neuralgia (n = 2) and cluster headache (n = 1). Of the migraine patients, 10 had migraine without aura, three migraine with aura and three migraine both with and without aura.
Follow-up examination
The second interview was performed 35.9 ± 21.0 months after the first examination (12–108 months later). Of the 45 patients who had suffered from single attacks or bouts of the disease prior to baseline examination, 37 (82%) had no further HSA. Six patients suffered from one other bout of the disease and one patient from two other bouts, but all were currently free of HSA. Further bouts had a duration of 2.1 ± 3.4 months. One patient who had had one bout of HSA type 2 at baseline examination developed a chronic course of the disease with ongoing attacks in <50% of sexual activity for the duration of 18 months. Of the 15 patients who had HSA for a duration of ≥12 months without remission at baseline examination, three had no further subsequent attacks. Of the 12 patients with further attacks after baseline examination, seven were in remission at follow-up examination and five had ongoing attacks.
Combining the retrospective baseline data about the previous course of the disease and the follow-up data, a disease period of 6.0 ± 5.2 years (1–24 years) was analysed. During this time period, five patient (8%) suffered from one single attack of HAS and 28 (47%) had one bout of the disease. Eight patients (13%) had two bouts and three (5%) more than two bouts. In those patients with initially episodic HSA (n = 45), the calculated relapse rate was 0.06 per year (16 relapses in 270 disease-years), the risk of developing chronic HSA 2.2%. In episodic HSA (n = 44), the risk of relapse during the overall observation period was not different in patients without additional headache disorders (n = 15, five with relapses) compared with patients with migraine (n = 12, three with relapses, P = 1.0), with patients with exertional headache (n = 15, four with relapses, P = 0.72), with patients with tension-type headache (n = 16, two with relapses, P = 0.28), or with patients with other headache disorders in general (n = 29, six with relapses, P = 0.47). Of the 16 patients (27%) with a chronic course of the disease, 13 had infrequent attacks (in < 50% of sexual activity) and three frequent attacks (in >50% of sexual activity).
Acute treatment with 25–50 mg indomethacin showed good results in three patients and limited success in two. Other non-steroidal anti-inflammatory agents (acetylsalicylic acid, n = 12; ibuprofen, n = 7; paracetamol, n = 4; diclofenac, n = 2) for acute therapy were of limited or of no value in most patients. Four patients reported experiences with triptans for acute treatment. One patient experienced good results with sumatriptan s.c. and zolmitriptan i.n., another patient with almotriptan p.o.; two patients had no success with zolmitriptan p.o. and sumatriptan s.c., respectively.
For preemptive therapy, 10 patients had received indomethacin (25–50 mg, intake 30–60 min prior to sexual activity). Nine patients reported good results and one limited success of this treatment. The frequency of successful preemptive treatment with indomethacin ranged from two to >30 times (median eight times). One patient received ibuprofen for preemptive therapy with limited success, two diclofenac without success and one patient naratriptan without success.
Prophylactic treatment with β-blockers was given in 18 patients (propranolol = 13, metoprolol = 4, bisoprolol = 1, non-permanent treatment n = 14, mean treatment duration 4.5 ± 6.2 months, 2 weeks to 24 months, permanent treatment in four patients because of arterial hypertension). The dose was 60–240 mg for propranolol, 50–200 mg for metoprolol and 5 mg for bisoprolol. Fifteen patients reported good results, one limited success and two no success of β-blocker prophylaxis. Other drugs applied for prophylaxis were carbamazepine, oxcarbazepine, tizanidine and losartan (for each n = 1), all without success.
The patients' contentedness with indomethacin preemptive therapy and β-blocker prophylaxis depending on HSA subtype and β-blocker subtype is shown in Table 2.
Patient satisfaction with indomethacin for preemptive therapy and with β-blockers for prophylaxis (number = HSA type 1 and type 2, proportion of HSA type 1 given in parentheses)

Comparison of HSA subtypes
In Table 3, a comparison of HSA type 1 and type 2 is presented. There was no significant difference regarding sex, age at onset or concomitant arterial hypertension between either subtype. The proportion of episodic vs. chronic courses, the relapse rate in episodic courses and the remission rate in chronic courses did not differ significantly between HSA subtypes.
Comparison between patients with HSA types 1 and 2

Comparison of episodic and chronic HAS
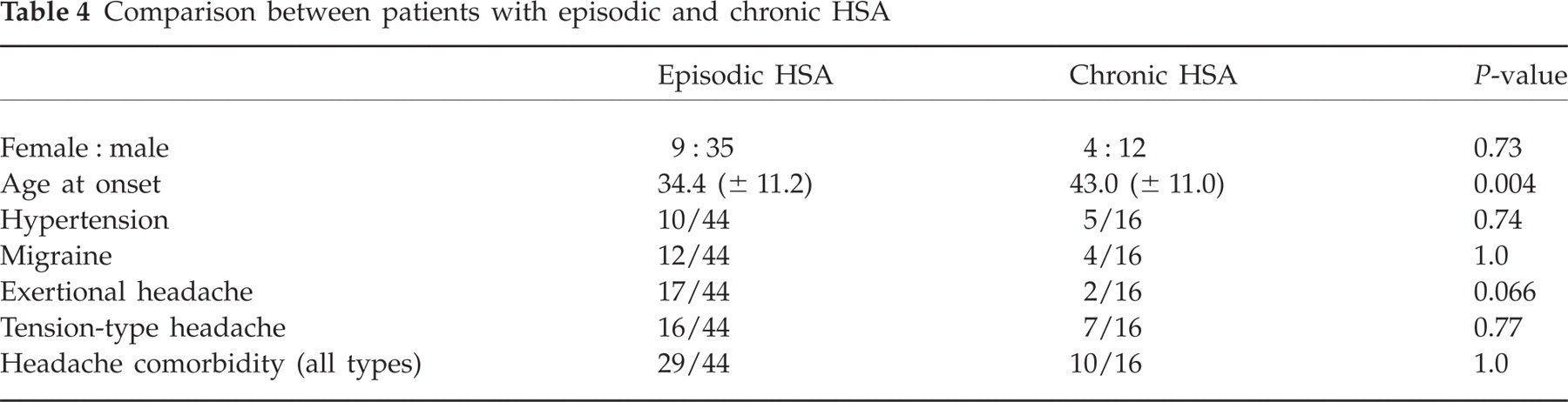
Table 4 shows a comparison of patients with an episodic and a chronic course. Patients with episodic HSA had an earlier age at onset and tended to suffer more often from concomitant exertional headache. No significant differences were found regarding sex, concomitant arterial hypertension or other concomitant headache disorders.
Comparison between patients with episodic and chronic HSA
Discussion
HSA has been regarded as a disease with a completely unpredictable clinical course. According to our data, there seem to be two different temporal patterns of HAS: an episodic course with remitting bouts and a chronic course. This is similar to other primary headache disorders such as cluster headache or paroxysmal hemicrania. Following the definition of episodic cluster headache, we defined a bout as at least two attacks occurring in ≥50% of sexual activity and then no attack for ≥4 weeks despite continuing sexual activity. The chronic course was defined as ongoing HSA attacks for ≥12 months without remission of ≥4 weeks. Applying these criteria, episodic HSA was diagnosed in approximately three-quarters and chronic HSA in approximately one-quarter of our patients. Changeover between the two courses of the disease was a rare event in our patients, with only one patient developing chronic HSA after an episodic start of the disease.
In most patients, HSA is a disease of limited duration occurring in bouts. We are aware of two other studies focusing on the prognosis of HSA (9, 10). In two follow-up studies of 30 and 26 patients, respectively, there were recurrence rates of 33% and 50% after follow-up periods of approximately 6 years (9, 10). Combining episodic and chronic HSA, our study found a very similar recurrence rate of 43% for the overall observation period of an average of 6 years. The presence of concomitant primary headache syndromes (migraine or tension-type headache) was hypothesized to be a risk factor for recurrence of HSA (9). Our study carefully documented concomitant headache syndromes, but could not confirm such a relationship (for migraine, for tension-type headache or for exertional headache). The most frequent concomitant headache disorder was benign exertional headache, which possibly shares similar pathomechanisms with HSA (10). However, concomitant exertional headache and an early onset of the disease seem to be associated with an episodic course of HSA, whereas a later onset of the disease seems to be associated with a chronic course.
HSA attacks are usually short lasting without need for acute medical treatment but the duration of pain varies widely (11). About 15% of patients suffer from severe pain for >4 h up to 24 h, necessitating effective acute treatment. Regarding different treatment modalities, data on acute treatment is the least valid due to the variable duration of headache and missing information on the number of treated attacks and the exact time of administration. Nevertheless, of all non-steroidal anti-inflammatory agents, only indomethacin showed positive results in some patients and can be recommended for acute treatment. Based on anecdotic reports, indomethacin has also been suggested for preemptive therapy of HSA (12, 13). Our study supports this, showing good results in 90% of our patients. Triptans for acute treatment and for preemptive therapy seem to be an alternative option for those patients not tolerating indomethacin. For triptans with low absorption rates (such as naratriptan), earlier administration >60 min before sexual activity might be favourable. Our detailed experiences with triptans in HSA treatment have recently been published (14).
For those patients with longer lasting bouts or with a chronic course of the disease, prophylactic treatment can be indicated. The largest previous case series dealing with prophylactic treatment reported eight patients with HSA type 2 completely relieved by propranolol (15). Another small case series has supported the use of propranolol in HSA (16). On the other hand, there have also been reports on treatment failure with propranolol (4, 10, 17). Our data emphasize the use of propranolol for prophylaxis of HSA with success rates of approximately 80%. Metoprolol seems to be an equivalent alternative. We are aware of the limitations of our study due to the open and retrospective design. However, we believe that the absence of controlled studies legitimizes our empirical approach to the treatment of HSA. From our experience, β-blockers (propranolol or metoprolol) for prophylaxis and indomethacin for preemptive therapy can be recommended. The optimal dose for β-blockers seems to be similar to that usually used in migraine. Data on HSA type 1 are limited, but there seems to be no substantial difference from HSA type 2 concerning the prognosis and treatment options. For prophylaxis, a short course (2–6 months) seems adequate because spontaneous remissions of HSA are frequent.
Competing interests
None to declare.