
Abstract
Epidemiological data on trigeminal unilateral autonomic symptoms in patients with migraine are scarce. The authors wanted to provide a population-based evaluation of the prevalence of unilateral autonomic features in migraine patients and an assessment of the expression of unilaterality of autonomic symptoms and head pain in patients with UAs compared to other migraine patients. A population based sample of 6000 inhabitants of the city of Essen in Germany was screened using a previously validated standard questionnaire. Three thousand three hundred and sixty subjects (56% of a total 6000) responded. 841 subjects had migraine, out of which 226 reported accompanying unilatral auetonomic symptoms (26.9%, CI 95% [23.9-30%]). Unilateral autonomic symptoms in patients with migraine are common and have been widely underestimated in the past. One out of four migraine patients regularly experiences one or more unilateral autonomic symptoms during their attack. Migraine patients with accompanying autonomic symptoms seem to experience their pain more unilateral and more severe than non-UA patients.
Keywords
Introduction
Migraine is a common, chronic, incapacitating, neurovascular disorder usually accompanied by autonomic symptoms such as nausea and vomiting. Cluster headache is a much less common headache disorder with strictly unilateral pain and shorter lasting attacks associated with one or more of the following ipsilateral symptoms: conjunctival injection, lacrimation, nasal congestion, rhinorrhoea, forehead and facial sweating, miosis, ptosis and eyelid oedema.
Clinical practice and several studies have shown an overlap of autonomic symptoms in cluster headache and migraine suggesting a common final pathway of these two different disorders. The clinically observed good response to triptans in both disorders may be associated with large-scale recruitment of peripheral neurovascular 5-HT1B/1D receptors specifically blocking plasma extravasation from blood vessels in the dura mater (1).
Unilateral cranial autonomic symptoms (UAs) such as lacrimation, conjunctival injection, eyelid oedema and nasal congestion are typical features of trigemino-autonomic cephalalgias (TACs) (2), but are frequently also reported by patients with migraine and often accompany the typical autonomic features of the migraine attack (3–5). It has been postulated that the presence of UAs may predict a positive response to triptans due to possible activation of the trigeminal autonomic reflex (6). A systematic assessment of frequency and clinical characteristics of these patients was done only recently, yielding a total of 45.8% of migraine patients with at least one UA in a tertiary headache centre (7–9). To date, there are no data on prevalence of unilateral autonomic features in patients with migraine in the general population.
The aim of this study was to provide a population-based evaluation of the prevalence of unilateral autonomic features in migraine patients and to assess whether the expression of unilaterality of autonomic symptoms as well as the unilaterality of head pain is more pronounced in patients with UAs compared with other migraine patients. Moreover, we tried to identify whether pain intensity of the migraine attack in patients with UAs is stronger compared with non-UA migraine patients.
Methods
Data collection
The current study was a part of an epidemiological survey of the German Headache Consortium which investigates prevalence and incidence of headache syndromes in the general German population.
Data for this study were collected during a baseline survey from December 2003 to November 2004. The study population comprised a random sample of 6000 inhabitants of the city of Essen, a town in the industrialized Region of North Rhine-Westphalia in the western part of Germany. The town covers an area of 210 360 km2 and has 585 481 inhabitants, including 305 726 women and 279 755 men. Inclusion criteria were: age 18–65 years and proper command of the German language.
Epidemiology
Figure 1 illustrates the screening procedure. Six thousand randomly selected subjects received a questionnaire per postal mail and, in a case of non-response, a subsequent reminder 2 weeks later. Subjects who did not respond were called and asked for an interview over the phone which was performed by trained medical students based on the same questionnaire. After eight unsuccessful calls subjects were considered non-responders. Individuals who refused the interview either by postal response or by phone were also considered non-responders.

Epidemiological screening procedure.
Questionnaire
The questionnaire has been constructed based on the criteria of the International Headache Society (IHS) (10) and validated prior to the survey. The data on validation of the questionnaire will be reported separately. Briefly, 278 consecutive patients with migraine (n = 97) or tension-type headache (n = 60), or a combination of migraine and tension-type (n = 23) headache as well as patients with cluster headache (n = 98), and healthy subjects (n = 30) were asked to fill out the questionnaire twice, before and after 4 weeks. All patients were examined by a neurologist.
Evaluation of the questionnaire revealed that sensitivity for migraine was 73.20%, specificity 96.13%, positive predictive value (PPV) 91.93%, negative predictive value (NPV) 87% and the likelihood ratio was 18.93.
Unilateral autonomic symptoms
The ‘migraine’ part of the questionnaire included six questions. The following unilateral autonomic symptoms were included in the questionaire:
Ipsilateral conjunctival injection
Ipsilateral tearing
Ipsilateral nasal congestion or rhinorrhoea
Ipsilateral eyelid oedema
Ipsilateral miosis or ptosis
Ipsilateral forehead or facial sweating
Patients with multiple UAs were identified and the number of UAs per patient was correlated to the expression of unilaterality of their respective migraine attack. In this regard, we also screened for a possible correlation of the number of UAs to the individual severity of pain experienced during the attack.
Statistics
Patients reporting at least one of the above symptoms during the attack were considered migraineurs with UAs, while remaining patients were considered migraineurs without UAs. The demographics and clinical features with and without UAs were compared by means of Student's t-test for unpaired data and χ2 test. All analyses were performed using SPSS 13.0 (SPSS Inc. Chicago, IL, USA).
Results
Initial sample
The study sample comprised 6000 subjects including 2971 (49.5%) men and 3029 (50.5%) women. Mean age was 44.7 ± 12.7 years. Distribution of gender and age was similar to that of the population of the region of ‘North Rhine-Westphalia’.
Responder
The overall response rate was 3336 out of 6000 contacted persons. Two thousand and four subjects (33.4%) responded per mail, 1332 (22.2%) were interviewed by phone, 2181 (35.1%) could not be reached, 549 (9.2%) refused and 14 (0.2%) were dead. Comparing ‘postal mail’ vs. ‘telephone’ responders we did not find significant differences. Only those patients were considered to have probable migraine who fulfilled the IHS time criterion for the duration of a migraine attack of 4–72 h (8).
Responders were slightly older than non-responders (mean age 46.3 ± 12.7 vs. 42.8 ± 12.4 years, NS) and consisted of more women (53.7% vs. 46.4%). Comparison of subjects who responded by mail with those who were interviewed by phone did not reveal significant differences (45.5 ± 12.7 vs. 47.5 ± 12.7 years, 55.4% vs. 51.3% women).
Unilateral autonomic features
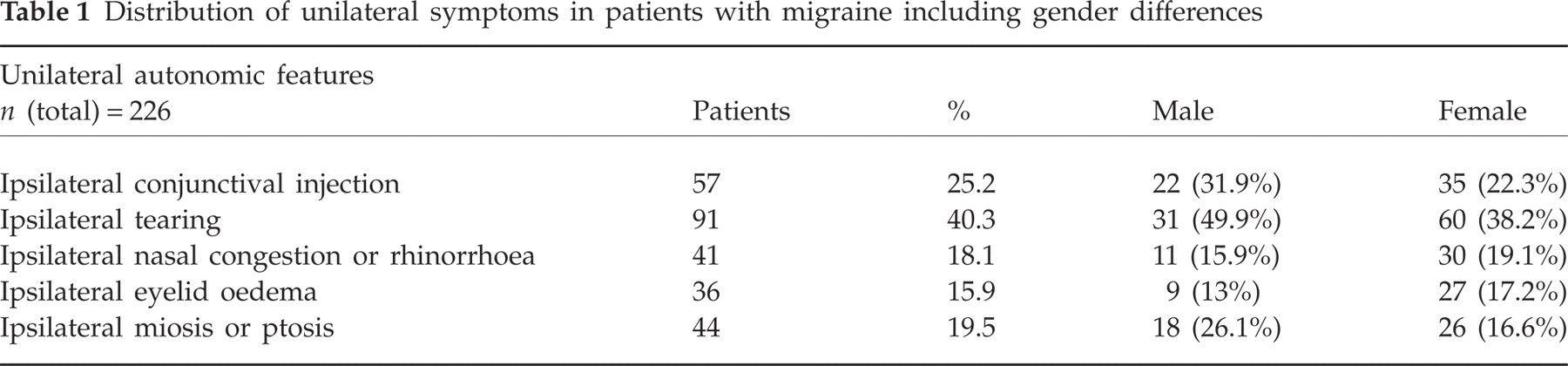
We found 841 (25.2%) persons with migraine (male = 252, mean age 43.27 years, range 21–65 years; female = 589, mean age 44.41 years, range 20–65 years), of whom 226 (26.9%; male 30.5%, female 69.5%; M:F ∼2 : 1) reported having at least one unilateral autonomic feature during their migraine attack regularly (male 69, age 43.54 years, range 21–65 years; female 157, age 46.00 years, range 20–65 years) (see Table 1).
Distribution of unilateral symptoms in patients with migraine including gender differences
Of these 226 migraine patients, 43.4% (male 38.3%; female 45.8%) reported having only one UA during the migraine attack regularly; 34.3% (male 40.4%; female 31.3%) reported having two, 15.4% (male 12.8%; female 16.7%) had three, 4.9% (male 6.4%; female 4.2%) had four and 2.1% (male 2.1%; female 2.1%) reported having five UAs during their migraine attack (see Fig. 2).

Distribution number of unilateral cranial autonomic symptoms (UAs) in patients with migraine in percent (n = 226).
Migraine patients with UAs experienced their head pain significantly more often unilaterally (38.5%; male 36.2%, female 45.8%) than non-UA patients (20.1%; P = 0.000) (see Fig. 3).
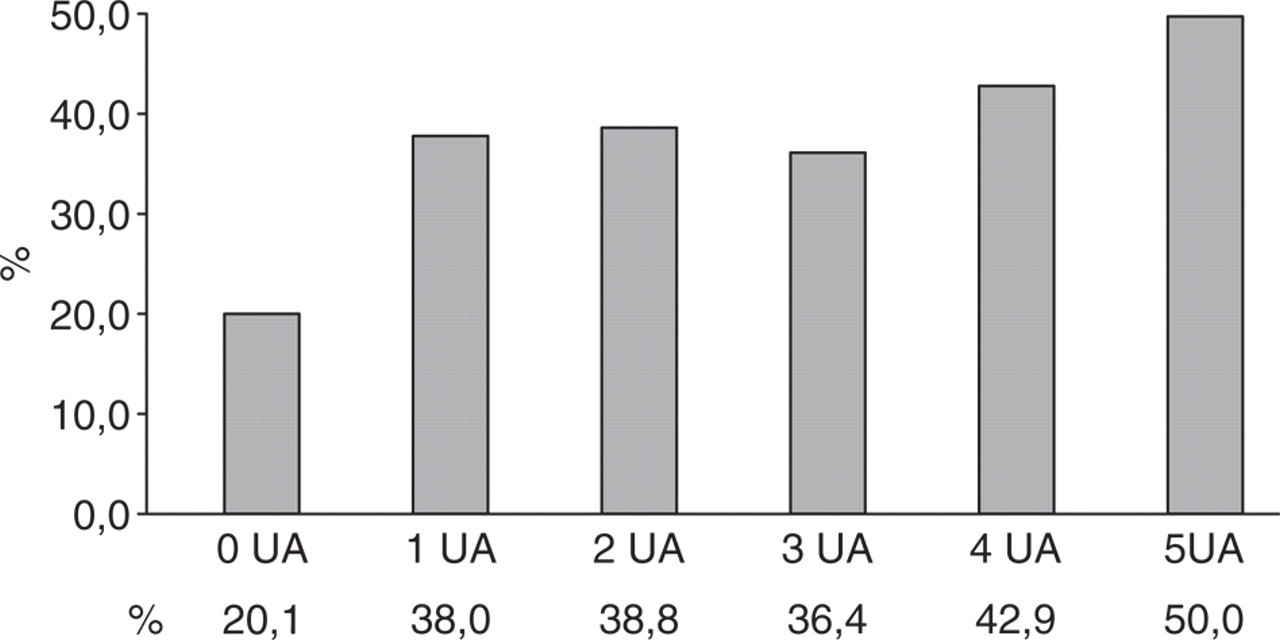
Distribution of unilateral expression of migraine symptoms in patients with unilateral cranial autonomic symptoms (UAs) in percent.
Patients with UAs experienced a significantly greater increase in pain intensity during a migraine attack compared with non-UA migraine patients [mean visual analogue scale (VAS) score 7.4 vs. 5.2; P = 0.034). No reasonable pattern was observed in the correlation of the amount of UAs to pain intensity in this respect.
Discussion
We used a combination of postal mail and telephone interviews achieving an acceptable response rate of 56%. Comparison of demography of responders and non-responders showed a trend toward a selection bias, which, however, is not uncommon in population-based surveys. Nevertheless, the differences did not reach the level of statistical significance. Finally, the distribution of genders across different age groups is comparable to the general population of the region of North Rhine-Westphalia. Hence, we think that with a reasonable approximation the studied sample can be considered representative for the general population in Germany.
The study achieved its main goal of estimating the prevalence of unilateral autonomic symptoms in patients with migraine in a representative population sample in Germany. We investigated 3336 subjects and found 841 (25.21%) subjects with migraine, of whom 226 [26.9%, 95% confidence interval (CI) 23.9, 30)] reported having at least one UA during their migraine attack regularly. Patients with UAs experience their headache more strictly located on one side and more severe than patients without UAs. There is a weak correlation between the number of UAs and pain severity in migraine patients.
There were a number of case reports addressing UAs in migraine, until Barbanti et al. conducted a systematic trial reporting the clinical features and frequency of these symptoms in a tertiary referral centre in Rome, Italy. They investigated 177 consecutive migraine patients and found UAs in 81 (45.8%) patients, which is almost double what we could find in our population-based setting. This discrepancy in UA prevalence is probably due to the selection bias a tertiary headache centre would have naturally.
Headache specialists are familiar with the occurrence in clinical practice of unilateral autonomic symptoms in patients with migraine. These features seem to be much more common than generally assumed. It is possible that migraine and cluster headache share a common pathway in the development of autonomic symptoms and head pain that might include functional alterations in hypothalamic or brainstem circuits (5). As one contributing factor, it has been postulated that pain intensity may correlate positively to the development of autonomic symptoms (7), i.e. the stronger the pain, the more likely the development of UAs. However, we found only a weak correlation between pain intensity and the number of UAs.
Even though the prevalence of unilateral autonomous symptoms in migraine patients seems to be much more common than previously expected, its pathophysiological origin is still not entirely understood. Migraine involves dysfunction of brainstem pathways that normally modulate sensory input. The trigemino-vascular reflex is most strongly expressed in patients with TACs, but also exists in normal persons (9) and may be active in patients with migraine (10). It consists of functional connections between trigeminal afferences and parasympathetic efferences. In migraine patients only the trigeminal afferent arm is active, while patients with UAs also show activation of the efferent arm of the trigeminal-autonomic reflex (7). Pain might work as a trigger for the occurrence of UAs. There could be a particular threshold for pain, after which the trigeminal system causes parasympathetic overflow leading to activation of the trigemino-vascular reflex and consequently to UAs, even though other trigger mechanisms have to be considered, as there are reports of UAs occurring without pain (11, 12).
Activation of the trigeminal autonomic reflex is probably associated with large-scale recruitment of peripheral neurovascular 5-HT1B/1D receptors, the target of contemporary acute migraine treatment with triptans. Previous open studies have reported responder rates after triptan administration in UA migraineurs of 30.6% after 1 h and 61.1% after 2 h (6) compared with all migraine patients ranging from 12.9 to 17% after 1 h and 42.1 to 52% after 2 h (9, 13). The overall pain-relief response seemed to be better in patients with UAs compared with the general migraine population. The authors suggested that unilateral autonomic symptoms could have a true predictive value in the complex issue of triptan response in migraineurs (6).
An even more pressing question in this regard would be whether UAs may have a predictive value in the use of prophylactic medication in migraine. Headache specialists often have a considerable range of prophylactic agents for migraine, such as β-blockers (propranolol, timolol, metoprolol), tricyclic antidepressants (amitriptyline), calcium channel antagonists (flunarizine), serotonin receptor antagonists and anticonvulsants (valproate, topiramate), with uncertain treatment success in the individual patient without knowing beforehand which substance helps which patient best. Would migraineurs with UAs benefit more from cluster headache prophylactic medication such as verapamil or lithium? Should prophylactic treatment of migraine patients with UAs concentrate on substances that have proven to work considerably well in both conditions, such as topiramate (14, 15)? The pathophysiological mechanisms of these substances are still unclear. To the best of our knowledge there are no studies that address the correlation of UAs and its impact on the prediction of prophylactic medication usage. Longitudinal assessment of UA patients' prophylactic medication will be the next step in our investigation, since we were not able to gather data on the prophylactic medication effect over time in the current study.
Limitations to our study are: (i) selection bias possibly leading to a higher migraine prevalence, which cannot be controlled properly in a self-reporting design. The influence of this selection bias on the true prevalence of UAs in the population of migraine patients remains hypothetical; (ii) self reporting of certain unilateral autonomic symptoms may be imprecise and incomplete, as patients may not have the proper necessary diagnostic ability, especially for symptoms such as miosis and ptosis; (iii) we failed to acquire pharmacological sensitivity in this study.
Conclusions
Unilateral autonomic symptoms in patients with migraine are common and have been widely underestimated in the past. One out of four migraine patients regularly experiences one or more unilateral autonomic symptom during their attack. Migraine patients with accompanying autonomic symptoms seem to experience their pain more unilaterally and more severely than non-UA patients.
More scientific research is necessary in order to unravel the pathophysiological mechanisms associated with migraine and accompanying autonomic symptoms, as well as the pharmacological impact of prophylactic antimigraine medication on migraine patients with and without UAs.
Acknowledgements
This research project was funded by the German Federal Ministry for Education and Research.