
Abstract
Headache and recurrent abdominal pain (RAP) are common disorders in children and adolescents, frequently referred to paediatricians. Both disorders show similarities in trigger and comorbid factors, their burden on family and individual life, and a paroxysmal trend with risks of chronicization over time. However, very few studies have compared directly headache and RAP. The main aim of this study was to compare the psychological profile of headache and RAP patients vs. healthy controls. A total of 210 children and adolescents [99 boys, 111 girls; age range 4-18 years; mean age (m.a.) = 11.04, SD 4.05] were assessed: 70 headache patients (m.a. 12.4 years; SD 2.9; F = 35, M = 35), 70 RAP patients (m.a. 9 years; SD 3.6; F = 30, M = 40) and 70 controls (m.a. 11.7 years; SD 4.6; F = 46, M = 24). The diagnoses had been made according to international systems of classification both for headache (ICHD-II criteria) and RAP (Rome II criteria). The psychological profile had been made according to the Child Behaviour Checklist 4-18 (CBCL). ANOVA one-way analysis was used to compare CBCL scales and subscales between groups. Headache and RAP showed a very similar trend vs. control for the main scales of the CBCL, with a statistically significant tendency to show problems in the Internalizing scale (anxiety, mood and somatic complaints) and no problems in the Externalizing (behavioural) scale. Only for the Attention Problems subscale migraineurs showed a significant difference compared with RAP. In conclusion, headache and RAP show a very similar psychological profile that should be considered not only for diagnostic and therapeutic purposes, but also from the aetiological aspect.
Introduction
Recurrent abdominal pain (RAP) without organic cause and primary headache are common paediatric problems.
Diagnostic criteria for RAP were proposed in the 1950s by Apley and Naish (i.e. at least three episodes of abdominal pain occurring over a period of at least 3 months and severe enough to affect the activities of the child) (1). The term ‘recurrent abdominal pain’ has being progressively dismissed, even though it is still used in clinical and scientific work. In 1999, the International Classification of Functional Gastrointestinal Disorders (FGIDs) (Rome-II criteria) was published (2), providing diagnostic criteria for childhood FGIDs. The diagnosis of RAP according to Apley and Naish criteria (1) was excluded, because they were seen to be too general and fulfilling criteria for other FGIDs [functional dyspepsia, irritable bowel syndrome (IBS) and functional abdominal pain (FAP)], all included in the category of abdominal pain (2). This diagnostic category encompasses five subcategories (functional dyspepsia, IBS, FAP, abdominal migraine and aerophagia). According to the main aim of our study, we considered only IBS and FAP, continuing to use the term RAP to refer to both of them.
It is surprising how many features RAP and headache share in different areas: (i) a high prevalence in children: headache and RAP are most common childhood somatic complaints (3–10); (ii) migraine shows a slight prevalence in males <10 years old (11, 12) and increases with age (13). From the pubertal period on the prevalence in girls is markedly greater than in boys (3, 14–18); (iii) headache is a familial phenomenon (3, 11, 12, 19). Children with RAP often have at least one parent who also suffers from FAP (14, 16, 18); (iv) paroxysmal trend and heterogeneous symptoms, with clinical features that may suggest severe organic pathology: a differential diagnosis is needed by instrumental examinations (3, 20–22); (v) risk of life-time duration (18, 23–25); (vi) burden on the quality of life and high (personal and familial) costs (6, 17, 26–29); (vii) influences of psychological triggering factors (3, 6, 8, 29–31); (viii) parental characteristics and response to childhood pain (18, 26, 27). Poor family atmosphere: severe familial disorder, stress, conflict or tension at home (3, 26, 30, 32, 33); (ix) common personality characteristics: fearful of novelty, prone to separation concerns, shy and withdrawn (3, 27, 34–36); (x) psychiatric comorbidity: mainly anxiety and depression (8, 16, 18, 37, 38); (xi) a role for serotonin has been suggested in both conditions (4, 38–40).
On one hand, several studies have stressed the co-occurrence of headache and RAP in children (4, 5, 18, 26, 39), although comorbidity rates vary widely from 14% to 90% (36). Studies comparing RAP patients with control groups have found a higher incidence of headache in the RAP group (18, 36). On the other hand, adbominal pain in children with migraine has been reported to occur in 50% of cases (5); moreover, other somatic complaints in children have been reported more often than non-migrainous headache (5, 39).
The diagnosis of ‘abdominal migraine’ has been used to describe RAP associated with a personal or familial history of migraine, even if the child does not complain of head pain during the attack of abdominal pain (5, 22, 36). Abdominal migraine has been recognized by the International Classification of Headache Disorders (ICHD-II) (22) and Rome-II criteria also (2).
Despite these similarities, few studies have directly compared RAP and headache and few have compared both conditions by the psychological point of view (3, 41). Adult psychiatric literature mentions headache and gastrointestinal complaints as symptoms of somatoform disorders, stressing indirectly both the reciprocal link and the involvement of psychological factors (42).
Headache and RAP have been associated with a variety of personal factors such as emotional stressors and physical antecedents: personal anger, disputes, family condition (3, 6, 26, 33). Somatization in children and adolescents has been associated with chronic physical illness or disability in a parent (37, 43).
Children with frequent complaints of pain and a history of medical visits for unexplained symptoms are more likely to have emotional and behaviourial problems (4, 16, 27, 36, 38, 39, 44–46). These studies agree that anxiety and mood disorders (internalizing disorders) are more prevalent in headache and RAP patients than externalizing disorders (e.g. conduct or behaviour disorders) (10). This topic needs attention because of its diagnostic and therapeutic implications.
The main aim of this study was to compare the occurrence of internalizing and externalizing disorders in headache, RAP and a control group. To the best of our knowledge, this is the first controlled study analysing the occurrence of psychological disorders in headache and RAP adopting international systems of classification for both conditions, and assessing the psychological profile using a standardized questionnaire.
Many studies (8, 38, 45, 47–49) have evaluated internalizing problems in childhood headache by the Child Behaviour Checklist 4–18 (CBCL/4–18) (50), but few (38, 44, 47, 49) have investigated the differences in emotional and behavioural problems across different headache subtypes.
This the first study to employ CBCL/4–18 (50) in childhood headache examining all migraine and tension-type subgroups according to ICHD-II criteria (22).
Methods
Headache and RAP diagnoses
Data on the clinical characteristics of headache were collected by a standardized questionnaire. Neurological examinations were performed by child neurologists under the supervision of the Head of the Headache Centre (V.G.). The final diagnoses were made according to ICHD-II (2004) (22).
We included only migraine and tension-type headache (TTH) diagnoses. Participants meeting all but one of the diagnostic criteria for a given headache subtype were classified as ‘probably’ having that headache type. Those diagnosed as migraine or probable migraine were considered to have migraine and those classified as TTH or probable TTH were considered to have TTH.
We excluded secondary headache, typical aura with non-migraine headache (N = 1, ICHD-II code 1.2.2), cluster headache (N = 1, ICHD-II code 3) and tension-type mixed with migraine (N = 4).
We did not distinguish TTH associated with pericranial tenderness (ICHD-II: 2.1.1; 2.2.1; 2.3.1) from TTH not associated with pericranial tenderness (ICHD-II: 2.1.2; 2.2.2; 2.3.2) (22).
RAP diagnoses were made according to Rome-II criteria (2).
The study included two diagnoses of abdominal pain among the five foreseen by the Classification of Functional Gastrointestinal Disorders: functional abdominal pain (G2c) and irritable bowel syndrome (G2b). We excluded functional dyspepsia (G2a), abdominal migraine (G2d), aerophagia (G2e) and all organic abdominal pain. Patients with headache did not have RAP and patients with RAP did not have headache.
Inclusion criteria for the control group were: headache and abdominal pain less than once per month, matched age, absence of other chronic pathologies.
Psychological evaluation
The assessment tool was the CBCL/4–18 (47). The CBCL is a parent-rating scale to assess competences, emotional and behavioural problems in children and adolescents aged 4–18; it is an easy-to-administer measure which takes about 20–30 min to complete. The questionnaire consists of two parts: ‘Competences’ and ‘Emotional and Behavioural Problems’ scales. In the first section, social competence is covered by three scales: Activity scale, Social scale and School scale.
According to the main aim of our study, we administrated only the second section of CBCL, because it deals with internalizing and externalizing disorders; moreover, Competences scale can be administrated only in schoolchildren (from 6 years). Multivariate analyses have identified two main group problems: ‘Internalizing scale’ (anxious and inhibited behaviour) and ‘Externalizing scale’ (aggressive and antisocial behaviour).
The second section assesses the psychological profile by a dimensional approach. Parents judge 118 items, according to different categories (each scored from 0 to 2): ‘not true’ (0), ‘somewhat true’ (1) or ‘always or often true’ (2).
Items are grouped in eight narrow-band subscales: ‘Withdrawn’, ‘Somatic complaints’, ‘Anxious/depressed’ (these first three scales are summarized under ‘Internalizing scale’), ‘Delinquent behaviour’, ‘Aggressive behaviour’ (summarized under ‘Externalizing scale’), ‘Thought problems’, ‘Social problem’ and ‘Attention problems’ (designated as neither ‘Externalizing’ nor ‘Internalizing’). Thirty-three items that could not be assigned to any of these scale are called ‘Other problems’. The sum of all items forms the ‘Total score’.
The CBCL was administered only to the mother, as the parent who usually spends more time with the children.
Subjects
A total of 210 children and adolescents [99 boys, 111 girls; age range 4–18 years; mean age (m.a.) = 11.04; SD 4.05] were assessed: 70 headache patients (m.a. 12.4 years, SD 2.9; F = 35, M = 35), 70 RAP patients (m.a. 9 years, SD 3.6; F = 30, M = 40) and 70 controls (m.a. 11.7 years, SD 4.6; F = 46, M = 24). Children were stratified in two age groups: 4–11 and 12–18 years (Table 1), as proposed by Achenbach (50).
Description of the three samples

FAP, Functional abdominal pain; IBS, irritable bowel syndrome; ETTH, episodic tension-type headache; CTTH, chronic tension-type headache; MA, migraine with aura; MoA, migraine without aura; RAP, recurrent abdominal pain.
Headache patients were consecutively enrolled from the Child and Adolescent Headache Centre and 70 children with RAP were recruited from the Department of Paediatric Gastroenterology of the University of Rome ‘La Sapienza’.
The control group had been recruited from different schools in Rome: inclusion criteria were the absence of headache and RAP (less of one episode every 2 months over the past 2 years).
Of headache patients, 42 (60%) had migraine and 28 (40%) TTH.
According to ICHD-II (22), 27 had migraine without aura (MoA, 1.1), eight probable MoA (1.6.1), five had migraine with aura (MA, 1.2) and two probable MA (1.6.2); among TTH patients, 16 had chronic tension-type headache (CTTH, 2.3), two probable CTTH (2.4.3), eight episodic TTH (2.2) and two probable episodic TTH (2.4.2).
The RAP group comprised 38 (54%) FAP (G2c) and 32 (46%) IBS (G2b) patients.
No sex differences in headache samples were seen: 35 were boys and 35 girls. According to headache subtypes, the migraine group was composed of 24 (57%) boys and 18 (43%) girls; the TTH group included 11 (39%) boys and 17 (61%) girls. The RAP group showed a slight prevalence of boys (M = 40; F = 30): 24 (60%) had FAP and 16 (40%) IBS.
Statistical analysis
Statistical evaluation was performed using Statistical Package for the Social Sciences (SPSS 12.0) software (SPSS Inc., Chicago, IL, USA).
Raw scores were analysed according to Achenbach, whose ‘raw scores can reflect greater differentiation among nondeviant subjects than T scores can on these scales’ (50).
Data were analysed in three stages: first, headache, RAP and control groups were compared without any distinctions in headache and RAP subtypes; second, control, migraine, TTH, FAP and IBS groups were compared; finally,
Duncan's post hoc test was used to detect any differences among groups. The level of statistical significance was set at P < 0.05.
The descriptive values were expressed as means, SD and percentages.
Results
Headache, RAP and control group: comparison between scales and subscales
The headache and RAP groups differed from the control group in the Internalizing scale of CBCL: by

Mean and SD of headache, recurrent abdominal pain (RAP) and control
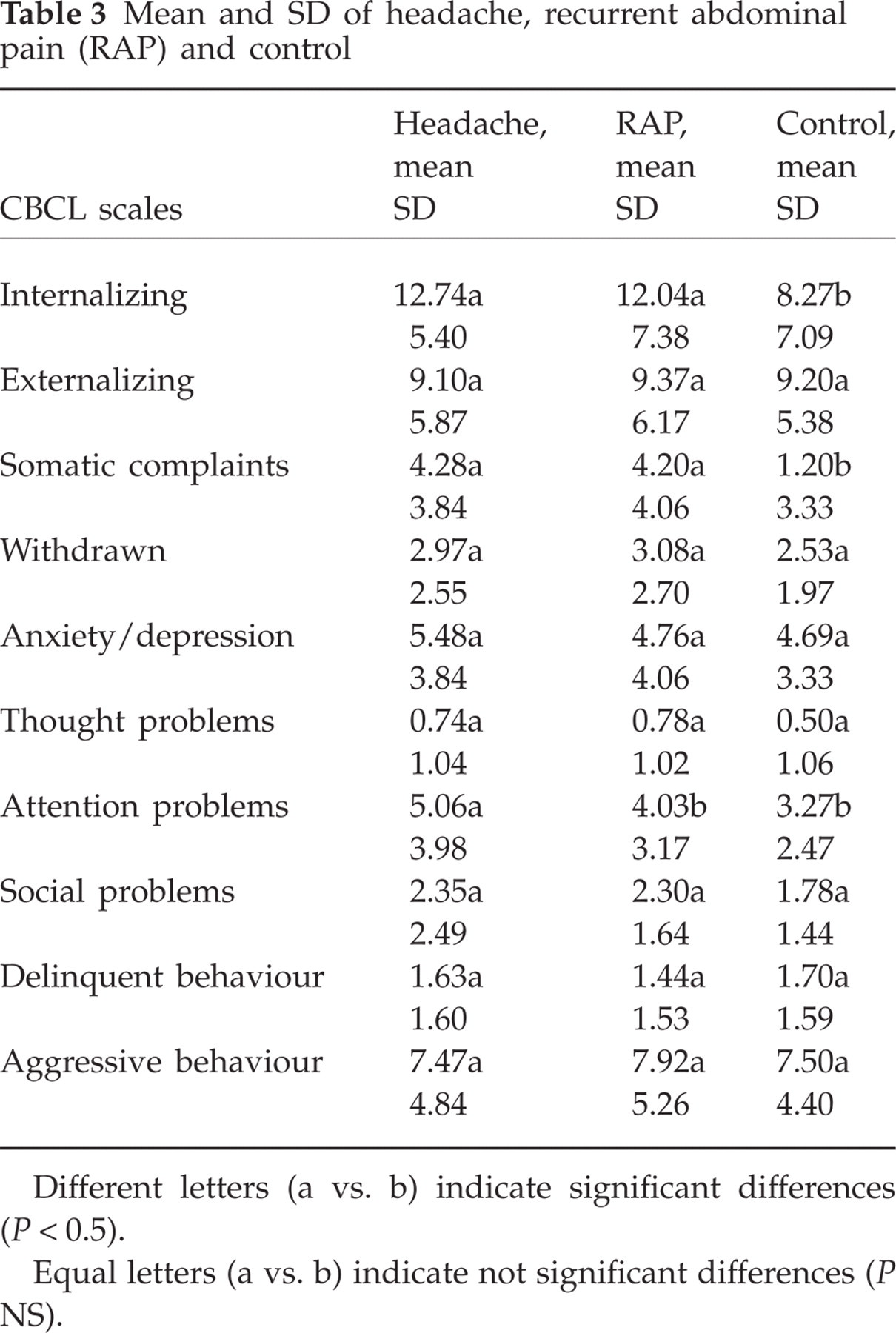
Different letters (a vs. b) indicate significant differences (P < 0.5).
Equal letters (a vs. b) indicate not significant differences (P NS).
No differences were found in Externalizing scale comparing control with headache and RAP samples (F(2,207) = 0.039; P = 0962). In the Internalizing scale, we found slight gender differences: in headache patients higher scores were found in girls (girls, mean 13.7; boys, mean 11.8); in RAP, boys had more problems than girls (boys, mean 13.1; girls, mean 10.7).
Moreover, the headache group showed no differences in age classes in the Internalizing scale: mean was 12.6 for 4–11 and 12.8 for 12–18 age classes. In RAP patients, we found higher scores in the 12–18 class (4–11, mean 10.9; 12–18, mean 16).
Analysing CBCL subscales, we found a significant difference in the Somatic Complaints subscale (Internalizing scale) between groups (F(2,207) = 49.136; P = 0000) (Table 2); headache and RAP subjects showed the same trend compared with control (Table 3).
The Attention Problems subscale showed a significant difference (F(2,207) = 5.268; P = 0006) (Table 2): headache patients showed more problems compared with control and RAP (Table 3). There were almost twice as many boys as girls with headache (boys, mean 6.2; girls, mean 3.9).
There were no differences in the other subscales between the three groups.
Migraine, TTH, FAP, IBS and control groups: a comparison between scales and subscales
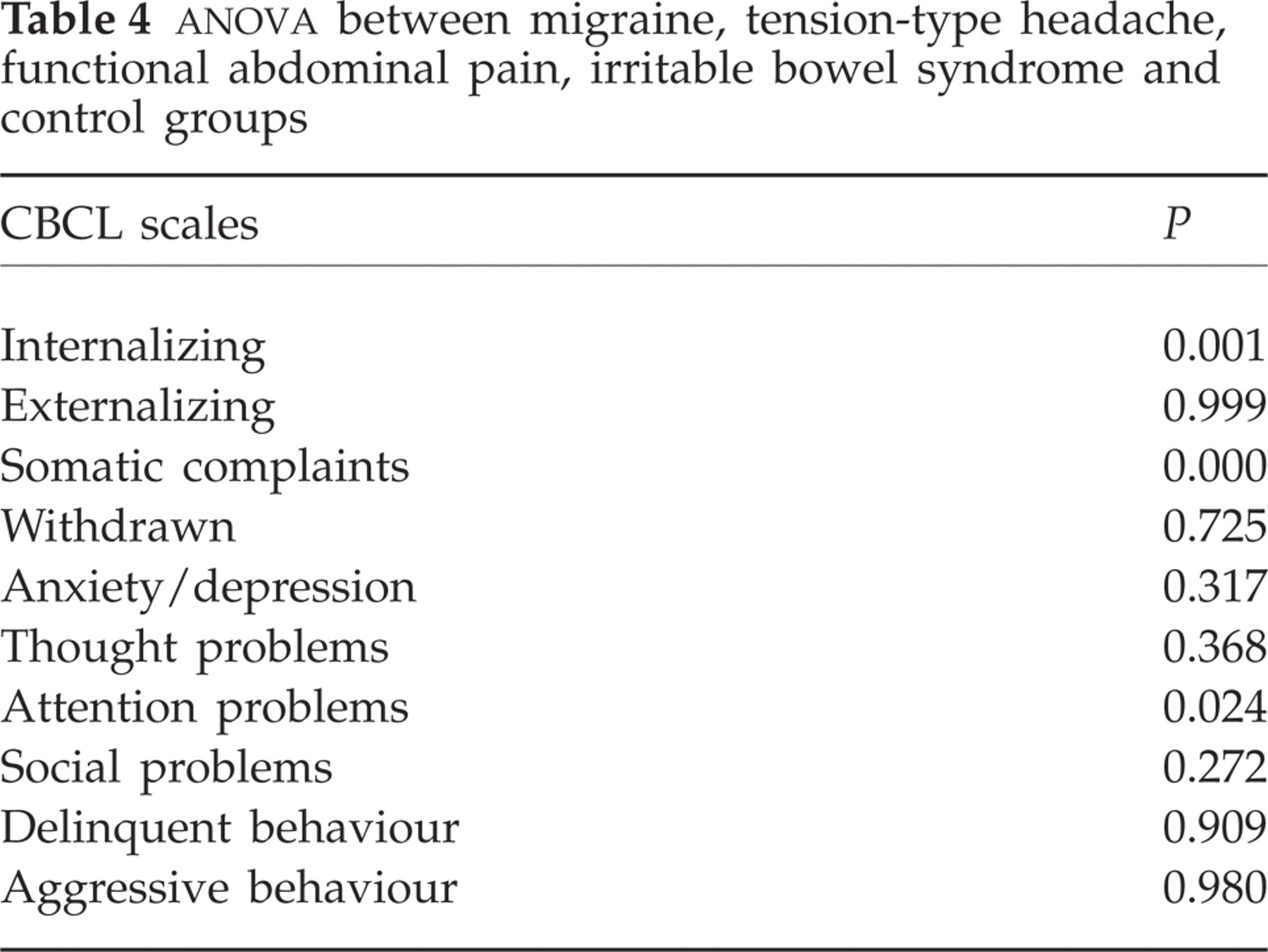
We found a significant difference in Internalizing scale between groups (F(4,209) = 4.923; P = 0001) (Table 4); Duncan's post hoc test revealed differences between control groups and all clinic samples (Table 5). IBS and TTH showed higher Internalizing scores, followed by migraine, FAP and control.
Mean and SD of migraine, tension-type headache, functional abdominal pain, irritable bowel syndrome and control groups

TTH, Tension-type headache; FAP, functional abdominal pain; IBS, irritable bowel syndrome.
Different letters (a vs. b) indicate significant differences (P < 0.5).
Equal letters (a vs. b) indicate not significant differences (P NS).
We found no significant differences in the Externalizing scale between groups (F(4,205) = 0,024; P = 0999) (Table 4), where we found a very similar mean trend for all subsamples.
Analysing all the subscales, Somatic complaints showed significant differences between groups (F(4,205) = 26,467; P = 0000) (Table 4). Children with IBS showed the highest Somatic complaints scores, closely followed by migraine, TTH and FAP, compared with the control group (Table 5).
A difference in the Attention Problems subscale was found only in migraine patients (F(4,205) = 2.876; P = 0024) (Table 4): this group had higher mean scores, followed by TTH, IBS, FAP and control (Table 5).
There were no significant differences in any other CBCL scales and subscales comparing the diagnostic groups.
MoA, MA, ETTH and CTTH: a comparison between scales and subscales
Comparing MoA, MA, ETTH and CTTH,
Regarding the Somatic Complaint subscale, we found no significant difference between the four headache subgroups (F(3,66) = 1.349; P = 0.266).
There were no significant difference in the Anxiety/depression subscale between headache subtypes (F(3,66) = 0.649; P = 0.586).
There were no significant difference in other subscales between the headache subgroups, and no significant differences in Externalizing scale (F(3,66) = 0.485; P = 0.694).
Discussion
RAP and headache showed a similar trend in the association with Internalizing disorders. The presence of Externalizing disorders was virtually identical in the three groups.
To the best of our knowledge, only two studies (3, 41) have directly compared children with headache and abdominal pain. However, the first study (3) compared only patients with TTH (N = 28) (no ICHD criteria) and RAP (n = 33) (Apley and Naish's criteria), enrolling patients with comorbid RAP and headache also (N = 8). The second one (41) compared ‘stomach aches’ and ‘headaches’ (no other kind of classification) in a preschool population and showed the influence of maternal depressed mood (but not their health problems) on somatic complaints of their children. Headache and stomach ache children showed more psychological symptoms (‘behaviour problems’) than healthy children (41).
The similarities in psychological profile in headache and RAP patients is intriguing, not only from the psychological standpoint. Mechanisms related to the perception of pain, to the possibility of a shared biological substrate involving anxiety and depression or cognitive factors may be called into question.
The involvement of the CNS has been evidenced both for RAP (‘gut brain’, visceral hyperalgesia) (51) and migraine (brainstem activation, cortical hypo/hyperexcitability) (52).
The mechanisms explaining the onset of recurrent and chronic painful disease in adults assumes that there is a dysregulation of endogenous pain-inhibiting mechanisms (53, 54). In the paediatric field, studies applying the cold pressor test to children with recurrent or chronic painful conditions have reinforced the hypothesis of dysregulated pain perception, which means a reduced capacity to tolerate induced pain in comparison with healthy children (55, 56). In children with RAP, a lower pain threshold has been evidenced than in their healthy peers, presumably because of alterations of central inhibitory endogenous centres (57). Pain experience is modulated by interactions of ascending and descending pathways, on the basis of sensory-discriminative and affective-motivational functions. Dysregulation of the modulation of these networks may underlie the development of chronic pain and comorbid conditions (58). This aspect might be hypothesized to be the mechanism involved in the well-known association of chronic pain and anxiety/mood disorders.
It is noteworthy that patients with RAP or headache had the highest score in the Somatic complaints subscale. This aspect is of interest also from a clinical point of view, because co-occurrence of multiple somatic complaints may be related to the beginning of a process of somatization, which in adults develops into a somatization disorder, according to DSM-IV criteria (42). However, other explanations exist: parents might pay excessive attention to somatic- and physical-type problems and neglect those of psychological type.
Analysing our findings according to headache subtype, only in the Attention problems subscale in migraineours did we find a difference to be stressed. Attention problems is also the only subscale to differentiate headache and RAP samples. We stress that the CBCL does not allow to make a clinical diagnosis, but the presence of attention problems in headache patients needs particular attention. Concentration difficulties have been shown to be associated with headache occurrence at preschool age (59). Other studies have shown the presence of attention-deficit symptoms in migraineours (44, 60) and of externalizing problem behaviours involved in the incidence of frequent headache among adolescents (61). Our findings did not support a role for externalizing disorders in headache patients, even if the presence of attention problems (without significant prevalence in migraineours) needs consideration in order to understand the meaning and direction of influence (from headache to attention difficulties?).
This study has a number of limitations that must be taken into account in interpreting the data. Our results derive from children who were clinically referred to third-level centres for the treatment of primary headache or RAP, and they may not be representative of the general population, even though one population-based study has shown similarities in demographic and social characteristics of children with migraine and abdominal migraine (62). The CBCL allows a psychological profile of children, not a clinical diagnosis. Further studies are warranted to study the psychological conditions using psychiatric or personality interviews. The CBCL is based on parents' reports, with their subjective point of view. Comparing multiple sources of information may be useful in forming a complete picute of the clinical condition.
In conclusion, the role of internalizing disorders in headache and RAP patients must be stressed, as well as the importance of psychological diagnostic work in headache and abdominal pain of children and adolescents, the sine qua non condition to realize a complete treatment.