
Abstract
Although migraine is less prevalent in older than in younger age groups, the absolute increase in the number of subjects in older age groups may lead to an increase in the total number of migraine patients. Consequently, more elderly migraine patients may seek medical attention. In this review, the epidemiology and clinical aspects of migraine in the age group of ≥60 years are summarized, with special attention to comorbidity. The review will focus on treatment choices in elderly migraine patients. These must be based on knowledge of mechanisms of physiological and pathological ageing.
Keywords
Introduction
Migraine usually begins in the first three decades of life, with a peak in puberty, around the age of 12 in boys and 15 in girls (1). However, attacks may start at any age. In cross-sectional studies, most active migraine patients have been found between the ages of 30 and 40 years, but there are also many migraine patients in their 60s, 70s and even 80s (2).
As with paediatric headache, there are several age-specific diagnostic and therapeutic considerations in geriatric headache sufferers (3–5). As the geriatric population continues to increase in most Western countries, so will the importance of this subject. This review will focus on the clinical and diagnostic considerations in treating geriatric headache.
Clinical aspects of migraine in the elderly
In this review, we focus on the special aspects of migraine in patients aged ≥60 years. This cut-off was chosen arbitrarily, because it lies above the median age of menopause, after which hormonal factors are less likely to play a role. In this way, men and women can be discussed together. Whereas the female : male ratio is around 3 : 1 in young and middle-aged patients, it declines to 2 : 1 after the age of menopause (6).
Prognosis of migraine
In general, migraine has a relatively favourable prognosis. From longitudinal studies it is has become clear that around 40% of migraine with aura (MA) and migraine without aura (MoA) patients stop having attacks (7–10). The decrease begins in the fifth or sixth decade of life (11) and occurs not only in postmenopausal women, but also in men. Numerous cross-sectional studies have shown that migraine can also persist in the age group of patients aged ≥60 years. For example, the 1-year prevalence of migraine in a Dutch population-based study was 5.63% in men and 20.4% in women aged >55 years (12). A Swedish population-based study found active migraine in 8.9% of women in the age group between 60 and 64 years, 6.8% between 65 and 69 years and 3.4% between 70 and 74 years (13). Comparable results have been found in Denmark (14), Canada (15), France (16), China (17), USA (2) and Italy (18, 19). One study even found migraine in 5% of patients over the age of 80 years (16). Although migraine is less frequent in those over 60 than in other age groups, the absolute number of migraine patients in many populations worldwide is considerable (20).
Changing symptoms during ageing
When migraine persists, its characteristics may change with advancing age (21, 22). The problem of transformation of migraine into a chronic daily form can occur at all ages, and also in the elderly (23). Medication overuse often plays a role. This transformation reflects a poor migraine prognosis, but fortunately occurs only in a minority of patients. Recently, the prevalence of transformed migraine was estimated to be 2%, with a male : female ratio of 1 : 3 (24). In a retrospective study in a headache centre, however, almost a quarter of patients (mainly women) had transformed migraine, but this was obviously a biased population (6).
During ageing, MA attacks may lose the headache element, so that only (visual) aura symptoms, called migrainous visual accompaniments, remain. More than 20 years ago, Miller Fisher published his landmark articles on late-life migraine accompaniments (25, 26). He described typical (mostly visual) migraine aura's without headache in patients aged >40 years. There is not a great diagnostic problem, when the patient also suffers or has suffered from MA, but uncertainty arises when these phenomena occur for the first time in a patient without headache. In such a case, extensive search for other (vascular) causes is needed before one can diagnose the phenomena to be migrainous. Only when an extensive work-up is unremarkable, and when the symptoms are typical of migraine aura, may they be called ‘migrainous’. Most patients have visual symptoms alone or in combination, and a typical sign is the gradual build-up and spread over time (21). In a general population sample of the Framingham study, 2110 subjects were systematically queried about the occurrence of visual symptoms (27); 1.33% of women and 1.08% of men reported visual migrainous symptoms. Episodes began after the age of 50 in 77% of the subjects. The diagnosis ‘migrainous’ was not difficult when the spells were typical (i.e. paracentral onset with a slow progression and expansion over the visual field, lasting between 5 and 60 min) and when two or more spells occurred. When the spells were atypical, or when they occurred for the first time, diagnosis was not straightforward.
New-onset migraine
New onset of migraine above the age of 50 is not rare. For example, a Scandinavian epidemiological study found that 19% of women with MoA had an age at onset of >50 years (14). However, there are few patients who develop new-onset migraine after the age of 60 (28, 29). When a patient in this age group develops migraine-like headache, an underlying disease such as a mass lesion or giant cell arteritis must always be ruled out (30). In a systematic study of elderly patients with new-onset migraine-like headache, most patients did not have an underlying disease (31). Only five of 69 patients in that study had an abnormality on cerebral imaging. All five were men with onset of migraine after the age of 50 years. All had a (silent) infarct on cerebral computed tomography or magnetic resonance imaging (MRI). Nevertheless, caution is advised when making the diagnosis of new-onset migraine over the age of 60 without appropriate investigations (3).
Comorbidity of migraine, relevant for the elderly
Advancing age in general comes with increased susceptibility to a great number of diseases. For example, people aged >70 years suffer from arthritis (58%), hypertension (45%), heart disease (21%), cancer (19%), diabetes (12%) or stroke (9%) (32). Many elderly migraine patients will also suffer from these age-related diseases, and especially vascular diseases such as atherosclerosis, hypertension and diabetes, and their consequences (heart disease and stroke) will influence the management of migraine in the elderly.
There are also several diseases that occur more often in association with migraine than expected by their prevalence in the general population (33). An example is ischaemic stroke, which has been associated with migraine in young women in several case-controlled studies (34). Not all comorbidities are specifically age related, and here some topics will be highlighted which can be of relevance in the elderly migraine population. These topics are: (cerebro)vascular disease, depression, cognition, vertigo and epilepsy.
Migraine and (cerebro)vascular disease
The association between migraine and ischaemic stroke is well known from case–control and cross-sectional studies, but only in young women (34). In older populations, findings are not consistent. Migraine was not significantly more present in elderly patients with ischaemic stroke than in patients without a stroke (35). No association was found between migraine and stroke in patients aged >55 years (36). Migraine was not associated with high blood pressure or increased intima-media thickness in elderly patients (37, 38). In contrast, a population-based study has found a higher cardiovascular risk profile in migraineurs, particularly with aura, than in individuals without migraine (39). This is in line with the finding of a strong association between MA and cerebrovascular symptoms and ischaemic stroke in patients aged >55 years in another study (40). There is, however, no increased risk of incident coronary heart disease in elderly migraineurs (33).
Whether or not there is a (causal) relation between migraine and ischaemic stroke or other vascular diseases, it is likely that a large number of patients with these diseases will have a history of migraine, given the increasing cardiovascular risk in older populations (41). So, although the association can be coincidental, it should be borne in mind, as it influences treatment.
Migraine and depression
The relationship between migraine and depression is bidirectional. Migraine patients are at risk of depression and a depressive patient suffers more often from migraine (42). This is also true for elderly patients, where there is a high comorbidity of migraine and depression (43, 44). A recent large Swedish study has shown that in women aged 60–74 years the risk of active migraine is strongly associated with a history of major depression (44). Although the pain intensity of migraine declined with age, the proportion of women reporting severe disability did not. This was interpreted as an age-related low threshold to experience pain caused by personality traits.
A history of major depression at any time during life has an age-specific effect on the prevalence of active migraine later in life. Depressive symptoms can influence the occurrence and severity of migraine in elderly patients. This not only predicts a worse prognosis of migraine in depressive subjects, but also influences treatment choices (see below).
Migraine and cognition
The finding of a high incidence of cerebral white matter hyperintense lesions on MRI in migraine patients (45) and the fact that migraine causes significant and often frequent disruptions of the physiology of the brain, could lead to the assumption that there is a migraine-related cognitive decline. Studies of cognition in younger migraine subjects, however, have yielded controversial results, and several well-conducted studies in aged patients have even failed to find a relationship between migraine and cognitive decline (46). Furthermore, a long history of severe migraine did not seem to impair cognition (47). Based on these observations, it is very unlikely that migraine and cognitive impairment in the elderly are related.
Migraine and vertigo
Patients with migraine frequently have vestibular complaints, such as dizziness, unsteadiness or head motion intolerance. As well as these often very vague and non-specific complaints, there is growing evidence of a clinical entity of recurrent vestibular symptoms related to migraine, called ‘migraine-related vertigo’ (48). In this entity, vertigo is described as the sensation of spinning or turning, interfering with daily life activities, in a patient with a personal history of migraine. Commonly, the vertigo follows migraine with a delay of months to years with respect to migraine onset. Although dizziness is a common complaint in the general population, and appears to increase with age, migraine-related vertigo is not specifically associated with age >60 years. Its occurrence peaks in the fourth decade in men and between the third and fifth decades in women.
Patients with Meniere's disease (MD) have more often migraine than controls (49). In approximately half of MD patients, attacks of dizziness are accompanied by migraine-like symptoms, such as headache, photophobia or phonophobia. In most patients, the onset of migraine precedes the onset of MD, sometimes by >30 years.
Migraine and epilepsy
Older epidemiological studies of the relation between migraine and epilepsy were unreliable, as they lacked strict criteria for the diagnosis of migraine and epilepsy, as well as a good control group. The first state-of-the-art epidemiological studies to use the International Headache Society criteria for migraine were performed in the 1990s. Marks and Ehrenberg found migraine in 20% of patients with epilepsy. In 3% of these patients the attacks of epilepsy occurred in a close temporal relationship with the attacks of migraine (50). In a population-based study of almost 2000 patients with epilepsy, Ottman and Lipton found concomitant migraine in 24% (51). Of the family members with epilepsy, 26% also had migraine, whereas only 15% of family members without epilepsy had migraine. Comparable results were found in later studies (review in (52)). It is remarkable that virtually all studies on a relationship between migraine and epilepsy have focused on younger age groups and ignored the elderly migraine population. For example, the landmark studies of Otmann and Lipton included only patients aged <40 years (51). As a consequence, there is no information about the specific comorbidity of migraine and epilepsy in the elderly. As potentially epilepsy-causing diseases such as Alzheimer's disease, stroke and other structural brain lesions are highly prevalent in the elderly, is likely that there will be patients with comorbid migraine and epilepsy in this age group. This is of importance, as it will influence choices of preventive migraine treatment (see below).
Treatment of migraine in the elderly (Tables 1 and 2)
Ageing is characterized by several physiological and pathological changes that together alter the effects of drug treatment. Physiological changes include gastric factors (decline of gastric acid secretion, slowing of gastric emptying, decreased peristalsis and changes in gut wall metabolism), hepatic factors (40% reduction of blood flow to the liver, reduction of liver mass and changes in liver metabolism), renal factors (decline in glomerular filtration rate and 25% reduction in kidney mass), changes in body composition and in vascular control systems (32). Pathological processes add to the physiological changes. Vascular diseases, such as hypertension and diabetes, lead not only to heart disease and stroke in the elderly, but also to decreased hepatic and renal function. The ageing kidney, for example, is characterized by increased fibrosis, tubular atrophy and arteriosclerosis. Taken together, age-related changes make older subjects more susceptible to the adverse effects of medication. The incidence of adverse drug reactions correlates with age (53). This is due not only to altered pharmacokinetics, but also to comorbidity and polypharmacy. Advancing age changes the risk–benefit ratio of many drugs. When adverse drug reactions occur in older people, they are more likely to be severe, and are even estimated to be the fourth to sixth greatest cause of death (32).
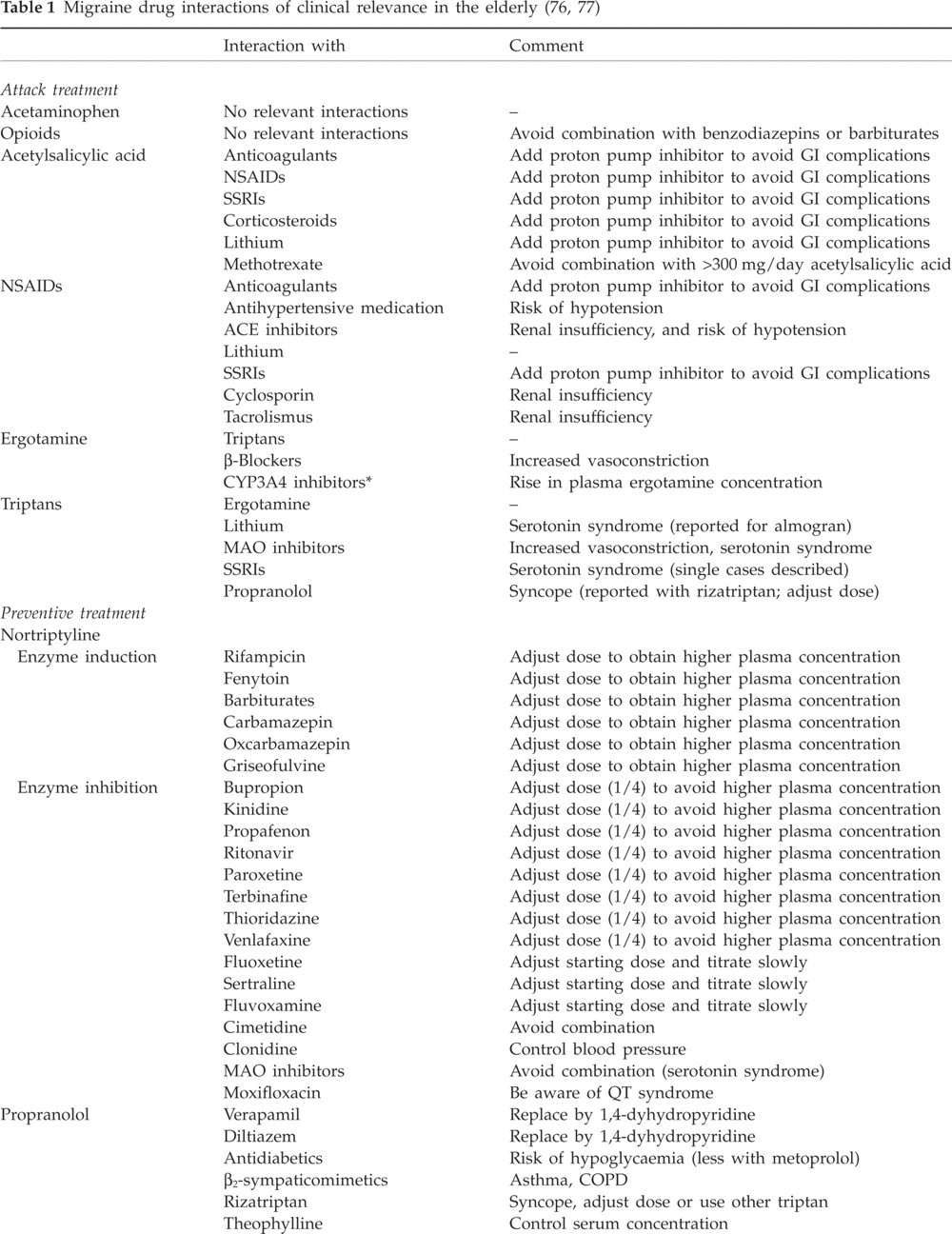
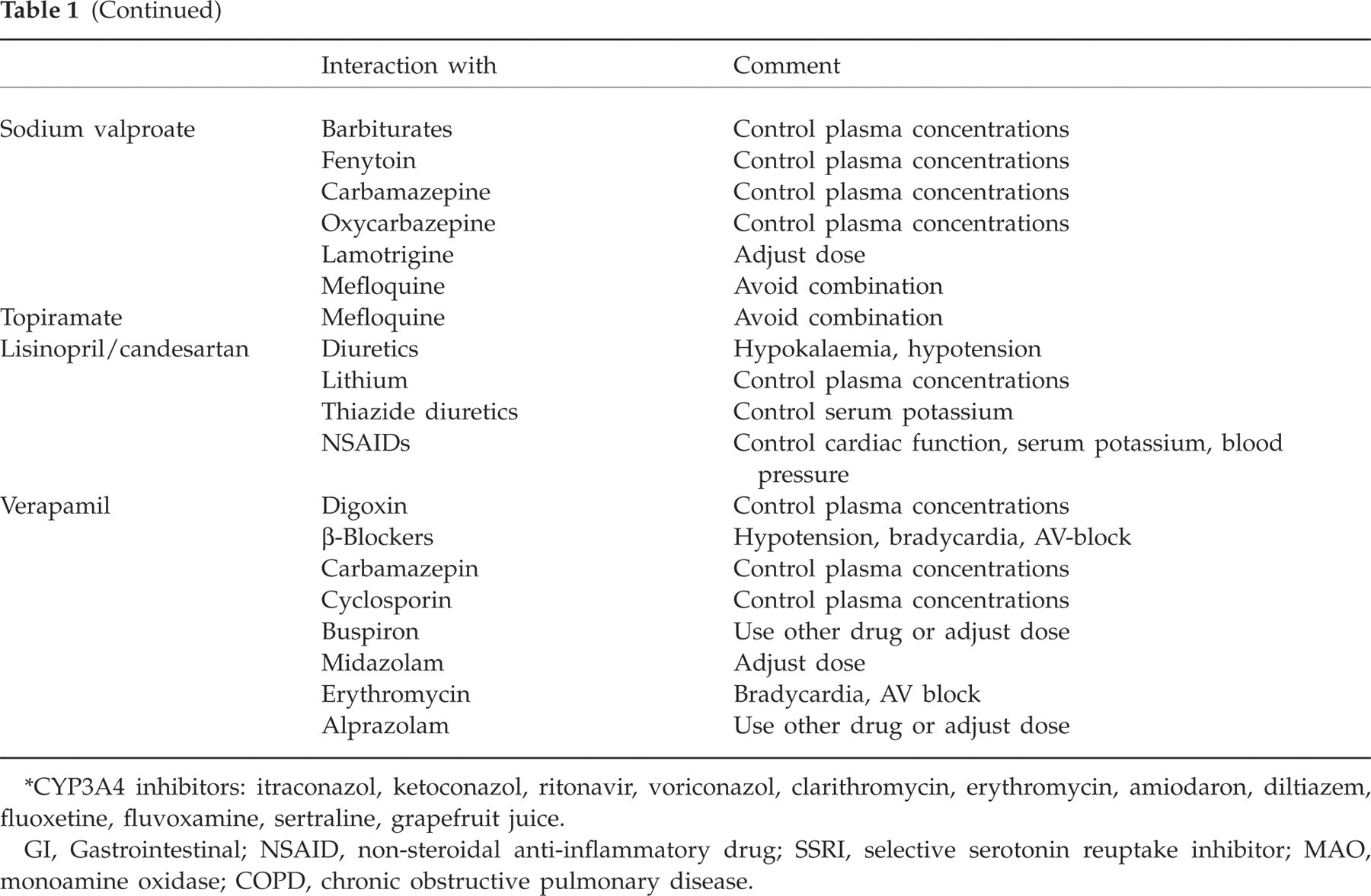
CYP3A4 inhibitors: itraconazol, ketoconazol, ritonavir, voriconazol, clarithromycin, erythromycin, amiodaron, diltiazem, fluoxetine, fluvoxamine, sertraline, grapefruit juice.
GI, Gastrointestinal; NSAID, non-steroidal anti-inflammatory drug; SSRI, selective serotonin reuptake inhibitor; MAO, monoamine oxidase; COPD, chronic obstructive pulmonary disease.
Which treatment should be used in the elderly?∗
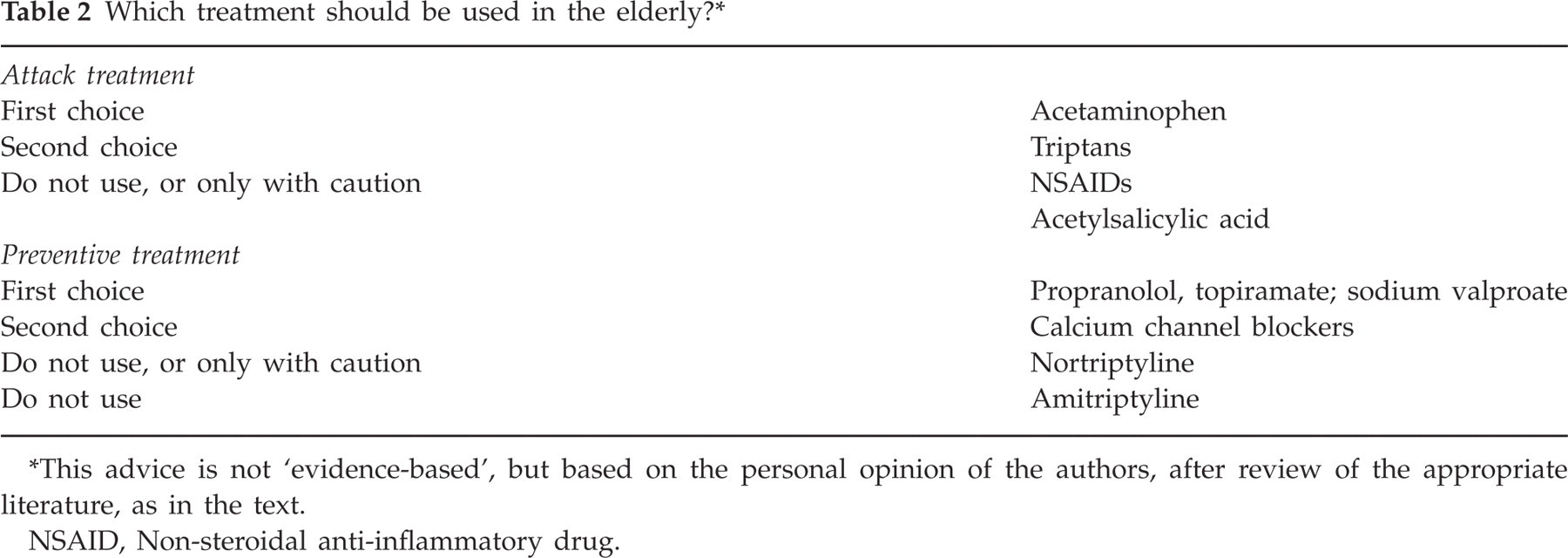
This advice is not ‘evidence-based’, but based on the personal opinion of the authors, after review of the appropriate literature, as in the text.
NSAID, Non-steroidal anti-inflammatory drug.
An important factor is that, in the majority of migraine trials, patients have been excluded on the basis of age >60 or >65 years without further justification (54). It is likely that this has been to improve the efficacy outcome of the study treatment and to decrease possible adverse events. This has led to an unjustified, scientifically unproven concern about perceived adverse events and to undertreatment of older migraine patients. In a recent study, almost all migraine patients aged >65 years took medication for their attacks, but >40% were reluctant to take drugs for every attack, particularly when they did not have to perform urgent daily life activities (20). Many physicians also feel uncertain with treating attacks or prescribing preventive drugs in elderly patients (5). Treatment options are considered to be restricted and this often leads to a failure of both elderly patients and their physicians to address specifically the topic of preventive treatment (55). Coincidental diseases and medication, however, rarely fully prohibit the use of migraine medication. When the various aspects are taken into account, treating migraine in the elderly can be successful and satisfying.
As in younger age groups, before drug treatment of migraine is tried, non-pharmacological measures, such as avoiding migraine triggers, should be advised. When these measures are not effective, treatment of migraine attacks, or a combination of attack treatment and preventive treatment, can be considered.
Acute migraine drugs
Simple analgesics
Paracetamol can be used in elderly migraine patients. Because hepatic metabolism is reduced in the elderly, it is advised to monitor liver function, especially when paracetamol is used regularly in doses of >3 g/day (56, 57). In cases of renal or hepatic dysfunction or hazardous or harmful alcohol use, a dose reduction of 50–75% is advisable (53, 56). Acetylsalicylic acid should also be used with caution, as the risk of a gastric ulcer or bleeding increases in the elderly (32). The addition of caffeine to the simple analgesics does not lead to an increased risk of adverse events in the elderly.
Anti-emetic drugs
Anti-emetic drugs, such as metoclopramide, introduce the risk of extrapyramidal adverse events (3).
Non-steroidal anti-inflammatory drugs
Non-steroidal anti-inflammatory drugs (NSAIDs) should be used cautiously, if at all, in elderly patients (55). Upper gastrointestinal haemorrhage or perforation increases substantially with advancing age in subjects taking NSAIDs (56). An estimated 15–35% of all peptic ulcer complications are secondary to NSAID use (53). Thousands of elderly patients die each year as a result of gastrointestinal complications from NSAID therapy (53). Therefore, NSAIDs should always be accompanied with a proton pump inhibitor. Advancing age is also a risk factor for NSAID-induced hypertension and renal impairment (32). When NSAIDs are used, renal function, liver function and gastrointestinal adverse events should be monitored (57). NSAIDs interact with anticoagulants, hypoglycaemics, digoxin, antihypertensive agents and diuretics (3). COX-2 inhibitors such as celecoxib can cause lower-limb oedema (57) as well as increase the risk of stroke.
Opioid analgesics
Opioid analgesics are limited by sedation and cognitive side-effects in the elderly (30). Propoxyfene can cause ataxia and dizziness (56). Tramadol often causes nausea and vomiting, and in higher doses can cause seizures (56). Consequently, the advice is not to use opioids in elderly patients with migraine, or to start low and increase the dose only slowly (55). Adverse events such as constipation and urinary retention must also be monitored (57). Opioids should always be accompanied by laxatives.
Ergotamine
Ergotamine has a low degree of receptor selectivity, which increases the risk of a drug-induced adverse effect in all age groups (58). Pre-existing hypertension can worsen and coronary vasoconstriction can occur, often with associated ischaemic changes and anginal pain, and peripheral vasoconstriction. Ergotamine should be avoided or used with caution in elderly patients (3, 30).
Triptans
The triptans (sumatriptan, rizatriptan, zolmitriptan, naratriptan, almotriptan, frovatriptan, eletriptan) are examples of drugs that have been thoroughly studied in clinical trials, but virtually always after excluding patients aged >60 or >65 years. It is, however, generally thought that they may be used after the age of 60 years if, and as long as, there are no cardiac contraindications (5, 54). However, especially in cases of cardiac ischaemia, one should show great care with vasoconstrictive drugs such as triptans. However, a recent large study of triptan use in general practice, also in elderly patients with various risk factors, has shown that there is no increased risk of stroke, myocardial infarction, cardiovascular death, ischaemic heart disease or mortality (59). When triptans are used in elderly patients, periodic cardiac screening (e.g. an ECG evey 3 months) is advised.
Some of the triptans have been studied in healthy elderly subjects. Plasma pharmacokinetics of rizatriptan appeared to be similar in the elderly and in the young (60). Zolmitriptan induced a statistically significant increase in systolic and diastolic blood pressure in the elderly compared with young adults, but this was not considered to be of clinical concern (61).
Preventive migraine drugs
The use of preventive migraine treatment in all age groups is increasing, although the efficacy of most of the prophylactic drugs is limited, and most of the available drugs are associated with many adverse effects, especially in the elderly (3, 62). An often heard argument is that preventive treatment is prescribed because it can reduce time lost at work. This argument of course is not valid in the elderly, as many are retired. This might be one of the reasons why a Dutch survey of migraine prophylactic medication usage pattern found that only 3.4% of patients using preventive treatment was aged >64 years (63). Another reason could be that preventive drugs are thought to lead to adverse effects in the elderly (3). In general, the advice in elderly is to start preventive treatment at low dosages and increase them slowly (56, 62). Anticholinergic drugs and treatment with multiple drugs must be avoided as much as possible, as these are risk factors for delirium in older patients (64).
Tricyclic antidepressants
Tricyclic antidepressants, especially amitriptyline, are often used as preventive treatment for migraine in adults, although without scientific evidence. Caution is advised when used in the elderly (53–56). Elderly patients who receive normal doses of tricyclic antidepressants usually develop higher plasma drug concentrations and metabolites than do younger patients (53). Amitriptyline can cause anticholinergic adverse effects (orthostatic hypotension), confusion, seizures and cardiac conduction disturbances (3). Fewer adverse events are associated with nortriptyline, which may therefore be an appropriate alternative to amitriptyline. Tricyclic antidepressants are contraindicated in patients with cardiac dysrhythmias, closed-angle glaucoma and urine retention (65). However, the doses used for chronic pain such as migraine are in general lower than those for treating depression, and adverse effects are less pronounced (66).
β-Blockers
The absolute bioavailability of propranolol doubles in the geriatric patient, thus the dose must be adjusted (32). Use may be limited because they influence congestive heart failure, conduction abnormalities, asthma, glaucoma, depressive symptoms and diabetes (3).
Sodium valproate
Sodium valproate is associated with a number of adverse events, and because of reduced hepatic mass and blood flow in the elderly these adverse events can occur more frequently in this age group. Sodium valproate can cause liver function disturbances, bone marrow suppression, decreased bone marrow density, delirium, tremor, ataxia and, in rare cases, an extrapyramidal syndrome with dementia (67–69). Alopecia will not often be a problem in an elderly migraine patient.
Topiramate
Topiramate is associated with a high risk of adverse events also in younger age groups (67). It can cause cognitive impairment, renal stones, body weight loss, sedation and agitation. In one study of epilepsy, however, it seemed to be well tolerated in the elderly (70).
Lisinopril and candesartan
The ACE inhibitor lisinopril and AT II inhibitor candesartan were tested only in patients <65 years old (71, 72). Adverse events were minimal. The compounds seem especially effective against migraine in patients with comorbid hypertension (73). In the elderly, ACE inhibitors and AT II inhibitors should be used with caution, as they can cause acute renal insufficiency.
Calcium channel blockers
Calcium channel blockers may be used for migraine prevention. However, there are several considerations with respect to their use in the elderly. A moderate decrease in the clearance of all calcium channel blockers occurs with ageing (74). Older patients experience greater reductions in blood pressure and greater suppression of heart rate. Postural hypotension occurs more frequently in the elderly. When calcium channel blockers are prescribed in elderly patients, the dose must be adjusted. Caution is needed in patients with concomitant congestive heart failure (3). In the geriatric population, verapamil has been associated with gastrointestinal bleeds caused by its antiplatelet effects (75). Suspected gastrointestinal bleeds or bleeding points are a contraindication. Flunarizin used to be prescribed in migraine several decades ago, but its use is now very limited. Elderly patients are more susceptible to side-effects, including depression and parkinsonism.
Treatment of comorbid disease
Several non-migraine drugs, commonly used in the aged, can aggravate migraine symptoms or cause migraine headache de novo (3, 4). They should therefore be chosen carefully. Examples of medications that exacerbate migraine are nitrate-containing drugs, oestrogen replacement therapies and vasodilating antihypertensive drugs, such as nifedipine.
Treatment of comorbid diseases can also be carefully chosen to improve migraine. Examples are β-blockers in cases of migraine with hypertension, antiepileptics (sodium valproate, topiramate) when the patient has migraine and epilepsy, and nortriptyline, which can also improve coexistent depression.
Conclusions
Migraine in older age groups has been neglected, although many subjects >50, >60 and even >70 years old suffer from migraine. Special attention is needed in the diagnosis of migraine in elderly patients, as other diseases causing headache should be considered and excluded, especially in cases of migrainous visual symptoms without headache. Comorbidity plays an important role not only in diagnosis, but also in treatment choice. Acute and preventive medication should be chosen carefully, but patient management should not be too negative. Even in these age groups, effective treatment is available and careful management can improve the quality of life.