
Abstract
Little is known of mechanism of dialysis headache (DH). As suggested for migraine, a role for neuropeptides has been investigated. Twenty-four patients under haemodialysis were studied. Twelve of them suffered from DH. The remaining patients were headache free. Blood samples for radioimmunoassay of calcitonin gene-related peptide (CGRP) and substance P (SP) were collected from the arteriovenous fistula before and after dialysis treatment. Basal plasma concentrations of CGRP were found to be higher in headache patients. Dialysis significantly decreased CGRP concentrations in both groups. No difference in basal plasma concentrations of SP was observed between groups. At the end of the treatment plasma SP concentrations were reduced in headache-free patients but increased in headache patients. Elevated plasma concentrations of CGRP in patients with DH could represent a biochemical factor contributing to susceptibility to headache. Because of the disputable role of SP in migraine, the significance of the increase of the peptide in plasma during DH remains to be elucidated.
Introduction
Dialysis headache (DH) is a disorder which is included in the classification of headache disorders of the International Headache Society (IHS) (1) and it is defined by the following diagnostic criteria: (i) at least three attacks of acute headache fulfilling criteria iii and iv; (ii) the patient is on haemodialysis; (iii) headache develops during at least half of haemodialysis sessions; (iv) headache resolves within 72 h after each haemodialysis session and/or ceases altogether after successful transplantation.
Bana and colleagues were the first to name this clinical condition, which is characterized by a headache beginning with the initiation of the dialysis sessions in patients without previous primary headaches (2). The authors suggested that the headache might represent an integral part of the dialysis disequilibrium syndrome, a clinical disorder which occurs in patients with end-stage renal disease who are being treated with haemodialysis (3). The syndrome may include headache, nausea, emesis, blurring of vision, muscular twitching, disorientation, hypertension, tremors, seizures, muscle cramps, anorexia, restlessness and dizziness. Mild forms of dialysis disequilibrium syndrome consist only of restlessness and headache. Clinical signs of the condition are attributed to brain swelling which occurs as a consequence of the dialysis procedure. This has been well documented in studies of uremic laboratory animals which have undergone haemodialysis (4, 5). Moreover, brain oedema has been confirmed by computed tomographic scanning in humans with renal failure who have undergone dialysis (6). The exact mechanism by which haemodialysis leads to cerebral oedema remains unclear.
A case of DH has recently been reported where the patient amielorated his headache during treatment with angiotensin converting enzyme inhibitors (7). The authors concluded that the activation of the renin–angiotensin system may be involved in the pathogenesis of DH.
The classical studies by Penfield (8) and Ray and Wolff (9) have demonstrated that it is only the large cerebral arteries at the base of the brain as well the meningeal (dural) arteries and veins that are sensitive to painful stimuli. The role that these structures play in headache initiation derives from their dense innervation by the trigeminal primary afferent neurons (10, 11) and by dorsal root ganglia of the upper cervical spinal nerves (11). Terminals of trigeminal neurons surrounding cerebral vessels contain calcitonin gene-related peptide (CGRP) and the tachykinins substance P (SP) and neurokinin A (12). There is evidence in experimetal animals that CGRP and SP are released upon trigeminal ganglion stimulation (13) and mediate some or all components of neurogenic inflammation (14). Findings in man indicate that CGRP is elevated in the extracranial venous blood during the headache phase of migraine (15, 16), cluster headache (17–19) and paroxysmal hemicrania (20). Moreover, infusion of CGRP has been shown to trigger a migraine attack (21) and the CGRP antagonist BIBN 4096 BS was effective in treating acute attacks of migraine (22). These data support the view that the trigeminovascular system may be activated in these conditions.
On the basis of these findings we investigated whether CGRP and SP plasma concentrations were different in subjects undergoing haemodialysis with or without DH and whether the haemodialysis procedure was able to affect the sensory neuropeptides in these patients.
Methods
Study population
Twenty-four patients with chronic renal failure receiving regular haemodialysis treatment three times a week were studied. The diagnoses were: chronic glomerulonephritis (n = 12), nephrosclerosis (n = 6), polycystic kidney disease (n = 3), chronic pyelonephritis (n = 2) and unclassified nephropathy (n = 1). All patients were treated with calcium carbonate and vitamin D. None was on erythropoietin therapy or treated with antihypertensive agents or steroids. Twelve patients (seven men, five women), with a mean age of 58 ± 4 years (range 41–75 years), complained of headache which fulfilled the diagnostic criteria for DH as proposed by the IHS (1). They had had no headache prior to beginning haemodialysis. The remaining patients (eight males, four females), aged 24–77 years (mean 55 ± 5 years), were headache free and served as controls. All patients had been on haemodialysis for >6 months: 45 ± 4 months for headache-free patients and 37 ± 3 months for headache patients. The difference was not significant. The study protocol was reviewed by an Institutional Ethics Committee and participating patients gave witnessed informed consent. The study was conducted in accordance with the Declaration of Helsinki.
Procedures
After an overnight fast, standard bicarbonate haemodialysis was performed. The patients were treated for 210 min. A plate dialyser whose properties are reported in Table 1 was used. The dialysate had the following chemical composition (mmol/l): 139 Na, 2 K, 1.75 Ca, 0.5 Mg, 107 Cl, 34 bicarbonate and 5 acetate. The temperature of the dialysis fluid was constant at 36.5°C. Blood pressure was monitored every 30 min. Blood samples for the determination of CGRP and SP (8 ml) and haematocrit were taken from the arteriovenous fistula before and after treatment. Dialysate (8 ml) was also collected at the end of dialysis.
Properties of the dialyser

Processing of blood samples
The tubes containing the blood samples were immediately transferred to a 4°C water bath. They were then centrifuged at 4°C for 15 min and the plasma was aliquoted and stored at −70°C until extraction. Extraction was carried out in Seppak C 18 (Millipore, Billerica, MA, USA) cartridges activated with 5 ml methanol and 10 ml H2O. Cartridges were then loaded with plasma to which 0.1 ml/min of 1 N HCl had previously been added. The precipitated samples were then washed with 10 ml of H2O followed by 10 ml of 4% acetic acid in H2O. Peptides were eluted with 5 ml of a solution containing 90% methanol and 10% acetic acid. Samples were dried under a nitrogen stream and after reconstitution with 0.1 M phosphate buffer pH 7.4, they were stored at −70°C until assayed.
Radioimmunoassay
The radioimmunoassay for CGRP-like immunoreactivity (CGRP-LI) was carried out according to the procedure reported previously (23). Aliquots (100 µl) of human CGRP-I standard or samples were incubated for 48 h at 4°C with the CGRP antiserum (100 µl). 125I-CGRP (100 µl) was added and the preparations incubated for a further 48 h at 4°C. After the addition of 1 ml of buffer containing 7.5% polyethylene glycol, 1 : 200 diluted goat antirabbit antiserum and 1 : 2000 diluted normal rabbit serum, bound and free antigen were separated by centrifugation at 2000
The radioimmunoassay for SP-like immunoreactivity (SP-LI) was performed as previously reported (23). Briefly, SP standard or samples were incubated overnight at 4°C with rabbit anti-SP antiserum and 125I-labelled Bolton and Hunter SP. After addition of 1 ml of buffer containing 7.5% polyethylene glycol, 1 : 200 goat antirabbit antiserum and 1 : 2000 normal rabbit serum, bound and free antigen were separated according to the procedure described above for CGRP-LI. The CV was <10% for values between 5 and 150 pg/ml. The interassay CV was 9%. The antiserum cross-reacts to 1% with neurokinin A, 0.5% with neurokinin B and <0.1% with physalaemin and eledoisin.
Statistical methods
Data are presented as mean ± SEM. Student's t-test for unpaired data was used to detect differences between headache and headache-free patients in: (i) mean blood pressure calculated as diastolic blood pressure and 1/3 of the difference between systolic blood pressure and diastolic blood pressure, (ii) time on regular dialysis, (iii) fluid removal, (iv) pretreatment body weight, (v) haematocrit and (vi) SP-LI and CGRP-LI plasma concentrations before the dialytic procedure. Student's t-test for paired data was used to determine changes induced by haemodialysis in: (i) mean blood pressure, (ii) haematocrit and (iii) SP-LI and CGRP-LI plasma concentrations, both in headache and headache-free patients. All tests of significance in the full analyses were two-sided and P < 0.05 was considered to indicate statistical significance.
Results
Clinical findings
All patients who suffered from DH complained of it during treatment, except for one who reported that headache started 3 h after the end of the dialysis. The average time of onset was 171 ± 18 min (range 60–390 min) from the beginning of dialysis. The headache had a mean duration of 176 ± 18 min (range 120–270 min). In most patients the headache was pressing/tightening in quality, mild or moderate in severity and bilateral in location. Nausea, photophobia and phonophobia were absent. Headache responded poorly to simple analgesics. All patients stated that the headache they complained of during the study was of the usual type.
There was no significant difference in body weight measured before treatment between headache patients (71.2 ± 6.4 kg) and headache-free patients (71.3 ± 6.1 kg). Fluid removal was nearly the same in both groups and represented about 4% pretreatment body weight (Table 2). No differences were found in mean blood pressure, which was calculated as diastolic blood pressure and 1/3 of the difference between systolic blood pressure and diastolic blood pressure, comparing the two groups before dialysis treatment (Table 2). Haemodialysis did not modify mean blood pressure values (Table 2).
Values of fluid removal (FR), mean blood pressure (MBP) and haematocrit (HCT) in patients under haemodialysis (HD) with dialysis headache or headache-free
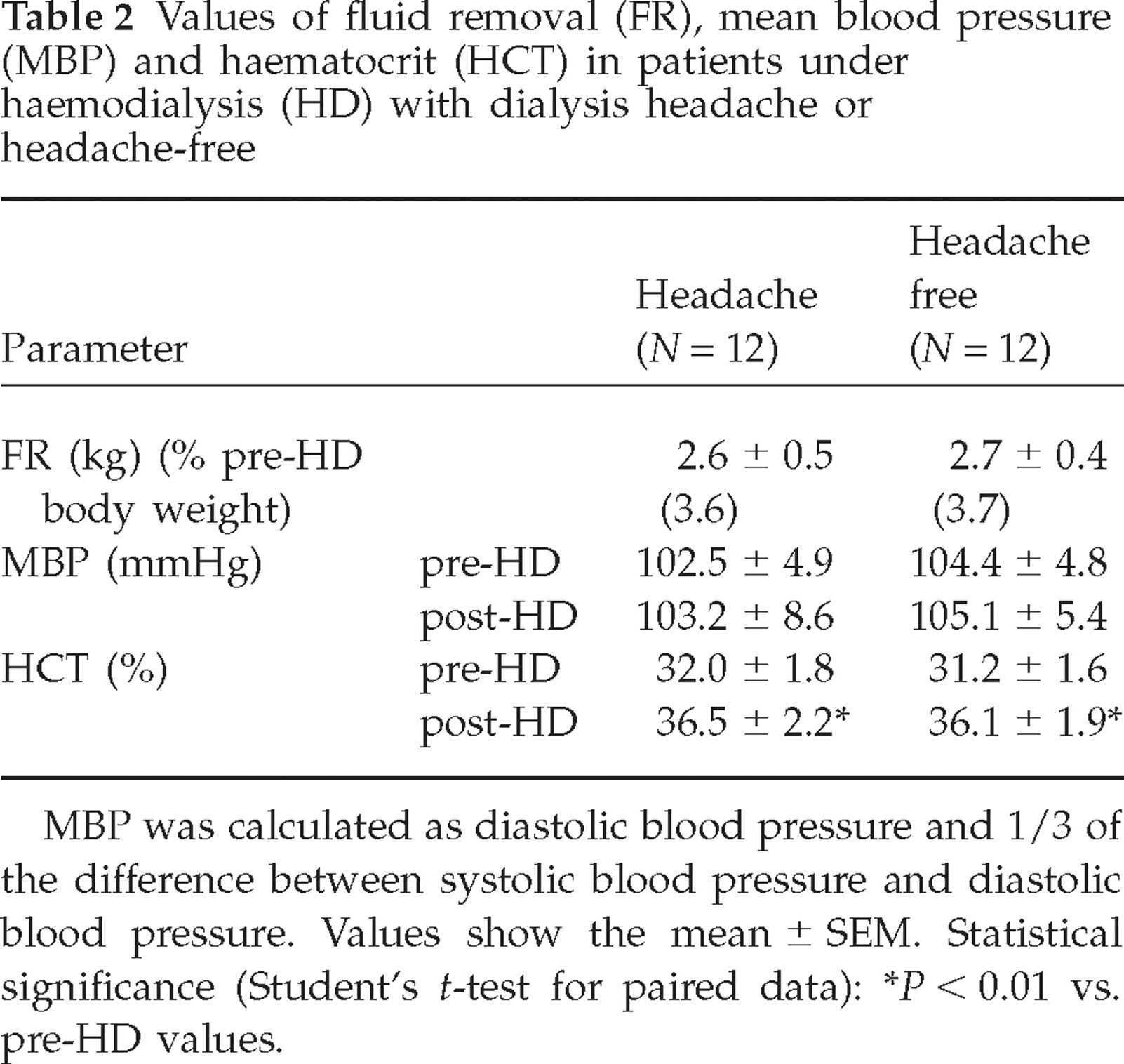
MBP was calculated as diastolic blood pressure and 1/3 of the difference between systolic blood pressure and diastolic blood pressure. Values show the mean ± SEM. Statistical significance (Student's t-test for paired data):
P < 0.01 vs. pre-HD values.
Biochemical findings
Before treatment no differences were observed in haematocrit values between groups (Table 2). After treatment, haematocrit increased (P < 0.01) in all patients (Table 2).
Concentrations of plasma CGRP-LI measured before treatment were about twofold higher in headache patients (P < 0.01) (Fig. 1). Mean plasma concentrations of CGRP-LI were decreased after treatment both in headache (P < 0.01) and headache-free patients (P < 0.05) (Fig. 1).

Calcitonin gene-related peptide-like immunoreactivity (CGRP-LI) was measured in plasma taken from the arteriovenous fistula of 24 patients receiving regular haemodialysis treatment. Twelve of them complained of dialysis headache (DH) and the remaining 12 were headache free. Measurements were performed before (▪) and after (□) treatment. CGRP-LI was also detected in the dialysate which was collected at the end of the dialysis procedure (hatched). Columns denote means ± SEM. ∗P < 0.05; ∗∗P < 0.01 vs. values before treatment (Student's t-test for paired data); †P < 0.01 vs. pretreatment values of headache-free patients (Student's t-test for unpaired data).
No difference between the patient groups was found in plasma SP-LI detected at the start of haemodialysis (Fig. 2). At the end of haemodialysis, plasma SP-LI concentrations were reduced (P < 0.05) in headache-free sufferers and increased (P < 0.05) in headache patients (Fig. 2). Measurable levels of immunoreactivity for both peptides were detected in the dialysate which was collected at the end of the treatment (Figs 1 and 2).
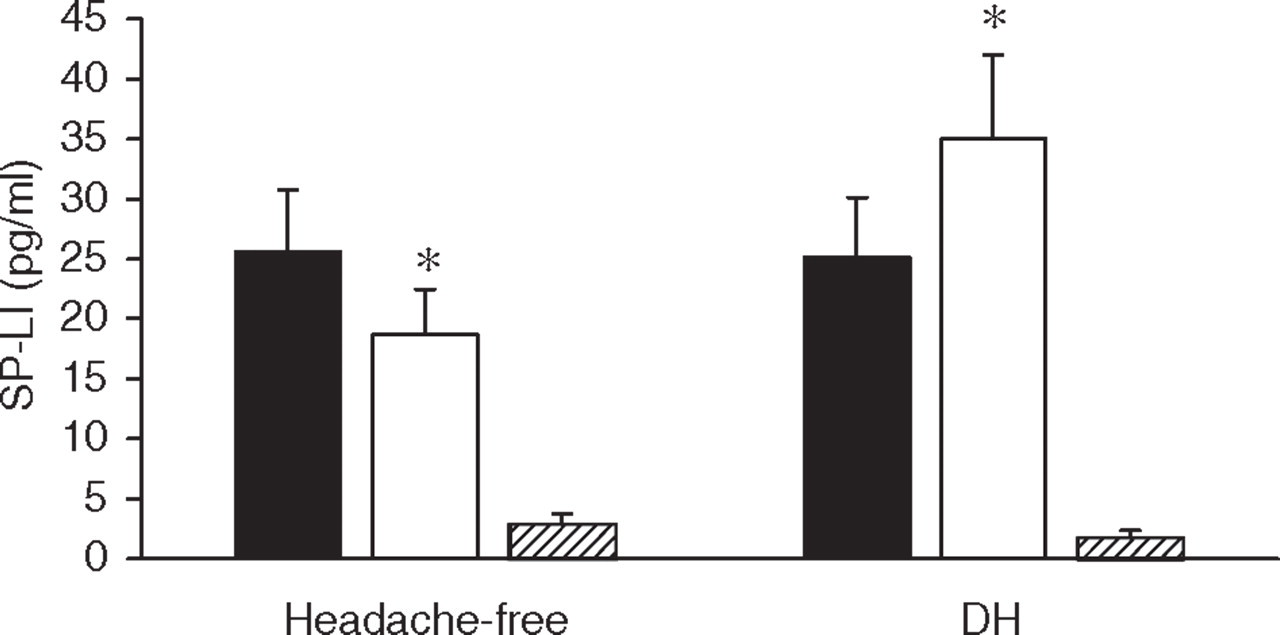
Substance P-like immunoreactivity (SP-LI) was measured in plasma taken from the arteriovenous fistula of 24 patients undergoing regular haemodialysis treatment. Twelve of them suffered from dialysis headache (DH) and the remaining 12 were headache free. Blood samples were drawn before (▪) and following (□) the dialysis procedure. SP-LI was also measured in the dialysate which was collected at the end of the treatment (hatched). Each column shows the mean ± SEM. ∗P < 0.05 vs. values before treatment (Student's t-test for paired data).
Discussion
Bana et al. (2) have described DH as usually beginning after a few hours of dialysis, starting as mild, bifrontal headache and often building up into a more severe, throbbing headache accompanied by nausea and vomiting. More recently, Antoniazzi et al. (24) have reported that DH may present both with migrainous and tension-type features, the former being prevalent (about 60%). Finally, Göksan and colleagues (25) observed that 87% patients with DH reported a throbbing-type pain. Patients in the present study reported a type of headache resembling tension-type headache. In fact, in most patients the pain was pressing-tightening in quality, mild or moderate in severity and bilateral in location. Nausea, photophobia and phonophobia were absent. Headache usually started at the end of dialysis (average 171 ± 18 min). These data agree with those of Antoniazzi and colleagues (24): the majority (62%) of their patients complained of headache at the 3rd to 4th hour after the beginning of dialysis. The headache duration of our patients was 176 ± 18 min, in agreement with data reported by Göksan and colleagues (25). The signs and features of DH described so far show that this kind of headache is not uniform in its clinical manifestation. Studies with a larger number of patients are desirable in order to clarify this important clinical aspect.
Our results show that pretreatment plasma concentrations of CGRP-LI measured in patients suffering from DH are about twofold higher than those detected in headache-free patients. CGRP is a neuropeptide present in the human trigeminal sensory neurons (26), is a potent dilator of cerebral and dural vessels (27, 28) and mediates arterial vasodilation, a major feature of neurogenic inflammation. Neurogenic inflammation has been proposed to play a major role in the pathogenesis of migraine and other headaches (13, 17, 20, 29). Differences in pretreatment plasma concentrations of CGRP cannot be attributed to specific clinical characteritics of the patient groups, as no differences in age, blood pressure or duration of chronic haemodialysis therapy were observed. Plasma CGRP concentrantions have been found to be significantly higher in haemodialysis patients with severe fluid overload than in those less severely affected (30). This finding has been proposed to be due to a defence mechanism against the most serious consequences of fluid overload, since CGRP is a powerful vasodilatory substance. However, there was no difference in body fluid volume status between our groups of patients; fluid excess in both groups was, in fact, <4% of body weight.
An increase of CGRP plasma concentrations has been found during the headache phase of migraine (15, 16) and other headaches (17, 20). It has also been observed that CGRP concentrations, measured interictally in the peripheral circulation of patients with chronic tension-type headache, tended to be higher than those in control subjects (31). It is possible that augmentation of CGRP plasma concentrations, detected before dialysis in patients with DH, is a condition not sufficient per se to initiate headache. However, it can be hypothesized that increased CGRP concentrations are required to induce headache if other, hitherto unknown, triggering factors or mediators are produced during dialysis. Finally, an involvement of the trigeminovascular system in the mechanism generating headache cannot be ruled out.
After dialysis treatment, plasma CGRP-LI decreased in both groups of patients. Moreover, measurable concentrations of CGRP-LI were detected in the dialysate which was collected at the end of the procedure. These results indicate that CGRP can be removed by standard bicarbonate haemodialysis which is performed with a copolymer polycarbonate–polyether plate dialyser. CGRP is a 37-amino acid neuropeptide with a molecular weight of 3800 Da (32). Uraemic solutes are arbitrarily divided into several groups, according to their molecular weight and, from this point of view, CGRP can be considered a middle molecule, as well as parathormone and β2-microglobulin (33). Niwa and colleagues (34) have observed that variations in plasma CGRP concentrations of patients after haemodialysis result from the type of dialyser membrane. Plasma concentrations of CGRP increased after haemodialysis using a dialyser made of polymethil methacrylate, decreased after haemodialysis using a high-flux membrane such as polyacrylonitrile and did not change after haemodialyisis using either a cellulose triacetate membrane or a conventional saponified cellulose dialyser. No changes in plasma concentrations of CGRP were also reported during standard bicarbonate haemodialysis where a cuprophan plate dialyser was used (35). The mechanisms by which CGRP concentrations increase or do not change after haemodialysis using certain dialyser membranes remain unclear. Niwa and colleagues (34) have suggested that CGRP may be produced by activated leucocytes or platelets in the dialysers and that the peptide may be used as an index of biocompatibility of membranes. It has also been hypothesized that vasoconstriction induced by hypovolaemia after excess removal of body fluid subsequently stimulates release of CGRP from perivascular nerves (34). The present and previous data suggest that the biocompatibility of the dialyser used in our study and the absence of variations of blood pressure during dialysis blocked the putative mechanisms responsible for activation of CGRP release.
In headache-free subjects, SP-LI was decreased at the end of the dialysis treatment. Measurable amounts of SP-LI were also detected in the dialysate. These results indicate that standard bicarbonate haemodialysis performed using a copolymer polycarbonate polyether membrane is able to clear SP. SP is an undecapeptide (36) which belongs to the tachykinin family (37), with a molecular weight of 1348 Da and it can be considered a middle-sized (middle molecule) uraemic solute (33). To our knowledge, there are few reports of SP measurement during standard haemodialysis. Hegbrant and colleagues (35) observed an increase of SP during standard bicarbonate haemodialysis and hypothesized that the phenomenon occurred to balance the augmentation of vasoconstrictive substances such as neuropeptide Y and plasma renin activity which was observed during the dialysis treatment.
Plasma SP-LI was increased at the end of the dialysis session in headache sufferers. This result is even more clear if considering that a large proportion peptide was removed from plasma by haemodialysis. Chronic inflammation and pain are associated with a number of diseases and it has been proposed that SP, released from endings of primary afferents, plays a role in these conditions (38). SP is also one of the most abundant neuropeptides in the peripheral and central nervous system (39), particularly expressed in nerve fibres distributed around cerebral arteries supplying the dura mater, arachnoid and pia mater of all brain regions (40). Studies carried out in patients with primary headaches or other chronic pain conditions have produced conflicting results. The platelet SP concentration was found to be significantly higher in patients with tension-type headache during the headache phase than in healthy controls (41). Significantly lower concentrations of platelet SP in the headache-free period were detected in patients with episodic tension-type headache compared with controls (42). Salivary SP concentrations during the headache phase in tension-type headache patients have been reported to be significantly increased compared with healthy controls (43). More recently, Ashina and colleagues (44) have found that plasma concentrations of SP are normal in chronic tension-type headache patients and are unrelated to the headache state. While normal concentrations of SP both during and outside of a migraine attack were reported in plasma (15, 16), an increase in saliva SP has been shown during migraine headache (45). Finally, during cluster headache SP concentrations have been reported to be normal in plasma (17) and cerebrospinal fluid (46), but elevated in saliva (45). The observation of augmented SP-LI plasma concentrations in patients who experienced headache during the dialytic procedure, in contrast to the reduction in peptide plasma concentrations occurring in headache-free patients, suggests that during dialysis either SP release is increased or SP metabolism or elimination is decreased. The nature of this phenomenon remains to be elucidated. The intriguing hypothesis that increased SP during DH may be one factor contributing to the ability of CGRP to generate the headache attack is worthy of attention. Nevertheless, the present findings show that measurement of sensory neuropeptides may contribute to clarify the genesis of pain in the otherwise poorly understood condition of DH.
Footnotes
Acknowledgements
We thank Mrs Emilia Galletti for technical help and for preparing the figures.