
Abstract
The aim of this research was to study the prevalence of chronic headache (CH) and associated socio-cultural factors in Turkish immigrants and native Germans. Five hundred and twenty-three Turkish and German company employees were screened using a standard questionnaire. Those who suffered from headaches were also examined by a neurologist. Complete data were available for 471 (90%) subjects. Thirty-four participants (7.2%) had CH. Two independent factors for association with CH could be identified: overuse of acute headache medication (OR = 72.5; 95% CI 25.9-202.9), and being a first-generation Turkish immigrant compared with native Germans (OR = 4.4; 95% CI 1.4-13.7). In contrast, the factor associated with chronic headache was not increased in second-generation Turkish immigrants. Medication overuse was significantly more frequent in first-generation Turkish immigrants (21.6%) compared with second-generation Turkish immigrants (3.3%) and native Germans (3.6%; X 2 = 38.0, P < 0.001). First-generation Turkish immigrants did not contact headache specialists at all, compared with 2.8% of second-generation Turkish immigrants and 8.8% of native Germans (X 2 = 118.4, P < 0.001). Likewise no first-generation Turkish immigrant suffering from CH received headache preventive treatment, compared with 6.6% of native Germans (X 2 = 19.1, P = 0.014). The data from this cross-sectional study reveal a high prevalence of chronic headache as well as a very low utilization of adequate medical care in first-generation Turkish immigrants in Germany.
Introduction
The term chronic headache (CH) usually describes migraine or tension-type headache that occurs on more than 14 days per month (1). Population-based studies suggest that CH is a common disorder and a growing health problem all over the world (2, 3, 5–7). Mechanisms and risk factors leading to the development of CH are still unclear. The majority of studies suggest the pivotal role of overuse of acute headache medication as the main risk factor in developing chronic headache (8, 9). Several epidemiological surveys have suggested a low socio-economic status to be associated with a higher risk of CH as well (10). The aim of the current study was to investigate the influence of socio-cultural factors that could be involved in developing CH.
Turkish immigrants represent the largest non-German population within the Federal Republic of Germany. Due to significant language barriers and socio-cultural and religious differences the integration of first-generation immigrants is rarely achieved, subsequently leading to poor socio-economic conditions and low-income households. Typically, the household income of first-generation immigrants is generated by low-income jobs in the service industry. We therefore studied over 500 subjects in a company that employs first-generation immigrants, second-generation immigrants and native Germans.
Methods
The study population comprised Turkish and German employees of a large company in Germany. We selected this company because besides the German employees, nearly half of the workers were Turkish immigrants and the vast majority of the employees, both Turkish and German, were living in the township. Our data collection took place during 2001 and 2002. Headache types (migraine, tension-type headache, chronic headache) were diagnosed according to the IHS (International Headache Society) criteria.
The study population comprised 523 subjects. All parts of the company structure (workers, trainees, administrators and managers), except those on the night shift, sick leaf or vacation, were included in the study. All subjects were screened using a structured headache questionnaire as described previously (8, 11). Screening interviews were carried out face-to-face by medical students of Turkish origin, who were fluent in both German and Turkish. All subjects who reported having headaches during the previous year were examined by an experienced neurologist of Turkish origin, who also was fluent in both languages. Subjects who reported having headache on more than 14 days per month were considered as patients with CH.
Study participants were asked about their demographic and socio-cultural characteristics, including age, gender, origin, nationality, religion, education, current occupation and fluency in the German language. We also collected data on headache characteristics, and intake of acute and preventive headache medication. Subjects were also asked about their contacts with physicians (headache specialists) as well as with other non-medical therapists (acupuncture, Jacobson muscle relaxation and physiotherapy). Turkish subjects were asked whether they consulted a Hoca (Islamic priest) because of suffering from headaches.
Statistical analysis
We used logistic regression to assess the association of potential associated factors with CH. The origin of subjects (‘ethnicity’, the variable of interest) was divided into three groups: Turkish immigrants of the first generation and Turkish immigrants of the second generation (who had been born and raised in Germany) and native Germans. In order to control for possible confounders we included the following variables into the model: age (interval scaled, years), gender (male vs female), overuse of acute headache medication, education and occupation. Subjects who graduated from high school or university were considered as ‘high education’, otherwise as ‘low education’. Occupation has been divided into ‘high occupation’ (executives) and ‘low occupation’ (subjects in training, workers and skilled workers).
We calculated crude and multivariable-adjusted odds ratios (OR) and their corresponding 95% confidence intervals (CI). We used a stepwise selection procedure to identify the most important multivariable adjusted associated factors for chronic status of headache using a P-value of ≤ 0.02 as inclusion or exclusion criteria. All analyses were performed using SPSS (version 11.0).
Results
We screened 523 subjects. Complete sets of data were available from 471 (90%) subjects. There were 246 women and 225 men, with a mean age of 29.7 ± 6.3 years; 222 (47%) subjects were German natives and 249 (53%) were Turkish immigrants.
Demographic, socio-economic and clinical characteristics of the studied population are shown in Tables 1–3. Overall, 45% of subjects reported having headache in the previous year. Thirty-four subjects (7.2%) fulfilled the criteria of CH, and 21 (4.5%) subjects overused the acute headache medication. Seventeen subjects overused analgesics and four subjects overused ergots.
Demographic and socio-economic characteristics of the studied population

Significant.
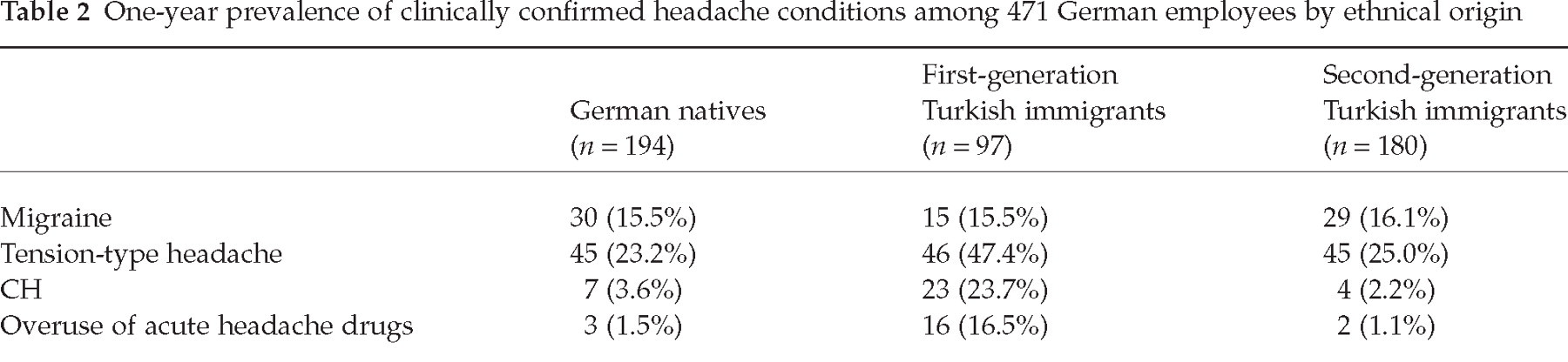
One-year prevalence of clinically confirmed headache conditions among 471 German employees by ethnical origin
Crude and adjusted odds-ratio for the relation of ethnicity to chronic headache

A comparison of demographic and socio-economic features of the studied population revealed that the group of first-generation immigrants was on average older and comprised subjects with a lower socio-economic status, while the subpopulation of the Turkish immigrants of the second generation did not differ from the group of German natives.
The stepwise selection procedures identified two main factors associated with CH: ‘overuse of acute headache medication’ and ‘ethnicity’ of the studied population. Subjects who overused acute headache medication had a higher prevalence of CH (OR = 72.5; 95% CI 25.9–202.9). CH was more than four times more likely (OR = 4.4; 95% CI 1.4–13.7) among Turkish immigrants than among German natives. The prevalence of chronic headache was not increased in Turkish immigrants of the second generation. All other evaluated variables were not included in the final models. Use of a backward elimination procedure yielded the same final model.
Prevalence of medication overuse was higher in Turkish immigrants of the first generation (21.6%) than in Turkish immigrants of the second generation (3.3%) and in Germans (3.6%; χ2 = 38.0, P < 0.001). The first generation of Turkish immigrants did not contact headache specialists at all (vs 2.8% of Turkish immigrants of the second generation and 8.8% of German patients; χ2 = 118.4, P < 0.001) and none of them received headache preventive treatment (vs 6.6% of German patients; χ2 = 19.1, P = 0.014). Twenty-three German headache sufferers (12%), but none of the Turkish headache patients, consulted a headache specialist. Thirteen subjects out of the total population (2.8%) received headache preventive therapy. All these subjects were German. In contrast, none of the Turkish subjects had medical headache prevention. Overall, 40 headache sufferers used non-medical treatment options, such as acupuncture, Jacobson muscle relaxation or physiotherapy. Subjects of Turkish origin of the first generation used non-medical treatment options more frequently than German headache sufferers (28.4% vs 4.5%; P = 0.001). Turkish headache sufferers (15 subjects) frequently contacted a Hoca (Islamic priest), especially Turkish immigrants of the first generation (14 subjects).
We furthermore analysed a subpopulation of subjects with headache. In this subpopulation the odds ratio for medication overuse was 24.0 (95% CI 5.7–104.1) and for ‘ethnicity’ (corrected for age, gender, education, occupation and overuse) 2.7 (95% CI 0.8–9.6).
Discussion
Using a cross-sectional design, we studied a mixed sample of German natives and Turkish immigrants in Germany to evaluate possible socio-economic and cultural factors associated with chronic headache.
We found the 1-year prevalence of headache to be 45%, which is basically lower than in most population-based studies (12–14). Some others, however, have reported comparable results (15). In our study, the lower prevalence could be explained by the fact that we investigated employed subjects, who probably are healthier than subjects of a population-based sample. The prevalence of chronic headache of 7.2% observed in our study was higher than in previous reports (2–7). Subgroup analysis suggests that this was due to a very high frequency (23.7%) in the subgroup of the first generation of Turkish immigrants. The prevalence of CH in the subgroup of Turkish immigrants of the second generation (2.2%), however, was similar to that in German natives (3.6%) and comparable with previous studies. The 1-year prevalence of migraine and tension type headache in both subgroups of Turkish immigrants observed in our study is in line with results of ‘The Turkish Headache Epidemiology Study Group’ (17).
The main finding of our study is that we were able to identify two factors associated with chronic headache: overuse of acute headache medication and being a Turkish immigrant of the first generation. Overuse of acute headache medication is well known as probably the strongest risk factor associated with chronic headache. Many cross-sectional studies demonstrated a coexistence of medication overuse in the majority of patients with chronic headache (2–6). Moreover, recent prospective studies clearly demonstrated that critically frequent use of acute headache drugs is a main risk factor for de novo development of chronic headache (8, 9, 16). In parallel with these reports the majority of subjects in our population overused analgesics. Interestingly, none of the studied patients overused triptans. This fact might indirectly indicate that triptans probably have not yet been introduced to this patient population. This is in line with another observation, that only 23 headache sufferers (all of them Germans) contacted a headache specialist and only 13 patients received headache preventive treatment. These observations clearly suggest a lack of adequate headache care in the studied population, especially in the subgroup of Turkish immigrants of the first generation.
We understand that the very high odds ratio for overuse of acute headache medication can be caused by comparison of subjects with chronic headache with subjects without any headache and therefore not taking any painkillers at all. We therefore analysed the subpopulation of subjects with headache and found a lower odds ratio for medication overuse, which is comparable with a previous study by our group (8).
A group of Turkish immigrants of the first generation had a fourfold increased prevalence rate of having CH. This finding could be explained by the following: Turkish immigrants of the first generation had poor knowledge of German language, were less educated and had a lower socio-economic status. Probably these factors were responsible for poor access to health care facilities. The rate of consultations with headache specialists was the lowest in this group. Consequently, Turkish headache sufferers did not use headache preventive medication but rather ineffective non-medical treatment options. Turkish immigrants of the first generation often consulted a Hoca to treat their headache. Magic conceptions of aetiology and pathogenesis of diseases have a broad acceptance in part of this population. Hocas are authorities to be consulted for treatment. In ritual acts they intend to stave off noxious influences and to strengthen the healing power with sacred formulas and through powerful objects. In contrast, the subpopulation of second-generation Turkish immigrants, who grew up in Germany, did not differ from the subgroup of German natives with regard to socio-economic characteristics. Probably therefore, the prevalence of CH in Turkish immigrants of the second generation was comparable with that in German natives.
In conclusion, our data suggest that inadequate medical care due to language barriers or socio-cultural differences leads to a higher rate of chronic headache. Turkish headache sufferers often do not realize that excessive or frequent self-treatment may perpetuate or exacerbate their headaches. Most of the Turkish headache sufferers of the first generation do not seek medical advice. The opportunity for diagnosis and adequate medical intervention to halt the cycle is often missed. Physicians need to screen CH patients for medication overuse. Turkish headache patients must be informed about the risks of analgesic overuse and rebound headache.
Footnotes
Acknowledgements
This study was supported by the Ministry of Health in Nordrhein-Westfalen, Germany.