
Abstract
We studied the association of chronic headache and chronic rhinosinusitis in 30 000 persons aged 30–44 years from the general population. They received a mailed questionnaire. Those with possible chronic headache were interviewed by neurological residents. The criteria of the American Academy of Otolaryngology—Head and Neck Surgery were applied to diagnose headache attributed to chronic rhinosinusitis (HACRS), otherwise the International Classification of Headache Disorders was used. The questionnaire response rate was 71%, and the participation rate of the interview was 74%. Compared with the general population, persons with chronic rhinosinusitis have an at least ninefold increased risk of having chronic headache. A 3-year follow-up showed that HACRS symptoms were significantly improved after treatment with nasal surgery, nasal corticosteroids, discontinuation of overused headache medications and discontinuation of nasal decongestants or unspecified reasons. Chronic rhinosinusitis is significantly associated with chronic headache, and HACRS is likely to be a distinct type of headache.
Introduction
Diagnostic criteria for chronic rhinosinusitis and headache attributed to rhinosinusitis

One of these signs of inflammation must be present and identified in association with ongoing symptoms consistent with chronic rhinosinusitis (see below):
Discoloured nasal drainage from the nasal passages, nasal polyps or polypoid swelling as identified on physical examination with anterior rhinoscopy after decongestion or nasal endoscopy. Oedema or erythema of the middle meatus or ethmoid bulla on nasal endoscopy. Generalized or localized erythema, oedema or granulation tissue (if the middle meatus or ethmoid bulla is not involved, radiological imaging is required to confirm a diagnosis. Imaging modalities confirming the diagnosis:
Computed tomography (CT) scanning demonstrating isolated or diffuse mucosal thickening, bone changes or air-fluid level. Plain sinus radiograph-Water's view revealing mucous membrane thickening of > 5 mm or complete opacification of one or more sinuses. An air-fluid level is more predictive in acute rhinosinusitis but may also be seen in chronic rhinosinusitis. Magnetic resonance imaging (MRI) is not recommended as an alternative to CT for routine diagnosis of chronic rhinosinusitis because of its excessively high sensitivity and lack of specificity.
Frontal headache accompanied by pain in one or more regions of the face, ears or teeth and fulfilling criteria C and D. Clinical, nasal endoscopic, CT and/or MRI imaging and/or laboratory evidence of acute or acute-on-chronic rhinosinusitis (1, 2). Headache and facial pain develop simultaneously with onset or acute exacerbation of rhinosinusitis. Headache and/or facial pain resolve within 7 days after remission or successful treatment of acute or acute-on-chronic rhinosinusitis.
Notes:
Clinical evidence may include purulence in the nasal cavity, nasal obstruction, hyposmia/anosmia and/or fever. Chronic sinusitis is not validated as a cause of headache or facial pain unless relapsing into an acute stage.
We investigated the risk of chronic rhinosinusitis in persons with chronic headache from the general population and tested the hypothesis that chronic headache is associated with chronic rhinosinusitis.
Materials and methods
This was a cross-sectional epidemiological survey of 30 000 persons, aged 30–44 years from the general population of eastern Akershus County, Norway. The sample was stratified for age and gender. A short postal questionnaire screened our population for chronic headache (≥ 15 days/last month and/or ≥ 180 days/last year). Those with self-reported chronic headache were invited to a clinical interview and examination conducted by neurological residents. The study was conducted at Akershus University Hospital. The explicit diagnostic criteria of the ICHD-II and the revised criteria for medication-overuse headache were applied (4,11–13). We defined secondary chronic headache as secondary headache ≥ 15 days/month for at least 3 months, as the ICHD-II do not provide an explicit definition on chronicity for secondary headaches. Medication overuse was defined as regular intake of simple analgesics or combination of acute medication on ≥ 15 days/month on a regular basis for > 3 months, or intake of one of the following; ergotamine, triptan, opioid, combination analgesics ≥ 10 days/month on a regular basis for > 3 months (11–13). Headache attributed to chronic rhinosinusitis (HACRS) was defined according to The AAO-HNS classification (Table 1) (3). Those with suspected HACRS were examined with anterior rhinoscopy. The participants completed the validated 20-item Sino-Nasal Outcome Test (SNOT-20), which examines general nasal symptoms: need to blow nose, sneezing, runny nose, cough, postnasal discharge, thick nasal discharge, ear fullness, dizziness, ear pain, facial pain/pressure, difficulty falling asleep, waking up at night, lack of a good night's sleep, waking up tired, fatigue, reduced productivity, reduced concentration, frustration/restlessness/irritability, sadness and being embarrassed. Each item is scored from 0 to 5, i.e. not present/no problem, very mild problem, mild or slight problem, moderate problem, severe problem and problem ‘as bad as it can be’.
The Migraine Disability Assessment Score was used to calculate the area under the curve (AUC), i.e. product of headache duration and intensity based on the following two questions: On how many days in the last 3 months did you have a headache? On a scale of 0–10, on average how painful were these headaches?
The response rate to the questionnaire was 71% and the participation rate of the interview was 74%. A more detailed description has been published elsewhere (14,15). Of those with HACRS, 83% (38/46) were followed up after 3 years. Three could not be reached by telephone after at least six attempts at different times, and five were not eligible.
Statistical analyses
Statistical analyses were performed using
Data based on clinical samples from primary care in Norway have reported a yearly incidence of sinusitis of 21.7 per 1000 inhabitants (19). Five persons from a sample of 386 persons with sinusitis were diagnosed as having chronic rhinosinusitis by an ear, nose and throat specialist. The population relative risk of chronic rhinosinusitis in persons with chronic headache was calculated as described above, i.e. by dividing the observed number of affected by expected number.
Ethical issues
The Regional Committees for Medical Research Ethics and the Norwegian Social Science Data Services approved the project. Participation was based on informed consent.
Results
Prevalence
The prevalence of chronic rhinosinusitis in epidemiological surveys
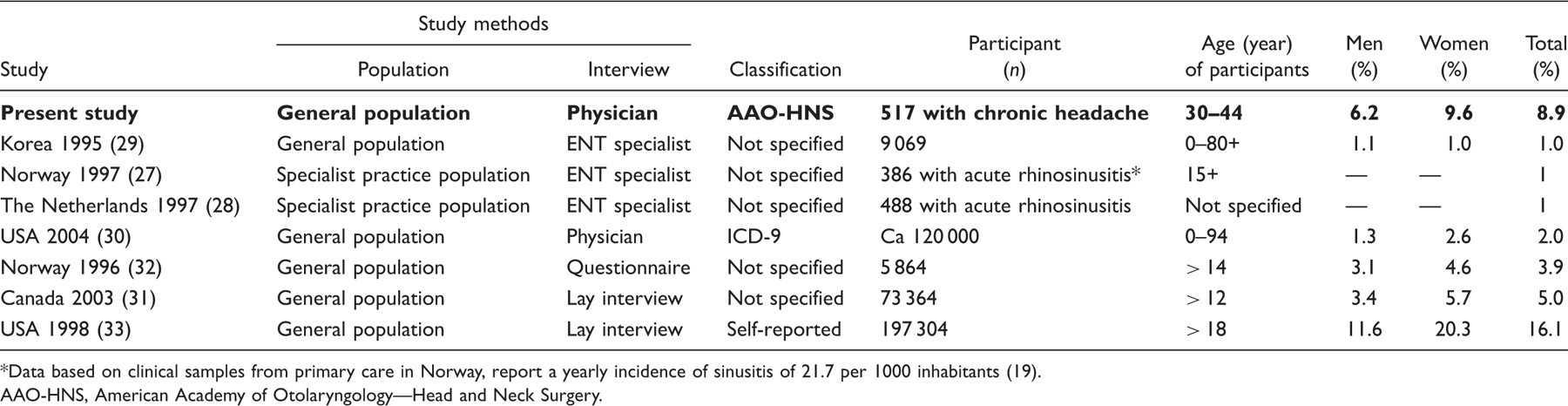
Data based on clinical samples from primary care in Norway, report a yearly incidence of sinusitis of 21.7 per 1000 inhabitants (19).
AAO-HNS, American Academy of Otolaryngology—Head and Neck Surgery.
Age at onset
The mean ages at onset of HACRS and CTTH were equal (22.7 years vs. 23.3 years, P = 0.40). Age and co-occurrence of migraine were significant confounders (P < 0.001). The mean age at onset of men with HACRS was significantly lower in those with than without medication overuse (20.8 years vs. 33.0 years, P = 0.04). Similar differences were not found for women.
Co-occurrence of migraine
Adjusted prevalences of migraine without aura (MO) and migraine with aura (MA) in people with headache attributed to chronic rhinosinusitis

Medication overuse
Twenty-four (five men and 19 women) of the 46 persons with HACRS had medication overuse. The majority (five men and 11 women) were overusing simple analgesics, while seven women had combination medication overuse and one woman had co-occurrence of migraine overused triptans. The prevalence of migraine was not significantly different in those with and without medication overuse (14/24 vs. 8/22, P = 0.14). Medication overuse was not associated with allergy, age at onset of HACRS, use of nasal decongestants or the SNOT-20 score.
Nasal decongestants and allergy
Eleven women with HACRS used nasal decongestants regularly, i.e. > 15 days/month. Those with HACRS were using nasal decongestants regularly more often than those with CTTH (24% vs. 1%, P < 0.001). Allergy was significantly more frequent among persons with HACRS than in those with CTTH (46% vs. 24%, P = 0.002).
Sino-nasal outcome test
The SNOT-20 score was significantly higher among persons with HACRS than in those with CTTH (39.2 vs. 28.5, P < 0.001).
Nasal- or sinus-related symptoms
Distribution of major and minor symptoms of headache attributed to chronic rhinosinusitis

Symptomatology
Pain characteristics and accompanying symptoms of headache attributed to chronic rhinosinusitis

Follow-up
At follow-up 27 persons had a significant reduction of their headache by means of AUC compared with 3 years earlier (mean AUC 322 vs. 158, P = 0.001). Improvement was related to nasal surgery in eight persons, regular use of nasal corticosteroids in four persons and discontinuation of nasal decongestants in three persons, while it was due to unspecified reasons in 12 persons. Of the 27 persons with improvement, 12 of 15 persons no longer had medication overuse. Eleven persons had unchanged headache and did not report having tried any interventions the last 3 years. Four of five of these continued to have medication overuse.
Discussion
Methodological considerations
The sample size was chosen to ensure adequate numbers of subjects with chronic headache for accurate descriptive statistics. The age range 30–44 years was chosen because the prevalence of chronic headache is higher than in a younger age range, whereas comorbidity of other diseases is less than in an older age range. As this was an epidemiological survey on headache, headache could be over-represented among responders to the questionnaire. However, similar replies to the first, second and third issued questionnaire suggest that the latter is not likely. Furthermore, a previous Danish epidemiological survey found no significant difference in the frequency of migraine among responders and non-responders (17). Questionnaires are generally not valid for diagnosing headache (20). However, a single question about self-reported migraine is a valid screening for migraine (17,20,21). Diagnosing headache is not an easy task, especially among those with chronic headache or those with co-occurrence of several headaches. The gold standard is an interview and a physical and neurological examination by a physician experienced in headache diagnostics. For that reason, neurological residents with experience in headache diagnostics conducted our investigation. Our data on migraine were adjusted according to age and gender when compared with Danish prevalence data, due to different age and gender composition in order to make the data comparable (17). Age, gender and co-occurrence of migraine are known to be confounders of CTTH, and for that reason we corrected for these factors in our analyses (21,22).
The AAO-HNS classification was used since HACRS is not accepted as a diagnosis in the ICHD-II. The diagnosis was given based on the headache history and clinical findings. We did not include a computed tomography scan of the sinuses in the study, since there is a discrepancy between radiological and clinical findings (23,24).
Prevalence
We found that the prevalence of HACRS was 0.33%, 0.13% in men and 0.48% in women. This is a prevalence eight times higher than reported in a Spanish epidemiological survey on chronic headache, where the prevalence of ‘headache associated with disorders of sinuses’ was 0.04%, diagnosed on slightly different criteria (25,26).
As presented in Table 2, chronic rhinosinusitis is common and is reported to affect 1–16% of the adult general population (27–33). The prevalence variability is most likely to be caused by lack of uniform definitions and different sampling methods (34,35). It is reasonable to believe that the most precise data are those provided by physicians and that lay interviews and questionnaires may be less precise. The prevalence of chronic rhinosinusitis could be influenced by race, climate and geographical area; accordingly, we used Norwegian data for our comparison. Data from the Netherlands are quite similar to those of Norway, as five of 488 patients with suspected sinusitis developed chronic complaints after 1 year (28). From these two studies it seems that acute sinusitis may develop into chronic sinusitis. The prevalence of chronic rhinosinusitis is estimated to be 1% in the Norwegian population. Thus, patients with chronic headache have an at least ninefold increased risk of chronic rhinosinusitis compared with the Norwegian general population. This calculation was based on a mean exposure of 37 years. However, children and adolescent rarely have chronic headache (36). If we had calculated with a mean exposure of 18 years, our result would be an 18-fold increased risk of chronic rhinosinusitis compared with the Norwegian general population.
Co-occurrence of migraine
The co-occurrence of migraine and the frequency of migraine attacks among those with HACRS were equal when compared with those with CTTH (22). A recent study has shown an increased risk of MO and increased frequency of MO attacks among persons with CTTH when compared with the general population, whereas MA did not seem to be interrelated with CTTH (22).
Medication overuse
Medication overuse in those with HACRS was similar to medication overuse in those with CTTH (22). This may imply that the association between headache and medication overuse is similar in HACRS and CTTH. Furthermore, almost all those with HACRS who had improved at follow-up and who were also medication overusers had stopped overusing their medications. Those who had not improved were in general still medication overusers at follow-up. It is a strong inverse relationship between medication overuse and headache improvement, although the direction of the causality can not be ascertained in our study.
Is HACRS an aetiologically distinct type of headache?
Comparison with CTTH was systematically performed because all 46 persons diagnosed with HACRS would have fulfilled the criteria for CTTH if the symptoms from the sinus region were not explored. HACRS and CTTH show both similarities and differences. The similarities are equal age at onset, headache symptomatology, prevalence of co-occurrence of migraine and medication overuse. All except three persons with HACRS had bilateral complaints, which in fact support the HACRS diagnosis, since the majority of patients with chronic rhinosinusitis referred to endoscopic sinus surgery have bilateral symptoms (37). Bilateral location is also typical for tension-type headache.
The differences are nasal- or sinus-related symptoms, regular use of nasal decongestants, frequent allergy and a high SNOT-20 score. Approximately 50% of those with HACRS reported allergy and 25% reported frequent use of nasal decongestants. Allergy is known to be an important predisposing factor for chronic rhinosinusitis. Rhinitis medicamentosa may be a cause of recurrent and chronic symptoms of nasal obstructions (38). A high SNOT-20 score is known to be associated with chronic rhinosinusitis, but also reflects high disability in general (39). Clinically, our patients with HACRS had positive symptoms according to the AAO-HNS classification, e.g. longstanding oedema of the nasal mucosa, which is a result of chronic rhinosinal inflammation.
Patients with chronic rhinosinusitis experience headache relief after sinus surgery (2,10,40,41). Our follow-up-data also indicate that nasal surgery contributes to headache relief, since a relatively high proportion of our chronic headache sufferers experienced pain relief after nasal surgery. Topic nasal corticosteroids were reported as the second most frequent reason for headache improvement. One of the participants was awaiting surgery because of the discovery of an ethmoidal cyst, and she experienced great headache relief by taking prednisolone tablets daily. The cessation of medication overuse may also contribute to improvement of headache.
One of the authors has extensive experience in the management of CTTH. Although not systematically recorded, about 10 patients within the last 2 years who did not respond to the usual prophylactic treatment for CTTH had an excellent effect with nasal corticosteroids, possibly due to their co-occurrence of nasal complaints.
Our results strongly indicate that chronic headache and chronic rhinosinusitis are interrelated, and that HACRS is likely to be an aetiologically distinct type of headache.
Footnotes
Acknowledgements
This study was supported by grants from the East Norway Regional Health Authority and Faculty Division Akershus University Hospital. Akershus University Hospital kindly provided research facilities.