
Abstract
This study investigated the impact of migraine on health-related quality of life (HRQoL) among patients with major depressive disorder (MDD). We prospectively enrolled 151 consecutive psychiatric out-patients meeting DSM-IV criteria for MDD. Migraine and other headache types were diagnosed based on the International Classification of Headache Disorders, 2nd edition (2004). The Short Form-36 (SF-36) was administered as a generic instrument of HRQoL. Among 151 patients with MDD, migraine (N = 73, 48.3%) was very common. Comorbidity of migraine predicted a significantly negative impact on all physical subscales and vitality but not on the other mental subscales of the SF-36 after controlling for depression, age and gender. The presence of migraine should be considered as an important physical symptom in clinic-based MDD samples. Simultaneous management of depression and severe headaches, especially migraine, might improve HRQoL in patients with MDD.
Introduction
Depression is one of the most common disorders causing disability. The overall economic burden of depression is comparable to that of serious physical illness, such as cancer or heart disease (1). Pain and other physical symptoms in patients with depression have gradually come to be emphasized because: (i) physical symptoms and pain interfere with accurate diagnosis and treatment (2); (ii) residual physical symptoms or pain after treatment impede complete remission of depression and predict early relapses (3); and (iii) depression with painful physical symptoms increases the economic burden of depression (1).
Headache is one of the most common physical and pain symptoms in patients with depression (2). Among different headache diagnoses, migraine is the most commonly studied headache type associated with depressive disorders (4–9). There is even evidence suggesting a close relationship between migraine and depression. A bidirectional relationship was observed between depression and migraine, with migraine predicting first-onset depression and depression predicting first-onset migraine (5). However, studies focusing on migraine among patients with major depressive disorder (MDD) are sparse, and in these studies only the frequencies of different headache types were reported (8–11).
Measuring patient-perceived health-related quality of life (HRQoL) has become one of the most important outcomes in health care. HRQoL instruments measure patients’ perceptions of daily functioning and well-being in physical, social, and psychological dimensions. Migraine and depression significantly decrease HRQoL (12–14). Nevertheless, their relationships are complex and not well understood. One population-based study demonstrated that patients with migraine had lower HRQoL even after controlling for depression (14). The more frequent the migraine attacks, the poorer the HRQoL (14). In contrast, previous studies on HRQoL among patients with MDD did not consider the impact of headache (12). Indeed, the impact of migraine on HRQoL in patients with MDD has never, to our knowledge, been reported. The purpose of this study was to investigate the impact of migraine on patients with MDD.
Methods
This prospective study was conducted in the Psychiatric Outpatient Clinic of Chang-Gung Memorial Hospital, a medical centre located in northern Taiwan, from November 2001 to October 2002. The government-run single-payer compulsory National Health Insurance programme in Taiwan enrolled more than 96% of Taiwan's population (15). Unlike USA or British managed care models, the insured in Taiwan has complete freedom to choose their healthcare providers. They can seek care at tertiary care institutions, regardless of the severity of their illness. Only 2.3% of patients in the clinics of a university teaching hospital in Taiwan were referred from primary clinics (16). Therefore, although our sample was collected from a medical centre, it did not greatly differ from the demographic patterns of patients attending primary psychiatric clinics.
Participants
Consecutive out-patients, 18–65 years of age, who presented at our psychiatric clinic for the first time and had never been treated with antidepressants, were interviewed by board-certified psychiatrists using the Mini-International Neuropsychiatric Interview (17). Patients who met the DSM-IV criteria for MDD (18) and experienced a major depressive episode (MDE) were enrolled after providing written informed consent and undergoing a neurological examination. To confirm that the severity and pattern of headaches had not been affected by medication or other medical conditions, the following exclusion criteria were established: (i) patients regularly treated with headache prophylactic agents in the previous month, because these treatments might confound the severity of depression or headache; (ii) patients with secondary headache, stemming from conditions such as brain tumours, encephalitis, stroke, or head injury; (iii) patients with a history of abuse or dependence on opioids or their derivatives, amphetamine or its derivatives, cocaine, cannabis, hallucinogens, inhalants, or alcohol; and (iv) patients with psychotic symptoms, catatonic features, or severe psychomotor retardation with obvious difficulties in being interviewed. It is of note that patients with medication overuse were not excluded because they were very common among headache patients. Moreover, patients with medication overuse headache (MOH) were not excluded from the category of chronic daily headache (CDH) based on the Silberstein–Lipton's (S-L) criteria (19).
The depressive severity of subjects who fulfilled these inclusion and exclusion criteria was evaluated using a 17-item Hamilton Depression Rating scale (HAMD) (20).
HRQoL assessment
We used the Short-Form 36 (SF-36), a widely used generic questionnaire, to assess HRQoL. The SF-36 questionnaire is a self-administered, 36-item questionnaire that measures HRQoL across eight dimensions: physical functioning (PF), role limitations-physical (RP), bodily pain (BP), general health perceptions (GH), vitality (VT), social functioning (SF), role limitations-emotional (RE), and mental health (MH) (21). According to the originators of the SF-36, these eight dimensions can be grouped into two health subscales: the physical subscales (PF, RP, BP, GH) and the mental subscales (VT, SF, RE, MH). The responses to items within each dimension are summed and linearly transformed to produce dimension scores ranging from 0 (lowest well-being) to 100 (highest well-being). The Taiwanese version of the SF-36 shows good validity and reliability (22, 23).
Headache diagnosis
All patients were asked to complete a structured headache intake form. This intake form contained 42 items based on the headache criteria proposed by the International Headache Society (IHS) (1988) (24). It was designed for both clinical and research use and emphasized the collection of information regarding lifetime headache history and current headache severity and the classification criteria of migraine or tension-type headache (TTH). Questions regarding the frequency, intensity, features, aura, location, duration, and precipitating factors of headache as well as frequencies and amount of painkiller usage were included. Moreover, subjects were requested to evaluate the headache intensity of their severe headaches in the past year on a numerical scale (0–10). To validate questionnaire contents, especially focusing on the frequency, intensity, features, and duration of headaches, after completing the headache intake form, patients were interviewed by an investigator who was blind to the results of psychiatric evaluation.
Although this study was performed during 2001 and 2002, the headache diagnoses were made based on new criteria of the International Classification of Headache Disorders, 2nd edition (ICHD-II) (2004) (25), for comparison with future studies. Since all headache profiles in each patient were well recorded, this made the application of ICHD-II criteria possible. In fact, the major criteria for migraine and TTH did not change greatly between IHS criteria (24) and ICHD-II (25). All headache intake form and interview results were re-evaluated for headache diagnoses based on the ICHD-II criteria.
To establish a diagnosis of ICHD-II migraine (i.e. migraine without aura), the following criteria had to be met: (i) five or more attacks per lifetime; (ii) headache attacks lasting 4–72 h if untreated or unsuccessfully treated; (iii) at least two of the following features: (a) unilateral location, (b) pulsating pain, (c) moderate or severe pain intensity, and (d) aggravation by or causing avoidance of routine physical activity; and (iv) at least one of the following: (a) nausea or vomiting, (b) photophobia and phonophobia. Migraine is frequently comorbid with other headache syndromes in clinical practice. However, compared with TTH or other headache syndromes, migraine is considered to be a more severe type of headache and causes more disability (13). Therefore, patients who fulfilled migraine diagnostic criteria and also had features fulfilling other headache characteristics, such as TTH, were categorized as migraine. This might not be a thorough method or even the best method of categorization, but it is easily applied for analysis since this study had been planned to focus on the diagnosis of migraine.
In patients with migraine, chronic migraine (CM) was diagnosed if patients had migraine without aura occurring ≥ 15 days per month during the last 3 months in the absence of medication overuse. Those who fulfilled the criteria for CM and probable MOH were diagnosed as probable CM and probable MOH. Subjects with migraine but who did not fulfil the criteria for CM or probable CM were classified into an episodic migraine group. The diagnosis of chronic tension-type headache (CTTH) was made if the subject had had headache for ≥ 15 days/month on average for > 3 months; headaches which lasted hours; and at least two of the following characteristics were present: a pressing/tightening quality, mild or moderate severity, bilateral location, no exacerbation on movement; no more than one of the following symptoms: mild nausea, photophobia, or phonophobia; and neither moderate nor severe nausea nor vomiting. Patients who fulfilled the criteria of CTTH but also overused medications were diagnosed as probable CTTH and probable MOH. CM and probable CM were grouped as a CM group, CTTH and probable CTTH, as a CTTH group. This was done because our study had a cross-sectional design and it is very difficult to withhold antidepressant treatment for 2 months to observe the effect of the withdrawal of overused medications because of the potential risk of suicide in MDD patients.
Statistical analysis
All statistical analyses were carried out using the Statistical Package for the Social Sciences (SPSS) for Windows 10.0 (SPSS Inc., Chicago, IL, USA). To understand further the impact of different headaches on HRQoL, patients were divided into six major headache diagnostic groups: CM, episodic migraine, CTTH, episodic tension-type headache (ETTH), other headache, and ‘headache-free’ groups. One-way analysis of variance (
In testing the impact of migraine, patients in the CM and episodic migraine groups were categorized as ‘migraine’, while other patients were ‘non-migraine’. General linear models were used to investigate the impact of migraine on each scale of the SF-36 after controlling for age, gender, and the severity of depression (HAMD scores). The estimated difference in score was calculated for each subscale the SF-36 contributed by migraine. A P-value < 0
Results
Study participants
During the study period, 170 consecutive patients were diagnosed for the first time as MDD at our clinic, of whom eight (two men and six women) were excluded due to having been treated previously by antidepressants. Of the remaining 162 fulfilling the diagnostic criteria for MDD and other study criteria, 151 (93.2%) (34 men, 117 women) agreed to participate in the study. The refusal rates did not differ significantly between men (N = 3, 8.1%) and women (N = 8, 6.4%) (χ2 test, P = 0.72).
Among these 151 participants, 134 (88.7%) reported having a headache history. Episodic migraine (N = 52, 34.4%) was the most common headache type (Table 1). Within the migraine category (including CM and episodic migraine groups), 54 (74.0%) had migraine without aura and 19 (26.0%) had both migraine with and without aura. The demographic data of these six major headache diagnostic groups are shown in Table 1. The CM group (N = 21), including 14 C M and seven probable CM with probable MOH, was larger than the CTTH group (N = 11), including 10 CTTH and one probable CTTH with probable MOH. Other headache group included nine probable migraine, 11 probable TTH, and three headache unspecified. MDD patients comorbid with CM showed higher HAMD scores than ETTH or the ‘headache-free’ group.
Demographic data for different headache groups among 151 patients with major depressive disorder a
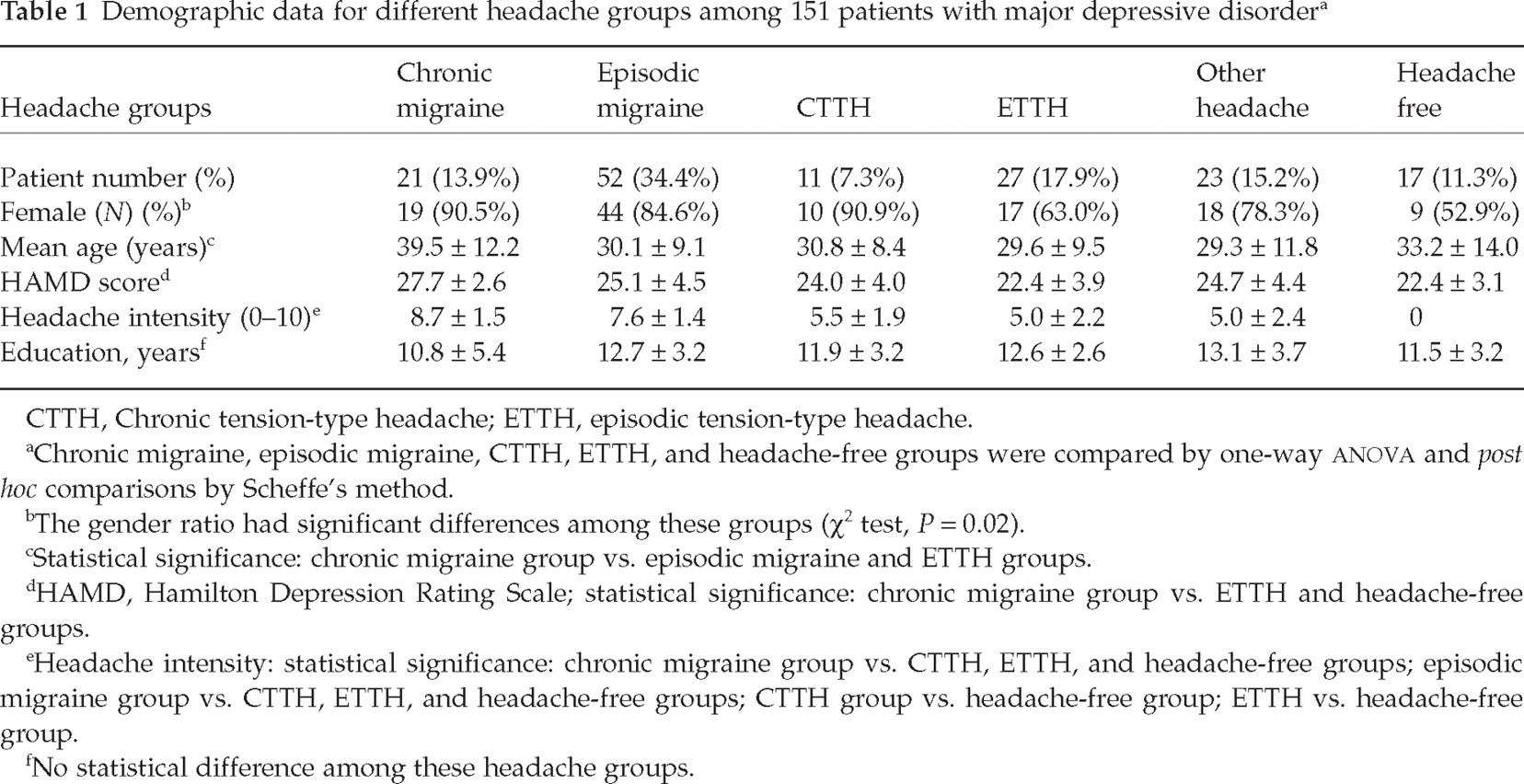
CTTH, Chronic tension-type headache; ETTH, episodic tension-type headache.
Chronic migraine, episodic migraine, CTTH, ETTH, and headache-free groups were compared by one-way
The gender ratio had significant differences among these groups (χ2 test, P = 0.02).
Statistical significance: chronic migraine group vs. episodic migraine and ETTH groups.
HAMD, Hamilton Depression Rating Scale; statistical significance: chronic migraine group vs. ETTH and headache-free groups.
Headache intensity: statistical significance: chronic migraine group vs. CTTH, ETTH, and headache-free groups; episodic migraine group vs. CTTH, ETTH, and headache-free groups; CTTH group vs. headache-free group; ETTH vs. headache-free group.
No statistical difference among these headache groups.
The correlation of subscales of SF-36, the severity of depression, and headache intensity are shown in Table 2. HAMD score was significantly correlated to subscales of the SF-36 except for the RE and SF subscales. Headache intensity was significantly correlated to all subscales of the SF-36. Moreover, the correlation between headache intensity and HAMD scores was also significant (r = 0.33, P < 0.001) in our participants.
The Pearson correlation coefficients of the severity of depression, headache intensity, and each subscale of the SF-36

HAMD, Hamilton Depression Rating Scale; PF, physical functioning; RP, role limitations-physical; BP, bodily pain; VT, vitality; GH, general health; SF, social functioning; RE, role limitations-emotional; MH, mental health.
Headache intensity of the severe headache in the past year on a 0–10 scale.
HRQoL among six headache groups
The scores on eight subscales of the SF-36 among the six headache diagnostic groups are shown in Fig. 1. Statistically significant differences among five groups in different SF-36 subscales – using one-way

Comparison of SF-36 scores among patients with major depressive disorder comorbid with different headache types. CM, Chronic migraine group; Migraine, episodic migraine group; CTTH, chronic tension-type headache; ETTH, episodic tension-type headache; PF, physical functioning; RP, role limitations-physical; BP, bodily pain; GH, general health; VT, vitality; SF, social functioning; RE, role limitations-emotional; MH, mental health.
There was a trend for the CM group to have the poorest HRQoL, followed by the episodic migraine group. Among the eight subscales of the SF-36, the scores of the BP and PF, which belong to the physical subscales, were the most discrepant among these groups; conversely, the scores of MH, SF, and RE, which belong to the mental subscales, did not differ statistically.
When the headache-free group was used as a reference, the biggest difference from the CM group was demonstrated for BP (mean difference 45.4 points, 59.7% lower), followed by PF (28.5 points, 31.4% lower), RP (28.0 points, 59.6% lower), and RE (22.7 points, 82.2% lower). The difference in the SF-36 score was less for the episodic migraine group: RP (22.5 points, 47.9% lower), BP (34 points, 44.7% lower), and PF (17.9 points, 19.7% lower).
Impact of migraine on the scale scores of the SF-36
The impact of migraine on each dimension of the SF-36 was calculated by setting migraine as the main factor in a general linear model after controlling for age, gender, and the severity of depression. The results are presented in Table 3. Migraine patients, compared with non-migraine patients, had clinically (scale scores > 5 points) and statistically poorer HRQoL on most subscales of the SF-36 except for SF, RE and MH subscales. It was noted that the decrease on physical subscales was greater than on mental subscales, such as BP (estimated difference = 22.3 points), RP (24.6 points), and PF (12.2 points). By using this model, we found that migraine accounted for 14–32% of the variance of all four subscales of the physical subscales and one mental subscale: VT.
Results of general linear modelling to calculate the estimated difference on each subscale of the SF-36 by using migraine as the main factor after controlling for age, gender, and the severity of depression a

Migraine included chronic migraine, probable chronic migraine, and episodic migraine; the severity of depression = the scores of Hamilton Depression Rating Scale; PF, physical functioning; RP, role limitations-physical; BP, bodily pain; VT, vitality; GH, general health; SF, social functioning; RE, role limitations-emotional; MH, mental health.
P < 0.05.
Discussion
In our study, we found migraine, either episodic or chronic, in MDD patients was associated with a further decrease in HRQoL (evaluated by the SF-36). About half of our clinic-based patients with MDD were diagnosed as having migraine. When using the headache-free group as a reference, patients in the CM group, i.e. CM or probable CM, showed 20–80% lower scores on the different dimensions of the SF-36, whereas patients with episodic migraine had 15–60% lower scores except for the SF subscale. In our MDD patients, headache severity was correlated with depression scores, which was in line with a previous study recruiting patients visiting primary care physicians (26). The severity of depression in this study also had a moderate correlation with all physical subscales of the SF-36. Therefore, poorer HRQoL among MDD patients comorbid with migraine might result not only from the effect of migraine but also from an interaction between depression and migraine. However, overall, migraine was still an important factor associated with a negative impact on HRQoL among MDD patients even after controlling for the severity of depression, age and gender.
It was found that MDD patients with migraine showed more impairment in the physical subscales (especially in RP, BP and PF) than in the mental subscales. Less difference in mental subscales might result from depressed mood and impairment in social or occupational functions, which were diagnostic criteria for MDD (18). However, a lower impact of migraine on mental subscales also implies that the impact of severe headache might be neglected in the management of these patients, because severity of depression is the major concern of physicians in treating MDD patients and most scales for depression have few items for pain (27). One recent study reported that increased pain severity in patients with MDD was not only associated with worse depression and poorer HRQoL across all dimensions, but also had a negative impact on responses to treatment for depression (28). Therefore, neglecting headache, especially migraine, in the treatment of depression might impede complete remission.
MDD patients with CTTH did not have such a low HRQoL score as did patients with CM, but their SF-36 scores were non-significantly higher than those in patients with episodic migraine. This result was different from that in our previous study conducted in a headache clinic, which showed that patients with CM or CTTH had poorer HRQoL than those with episodic migraine (13). The exact cause for this discrepancy is unknown. It is well known that multiple or vague pain or soreness is not uncommon in patients with MDD (2). The impact of persistent mild or moderate pain caused by CTTH is similar to that of other vague somatic discomforts or pain with only limited impact. This finding is compatible with one recent report that increased headache intensity, but not headache frequency, was associated with higher levels of headache-related disability, depression and emotional distress (29). In fact, our study also demonstrated that the intensity of severe headaches in the past year was correlated to subscales of the SF-36. Therefore, headache intensity might be a more important factor for predicting disability than headache frequency. In patients with MDD, frequent or episodic severe pain, such as that of CM or episodic migraine, predicts a poorer HRQoL than persistent mild or moderate pain, such as that of CTTH. It is also possible that healthcare-seeking behaviour is determined by disease severity, i.e. patients with more severe depression might be more likely to consult psychiatrists, whereas patients with more severe CTTH might visit headache clinics. This might explain the reported discrepancy in HRQoL scores in CTTH patients in headache vs. psychiatric clinics.
Some methodological issues or limitations should be addressed. First, patients in this study were limited to those who had never been treated with antidepressants. This criterion prevented the confounding treatment effect on headaches or migraine by antidepressants. Second, the SF-36 was not designed to measure limitations or restrictions specifically associated with migraine or depression. Nevertheless, the strength of this study is that previous studies of headache and HRQoL frequently used the SF-36 to evaluate HRQoL. Therefore, using the same instrument makes comparisons between these studies possible. Third, the lack of diary recording of headache pattern change after the withdrawal of deleterious overused medications hindered the diagnosis of ‘definite’ MOH, CM or CTTH in those CDH patients with medication overuse based on the ICHD-II criteria. Finally, our sample had a higher percentage of female patients, possibly because of the higher medical care-seeking behaviour as well as the higher lifetime prevalence of MDD in women (30).
Comorbid headache disorders, especially migraine, have important implications for treatment of patients with MDD. First, comorbidity with migraine is very common in patients with MDD in clinic-based studies such as our own and previous studies (10, 11). Second, comorbid headache disorders should be addressed if treatment is to remedy impairments and improve HRQoL, since comorbid migraine causes a further impairment of HRQoL in MDD patients. Third, the presence of a second illness provides therapeutic opportunities. In certain cases, migraine and MDD may be treated together with a single drug. Fourth, treatment of physical symptoms is considered to be increasingly important in the comprehensive treatment strategy for MDD patients if complete remission or relapses are taken into consideration (3, 27).
Footnotes
Acknowledgements
This study was supported in part by National Science Council grants (NSC 93-2314-B-182A-200), Chang-Gung Research Program (CMRPG32010), and Veterans General Hospital (VGH 331).