
Abstract
Pain syndromes are often associated with depression. In a prospective study we analysed if determinants of depression differ among patients with different primary headaches and between headaches and non-headache pain. During a 2-year period between 1 February 2002 and 31 January 2004, 635 subjects (migraine n = 231; tension-type headache n = 176; cluster headache n = 11; patients with low back pain n = 103; and healthy subjects n = 114) seen by two neurologists filled in a questionnaire on pain characteristics, the MIDAS questionnaire and the Beck Depression Inventory. A multivariate general regression model was used to identify independent predictors of the severity of depressive symptoms. Pain was most frequent in chronic tension-type headache and most intense in the cluster subgroup (P < 0.001, Kruskal-Wallis ANOVA). In univariate tests gender, age, pain frequency, pain intensity and disability were all significantly associated with the severity of depressive symptoms. In the multivariate model disability was the most important independent determinant of the severity of depressive symptoms in the pooled headache group as well as in the migraine and tension-type headache subgroups. In contrast to patients with headache, pain frequency and pain intensity were the significant independent predictors of the severity of depressive symptoms in patients with low back pain. In a multivariate model, after controlling for other factors, determinants of the severity of depressive symptoms were different in headache and non-headache pain subjects, suggesting a different mechanism for developing depression in primary headaches and in other pain syndromes.
Introduction
Primary headaches – mainly tension-type headache and migraine – as well as depression affect a significant portion of the population. The coexistence of a primary headache and depression in the same patient might be a coincidence due to the high prevalence of these conditions, but there might be a causal relationship between them, or headaches and depression might have a common background (1). Depression is more prevalent in headache patients than in the headache-free population, and this association was found to be more dependent on headache frequency than the headache diagnostic category (2).
Headaches cause a considerable disability in everyday activities and a positive relationship was found between depression and disability in headache (3). In a Canadian study of 115 migraine sufferers, higher mean headache intensity levels were associated with higher levels of headache-related disability, and there was a tendency for the association of increased headache intensity with higher levels of depression (4). In contrast to pain intensity, headache frequency did not correlate with disability and depression in this study, a finding challenging the results of Zwart et al. (2). Migraine and depression are highly comorbid and each exerts a significant and independent influence on health-related quality of life (5). In a sample of both migraine and non-migraine headache patients, a significant association was found between the migraine disability score (MIDAS (6)) and the presence of depression (7). In contrast to migraine, the effect of other primary headaches on the quality of life has been evaluated by few studies. Chronic tension-type headache was found to have a greater impact on individuals’ lives than has generally been realized, with affective distress being an important correlate of impairment (8).
Pain syndromes other than headaches are also known to be associated with depression (9). In a study of Marcus (10), pain characteristics, depression and disability differed in patients with headache and non-headache pain, and the latter group had more severe depression and disability.
We hypothesized that the severity of headache-associated depressive symptoms is determined by several factors, including the gender and the age of the patient, the frequency and the intensity of the pain, and the disability caused by the pain. We also assumed that the structure of this relationship might differ among patients with different headache categories as well as between headache patients and a patient group of non-headache pain. To test these hypotheses we performed a 2-year prospective study in two neurology practices and included patients with primary headache as well as those with low back pain.
Patients and methods
All consecutive patients with either migraine, tension-type or cluster headache, consulted by two neurologists in a 2-year period between 1 February 2002 and 31 January 2004, were asked to fill in a questionnaire containing the age and gender of the patient, the duration of the headache history, the frequency, duration, severity and other characteristics of pain. Consecutive patients below 60 years of age with low back pain but free from primary headache, examined by the same two neurologists, were included as a non-headache pain patient group. A healthy control group was recruited from a local cardiovascular screening programme, including a neurological examination, offered to all employees of the local branch of the national telephone company by its health insurance system. Consecutive participants of this screening programme seen by one of the authors (D.B.), who declared themselves healthy and free of headache or other pain, were asked to fill in the same questionnaire. As some of these healthy subjects eventually reported some headaches in the written questionnaire, we exclude those who reported either more than one headache day per month even if the headache was very mild, or who had a headache more severe than 5 on a scale from 0 to 10 even once in the preceding 3 months, where 0 means no headache and 10 means an extremely severe headache. The migraine disability score (MIDAS) questionnaire was used to evaluate the impact of headache on work, household and social activities (6). Severity of depressive symptoms was evaluated by the Beck Depression Inventory (BDI (11)). Headache diagnoses were assigned using the criteria of the Headache Classification Committee of the International Headache Society (12). The study was approved by the Ethics Committee of the University of Debrecen, and all participants signed an informed consent after reading and understanding the purpose of this study.
Data are presented as means ± SD or medians with 25 and 75 percentiles. Normality of continuous variables was checked by the Shapiro–Wilk test. The Mann–Whitney test, the Kruskal–Wallis
Results
Characteristics of study population
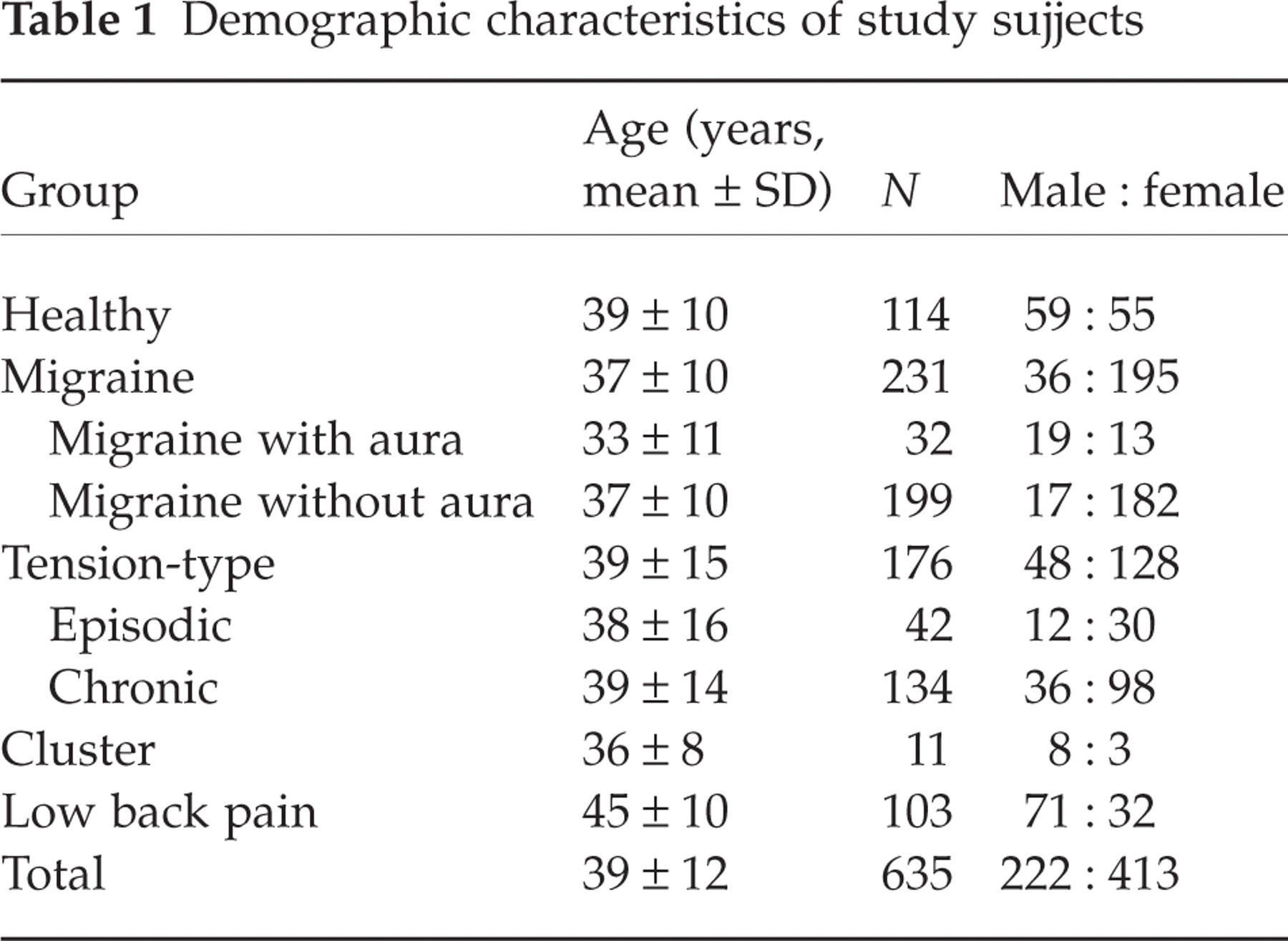
Demographic characteristics of the study population are given in Table 1. The mean age of the 635 subjects was 39 years, and about two-thirds of the study subjects were women. Severity of depressive symptoms and of disability in each subgroup is given in Table 2. There was a statistically significant difference among groups for the Beck score and the MIDSAS score also (Kruskal–Wallis

Pain frequency in subject groups. Values are medians, 25 and 75 percentiles and min–max values. MA, Migaine with aura; MoA, migraine without aura; ETTH, episodic tension-type headache; CTTH, chronic tension-type headache. There was a statistically significant difference among the groups (Kruskal–Wallis

Pain severity in patient groups. Values are medians, 25 and 75 percentiles and min–max values. MA, Migaine with aura; MoA, migraine without aura; ETTH, episodic tension-type headache; CTTH, chronic tension-type headache. There was a statistically significant difference among the groups (Kruskal–Wallis
Demographic characteristics of study sujjects
Severity of depressive symptoms and disability

Values are: medians and 25 and 75 percentile values. Values below the 25 percentile represent the first quartile, values between the 25 percentile and the median are the second quartile, values between the median and the 75 percentile represent the third quartile and values over the 75 percentile are the fourth quartile for the Beck and the MIDAS scores.
Univariate correlates of depressive symptoms
We checked if gender, age, pain frequency, pain intensity and disability have significant effects on the severity of depressive symptoms separately in healthy controls, in patients with low back pain, in patients with headache and in the total study population (Table 3). As in headache patients as well as in the total study population all of these factors had a significant effect on the Beck score (female gender, higher age, more frequent and more intense pain, and more severe disability were associated with more severe depressive symptoms), all of these factors were entered in a multivariate model to test which factors remain significant (i.e. independent predictors of depression severity) after controlling for the effect of other factors.
Significance levels of univariate tests regarding the severity of the depressive symptoms in different patient groups

The Mann–Whitney test was used to test the effect of gender on the severity of depressive symptoms. The Spearman rank order correlation was applied to test the relationship between the severity of depressive symptoms (i.e. the Beck score) and age, pain intensity, pain severity and disability, respectively.
Independent predictors of the severity of depressive symptoms
The result of the multivariate test is shown for the headache population (including all patients with migraine, tension-type, or cluster headaches) in Fig. 3. Although the levels of disability and age are the most significant determinants of the severity of depressive symptoms in headache patients, the frequency of pain and gender also had significant effects in the total headache group.

Determinants of the severity of depressive symptoms in all subjects with headache in a general regression model. Disability (the MIDAS score), age, frequency of headache and gender are significant independent predictors of the severity of depressive symptoms in the pooled headache group. Of these factors, disability is the most important determinant: t = 6.65, P < 0.0001, regression coefficient 0.344 (95% confidence interval 0.242, 0.446).
In the final analysis the general regression model was applied separately for the migraine and tension-type headache subgroups and for the group with low back pain to test if the predictors of the severity of depressive symptoms do or do not differ among these subgroups (Table 4). Due to the small number of cases, the cluster group (n = 11) was omitted from this analysis. It can be seen that disability is the most important independent predictor of the severity of depressive symptoms in all of the headache subgroups, but not in low back pain. Age is also a significant or at least a marginally significant predictor in chronic tension-type headache and in migraine without aura, but not in the low back pain subgroup. Pain frequency was not an independent significant predictor in any of the headache subgroups, and headache intensity remained significant only in the chronic tension-type headache subgroup after controlling for the other variables. In contrast to the headache subgroups, pain intensity and frequency, but not disability and age, were significant independent predictors of the severity of depressive symptoms in patients with low back pain.
Independent determinants of the severity of depressive symptoms in the different patient groups

The general regression model was used for the multivariate analysis. Regression coefficients (beta) and their 95% confidence intervals are given. Statistical significance denotes that the factor is an independent determinant of the severity of depressive symptoms in the particular patient subgroup. The cluster subgroup is not included due to the small number of subjects. NS, Not significant.
Discussion
Depression in headaches and other pain conditions
Pain is often associated with depression: in a neurological out-patient setting the odds of having depression were increased to over two-fold in those with pain (13). Depression in patients with pain is associated with more pain complaints and greater impairment (9). Prospective epidemiological studies suggest a common genetic, biochemical or environmental background behind primary headaches and depression (1, 14). When examining a headache patient, special attention should be paid to the recognition of comorbid depression. Comorbid depression was found to be associated with female gender, higher age, and higher frequency and longer history of headaches (15, 16). Moderate or severe depressive symptoms were reported by 21% of our headache patients and by 18% of those with low back pain, confirming the high prevalence of comorbid depression in patients with pain. It should be emphasized that both the headache and the low back pain patients of the present study are probably more severe sufferers from pain than those who do not seek medical help for their symptoms. Therefore, the conclusions of the study may not be generalized for the total headache and low back pain population.
Differences in depression and disability among headache subtypes
Most studies analysed the relationship between depression and migraine headache (1, 17–19). Patients with tension-type headache were also found to have high depression scores, and the frequency of headaches influenced the coexistence of depression in this patient group (20). Marchesi et al. (21) found no significant difference in the prevalence of migraine and other headache types in patients with depressive syndromes. Venable et al. (22) found that a group with combined headaches scored high on measures of depression, and they experienced more psychological distress than those with tension-type headache. Patients with chronic tension-type headache had higher levels of depression than controls and patients with migraine (23). In a study of migraine and non-migrainous headaches, depression was more dependent on headache frequency than the headache diagnostic category (2). Among our patients, those with chronic tension-type headache scored higher on the Beck scale than migraine patients (Table 2), although the episodic tension-type headache group had a similar score to the total migraine population. Pain frequency was a stronger predictor of depressive symptoms than pain intensity in headache patients in univariate (Table 3) as well as in multivariate testing (Fig. 3).
Recognizing coexisting mood disorder and disability helps to make the best treatment choice for the acute and preventive treatment of headaches. In an analysis of disabling headaches, migraine and major depression had a bidirectional relationship, whereas major depression did not predict a significantly increased incidence of other severe headaches (24). Regarding primary headaches, although most frequently migraine is considered in the context of disability, significant impairments in functioning and well-being were also evident in chronic tension-type headache (8) and episodic tension-tension-type headache (25). Disability in the tension-type headache subgroup in our patient population was more severe than in our migrainous patients (Table 2) due to the high proportion of chronic tension-type headache.
Differences in depression and disability between headache and non-headache pain
Depression was found to be present in 5–85% of patients with different pain conditions (9). The question arises, whether the determinants of depression are the same or different in different headache subtypes and in patients with headache and non-headache pain. Depression was an important disability predictor in chronic pain patients with extended follow-up (26). In a sample of chronic headache patients a significant positive relationship was found between depression and perceived disability (3). In low back pain the rate of major depression increased in a linear fashion with greater pain severity (27). The determinants of the severity of depressive symptoms in headaches and in low back pain differed in our study. Whereas disability and age were the significant predictors of the severity of depressive symptoms in primary headaches (Table 4), these factors were not independent predictors in low back pain after controlling for the other factors. Pain intensity and, to a lesser extent, pain frequency were the most important independent determinants of the severity of depressive symptoms in low back pain. Disability did not have a significant association with self-reported depression in low back pain in the study of Maxwell et al. (28) also. In a study of Marcus (10), pain characteristics, depression and disability differed in patients with headache and non-headache pain. These findings, together with ours, suggest that there might be a different aetiology for depression in primary headaches and non-headache pain syndromes.
The major limitation of our study is the application of a questionnaire, i.e. the data and the conclusions of this survey are based on patient report rather than on objective observation. The two major parts of the questionnaire used in this study, i.e. the Beck Depression Inventory and the MIDAS questionnaire, have been validated in many populations, and were found to be valid indicators of the severity of depressive symptoms as well as of the severity of disability (29, 30). The MIDAS score was found to be valid when compared with a reference diary-based measure of disability (31), and was also valid in an international study (32), and was applied in both migraine and non-migraine headaches (6, 33–35). As the items of the MIDAS questionnaire are not specific to headaches, for the current comparisons we felt it justified to use this measure of disability – quantified as the number of days lost from work, household, and social activities – to score patients with low back pain as well.
As a conclusion of our study, we can state that depression is often associated with pain syndromes, including primary headaches. The severity of depressive symptoms in primary headaches is mainly determined by the disability caused by the headache and to a lesser extent by the age of the patient. The determinants of the severity of depressive symptoms are similar in various primary headaches. In contrast to primary headaches, not the level of disability, but pain intensity and frequency are the most important determinants of the severity of depressive symptoms in low back pain. One possible explanation for this might be that low back pain affects one's life differently from headache pain, and the cause of disability might be different in headache and low back pain patients. The difference in the public perception of disability caused by primary headache and by low back pain might be another factor: disability due to an organic disease, such as spondylarthrosis or herniation of an intervertebral disk, might be socially more acceptable, therefore results in fewer conflicts for the patient. The hypothesis generated by the results of our study, i.e. that the pathomechanism of depressive symptoms is different in primary headaches and in other pain syndromes, should be tested in further studies.
Footnotes
Acknowledgements
The work was partly supported by grant No. ETT 130/2003 from the Ministry of Health, Republic of Hungary.