
Abstract
Jabs (stabs) usually last ≤3 s and are located in the skull area, mostly anteriorly. In many cases, there are only a few jabs during lifetime. With this definition, jabs are frequent, thus at 35.2% in the Vågå study of headache epidemiology. Long-lasting jabs (?), i.e. paroxysms lasting 10-120 s, were present in six out of 1779 parishioners. These pain paroxysms seemed mainly to be side-locked, but could not be provoked. Possibly, these long-lasting jabs after all mainly are regular jabs. To include the ≤2-minute-long paroxysms among the jabs will necessitate a rather drastic change of criteria. This group of jabs may, nevertheless, be heterogeneous. In two parishioners, the paroxysms were associated with a migraine-like pain. The paroxysms occasionally became most intense (2-10 times the basal pain), and then, and only then, were they combined with stark, visual phenomena: wave-like movements ('undulation'), anopsia, but also: immense dizziness, nausea/vomiting. The nature of the side-locked basal pain, although migraine-like, remains unsolved.
Introduction
‘Jabs’ or ‘stabs’ are ultrashort cephalic pain paroxysms. That jabs exist has been known for decades. They occur both in combination with – and independent of – primary headaches. The International Headache Society (IHS) criteria (1) state that what is termed ‘idiopathic stabbing headache’ lasts a ‘fraction of a second’ and is ‘exclusively or predominantly’ located in the distribution area of the first trigeminal branch. Both statements may seem disputable:
Raskin & Schwartz (2) found stabs (‘icepick-like pain’) to be located occipitally in 19% of their cases and Pareja et al. (3) in 12%. In a large-scale population study, we recently (4) demonstrated a location of jabs outside the trigeminal area in 22% of the cases. Purely extratrigeminal icepick pain-status has also been described (5).
In the series by Pareja et al. (3), stabbing pain lasted 1 second in 69% of the cases. In 82% of the cases, the attacks seemed to last ≤ 3 s. In some of their cases, however, attacks lasted up to 10 s, where the line for inclusions was drawn. There is some precedence for accepting even longer-lasting attacks. The International Association for the Study of Pain (IASP) states that although ‘jabs’ usually last 1–2 s, they may occasionally last up to 1 minute (6).
In our study, the majority of attacks seemed to last 1–3 s (7). Since in our cases, jabs duration seems to be in conformity with the stipulation of IASP (6) (and Pareja et al. (3)), we prefer the term ‘jabs’ in this context.
Some parishioners claimed that although their regular attacks lasted 1–3 s, occasional attacks could last up to 5–10 s. These parishioners have been listed as having 1–3 s long attacks, since the majority of their attacks seemed to fall within that group. There were some parishioners, however, who left little doubt that their attacks generally would last > 10 s and even considerably more than that. These relatively long-lasting paroxysms frequently seemed to be associated with migraine/migraine-like attacks. To explore the characteristics – and nature – of attacks lasting > 10 second is the main aim of the present communication. Are such paroxysms really jabs (or stabs) by nature?
The Vågå study: a brief outline
An epidemiological study of headache was carried out in the commune of Vågå in southern Norway, during a 2-year period, 1995–97. Details of the study design have been published previously (8). The total number of parishioners was 3907 just prior to the initiation of the study (7, 8). All 18–65-year-old parishioners were invited to participate in this study. The target group consisted of 2075 parishioners. Of these, 1838 (88.6%) were personally examined by the principal investigator, OS. A total of 1779 (97%) of those examined, were asked about jabs. In the latter group, 627 (35.2%), had had jabs, according to the adopted definition (7). Each parishioner was questioned according to an elaborate questionnaire, in what probably best can be described as a ‘semistructured’ interview: The wording of the questions was stereotyped, and the questions were presented in a stereotyped way; this even included the body language, with which the questions were presented. It was, nevertheless, not infrequently necessary to make some deviations from the main track (8).
Materials and methods
There were 915 females and 864 males in the group asked about jabs, with a female/male ratio of 1.06, which entirely corresponds to the gender ratio (1.05) in the target group (7). The present subgroup consisted of parishioners who stated that they regularly had long-lasting, cephalic paroxysms, in this context defined as paroxysms regularly lasting ≥ 10 s, but probably lasting no longer than 120 s. It should be emphasized that none of them have been observed during paroxysms. The data herein are mostly based on retrospective information. However, some of them have been followed for a considerable period (up to 6–7 years) because of the intricate nature of the paroxysms (nos. 1 & 4).
The IHS diagnostic criteria for headaches (1) have generally been adhered to. A partial, neurological examination was carried out routinely, including cranial nerves and facial/cephalic/nuchal structures (8). Cases 1 and 4 underwent a complete neurological examination. If indicated, supplementary examinations, like cerebral CT or MRI would be carried out.
Results
Characteristics of paroxysms, lasting ≥10–120 s
Such paroxysms were not included among the regular jabs (4, 7), since they from a temporal point of view fell outside the group. A total of 6 cases seemed to fall into the ≥10–120 second-long category, 3 females and 3 males, in other words, a prevalence of 0.34%(Tables 1–3). The mean age of onset was approximately 23 years (Table 1) (mean age of onset for jabs in general: approximately 28 years (7)). All the paroxysms were cephalic, since this was an inclusion criterion. Most frequently, the paroxysms seemed to be localized; in the one parishioner with occipital localization of the paroxysms, no definite laterality was reported (Table 1). The intensity mostly seemed to be ‘severe’; in two cases (nos. 1 & 4), it was excruciating.
Long-lasting paroxysms (‘jabs’?). Demographic data and some clinical characteristics
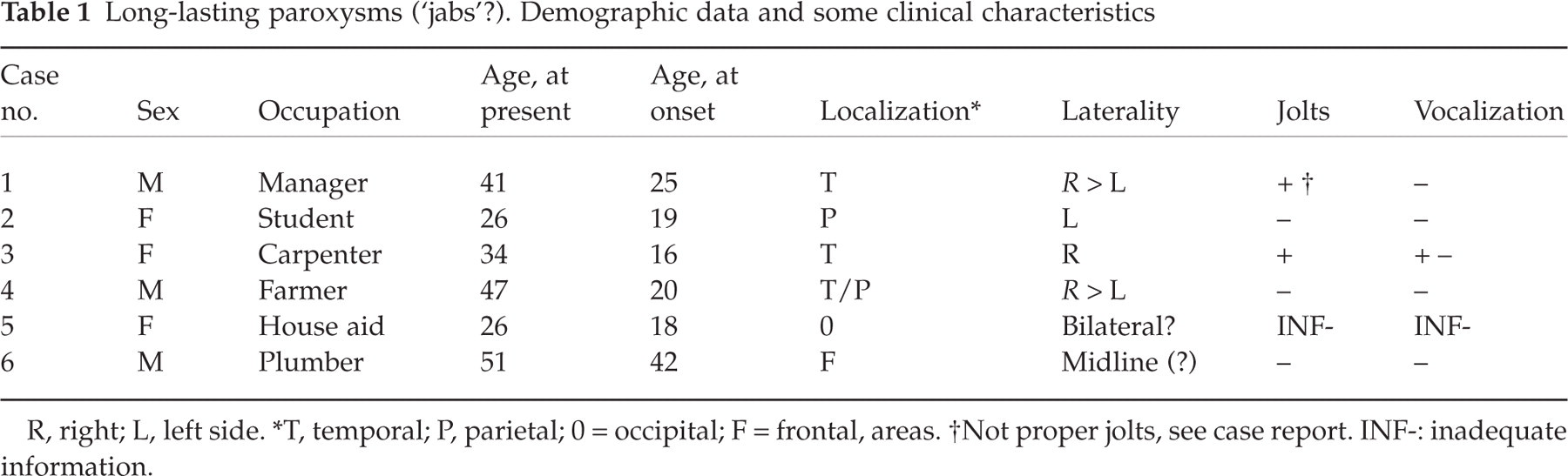
R, right; L, left side.
T, temporal; P, parietal; 0 = occipital; F = frontal, areas.
Not proper jolts, see case report. INF-: inadequate information.
It is noteworthy that although paroxysms might last up to approximately two minutes, in all except one (no. 5, Table 2), they might also be of only 10–15 s duration; in case 1, possibly the paroxysms could last even shorter time, occasionally. In three cases, the attacks at times seemed to exceed one minute. Based on the lowest value of duration in case 2 and on putative, individual means in the other ones, the average duration would seem to be around 3/4 minute (Table 2). One will, accordingly, get some problems with the categorization of at least some of these cases when considering the temporal boundaries for stabbing pain, according to IHS (1).
Long-lasting paroxysms. Temporal pattern
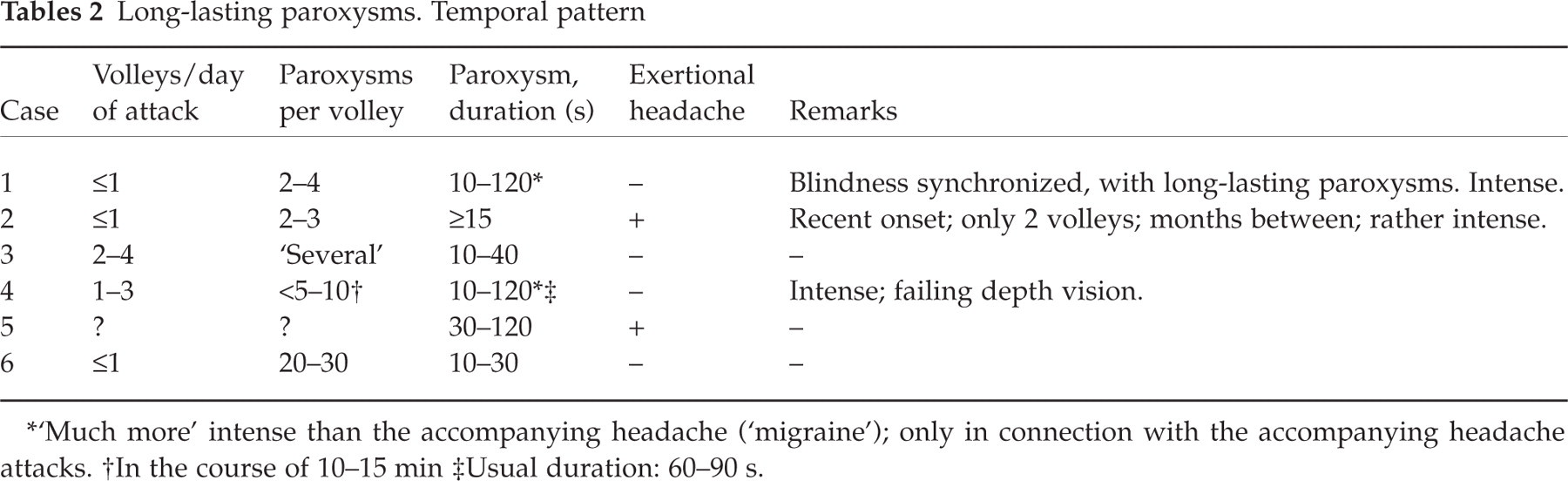
‘Much more’ intense than the accompanying headache (‘migraine’); only in connection with the accompanying headache attacks.
In the course of 10–15 min
Usual duration: 60–90 s.
Volleys were not infrequently present (Table 2). Jolts (n = 1, see Table 1) and vocalization (n = 1, and only occasionally) seemed to occur with approximately the same frequency as in jabs in general (4). The one with occasional vocalization had intense paroxysms. There were clear indications that, in some of them, the jabs were more severe than jabs in general (in particular nos. 1, 3, and 4; see also case histories). There were no clearly recognizable, localized, autonomic phenomena in any one of them, and no trigger zones had been noted. In particular, there was no increased supraorbital tenderness in any of these cases. Two parishioners – but none of the most severely afflicted ones – had additional exertional headache, a condition that also has been claimed to be partially indomethacin-sensitive (Table 2). There seemed to be a clinical involvement of the neck in two of the three worst cases (Table 3).
Long-lasting paroxysms. Accessory headaches
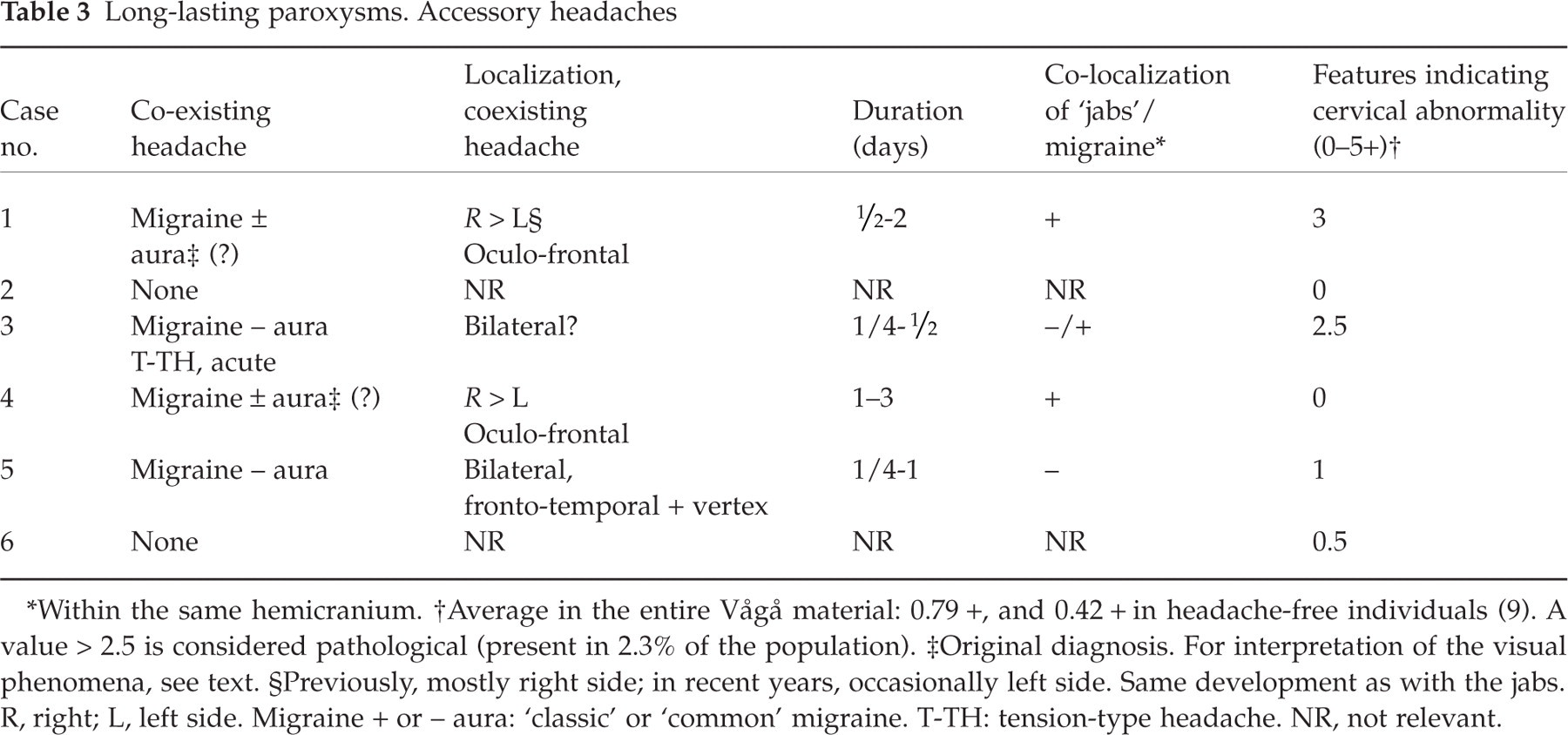
Within the same hemicranium.
Average in the entire Vågå material: 0.79 +, and 0.42 + in headache-free individuals (9). A value > 2.5 is considered pathological (present in 2.3% of the population).
Original diagnosis. For interpretation of the visual phenomena, see text.
Previously, mostly right side; in recent years, occasionally left side. Same development as with the jabs. R, right; L, left side. Migraine + or – aura: ‘classic’ or ‘common’ migraine. T-TH: tension-type headache. NR, not relevant.
It is striking that four of the six parishioners were migraineurs, or at least at some stage had been diagnosed as such (Table 3). The ‘classic’ (+ aura) and ‘common’ (– aura) varieties of migraine had been considered to coexist in two of these parishioners (for details, see case histories). This group of six does not seem to be homogeneous: There were two parishioners who exhibited particular traits; these two case histories will be detailed.
Case reports
Case 1
A 41-year-old male (Tables 1–3) had had a headache from the age of 8, with 2–8 attacks per month, each generally of ½−2 days’ duration. Childhood attacks usually started during school hours. Occasionally, he could stay in bed for a whole day. However, on rare occasions, attacks lasted no more than half an hour. These attacks have become milder after puberty. The headache fulfilled the IHS migraine criteria: It was characterized by photo- and phono-phobia (invariably present); nausea; vomiting (occasionally present, depending upon the intensity of pain and nausea); and an intensity up to severe; throbbing headache. He frequently wears sunglasses. The headache had been rightsided in younger days, but occasionally had a leftsided localization in recent years. In addition, there was aggravation of headache upon minor movements of the head. He was quite well inbetween attacks.
There had never been ‘zig-zag’ visual phenomena; as a kid, he experienced photopsias and dark spots in the visual fields, but asynchronously with the headache attacks.
At the age of approximately 25, headache attacks of another type were added: long-lasting, jabs-like paroxysms (10–120 s duration). At the peak of the pain curve of a migraine-like attack, never in front of it, the following could occur: He would, absolutely abruptly and unannounced, get a particularly long-lasting and vehement paroxysm, approximately twice–thrice as strong as the basal headache (probably ‘as strong as dental pain’). The paroxysms would occur repetitively for 10–20 min, but the symptomatology would be less ‘rich’ with reiterative jabs in a volley (Fig. 1). During attack, he experienced complete anopsia, everything being ‘dark’/‘black’, and he was absolutely incapable of discerning any contours. He could also get ‘wave-like phenomena’ in the visual fields, like ‘northern light, but without colour’, and also dizziness and nausea; he felt unconcentrated and felt as though the whole body was rocking. The feeling of undulation may have diminished slightly since the first examination (7 years ago): possibly, the present descriptions lack some of the vividness of the first descriptions. These waves did roll rather than proceed slowly, in this way differing from the crescent of scintillating scotoma. Due to the intensity of the pain, he would also squeeze his eyes (which was the reason why he originally mentioned ‘jolts’, see Table 1). When the short-lasting pain disappeared in the course of ≤ 2 min, vision would reappear and the wave-like phenomena stop, suddenly and completely. There seemed to be an unwavering temporal connection between jabs-like and visual phenomena. Numerous consultations/contacts have fortified the impression that the visual phenomena started absolutely synchronously with the severe pain, and they also ended simultaneously. The visual phenomena had the characteristics of an ‘on-off phenomenon’. However, most attacks of the basal headache (‘migraine’) appeared without pain paroxysms/visual phenomena. The paroxysmal pain seemingly was most marked in the right temporal area in earlier years; more recently, it seemingly was occasionally on the left side, in correspondence with the development as regards the migraine-like headache (Tables 1 and 3), The two headaches were, nevertheless, not quite colocalized (Tables 1 and 3). The paroxysmal pain seemed to be ‘deep in the head’; he could not ‘touch’ it when he rubbed his temples, and this pain was absolutely immobile/stationary.

Patient 1. ‘Long-lasting jabs’. Schematic drawing. These attacks appear at the peak of the pain curve of a migraine-like attack. The relative intensity seems to diminish markedly with sequential attacks in a given volley; with decreasing intensity, the symptomatology becomes less ‘rich’.
As regards the family history, the eldest of three daughters, 10-years-old, had episodes of headache with nausea and occasional vomiting. Otherwise, the family history was negative. Neurological examination was negative. ‘Cervical features’ was 3.0 + (9). A MRI scan of the brain could not be obtained for technical reasons.
Case 4 (40-year-old farmer)
The ‘basal’ headache
From around 10, there had been 1–3-day-long, frequent (one or more times/week), and relatively severe headache attacks, the worst attacks occurring during late winter and spring/autumn –‘when the sun was low’. The intensity and duration of attacks have increased with age. He had a clear feeling that he was oversensitive to strong light and that this excessive sensitivity not only aggravated already existing headache, but that it even could provoke attacks. He constantly wore sunglasses on sunny days. Occasionally, though, he woke up with a pulsating headache. He was also oversensitive to high-pitched sounds and mentioned particularly classic music; he never attended concerts. He had to use an ear protector during farm work.
The basal headache contained all the 9 migraine criteria of the IHS (1.1. Migraine without aura; B–D). It was fronto-ocular and unilateral in location, in earlier years almost only on the right side; more recently, more than just occasionally the headache would be on the left side. Ergotamine at an oral dosage of 1.5 mg apparently modified the attacks in earlier years, but at one time he developed a more chronic headache, probably due to ergotamine overuse; ergotamine was discontinued and the original attack pattern was re-established. After re-start of this therapy, it still seemed to keep the headache at bay. But in periods, there was medication on a close-to-daily basis, with an annual consumption of approximately 300 mg of ergotamine; the headache again became chronic/fluctuating over prolonged periods.
The prolonged paroxysms
From the age of 20, the following could happen in connection with a crescendo or maximal basal pain: He suddenly got extremely severe paroxysms, each of them lasting up to 2 min (Fig. 2, pattern VI). If exposed, the depth vision proved to be failing in such periods. As an example: he would not be able to sort out the near/far end of a stick of some length, pointing towards him; he would feel that the stick was coming onto him, penetrating his sick-side eye. This would create dizziness, enormous nausea, and even, on rare occasions, profuse vomiting. A pulsating quality would then be added to the headache. The photophobia was excessive during attack, for which reason he squeezed his eyes. There were no visual disturbances antedating the basal headache attack as such.

Patterns of relatively short-lasting unilateral headaches. With focus on duration. Schematic drawing.
The prolonged paroxysms were located ‘deep in the head’, but appeared to have ‘a link to the pain side of the basal headache’: in other words, mostly the right side. After having become established, the pain remained stable at this level for the remaining part of the paroxysm. He claimed that such jabs were from 2 to 3 times up to 10 times as intense as the basal headache – and took all his attention (Table 4); if driving a car, he was forced to drive to the side and take a rest. There was invariably a close temporal connection between the pain paroxysms and the visual disturbances, the pain paroxysms possibly appearing just a second or so prior to the visual disturbances. The visual disturbances occurred under no other circumstances, but they did not materialize in connection with every paroxysm (Fig. 2, pattern VI). This complex of events appeared during the most severe attacks of the basal headache or in the presence of exacerbations when the headache was chronic/fluctuating. The paroxysms occurred in volleys (Table 2), each volley usually consisting of duplets, triplets or quadruplets (but there might have been up to 5–10 in a row, the later ones in a series then clearly inferior in severity), see Fig. 2, pattern VI. They usually occurred in the course of 10–15 min. The worst paroxysms occurred approximately twice a month; more low-degree paroxysms occurred in approximately 50% of basal pain exacerbations.
Combination of ‘jabs-like’ paroxysms and migraine-like headache. Characteristic traits

Preponderance of the male sex (?); may be only apparent.
Ergotamine: effect in one of two patients.
As regards the family history, the father may have had a ‘similar headache’, and the maternal grandmother may have had migraine. MRI of the brain with angiographic studies was normal.
Comments, cases 1 & 4
Is the basal headache in these two cases compatible with migraine? Maybe it is. At least, the IHS migraine criteria were clearly fulfilled. The apparent ergotamine effect in case 4 may at face value count in the same direction.
There are, nevertheless, various features that count against a migraine diagnosis, as regards the basal headache: Ergotamine was used in too high dosages (due to only partial effect??). Moreover, ergotamine efficiency is not specific to migraine; ergotamine may be effective in any headache with a ‘vascular’ component, e.g. cluster headache. Being ‘migraine-like’ does not prove that the picture is identical to migraine. To a certain degree, the male sex, the occurrence during fall/spring (particularly in case 4); the partly fixed laterality count against migraine in these cases.
When seen in context with the visual phenomena, the problem becomes even more complex. The onset – and discontinuation – of the visual phenomena was abrupt, sort of an ‘on-off phenomenon’ (Table 4). And the close temporal association between the pain paroxysms and the extraordinary, visual disturbances/nausea/vomiting are not fully compatible with ordinary migraine either. Although many features are common to our two cases (Table 4), the picture does not seem to be quite homogeneous. Whether these discrepancies are marked enough to distinguish between them is more doubtful.
The clinical neurological examination (n = 2 and 3, in cases 1 and 4, respectively) did not reveal significant pathological findings. The diagnosis in case 4 has been felt to be so indistinct that cerebral CT and MRI, and EEG have been carried out: all with negative result. The follow-up time for these two parishioners was 7 and 6 years, respectively, with multiple interviews in each. The case histories seem to be concise and rather consistent over this period.
Discussion
The duration of cephalic jabs
The IHS definition (1) states, without reservation, that stabs last ‘a fraction of a second’. Some authors have, accordingly, felt that stabs lasting up to 10–20 s are atypical (10). Pareja and coworkers (3), in their hospital-based series, found that in 5% of the cases, paroxysms might last around 10 s. The IASP classification (6) accepts jabs of more than just a couple seconds’ duration. The parishioners described in the present communication (Tables 1 and 2), all seemed to have experienced pain paroxysms, exceeding just a few seconds’ duration (Fig. 2, pattern II).
The ultrashort, cephalic paroxysms described as ‘jabs and jolts’ syndrome in 1979–80 (11, 12) rather clearly were core cases of stabbing pain, with ‘multidirectional, knife-like head pains’ (12). These could be separated from and were – clearly – unrelated to regular paroxysms of chronic paroxysmal hemicrania (CPH), from a locational as well as from a temporal point of view.
However, in addition to these brief paroxysms, a more long-lasting variety(lasting up to 20–25 s, and later observed to last up to approximately 1 minute) was also described at that time(11,12, see Fig. 2, pattern III), primarily as a constituent of the pain panorama of CPH. There was a marked ability to precipitate attacks mechanically (11), also when the patient was in a relatively good, but far from optimal, shape, e.g. after a ‘drug holiday’ (discontinuation of indomethacin) of a day or two's duration (13). The absolute indomethacin response, the mechanical precipitation of the paroxysms, and the side-locked unilaterality (11, 14), all are properties at variance with the regular characteristics of the ‘jabs and jolts’ syndrome proper (Table 5). Also Lance (15) suggests that these attacks in nature entirely differ from ordinary jabs. The most correct characterization of these attacks is probably that they are abortive attacks of CPH. These early observations should, in other words, not confound the temporal definition of jabs as such.
A comparison between ‘regular’ jabs, longlasting jabs, and paroxysms associated with CPH∗)
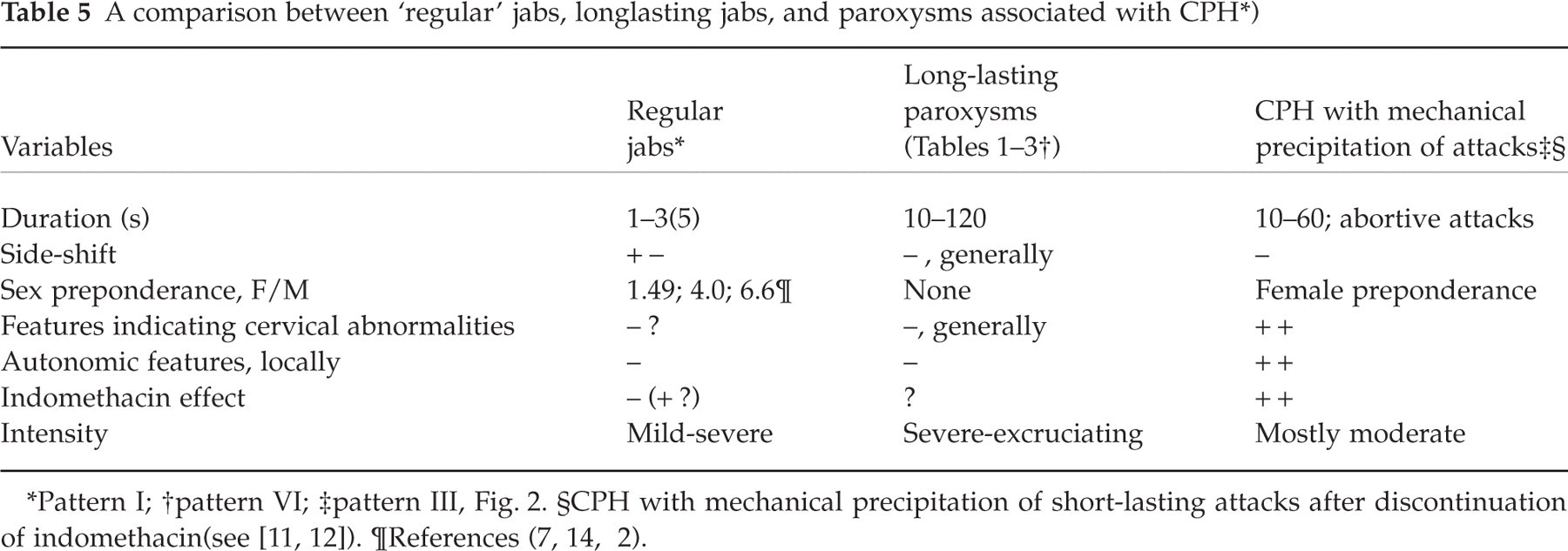
Pattern I;
pattern VI;
pattern III, Fig. 2.
Inclusion of paroxysms of the length presented in the present communication into the 4.1 category of the IHS classification should not create an overwhelming problem, numerically speaking. It would, however, necessitate a rather drastic conceptual change as far as temporal aspects are concerned. The nature of some of these paroxysms should be explored further before flatly accepting them as jabs, as will be elaborated upon in the forthcoming. A number of short-lasting (i.e. of ≤ 2 min duration) cephalic paroxysms, e.g. SUNCT syndrome (16, 17) can now be distinguished, as schematically depicted in Fig. 2.
On the nature of the relatively long-lasting paroxysms
Intensity evaluation is difficult in jabs in general, due to the briefness of the pain. However, several parishioners indicated that if the pain of ‘regular jabs’ had been more long-lasting, social and occupational functioning could have been jeopardized (4). Jabs may thus probably in the occasional case lead to considerable pain. The jabs-like phenomena in the two present cases markedly differ from regular jabs in various respects: an intensity out of proportion to that in ordinary jabs, temporal and locational link to attacks of a migraine-like headache, with massive, strange visual symptoms and possible male preponderance (Tables 4 and 5), in addition to the duration. This temporal link was so rigid and occurred over so long time that a by–chance association seems highly unlikely. Are these deviating features sufficiently ponderous to bring these jabs-like phenomena into a separate category? The nature of the basal headache seems to be somewhat unclear, in spite of clear migrainous traits.
Own observations on the temporal associations of jabs-like phenomena and migraine ± aura-like headache
A high prevalence of ordinary duration jabs, i.e. of 1–3 s duration, has previously been demonstrated in migraine (2, 3). In such cases, the jabs as frequently seemed to occur outside the headache phase as they concurred with the headache (3).
We recently reported (4) that regular-duration jabs might be followed by migraine attacks, partly regular with aura attacks (n = 2), and partly vague attacks with inherent episodes of dimmed vision (n = 1). A similar link to migraine without aura was also observed (n = 3). Even ‘facial jabs’ (18) seemed to herald migraine without aura attacks in one solitary case. Because of the frequency with which also this combination of phenomena occurred intra-individually, this probably represented something more than just a random association of the two brands of pain.
Observations by other observers
A similar sequence of events as in our cases has also been observed by others (2, 10): Thus, in Dangond & Spiering's experience (10): ‘These stabbing pains lasted ‘about 10 seconds’ and occurred every minute. With the most severe pains, the patient experienced nausea, blurring of vision in both eyes and occasional vomiting. The headaches were so intense …’ (26-year-old female (Fig. 2, pattern IV)). In Raskin & Schwartz's experience (2): ‘For seven patients, icepick-like pain heralded the onset of a migrainous episode. In a few patients, scintillating scotomas … had occurred on several occasions in association with jabbing pain’ (underlining made by the present authors).
The relationship between such visual phenomena and migraine
We now arrive at a somewhat disturbing point in our deliberations: The extraordinarily strong visual disturbances (‘northern light’ phenomena/transitory blindness/autokinesis) do not unambiguously point in the direction of a ‘migrainous’ headache. The fact that the visual phenomena in our cases occur at the pain maximum may still be consistent with a migraine diagnosis: Many investigators state just that there may be such a reversed sequence of events (19–23). They immediately go on to asserting that usually the visual phenomena appear in front of it (e.g. 19, 20). However, according to Klee (24), visual disturbances in ‘severe migraine’, for a great part bizarre ones, appear more than twice as frequently during as prior to the pain phase of the attack.
Klee's cases were described a long time prior to the IHS migraine criteria. Details of his cases are, nevertheless, recorded. It is obvious that the ‘autonomic part’ of the migraine criteria (nausea, etc.) is present to a great extent in his patients. Also the ‘pain part’ of the criteria seems to be present to an adequate extent, his cases thus exhibiting ‘severe’ headache. ‘Walking and other necessary movements’ would make the pain more intense. The ‘lowest’ figure for a migraine feature mentioned seems to be for unilaterality (64%); unilaterality is, however, an altogether nonobligatory feature in the IHS system. There is thus little doubt that Klee's patients, grossly, would have fulfilled the IHS migraine criteria. Klee's work therefore represents strong evidence that in migraine (‘severe migraine’), visual disturbances frequently occur during the pain phase.
Interestingly, Klee may also have observed ‘jabs’/′stabs’ already in 1968 (described as ‘darts of pain’). These ‘darts’ appeared at the pain maximum during ‘severe’ migraine attacks, and the ‘darts’ were apparently stronger than the ‘severe migraine’ (24). They usually lasted less than 30 s. These features suit with those observed for the paroxysms in the present cases.
Visual disturbances in migraine have been dealt with carefully by, e.g. Klee & Willanger (24, 25) and Alvarez (26). Many observers state that while positive visual disturbances are the rule in the typical cases of migraine with aura, negative phenomena may also occur in connection with migraine (or migraine-like) attacks. Such negative phenomena include dimness of vision, obscuration, and transitory, global anopsia (19, 21, 24–29). In addition, both macropsia and micropsia (22–24), disturbances as regards judgement of distances, movement of stationery objects (‘autokinesis’) (22–25, 30), and ‘wave-like’ metamorphopsia (24) have been described. ‘Total anopsia’ occurred in 6% of Klee's patients; always during the attack (n = 50) (24). Hachinski et al. (29) state that negative visual phenomena: ‘Transient blindness, blurring of vision, and varied scotomas were most common’ during attacks (in 77 out of 100 children with visual disturbances). Klee defined the difference between anopsia and obscuration in this way (24): Obscuration meant that contours could be discerned vaguely at times. Anopsia meant: no vision at all, in part of or in the entire visual field. The anopsia episodes in Klee's cases were ‘short’ or lasted ‘for minutes’. In one patient examined during an ongoing spell, the blindness seemed to be of cortical nature, since the menace reflex was lacking, while the light reflex persisted.
Global anopsia is also a feature of basilar migraine, code 1.2.4, IHS (1). Attacks of basilar migraine (31, 32) are, however, long-lasting and are usually accompanied by massive symptoms and signs of brain stem affection, features that do not quite fit with the presently reported attacks.
The two components of the presently presented constellation, the jabs-like phenomena (‘darts’) and the unusual visual disturbances, i.e. anopsia, autokinesis, and undulation, and even their respective duration, have, in other words, also been described by Klee (24, 25) and in connection with the pain phase of migraine. In our opinion, it is an achievement to have found these separate elements at that early stage, i.e. in 1968. The invariable and strict concurrence of these two components, the jabs and the visual phenomena, temporally speaking, does, however, not seem to have been described by Klee; nor that the jabs were reiterative on the pain side, with loss of vigor as the volley proceeded (Figs 1 and 2). The anopsia episodes described in the present communication, and probably also those described by Klee (24), do not without reservation fall under the IHS definition of migraine with aura:
According to the IHS (1), fortification spectra (scintillating scotoma) of migraine with aura last > 4 min; visual phenomena that last a minute or two – like in our cases – should accordingly not be migrainous in nature. In case 1, there was undulation in the visual field and no slowly progressive crescent, like in migraine. One may, however, suspect that vague, uncharacteristic visual phenomena at the pain maximum of migraine attacks may not have been paid due heed to in all contexts and for that reason, our insight in these matters may be limited.
In a previous study of four cases of headache and global blindness, the blindness was invariably substituted by either attack-related, monocular visual loss or homonymous fortification spectra after a period of up to 10 years, or: the attacks stopped altogether (27). Such attacks of anopsia therefore seemed to be transformed to ‘migrainous’ attacks or attacks of ‘retinal migraine’. In the present cases, however, the visual phenomena continued in principle more or less unaltered after approximately 17 and 27 years, respectively. Neither in this respect, did the episodes resemble migraine proper. The previously observed blindness episodes (27) were, admittedly, of longer duration than the shortlasting ones in the present context. Moreover, both case series are limited in number.
Scintillating scotomas seem to be so typical of classic migraine that they almost are diagnostic. The following question therefore becomes central: other visual phenomena, like obscuration and anopsia, are they also necessarily ‘migrainous’; are they diagnostic? The present authors reason this way: if, such as in our previously observed patients (27), sooner or later these visual symptoms are replaced by typical, scintillating scotoma, the migrainous nature even of such visual phenomena is, at least to some extent, certified. Stereotyped, short-lasting, global anopsia episodes and other ‘drastic’ visual symptoms, such as in case 2, over more than a decade, may phenomenologically seem to be in an entirely different category than the anopsia disturbances observed in migraine. Whether this indicates that they differ aetiologically is another matter.
Although the basal pain in both our cases fulfills the IHS migraine criteria (1), there are many exceptions to a homogeneity of the picture. The gross differences between the jabs and visual disturbances seen in the present cases and in migraine are summarized in Table 6.
Similarities and differences between migraine (‘with aura’) and the present two cases

Ref (15).
According to Pareja et al. (3).
In approximately 50% of the cases, jabs occur frequently during attacks; in the remainder, they seem to occur between attacks (3).
Those who belong to this category, as a rule also – sooner or later – seem to develop attacks with typical fortification spectras or ‘retinal migraine’ (27).
Conclusion
Without committing ourselves, we are inclined to believe that in solitary cases, duration of jabs can be considerably extended, without violating the link to the jabs proper, like in four of our six cases (Tables 1–3). There is, however, clearly room for skepticism in this respect.
The other information herein that to some extent may seem to disrupt the traditional way of thinking is the description of strict and invariable concurrence of jabs-like and migraine-like phenomena. These jabs can, conceivably, be of another nature than other long-lasting jabs.
The problem of the interrelationship between the jabs (stabs) and migraine/migraine-like headache may be a threefold one:
Jabs (Fig. 2, pattern I), that may appear inside (2, 3) or outside (33) attacks of migraine. They occur haphazardly and apparently have a mean duration of 1.4 s (33). We have little or no reason to suspect that they differ from jabs in general. Such jabs hardly have any impact on the solitary basal headache attack or the long-term development.
The jabs (stabs) described by us (4) and by other workers in the field (2, 10) that appear in front of migraine attacks may, in theory, be in an essentially different category. These jabs (Fig. 2, pattern IV) are of ‘regular’ duration – or can be ‘prolonged’. However, the very fact that they appear in front of pain attacks may be consistent with the view that they ‘spark’ or ‘ignite’ the attack, that even may be characterized by scintillating scotomas (4, 10). Or: if the visual phenomena are part of the attack, they could be inherent qualities of the initial phase of attack (cf. migraine + aura). The latter alternative may seem less likely.
With regard to the relatively long-lasting pain paroxysms, as described by Klee (24) and herein, the situation may seem to differ essentially: The pain attack had lasted for some time and was in a crescendo phase or had even reached the point of culmination, when the atypical jabs set in. Accordingly, the jabs/visual disturbances are likely to be a not insignificant part of these ‘severe’ attacks, since the temporal association is so distinct and persistent. That being said, the jabs-like phenomena/visual disturbances ‘complex’ is unlikely to have any ‘ignition’ function for the basal headache, since the attack is under way. This complex to some extent changes the characteristics of the attack, and the victims describe this as their real complaint, i.e. what they are afraid of.
The basal headache, although being ‘migraine-like’ may be a migraine variant, or it may be entirely different from migraine. Would all migraineurs experience this ‘complex’ provided the pain was intense enough? Hardly. In our case no. 3 (Tables 1–3) and in many other migraine patients of ours, the pain has been considerable without any such symptoms.
Not at any time during the protracted period of suffering have these visual phenomena been transformed into positive visual phenomena, typical of migraine. The characteristics of this constellation of symptoms have been set forth in Tables 4 and 5. Some of these traits, e.g. a male preponderance, may be only apparent, but at this stage – and on the basis of only two cases – it is hard to distinguish between essential and nonessential matters.
The jabs-like and the migraine-like symptoms are likely to be manifestation of the same pathological process that, accordingly, seems more likely to be at variance with ordinary migraine than not.
Footnotes
Acknowledgements
We are indebted to GlaxoSmithKline of Norway, Pharmacia & Upjohn, and the Alf Harborg Foundation, Department of Neurology, St. Olavs. Hospital, Trondheim, for generous support during the various phases of the investigation. The authors are also grateful to the personnel at the Vågå Health Centre at Vågåmo for their aid. Last, but not least, we thank the inhabitants of the Vågå commune for their collaboration.