
Abstract
In a large-scale study of headache epidemiology in Vågå, Norway, 1838 adult parishioners(18–65 years of age) were examined, and this represents 88.6% of the target group. Jabs and jolts syndrome/idiopathic stabbing headache (ISH) was verified in 35.2% of the questioned parishioners. This prevalence is much higher than previously observed ones. There were clearly more females than males, the female/male ratio being 1.49, as compared to a ratio of 1.06 in the study cohort (P-value: < 0.0001, χ2 test). The ratio, 1.49, also differs clearly from a previously observed one: 6.6 (P-value = 0.0003, Fisher's exact test). Control studies included blinded re-check of 100 work-ups, with complete concurrence (kappa-value of 1.00 and blinded re-check of 41 individuals (kapp value of 0.841). Jabs and jolts/ISH are frequent and almost the sole shortlasting (generally < 3 s duration) cephalic paroxysms.
Introduction
That ultrashort head pain paroxysms exist has been known for decades. In two population studies, where prevalence of such paroxysms has been estimated, idiopathic stabbing headache has been found to be rare, i.e. at the level of < 1–2% (1, 2).
Since such paroxysms are known to coexist with other headaches (3–6), it may be hard to estimate the real prevalence: The associated, major headache will naturally receive the almost undivided attention, not only in studies based on data collection through questionnaires (where this danger is overwhelming), but also in studies based on the clinical interview.
The present report is part of the Vågå study (7), a large-scale epidemiological study of headache in a parish in the mountainous heartland of Norway. To estimate the prevalence of such paroxysms in this circumscribed geographical area is the principal aim of the present communication. Tests of the reliability of the data collection techniques employed will also be reported.
There are two major categorization/classification schemes in the headache field, i.e. the International Headache Society (IHS) classification (8) and the International Association for the Study of Pain (IASP) classification (9), the latter comprising the total array of human pain disorders. IHS uses the term ‘idiopathic stabbing pain’ (ISH) and IASP the term ‘jabs and jolts syndrome’ (jabs) for these ultrashort paroxysms. Several other appellations have also been used, such as ‘ice-pick pain’ (6). Lansche (10) may have given the first description of this form of headache in 1964, and he termed it ‘ophthalmodynia periodica’. There actually seems to be little doubt that all these terms refer to the same ‘core’ condition. The terms could thus probably be used interchangeably. There are, nevertheless, some variations in the descriptions. In the fringes of this disorder there may – putatively – be variants, with regard to duration and localization, or even with regard to these two qualities combined.
The ‘regular’ jabs, the topic of the present communication, will in the forthcoming be referred to as ‘ISH’ (or ‘stabbing pain’) or ‘jabs’.
Materials and methods
The design of the Vågå study has previously been described in greater detail (7). A short-version description is given in this context:
The total population of Vågå was 3907 individuals, just prior to the start of the study in 1995 (Table 1). Of these, 2075 were in the target group, i.e. 18–65 years of age and accessible for study (for details, see 7). A total of 1838 individuals(88.6%) went through the program. Of these, 942 were females, and 896 males. The examination program consisted of the filling in a questionnaire as part of a semistructured interview and, finally, of a neurological/physical examination. The clinical part, inclusive of the filling in of the questionnaire, was entirely in the hands of the principal investigator (O.S.) to avoid inter-examiner bias. In other words, the extensive questionnaire was not even seen by the parishioner.
Study population, parish of Vågå

Drop-out being mainly due to lack of opportunity/motivation.
88.6% of the accessible ones.
The parishioners were questioned as to occurrence of ‘piercing/boring head pains’ of short duration, with the corresponding words in either ‘nynorsk’ (‘new Norwegian’) or ‘bokmål’ (the other official Norwegian language) according to their daily usage: (‘stikkende, borende smerter’). They were then presented with the synonymous local dialect words: ‘flogg’, ‘skjæring’, ‘riv(n)ing’, all of which seem to have more or less analogous meaning.
In the present context, cases of ‘definite jabs’ were taken into consideration, as well as a few cases in the ‘probable jabs’ category (actually n = 5) where such paroxysms were felt most likely to be present. ‘Possible’ cases were thus discarded. Cases of typical jabs associated with a more ‘neuralgiform’ cephalic pain condition – the nature of which was dubious – were included. This situation in our estimation is analogous to the one of the migraine/IHS combination. While the jabs as such will be dealt with presently, the association of this (neuralgiform?) condition and the jabs will be dealt with elsewhere. This combination was, however, found only in a few cases.
The total examination time was generally around 60 min, but could occasionally last considerably longer. The subsection of the questionnaire concerning jabs consisted of 25 items.
Not all parishioners were asked about ISH/jabs (Table 1). This omission for various reasons concerns a total of 59 individuals: When the headache history was complex with several headache forms present, one would occasionally refrain from asking about jabs at all. Occasionally, one would for similar reasons refrain from further penetration into the matter. Therefore, satisfactory information could not be obtained in 100% of the cases, for all variables.
An elaborate examination of head and neck and cranial nerves was routinely included, as detailed elsewhere (7). A full neurological examination was carried out if the total situation (the other headaches present) or special features made this advisable (7).
A special problem concerns the duration of jabs. The IHS (8) defines ISH as lasting ‘a fraction of a second’. The IASP (9) definition is more liberal and states that jabs may last 1–2 second, but adds: ‘occasionally last up to 1 minute’ (9). Pareja et al. (11) demonstrated that if the upper border was set at 1 second, only 69% of the cases would be included. A higher sensitivity would be achieved with a border of 3 s, which would include 82% of the individuals. This observation made us choose 3 s routinely as the upper border.
Further conditions for being eligible for inclusion were: the pain must be above a line between the nasion and the tendine insertions in occipital area of the skull. Furthermore, at least ‘a couple’ paroxysms must have appeared during lifetime.
Results
There were 1779 parishioners asked about jabs (Table 1) and of those, 915 were women and 864 men (Table 2). The sex ratio among the questioned parishioners was the same as in the total cohort (Table 2).
Female/male ratios

P-value 3 vs. 2: < 0.0001, χ2 test. P-value 3 vs. 4: = 0.0003, Fisher's exact test.
Prevalence of jabs
A total of 627 of 1779 parishioners indicated that they at some time had had jabs, i.e. 35.2% (CI 32.4–37.5) of those who were asked about jabs. When performing a study on first-come/first-served basis as in the first part of the present study, jabs cases seem to be particularly well represented during the early part of the study (Fig. 1). In this respect, they seem to show the same trend as patients with severe headache, like migraine (unpublished results).

Percentage of parishioners with jabs as a function of the progression of inclusions. No. 100 along the abscissa = parishioners nos. 1–100, etc. Mean frequency of jabs among parishioners nos. 1–300: 42%; 1600–1800: 28%.
Sex ratio
Among those asked about jabs, there were 375 females with jabs; in other words 21.0% of individuals among the 1779 questioned ones were females with jabs. The corresponding figures for males were: 252 males and 14.2% (total = 35.2% percent jabs). Of those with jabs (n = 627), 59.8% were females, as against 40.2% males.
The female to male ratio was 1.49. The female/male ratio in this series was, accordingly, clearly higher than in both the total cohort and in those questioned about jabs (Table 2) (P < 0.0001, chi square test). Among the females questioned (n = 915), 41.0% (CI 37.8–44.2) had jabs, the corresponding figure for males (n = 864) being 29.2% (CI 26.2–32.2). Interestingly, not only the frequency of jabs (Fig. 1), but also the female dominance of jabs was most marked in the early phase of the study (Fig. 2). In the ultimate stages of the investigation, the sex ratio was around 1.0 (Fig. 2).

Sex ratio (females:males) of jabs as a function of the progression of inclusions. Mean sex ratio (whole series): ∼ 1.49.
Age of onset
In 142 cases, no reliable information as regards age of onset was obtained. In 127 cases, only coarse information was obtained, like ‘school-age’, ‘teens’, and ‘grown-up age’ (Fig. 3). Jabs more often seemed to start in the grown-up age than prior to 20 (ratio 96:31 = 3.1).

Age of onset in those parishioners (n = 127) who only were able to indicate roughly when the paroxysms had started. They were only able to indicate a special period of life, e.g. grown-up; age ≥20 years.
In the remaining cases (n = 358), a fairly exact time of onset was given, see Fig. 4. The mean age was: ∼28 years. The ratio grown-up age: age prior to 20 was 4.2. Also this then shows the preferential onset in adulthood.
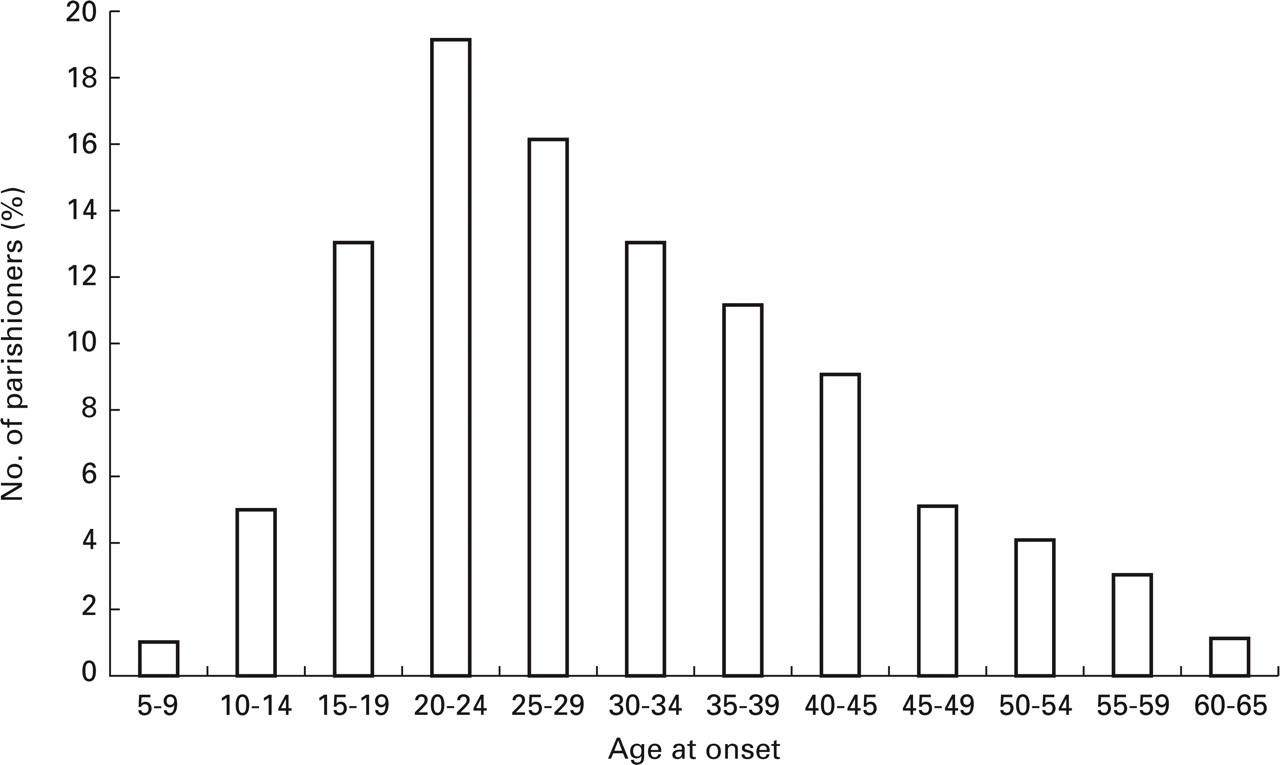
Age of onset in 358 parishioners who gave fairly exact information.
In those who gave a rather precise time of onset, this had taken place most often up to 5 years ago, more infrequently between 5 and 10 years ago, and only exceptionally > 10 years ago. A relatively long duration of the interval from the onset of jabs seemed to lead to imprecise statements concerning the actual age of onset.
Duration of paroxysms
In the vast majority of cases, the paroxysms lasted up to 3 s (Table 3). Many patients claimed that the jabs were extremely brief, just lasting a second or even only a fraction of a second. Others claimed that the paroxysms rather lasted 3 s than 1 second. Still others, however, were unable to specify any specific number of seconds, other than that they felt rather certain that the jabs did not exceed 3 s. All these have been categorized as belonging to the 1–3 second duration group, without any further attempts at subclassifying them from a temporal point of view. Some claimed that although the attacks generally lasted 1–3 s, occasional attacks might last longer, at times 5–10 s (i.e. in 5.4% of the cases, Table 3). Except for the duration, the symptomatology in this subgroup did not seem to differ from that in the other ones. Since the majority of attacks seemed to be within the 1–3 s duration group, this group forms the basis of the present study.
Duration of paroxysms
Some had only longerlasting attacks. They will be dealt with separately.
In a number of cases, there were more than just occasional attacks that seemed to last 5–10 or more seconds. Because of the uncertainty as to the nosologic positioning of these paroxysms, they are not included in this context. Attacks lasting ≥10 s will be scrutinized in a separate communication.
Validation of data collection
Putative negative effect of compliance
Low compliance might have a ruining effect upon prevalence figures, also in a study like this. The impact of the nonexamined fraction upon the final prevalence figures may at times only be conjectured.
In the present study, the inclusion percentage was high(88.6%). The error introduced by noncompliance in the present study will therefore anyhow be of minor importance. Even with the ‘worst scenario’, i.e. that the remaining, nonexamined, parishioners had no jabs, the mean percentage of jabs would still have been high (Table 4).
Dependence upon compliance

If so: overall mean (i.e. 627 of 2016 (i.e. 2075–59, Table 1)) 31.1%.
Jabs in the late-comers
A good hint at the prevalence of jabs in the nonexamined parishioners can be obtained from the observations in the group of late-comers.
The study was intentionally interrupted at 1809 parishioners, because the daily ‘gain’ of new parishioners was clearly declining. By concerted effort, however, we succeeded in bringing the investigation back on the rails ∼2 months later and succeeded in including another 29 parishioners; these were mostly long-distance commuters, draftees and students (7). The percentage of jabs among these proved to be of the same level of magnitude as in the total cohort, i.e. 34.5% vs. 35.2% (Table 5).
Jabs among the 29 last examined parishioners

Percentage with jabs: 34.5%.
Along the same line, the jabs frequency curve seemed to flatten out at around 1100 inclusions (Fig. 1). This is further evidence that probably the prevalence rate jabs would not have fallen drastically, had the study been extended.
Intra-rater consistency as regards questionnaires
The jabs part of the questionnaire as such was validated with two different approaches. In both situations, sufficient time had been allowed to elapse to hinder any memory from the first examination on the part of the principal investigator (O.S.). Most parishioners had been examined > 9 months earlier, and several of them even ≥ 1.5 years earlier.
Re-check of records (n = 100)

Kappa value: 1.00.
Re-examination of parishioners regarding jabs (n = 41)

Kappa value: 0.841 (S.D. 0.162).
In the one case, jabs were present on examination I, but only possibly present on examination II. In one case, adequate questioning was not carried out concerning jabs on the second examination. Both were, nevertheless, reckoned as failures.
Patients excluded due to inadequate information (n = 2); and one patient was not asked regarding jabs – on both occasions. (The original number in this group is accordingly=23).
Another parishioner had a positive jabs history at examination II, but the jabs proved to have started after examination 1, for which reason this case is not reckoned as a failure.
These parishioners were randomly selected, using identification numbers ending on 0 or 5. The selected individual would be changed if: the parishioner selected was well known to the investigator (so that he could remember something about the headache), and/or the headache had such characteristics that the investigator could remember some of the case history, and/or the parishioner was not so easily accessible or demonstrated some kind of unwillingness to be examined a second time. In that case, the number above/below the selected number would be chosen. There were only six exceptions to these rules. The parishioners were accordingly not selected according to age, sex, or similar variables. The selected group consisted of 21 females and 20 males.
There was a striking concurrence between jabs-positive findings on both occasions; there was also a satisfactory concurrence between the jabs-negative findings (Table 7) on both occasions. A kappa value of 0.841 (S.D. 0.162) was found. In one case with a negative story of jabs on examination I, jabs was present on examination II. Jabs had, however, arisen after examination I. This possibility must be reckoned with when the respite between examinations is of this magnitude. Consequently, this single case was not considered as a failure.
It should be emphasized that with this latter design the potency, robustness, and steadfastness of the questionnaire is really put to the test. However, the favourable statistical outcome does not prove that the high jabs prevalence is ‘pure silver’. The strong similarity in the findings of the principal investigator concerning jabs (intrarater consistency), does not entirely exclude the possibility that the findings may have been skewed to the same extent on the two occasions, due to slight misconceptions on the part of the investigator and/or his interviewed subjects. The following observations count against this view:
The first author has extensive experience with this type of pain since the first description of jabs and jolts in 1979. The manifestations described in the present work are consistent with the original concept of jabs.
The manifestations of jabs in the present work are also strikingly similar to detailed descriptions given elsewhere (e,g 9–11).
The dialect synonyms that were presented to the parishioners in addition to the regular Norwegian words appeared to be well apprehended and perceived by the parishioners.
Discussion
This study was first and foremost a cross-sectional study. Although one also had the parishioners' life-long experience with jabs in mind, it is in the cards that this information is less valid.
With these reservations, this study has shown a prevalence of jabs (ISH) of 35.2% among an unselected rural Norwegian population, aged 18–65 years.
The extraordinarily high prevalence of jabs is an entirely new feature made in this study. Because of recall bias, the obtained figures may actually be minimum figures.
It is remarkable that the number of jabs varied so much in the course of the study period (Fig. 1), with an extraordinarily high frequency in the initial phase – the curve flattening out in the end phase. This may, at least partly, be a consequence of the fact that many of the worst headache cases, and many migraineurs (Sjaastad: unpublished data) and among them many females – were enrolled in the early stages of the study.
The finding of a higher prevalence among females than among males is in concurrence with previous findings (11). However, the relative female/male prevalence of ∼1.49 in our cohort, differs essentially (P = 0.0003, Fisher's exact test) from the previously observed ratio of 6.6 (11). The observation of a relatively high prevalence also among males is another new feature.
As regards the duration of the single paroxysm, this seems to be in agreement with the findings of Pareja et al. (11): the duration was 1–3 s in the vast majority of the cases. The duration may, in other words, frequently seem to be longer than ≤1 s, as stipulated by IHS. The term jabs has therefore preferably been used as regards the present findings.
Finally, the mean age of onset seems to be younger than hitherto known: ∼28 years, vs. 47.1 in a previous series (11).
Previous epidemiological studies
‘Indirect’ studies
Various previous studies pertain to the frequency of ISH. The Pareja et al. study (11) was a hospital-based investigation, comprising patients who consulted the Departments of Neurology or Eye Diseases in the course of 1 years. The reasons for consultation were partly more than just minimal eye diseases, e.g. glaucoma and cataract. It is unclear whether anyone really made a Hospital contact only because of the ISH. The occurrence they observed per year and per 100.000 of the population, i.e. 33, cannot – under those circumstances – be expected to be a true prevalence figure for ISH. The finding that 5 patients in their series(14%) had a chronic ISH, defined as paroxysms on ≥ 80% of the days, may to some extent indicate that rather severe jabs made up this group. The value of the Pareja and coworkers' study is probably first and foremost that it describes in exact terms the clinical manifestations of ISH, with and without an accompanying, major headache.
Two studies pertain to the relative frequency of ISH among migraineurs/controls (6) and migraine/tension headaches (12), and for those reasons have an indirect bearing upon ISH in the population at large, since both migraine and tension-type headache are so prevalent.
Raskin & Schwartz (6) found a prevalence of ISH of 42% among migraineurs, as against 3% among controls. Support for the high prevalence of ISH in migraine is at hand in another study, with 200 cases of ISH in 530 headache cases (a mixture of migraine/tension headache cases), i.e. in 38% of the cases (12). Migraine (with and without aura) and tension-type headache are prevalent in the population at large: 15% and 66%, respectively, of the individuals in Rasmussen's study (1); thus, 81% of the population had either migraine or tension-type headache. This would indicate that in unselected population groups, the prevalence of ISH would be high: If around 38% of migraine plus tension-type headache had ISH, then that could indicate a prevalence of ISH of around 30% in the general population. This reasoning will probably grossly apply even though in many of the cases there has undoubtedly been a ‘double headache’. The figures would be approximately the same if the data from Monteiro's study concerning headache prevalence were to be used as a basis for calculations (2).
(b) Population studies
There are two studies pertaining to ISH prevalence proper (1–2), the one based on townsfolk from Porto (n = 2008) (2), the other (1) on 740 individuals in Copenhagen (Table 8), showing prevalences of 0.2% and 2.0%, respectively. The difference in prevalence between these studies is actually only 1.8% (Table 8), but the ratio between them 10 (i.e. 2 vs. 0.2%). Even more impressive are the ratios between the present prevalence on the one hand and the ones from the other two studies (1, 2, see Table 8). These differences are so marked that they cannot be explained on the basis of chance variation.
Population studies of ISH/jabs

P.E.,Personal examination, semistructured interview; Q, Questionnaire;
Ca. 20% of the study group examined personally by P.M. ISH prevalence: 0.5%.
An extensive questionnaire was also filled in by the principal investigator (O.S.).
Since the other studies concerning prevalence in the population at large are in duplicate and the present one is a solitary one, it would not be unreasonable to surmise that in the present one, some type of error might have been introduced. The other two studies might putatively represent the truth. The design of the present study has already been detailed herein. What is then the design of the previous studies?
A crucial question is whether the design of the studies is such that ISH can be unravelled. The salient facts concerning the Portuguese study (2, +personal communication, March and July, 2000), have been scrutinized. In brief, the main questions pertaining to a putative, shortlasting headache in the Portuguese questionnaire were:
How long time does the pain actually last with (7.1) and without (7.2) treatment? There were the following response alternatives: seconds/minutes/hours/days. Prior to these questions, there were questions regarding a main headache: have you had headache; if so, from which age; when was the last time; what was the frequency? and so forth.
When the questioning in a given case had proceeded to the question concerning duration, the emphasis would in all probability already be so heavily focused upon a major headache (present in ca 83% of their cases), that a deviation from the main track is unlikely to happen. The task amounts to the following: would it be possible in this setting, with the aforementioned question(s), to identify another headache, inferior in every respect, on top of the major headache in focus? And this should be done without flagging that one now was going to ask about a putatively different headache, emphasizing its brevity and other specifics. The answer, in all probability, is: no. Furthermore, the interviewers were medically untrained. Grossly speaking, the design of the study probably was one for major headaches (and for those it was excellent!), but not for ISH.
Details are not known to the same extent about the Danish study (1). However, some of the above reasoning may also pertain to that study.
The moral may seem to be that if one wants to study specific headaches, the design must be adapted accordingly. As it may have emanated from the control studies and the aforementioned reasoning, we firmly believe that the present investigation reflects the situation as regards jabs in this part of the world – and at this time. We have little reason to believe that the situation would be widely different elsewhere.
Duration of attack
A special problem concerns the duration of ISH (8), which by the IHS has been stated to be ‘a fraction of a second’. Paroxysms ‘lasting a few seconds’ have accordingly by some researchers (14) been considered atypical; this goes for paroxysms down to 2–3 s duration (13). The present study demonstrated that a duration of 1–3 s seems to be the rule, not the exception. The IASP description states that the duration may be 1–2 s; (there may also be a lingering pain lasting up to a minute). Pareja et al. (11) used as an inclusion criterion only ‘ultrashort stabbing pain’, without specifying any set upper limit of duration (11). However, of their patients, 69% experienced 1-second-long attacks, whereas 82% of the cases would be included in the category: duration ≤3 s; the remaining 18% had attacks of 5–10 s duration. As a consequence of their results (11), a duration of ≤3 s was used as a routine standard in the present study. The fault one introduces by not primarily integrating those lasting ≥4 s would probably be a minor one (Table 3) and could be compensated for by the ‘purity’ of the series obtained. On the other hand, it was felt that inclusion of only around 70% of the cases (i.e. ≤1 second duration (11)) would be to introduce too great an error.
Parishioners exhibiting longerlasting paroxysms will be treated as a separate group. At a later stage, one will try to explore whether such longlasting jabs in any other way seem to differ from the main body of jabs, or whether there are indications that they may be of an entirely different nature.
Age at onset
Variables like age at onset may be markedly affected by recall bias. This is a rather problematic issue: First of all, there may have been few jabs in the course of a lifetime: it may have been far between them, and they may have appeared far back in time. In a 65-year-old parishioner, jabs may have started 20–40 years ago, for instance. On top of that, jabs may have been of only mild/moderate severity. This combination of brevity, lack of impact, and distance in time may understandably create a situation where a precise memory as to onset may be weak (Fig. 3). For that reason, the mean age of onset among those with a fairly precise memory as to this variable is only recorded as ∼28 years.
As already alluded to (7), and as demonstrated herewith, jabs in all probability occur frequently. Although jabs are most frequent in females, they are also not infrequently observed in males. Jabs generally last up to 3 s and appear all over the head, but more frequently in the anterior than posterior parts.
Footnotes
Acknowledgements
The authors are indebted to Glaxo-Wellcome of Norway for their generous support of this study. We are also most grateful to the staff members of the Health Center in the commune of Vågå, at Vågåmo, for all their chores in keeping this investigation on the rails. Thanks are also due to the various Institutions that were helpful with regard to the recruitment. Finally, we want to thank the parishioners in Vågå who wholeheartedly collaborated with us during this investigation.