
Abstract
As migraine is the result of an inflammatory mechanism with serotonergic signalling, leucocyte function, platelet function and intercellular communication between those cells is likely to be connected to the final pathway of the disease. We examined P-selectin expression on platelets (platelet activation) and leucocyte-platelet aggregate formation in 72 migraine patients during their attack-free interval and controls using a flow cytometric assay. Patients suffering from migraine without aura had a significantly increased platelet activation and leucocyte-platelet aggregation compared with the control group, unlike the migraine patients with aura. Patients who had taken a triptan within 3 days prior to the investigation showed platelet activation values similar to the control group. The variations in platelet activation patterns of migraine subgroups could indicate different pathomechanisms. Even outside an attack, migraine patients, particularly those without aura, show an increased level of platelet activation which seems to be down-regulated by triptans. This mechanism may account for the triptan-induced increases in headache frequency. The involvement of proinflammatory platelet-leucocyte cross-talk suggests a possible therapeutic strategy using anti-inflammatory drugs.
Introduction
For many years the pathophysiology of migraine has been linked to platelet dysfunction, particularly since 90% of body serotonin (5-HT), the main neurotransmitter involved in migraine, is stocked and released on demand by platelets. After the initial assumption that migraine might be simply a platelet disorder (1), many now believe that irregular platelet function is a secondary effect rather than causative. Previous findings still suggest that platelets may serve as a cellular model for the changes in the central nervous system (2–4).
Although conflicting reports have been published, most investigations found evidence of increased platelet activation even during the headache-free period (see (5) for reference). After ex vivo stimulation some studies suggested decreased platelet responsiveness in aggregometric assays (6, 7), which was attributed to an expression of ‘exhausted’ platelets after in vivo stimulation, possibly related to an increased vulnerability to oxidative stress.
Recent research on migraine pathogenesis has been focused on the putative central nervous signal transmission and neuronal regulation in the trigeminovascular system which has become increasingly understood during the past 20 years (8). However, the final pathway with its cellular regulation also plays an obligatory role in the feedback mechanism, and it may have clinical importance as one gate to the therapeutic approach with serotonin agonists.
We have learned that the dynamic functional platelet changes in vivo do not occur independently of other cells (9): for many conditions such as infection (10), diabetes (11, 12), cardiovascular (13, 14) and cerebrovascular (15) disease, the cellular interaction represents a crucial mechanism which could play a role in propagating or maintaining headache pain. Recently, we demonstrated increased platelet activation and platelet–leucocyte interaction in migraine patients and suggested that the intercellular interaction between platelets and white cells may contribute as one factor to the well-established coincidence of migraine and stroke (16).
Another common clinical finding that is not yet fully understood relates to migraine treatment with triptans: often headache therapists encounter an increasing frequency of migraine attacks in those patients who often use triptans, leading to even higher triptan use. This phenomenon can be clearly distinguished clinically from other analgesic-induced headaches (17) and has already been separately categorized in the reviewed International Headache Society (IHS) classification as IHS-ICHD-II code 8.2.2 (18).
In this study we aimed to find specific subgroups contributing to the differences in leucocyte–platelet interaction between migraine patients and controls, and sought evidence of a triptan-related influence on the investigated haematological parameters.
Patients and methods
Patients
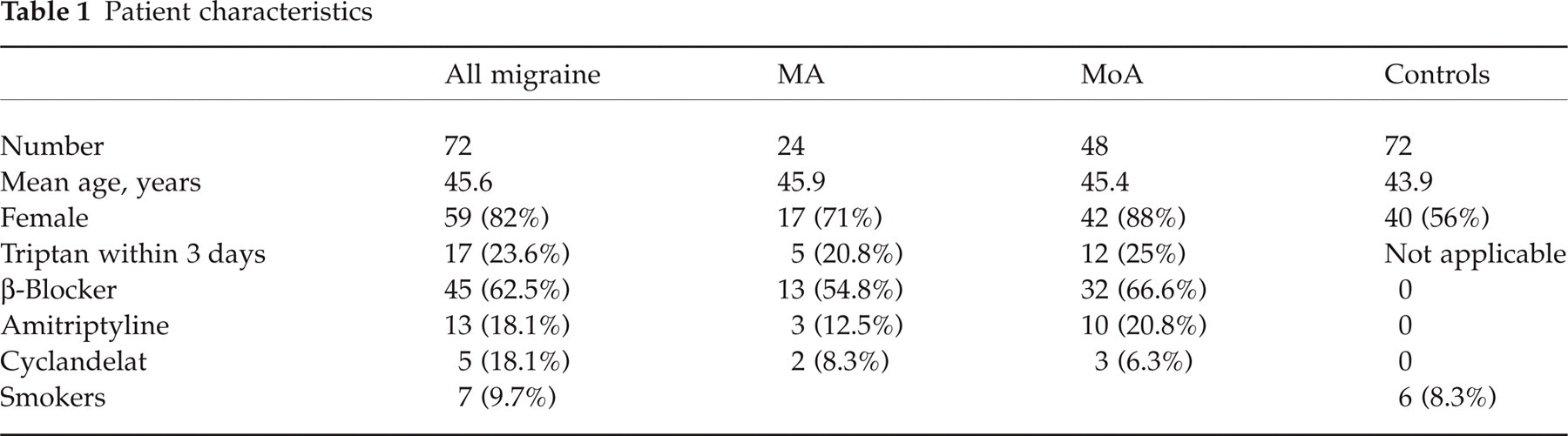
Seventy-two patients attending our headache out-patient clinic at the University Hospital Kiel with confirmed diagnosis of migraine according to IHS criteria (18) were included. Forty-eight suffered from migraine without aura (MoA), 24 from migraine with aura (MA). The study was approved by the local ethics committee, and all participants gave written informed consent. Three patients had previously experienced intermittent cardiac arrhythmia without the need for specific treatment. Two patients were non-insulin-dependent diabetics. No patient had experienced an infectious or febrile illness at least 1 week prior to the study. The control group consisted of volunteers from medical staff and patients who were all free from headache, history of cardiac or cerebrovascular disease, diabetes, and acute infection. Both patients and controls had been free from drugs known to affect platelet function for at least 2 weeks. Of the 72 migraine patients, 19 had suffered an acute migraine attack and 17 of those patients (23.6% of the whole patient group) had subsequently taken an oral or subcutaneous triptan during the last 3 days. Further details of comedication, patient and control group characteristics are reported in Table 1.
Patient characteristics
Methods
Venous blood was drawn from an antecubital vein only during morning hours and anticoagulated with 3.8% sodium citrate. After 10 min of resting time without further manipulation at continuous body temperature, samples were processed. For flow cytometry we used direct fluorescent markers (all commercially available by Coulter Immunotech, Krefeld, Germany). Whole blood was diluted 1 : 10 with warmed HEPES buffer and aliquots of 50 µl were incubated for 5 min with CD61–PE (a non-activation-dependent subunit of the GP Iib–IIIa complex) and CD45–FITC or CD62P–FITC.
Platelets were identified by forward/sideways scatter properties and again by triggering on FL2 to detect CD61–PE+ cells only. To measure platelet activation we quantified the surface expression of the CD62P epitope (P-selectin) on the platelet, which has been shown to be a reliable activation marker in cardiac and neurovascular patients (19). The results were recorded as mean fluorescence in the CD62-P-FITC channel. Leucocytes were identified by using the quantification of the panleukoytic marker CD45 and their forward/sideways scatter properties, then the double fluorescent events positive for both CD45 and CD61 were counted as platelet–leucocyte aggregates. For statistical analysis we used the percentage of platelets aggregated to leucocytes in relation to all platelets detected. This assay had been in routine use in our laboratory for 3 years prior to this investigation.
A parallel blood count ascertained platelet and leucocyte numbers within the normal ranges in all participating patients and controls.
Statistic analysis
All values are expressed in mean ± SD. The Mann–Whitney U-test was used to compare groups; significance was considered with P < 0.05 in two-tailed tests.
Results
Platelet activation
During the headache-free interval investigated here, migraine patients expressed more of the activation-dependent platelet epitope P-selectin compared with the control subjects. This was due to a highly significant (P = 0.001) difference in patients suffering from migraine without aura; in those affected by migraine with aura the slight difference failed to reach significance in this sample size (Table 2a). Patients who used a triptan within the last 3 days did not show this significant increase in platelet activation, unlike those without recent triptan intake (Table 2b). Since the group of patients with MoA and triptan use comprised only five patients, we analysed both groups of migraine patients together; however, this result of ‘normalized’ activation status after triptan use was detectable in both groups separately.
Platelet activation and leucocyte–platelet aggregation

Platelet–leucocyte aggregation
With regard to platelet–leucocyte aggregation, a substantial difference between the two migraine subgroups could also be demonstrated: MA patients had moderately elevated numbers of aggregates (4.9 vs. 3.9% in controls, not significant), whereas patients suffering from MoA showed a markedly increased proportion of platelet–leucocyte aggregation (6.1%, P < 0.001). In this migraine group a relative decline in the ratio of monocyte–platelet aggregates in favour of polymorph–platelet aggregates was seen, when compared with normal controls (Table 2a).
Discussion
Platelet activation
We found evidence that migraine is linked to a higher baseline of platelet activation compared with controls outside the duration of a migraine attack. In addition, we saw particularly the subtype of migraine without aura increased in both linkage to leucocytes and activation-dependent epitope expression. Considering that activated platelets have undergone a conformational change and express more IIb-IIIa receptors, which mediate aggregation, it readily explains the observation by Kozubski et al. (20) of a significantly increased number and affinity of fibrinogen receptors on the platelet surface in migraineurs. A direct measurement of activation-dependent platelet epitopes as performed in this study has not been done before; however, previously reported results have already indicated increased platelet activation using quantification of thromboxane production (5, 21) and platelet secretion products (22, 23). Although our method is likely to be less prone to artefacts, augmented platelet activity in these patients can still not necessarily be referred to as a suitable indicator of an initiating mechanism in migraine pathology.
What is the meaning of augmented platelet activation? If this was not an effect purely secondary to leucocyte-mediated up-regulation or inflammatory kinin action, the increased platelet activation demonstrated here could mirror a new biological baseline setting in adaptation to a migrainous disposition.
In 1966, on the basis of their research on platelet and plasma serotonin content in migraine patients, Lance and Anthony (24) postulated a serotonin-releasing agent which may induce serotonin discharge from platelets during a migraine attack. Subsequent research was controversial but a decrease in platelet serotonin after acute migraine proved to be a consistent finding which could be attributed to depletion of 5-HT storage. The release of 5-HT from platelets during the attack may serve in part as an endogenous analgesic principle. Fast 5-HT release is most effective from a preactivated platelet state. The up-regulation of platelet activation during the headache-free interval could be explained as a mechanism to achieve higher thrombocytic potential to release endogenous serotonin.
Platelet–leucocyte interaction
Another basic difference with regard to platelet function that we found during this investigation of migraine patients was the formation of aggregates with leucocytes. Both platelet–leucocyte aggregates and platelet activation are closely linked phenomena, as has been shown in diabetes, inflammation, cardiovascular disease, and stroke. Leucocytes can communicate with activated platelets via specific binding sites [e.g. P-selectin glycoprotein ligand 1 (PSGL-1)] which itself leads to enhanced leukocytic properties. This platelet activation and leucocyte binding is propagated by infection or inflammation (10) and may well be part of an inflammatory vascular process underlying migraine.
Various research groups have investigated the role of leucocyte function in migraine; a study of lymphocyte subsets and integrin expression in peripheral blood was performed by Empl and coworkers (25), who found an up-regulated humoral and cellular inflammatory signalling system with significantly higher proportions of integrin high-expressing T-helper cells in subjects with MoA compared with MA, a finding parallel to our observation of an increased intercellular communication in MoA patients as opposed to those with MA.
It is noteworthy that in our study cohort immunological activation in migraine patients is indicated not only by lymphocytic reaction with memory cells representing a long-standing process of neurogenic inflammation, but acute-phase leucocyte subsets are also involved (as seen by the increased neutrophil fraction attached to platelets). This suggests a continuous inflammatory process even in the pain-free state, and emphasizes the role of inflammation in migraine pathophysiology.
Various different platelet–leucocyte interactions are known: recognition and adhesion is mediated between P-selectin and PSGL-1 on leucocytes, as there is a β2-integrin (MAC-1)-dependent adhesion step between both cell types (26, 27). Different, in part antipodal reactions follow: ploymorphonuclear lymphocytes (PMN) can, depending on their activation to a variable extent, inhibit platelet aggregation (28, 29). This effect is mediated by release of nitric oxide and short-lived reactive oxygen species and can be enhanced by ascorbate (30). PMN, in contrast, also have a well-described capability to propagate platelet activation by releasing platelet activating factor. Both effects are in fine balance. In these patients our data support an emphasis on a platelet-stimulating effect of aggregated leucocytes since PMN–platelet aggregation is changed in parallel to platelet activation.
In this context, anti-inflammatory steroid treatment of migraine should be mentioned. In small reports the use of dexamethasone has proven successful in treating acute migraine attacks (31–33) or in preventing early migraine recurrence as an medication additional to triptans and non-steroidal drugs (34). The Canadian Association of Emergency Physicians has integrated this approach into their guidelines (35). The steroids interact with the intercellular communication between leucocytes and platelets, reduce inflammation and may thus alleviate headache. However, there are no data showing a beneficial effect of steroids in prophylactic therapy. It seems reasonable that the effect of non-steriodal anti-inflammatory drugs commonly used in the treatment of migraine is at least partly exerted by the mechanism of blocking inflammation at the beginning rather than only acting on the result of inflammation, the cyclooxygenase-mediated pain signalling alone.
Reducing platelet–leucocyte cross-talk could play an additional part in the treatment of migraine. This therapeutic approach has already been successfully evaluated in cardiac ischaemia by using soluble antibodies against P-selectin or against PSGL-1 on the leucocyte (36).
Influence of triptans
In patients who had recently experienced migraine attacks and had used triptans, platelet activation was reduced to normal values, whereas in those patients without triptan use a similar effect was not seen. Since platelet–eucocyte aggregation was not substantially changed, triptan may exert a direct effect on the platelet surface by inhibiting the transformational changes in the transition from resting to activated status.
Although by acting as 5HT-1B and 1D agonists triptans ameliorate migraine headache, they seem simultaneously to down-regulate the activated state of the platelets and could thus weaken the endogenous thrombocytic counterreaction. This may result in the commonly seen reduced duration of drug action and interval between the attacks.
On the basis of the current data it can not be excluded that this effect may not be drug-related but due to the fact that all patients who had used a triptan within the previous 72 h obviously had a migraine attack which was considered by the patients worth treating, unlike the other patients, who had not. This would be indicative of a periodic systemic undulation of the platelet activation status in migraine. However, this theory would not explain the increasing headache frequency in triptan users. Whether the changes we observed are a function of time in relation to migraine attacks themselves or to migraine-related triptan medication is the subject of a study sequel currently underway.
An unexpected finding was the observed difference between migraine patients with vs. without aura according to the IHS diagnostic criteria.
As clinicians in a specialized reference centre, we see a high proportion of complicated and disabling forms of migraine headache and, particularly, more often among MoA than among MA patients. This might be an indication that a blood-based proinflammatory process involved in the pathophysiology of migrainous headache outside neurovascular structures is more pronounced in MoA patients. The higher rate of platelet activation and leucocyte platelet aggregation would support the pathophysiological hypothesis.
The reported findings of intercellular communication and platelet activation in migraine raise new questions on possible basic differences between the pathophysiology of migraine with and without aura; on a stronger therapeutic approach to acute migraine with drugs that modulate inflammation; and on the mechanism of triptan tolerance in migraine. These need further examination.