
Abstract
The aim of the present study was to decide on which day in the course of postlumbar puncture headache (PPH) an epidural blood patch (EBP) should be performed to minimize suffering. A cohort of 79 patients (64 female, 15 male) was followed prospectively for 14 days and the consequences of performing an EBP on different days were studied. If no EBP was performed, the patients would accumulate 141 days with PPH5 (bedridden most of the day), 216 days with PPH4-5 (bedridden more than half the day), and 293 days with PPH3-5 (bedridden half the day or more). If these patients were patched on day 2, 3 or 4 after an initial observation of the PPH grade on day 1, the expected suffering was substantially reduced, and the more the earlier in the course the EBP was performed. If the strategy was to treat only patients with PPH5 with an expected 90% success rate, the reduction compared with no treatment was 50% if treated on day 2, 37% if treated on day 3, and 29% if treated on day 4. The corresponding figures for treating patients with PPH4-5 was a 51, 44 and 29% reduction, and for PPH3-5 the reduction was 62, 49 and 35%, respectively. Irrespective of strategy, the expected reduction of suffering in the cohort was greatest when the EBP was performed early in the course of PPH. It is suggested that the decision to perform an EBP should be made at an early stage and offered to patients who have to lie in bed for more than half a day despite conservative treatment.
Introduction
Postlumbar puncture headache (PPH) is a position-dependent headache, which is generally believed to be the consequence of leakage of cerebrospinal fluid (CSF) through the dural rent created by the lumbar puncture (LP). When the leakage is sufficiently extensive for the brain to lose its CSF cushion in the upright position, headache ensues (1). The duration of headache may vary, but the median duration is about 6 days in most studies (1–3). The headache may be very severe and is frequently associated with nausea, vomiting, dizziness, tinnitus, and visual disturbances (4). The degree of suffering may be rated according to how much of the waking day the patient has to lie down due to PPH. This rating scale closely correlates with the degree of headache as reported on a visual analogue scale both in the recumbent and the upright position (3) and also reflects the additional burden of associated symptoms. Several studies have shown that the frequency of PPH is reduced by using thin (1, 5, 6) and/or blunt tipped needles (7) to create smaller rents in the dura. Females and younger people are at highest risk of developing PPH (5). Caffeine seems to have a moderate effect on the symptoms (8), but in most cases it is only recommended to lie down as long as the symptoms are severe and to take mild analgesics if necessary. The application of 10–20 ml autologuous blood as an epidural blood patch (EBP) near the rent has been shown to be immediately effective in about 90% of patients with PPH in several studies (9), but may be associated with side-effects such as low back pain (10). However, the therapy has become increasingly popular, although no definite guidelines for its use have been established.
We wanted to determine on which day in the course of PPH an EBP should be performed to minimize the suffering due to PPH. For that purpose we studied the expected consequences of performing an EBP on different days in a cohort of PPH patients, which we have followed prospectively without any EBP treatment in a previous study (3).
Subjects and methods
A total of 239 out-patients (155 female, 84 male), who were under investigation for a non-infectious neurological disease, participated in the investigation. Exclusion criteria were continuous use of analgesics or conditions which might confuse the evaluation of PPH later on, e.g. some cases of migraine or tension-type headache. This judgement was always made prior to inclusion. Demographic data included sex, age and drugs in use.
A diagnostic LP was performed at about 08.00 h and the patients were allowed to rise within an hour. The LPs were performed by different neurologists according to their preferred technique in each case. The first 137 patients were punctured at the Central Hospital of Akershus with a 22-G Quincke needle. Because both investigators moved to other hospitals, the last 105 patients were punctured with an identical technique at Ullevaal Hospital (n = 100) and the Central Hospital of Vestfold (n = 5) with a 20-G Quincke needle, which was in general use at these hospitals.
The patients filled in questionnaires at home, answering the following questions: if the patient experienced a headache which they believed was the result of the LP in the course of 1 week, the date and hour when the headache was first experienced and when it stopped were recorded and filled in prospectively. Only mild analgesics were allowed during the course of the illness, and no patient was treated with caffeine, epidural saline infusions or an EBP. Patients were considered to be suffering from PPH if they reported a postural headache within a week after lumbar puncture. They were asked to indicate on a 5-point scale how much of the waking day they had to lie down because of headache and/or associated symptoms: practically not (grade 1); less than half the day (grade 2); about half the day (grade 3); more than half the day (grade 4); practically the whole day (grade 5). In cases where the data were not filled in correctly and completely, an evaluation was made prior to analysis, and only data considered valid were used. We studied the course of the PPH grades within a frame of 14 days, which is the limit for PPH duration set up by a committee of the International Headache Society (IHS) in its definition of PPH from 1988 (11) and is in accordance with data from several studies (1). We considered the data regarding the PPH grade valid for a whole day if the onset of PPH was before 11.00 h.
We calculated the total suffering in the cohort expressed as days with PPH as a consequence of different strategies of treatment within a frame of 14 days. The total number of days with a certain PPH grade in the cohort is the sum of days with this PPH grade already experienced by the patched patients and days with the same PPH grade suffered by the non-patched patients during the 14-day period (NP in Table 1).
Consequences of different strategies for treatment of postlumbar puncture headache (PPH) in a cohort of 79 patients: no epidural blood patch (EBP) or EBP given on days 2, 3 and 4
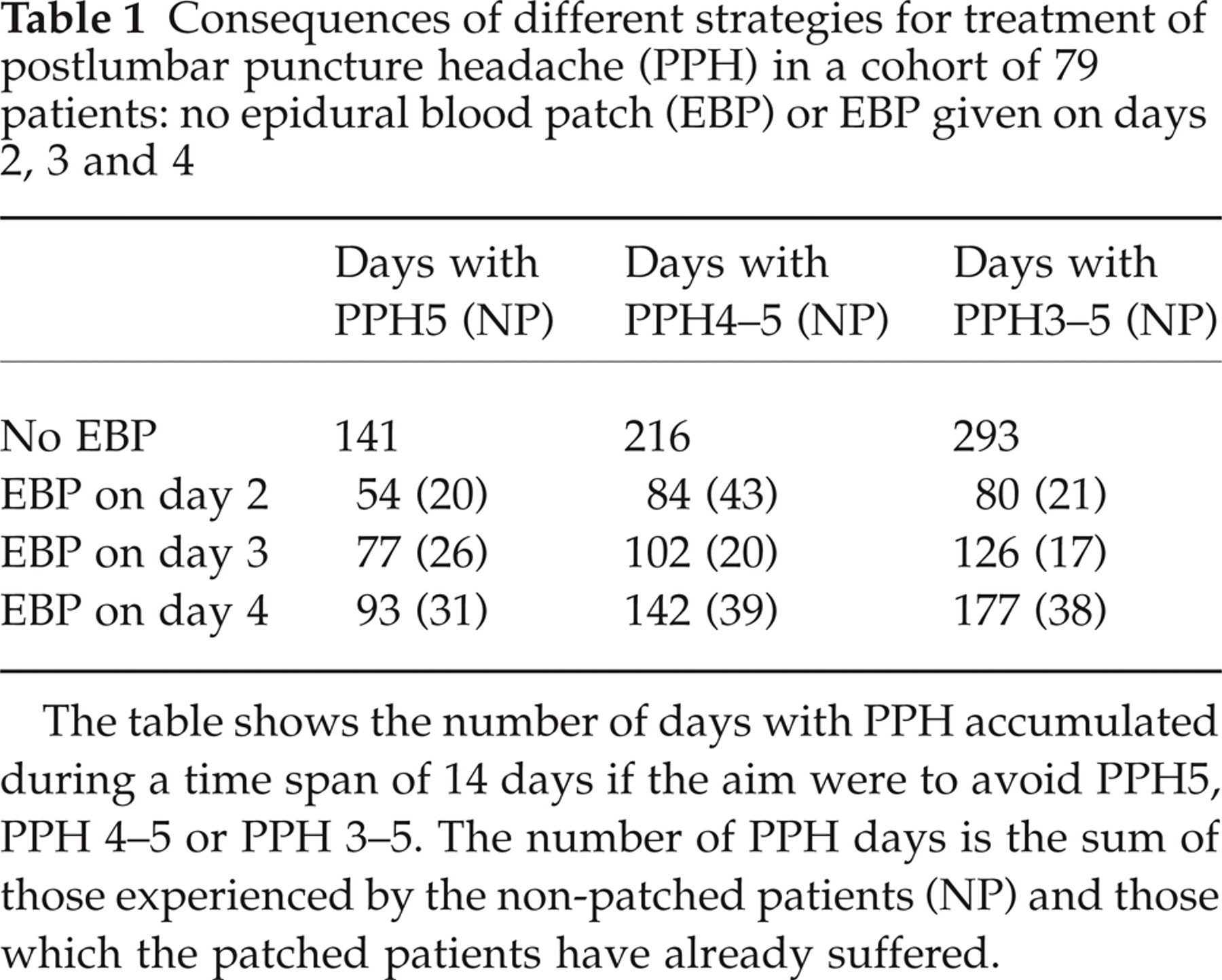
The table shows the number of days with PPH accumulated during a time span of 14 days if the aim were to avoid PPH5, PPH 4–5 or PPH 3–5. The number of PPH days is the sum of those experienced by the non-patched patients (NP) and those which the patched patients have already suffered.
Results
Eighty-eight (37%) of the 239 investigated patients experienced PPH. Seventy-nine of these patients delivered reliable PPH data and constituted the cohort (64 female, 15 male). The mean age was 38 years for both sexes. Fifty-eight per cent of the patients in the cohort had been punctured with a 20-G, the remainder with a 22-G needle. Figure 1 shows the percentage of different PPH grades and recovery from PPH in the course of 14 days. About half the patients had recovered from PPH in 6 days. After 14 days three patients still reported PPH, two of them experienced the lowest grade form, but one patient still reported PPH in its most severe form.

Percentage of patients with different postlumbar puncture headache (PPH) grades and patients who have recovered from PPH during a course of 14 days. Results from a cohort of 79 PPH patients.
Non-patched patients accumulated 141 days with PPH5 within 14 days, 216 days with PPH grade 4 or 5, and 293 days with PPH3–5 (Table 1). An EBP would reduce the total number of days with PPH, although the cohort would still be burdened with suffering from PPH experienced by the non-patched patients (NP in Table 1), and by the patched patients prior to the patch. Table 1 shows the consequences of performing an EBP with a lag of different numbers of days following PPH onset. If the aim were to avoid PPH5, the accumulated failures as expressed by the total number of days with PPH5 in the cohort would be 54 days if patched on day 2, 77 days if patched on day 3, and 93 days if patched on day 4. By postponing the EBP, an increase in suffering for the total cohort would also be observed if the aim were to avoid PPH4–5 or PPH3–5. An EBP postponed to day 5 would be associated with the highest number of days with PPH, but for the sake of simplicity these results are not shown. By delaying the EBP, the expected number of days with PPH in the cohort increased mainly due to an increase in the number of days with PPH prior to the patch, whereas the number of days with PPH in the non-patched group (NP in Table 1) was minimally affected by the delay.
These results are based on the supposition that an EBP is 100% effective, which it is not. The more ineffective the EBP, the more additional days with PPH would be experienced by patched patients. In the present study the median duration of PPH was 6 days (Fig. 1). By multiplying the expected number of remaining PPH days with the number of patients who do not profit from an EBP it is possible to calculate the expected number of additional days with PPH as a consequence of an EBP performed on different days. If the failure rate is set to 10 or 20% (Table 2), the pattern visible in Table 1 still emerges. The longer an EBP is delayed, the more days with PPH are experienced by the patients in the cohort.
Consequences of different strategies for treatment of postlumbar puncture headache (PPH) in a cohort of 79 patients: no epidural blood patch (EBP) or EBP given on day 2, 3 and 4

The table shows days with PPH accumulated during a time span of 14 days according to principles described in Table 1, but taking into account the possibility that an EBP might be non-efficient in 10 or 20% of the cases.
Figure 2 shows the reduction in number of days with PPH as a consequence of an EBP given on days 2, 3 and 4 compared with no EBP, given that an EBP is effective in 90% of cases. Irrespective of strategy, the expected reduction of days with PPH was greatest if the EBP was performed on day 2. If the strategy were only to treat PPH5, the reduction compared with no treatment would be 50% if treated on day 2, 37% if treated on day 3, and 29% if treated on day 4. The corresponding figures for treating the patients with PPH4–5 would be a 51, 44 and 29% reduction, and for PPH3–5 the reduction would be 62, 49 and 35%, respectively.

Reduction of days with different postlumbar puncture headache (PPH) grades as a consequence of performing an epidural blood patch on day 2, 3 or 4 if the epidural blood patch were inefficient in 10% of the cases. The reduction is shown in per cent of expected number of days with PPH for untreated patients corresponding to the indicated PPH grades. ▪, PPH5; , PPH4–5; □, PPH3–5.
The expected number of days with PPH was lowest when all PPH grades from 3 to 5 were treated (Table 1). However, based on observations from the day prior to treatment, it would be necessary to perform an EBP on 75% of the patients on day 2, 72% if the EBP were delayed to day 3 and 63% if it were performed on day 4 (Fig. 1). The corresponding percentages for treating patients with PPH4–5 or only PPH5 would be substantially reduced, but the numbers of patients in need of treatment would still be high (29–59%).
Discussion
The study of the present cohort of 79 PPH patients, which was followed prospectively for 14 days, permits calculations regarding expected suffering expressed as total number of days with different PPH grades as a consequence of an EBP performed on different days or not at all. The results suggest that if EBP is regarded as an effective and safe treatment for PPH, it should be performed at an early stage to minimize suffering from PPH.
EBP was introduced as an efficient treatment for PPH more than 40 years ago. After many years of experience with this treatment it is now generally recommended to offer this therapy to patients with moderate to severe PPH and to inject 10–20 ml of autologuous blood near the rent and to let the patient stay in bed for 2 h after the injection. Contraindications may be coagulopathy and systemic or local infection (9). The treatment has been estimated to be effective in 60 to nearly all patients with PPH (9). The beneficial effect is probably due to the creation of a gelatinous tamponade followed by a coagulation of blood at the site of the rent (12). Anaesthesiologists usually recommend this therapy at an early stage, but not during the first 24 h after LP when the failure rate seems to be high. Performed after 24 h, the failure rate is only 4% according to one study (13). Neurologists are usually reluctant to recommend EBP, and only if the symptoms prove to be intractable after several days, since it is imperative that any method of treatment ‘does not have more side-effects than the symptoms being treated’ (14).
However, most studies conclude that the EBP is a safe and effective treatment which is not connected with unacceptable side-effects. In a recently published review article it was concluded that mild transitory backache are most frequently observed, and only exceptionally have severe radicular pain in the legs and other more serious complications been observed (10). The review concluded that EBP performed more than 24 h after LP is an effective and easily performed treatment for PPH. This review contrasts with a recently published Cochrane database review, which correctly points out the paucity of adequately powered, randomized trials (15), but the conclusion that EBP should be reserved for ‘exceptional cases only’ will probably be disputed by anaesthesiologists and neurologists with experience in the use of EBP.
In the present study the strategy was to observe the patient for at least 1 day as a basis for the decision whether or not to perform an EBP. Irrespective of the degree of PPH, early treatment should be preferred. There are, however, a few dilemmas to be recognized. In the present cohort the number of patients who had to lie down at least half the day (PPH3–5) because of PPH and/or associated symptoms was exceptionally high (75% on the first day with PPH). If patients with a more severe grade of PPH are selected as canditates for EBP, the number would be reduced, but still high. Therefore, the use of resources may seem too extensive and an effort to reduce the number of candidate patients seems warranted. This may be accomplished by conservative treatment such as analgesics and caffeine in some cases, and the use of thinner needles than we used in the present investigation would certainly reduce the number of candidate patients. Also, some patients may refuse an offer to be treated with an EBP and prefer to lie down as long as the symptoms continue to be severe.
Previous studies show that the headache and PPH grade tend to decrease substantially in the last 2 days of the PPH period and the time for the headache to start or increase upon rising from the recumbent position increases (16). If this happens, the EBP should not be performed. However, the tempting strategy to wait and see if the symptoms are ameliorated or disappear spontaneously only increases the suffering in the cohort. Postponing the decision to treat leads to only a moderate reduction in the number of candidate patients and more suffering in the cohort as a whole. It does not seem warranted to avoid EBP because of a high risk of severe side-effects (9).
Although the use of EBP as a treatment for PPH is debated because of the lack of controlled studies, it continues to be commonly used. Those who advocate this treatment may disagree among themselves as to the indications for its use and how long after the onset of PPH one should wait before an EBP should be performed. Our findings suggest that patients who have to lie in bed for more than half a day despite conservative treatment with analgesics and/or caffeine should be offered an EBP the next day. The benefits and possible complications of the procedure should be explained to the patients, for them to decide for themselves if they want the treatment. The decision to perform an EBP should be made at an early stage.
Footnotes
Acknowledgements
The authors thank (in alphabetical order) Helge Nordal and Bodvar Vandvik for their stimulating assistance.