
Abstract
In this prospective study 37% of 239 patients developed a post-lumbar puncture headache (PPH) after a diagnostic lumbar puncture. PPH was more prevalent in females than males (46% vs. 21%; P = 0.0003) as were the severest form of PPH (64% vs. 23%; P = 0.02) and nausea (74% vs. 39%; P = 0.01) in those who developed PPH. Females scored their pain in the upright position more severe on a 100-mm visual analogue scale than males (median 60 mm vs. 47.5 mm; P = 0.02). The frequency of PPH was higher with the use of a 20-gauge compared with a 22-gauge needle in all patients (50% vs. 26%; P = 0.0002) and in females (57% vs. 36%; P = 0.02) and males (38% vs. 10%; P = 0.004), separately. Neither age, weight, height, nor body mass index (BMI), influenced the prevalence of PPH, but tinnitus was more prevalent in tall compared with smaller patients (53% vs. 17%; P = 0.02). Old age was associated with a long median pain delay upon rising, and also, small patients tended to report a longer median pain delay than tall patients. The pain intensity changed more slowly upon rising and reclining in patients with a high BMI than in those with a lower BMI (median 60 s vs. 12 s; P = 0.02). The results concerning height, BMI and needle size might be anticipated according to the leakage theory. In a multivariate analysis sex (P = 0.0003) and needle size (P = 0.0002) were related to the development of PPH on a statistically significant level. Furthermore, the pain severity was positively related to female sex (P = 0.03) and young age (P = 0.03). The pain delay increased with age (P = 0.008) and the pain decrease time increased with an increasing BMI (P = 0.04).
Keywords
Introduction
Post-lumbar puncture headache (PPH) is a position-dependent headache, which is frequently associated with nausea, vomiting, dizziness, tinnitus and visual disturbances. It is generally believed to be the consequence of leakage of cerebrospinal fluid (CSF) through the dural rent created by the lumbar puncture (LP). When the leakage is sufficiently extensive and the brain loses its CSF cushion in the upright position, headache ensues (1, 2). Presumably, the headache may be avoided if the leakage is insignificant and compensated for by the production of CSF and/or a high resistance to the CSF outflow. The CSF production and outflow rate might influence the time and pain parameters in relation to a rising test (Figs 1 and 2) described in a previous paper (3). Leakage may be favoured by a high CSF pressure at the level of the dural rent, and this pressure is assumed to be higher for taller compared with smaller persons in the upright position due to the weight of the CSF column. Furthermore, a large rent may leak more rapidly and extensively than smaller rents. The resistance to outflow may be dependent on the structure of the fatty epidural connective tissue, and also the capacity of the escape route through the intervertebral foramina, which get smaller with age due to osteochondrosis. To test elements in this theory, we studied the frequency and clinical characteristics of PPH as a consequence of sex, age, needle size, height and body mass index (BMI).

Schematic figure describing anatomy related to the aetiology of post-lumbar puncture headache (PPH). When the dura is punctured at B, CSF leaks into the surrounding fatty epidural connective tissue (C) and then leaves through the intervertebral foramina (D). In the erect position, leakage of fluid may cause pain as a consequence of the brain descending on the base of the skull, pressing the arteries and meninges and stretching the sagittal sinus. Leakage might increase as a consequence of high pressure at the dural rent in tall persons (a heavy CSF column; A), a wide dural hole due to a thick needle (B), a loose fatty epidural connective tissue in slim persons (C), or wide intervertebral foramina in young persons (D), thereby increasing the prevalence and severity of PPH.

PPH profile for tall (□) and small (▲) females. The profiles reflect median time and pain values based on each patient's median PPH profile. The body position is indicated for small females.
Subjects and methods
A total of 239 outpatients (155 female, 84 male) participated in the present investigation. Age was recorded for each patient, as were weight in kg and height in cm, and the BMI was calculated (weight/height2). Details concerning demographic data and inclusion and exclusion criteria have been published elsewhere (3).
A diagnostic lumbar puncture was performed at about 08.00, and the patients were allowed to rise within an hour. The first 137 patients were punctured at the Central Hospital of Akershus with a 22-gauge needle. Because both investigators moved to other hospitals, the last 105 patients were punctured with an identical technique at Ullevaal Hospital (100 patients) and the Central Hospital of Vestfold (five patients) with a 20-gauge needle, which was in general use at these hospitals. Three patients did not return reliable data and were excluded from the study.
The patients filled in questionnaires at home, answering the following questions: if the patient experienced a headache which he/she believed was the result of the lumbar puncture in the course of 1 week, the date and hour when the headache was first experienced and when it stopped were recorded prospectively. Only mild analgesics were allowed during the course of the illness, and no patient was treated with caffeine, epidural infusions or blood patch. Those who experienced headache were instructed to perform a rising test (3) in the morning (about 08.00) and evening (about 20.00) as long as the headache period lasted. Severity of the headache was recorded on a 100-mm visual analogue scale (VAS) in the recumbent position (VAS1): 0 mm = no headache, 100 mm = worst possible headache. If a headache occurred or worsened when the upright position was assumed, its maximal severity in the upright position was recorded (VAS2). The recorded time variables were the time interval from rising till the headache appeared or started to worsen (T1, ‘the pain delay’); the time from rising till the headache was maximal, permitting calculation of the time interval from worsening till the pain became maximal (T2, ‘the pain increase time’); and the time interval till the headache reached its lowest level or disappeared after resuming the recumbent position (T3, ‘the pain decrease time’). These time and pain variables were combined in a PPH profile as can be seen in Figs 2 and 3.

PPH profile for females with a low (□) and high (Δ) body mass index. The profiles reflect median time and pain values based on each patient's median PPH profile.
Patients were considered to be suffering from PPH if they reported a postural headache within a week after lumbar puncture. They were asked to indicate on a 5-point scale how much of the waking day they had to lie down because of headache and/or associated symptoms: practically not (grade 1); less than half the day (grade 2); about half the day (grade 3); more than half the day (grade 4); practically the whole day (grade 5). In addition, on days with PPH the patients were asked to indicate the presence or absence of dizziness, nausea, vomiting, tinnitus and any kind of visual disturbances in the upright and recumbent position. Visual disturbances were infrequently reported, and vomiting was shown to be merely a severe consequence of nausea (4), and only nausea, dizziness and tinnitus in the upright position were analysed in the present investigation. In cases where the data were not filled in correctly and completely, an evaluation was made prior to analysis and only data considered valid were used.
The chi-square test with Yates correction was used for binary variables and the Mann–Whitney U-test was used for continuous variables. Linear and logistic regression analyses were performed with the SPSS statistical package. A P-value of ≤ 0.05 was considered statistically significant.
Results
Sex and age
Eighty-eight of the 239 investigated patients experienced PPH (37%). Table 1 shows that PPH was significantly more prevalent in females than males (46% vs. 21%; P = 0.0003). Also, females with PPH reported grade 5 PPH (64% vs. 23%; P = 0.02) and nausea (74% vs. 39%; P = 0.01) more frequently than males, whereas dizziness and tinnitus were equally prevalent in the two sexes. The median maximal pain in the upright position (VAS2) was scored higher by females than males (60 mm vs. 47.5 mm; P = 0.02), otherwise the PPH profiles were similar. The 20-gauge needle was used with a similar frequency in females and males (44% vs. 41%). Mean age was 39 years in females (range 16–75;
Prevalence of PPH, the severest form of PPH (grade 5 PPH), and associated symptoms in females and males. The results are given in percentage of number of studied patients (n); P-values less than 0.05 are indicated

Needle size
PPH was significantly more prevalent with the use of a 20-gauge compared with a 22-gauge needle in all patients (50% vs. 26%; P = 0.0002) and in females (57% vs. 36%; P = 0.02) and males (38% vs. 10%; P = 0.004), separately (Table 2). Mean age was similar in the studied groups (range 39–43 years;
Prevalence of PPH, the severest form of PPH (grade 5 PPH), and associated symptoms related to needle sizes of 20 and 22 gauge. The results are given separately for females, males and all patients, and shown as percentages of number of studied patients (n); P-values less than 0.05 are indicated

Height
The patients were divided in quartiles according to height, and patients above median height (tall patients) were compared with those below (small patients). Tall and small patients were equally prone to develop PPH both in the total patient group and among females and males, separately. Both age and the frequency of application of the two different needle sizes were similar in the groups. Tinnitus was most frequently reported by the taller patients (44% vs. 24%), especially in females (41% vs. 19%), but these differences were not statistically significant. The occurrence of dizziness and nausea were similar for small and tall patients. No statistically significant differences were observed in the PPH profiles, but there was a tendency towards a shorter median pain delay in taller compared with smaller patients both among males (8 vs. 31 s) and females (14 vs. 70 s; P = 0.08) (Fig. 2).
Body mass index (BMI)
BMI was investigated according to the principles applied for height. Mean low vs. high BMI was 20 vs. 24.1 for females, 21.8 vs. 26.1 for males, and 20.5 vs. 24.9 for all patients. The frequency of PPH, grade 5 PPH and associated symptoms was insignificantly influenced by BMI. However, the PPH profile was different for females with a low and high BMI (Fig. 3). Females with the highest BMI tended to develop PPH more slowly upon rising and to gain pain relief more slowly upon reclining than those with a lower BMI, but only the difference in pain decrease time was statistically significant (60 vs. 12 s; P = 0.02). The PPH profiles for males rested on too few recordings to be analysed statistically.
Onset and duration
In 89% of the patients with PPH, the first onset of headache occurred within 2 days of LP and the median duration of PPH was 6 days. Neither the first onset of the PPH period nor the duration of PPH was significantly influenced by sex, needle size, height, weight or BMI.
Multivariate analyses
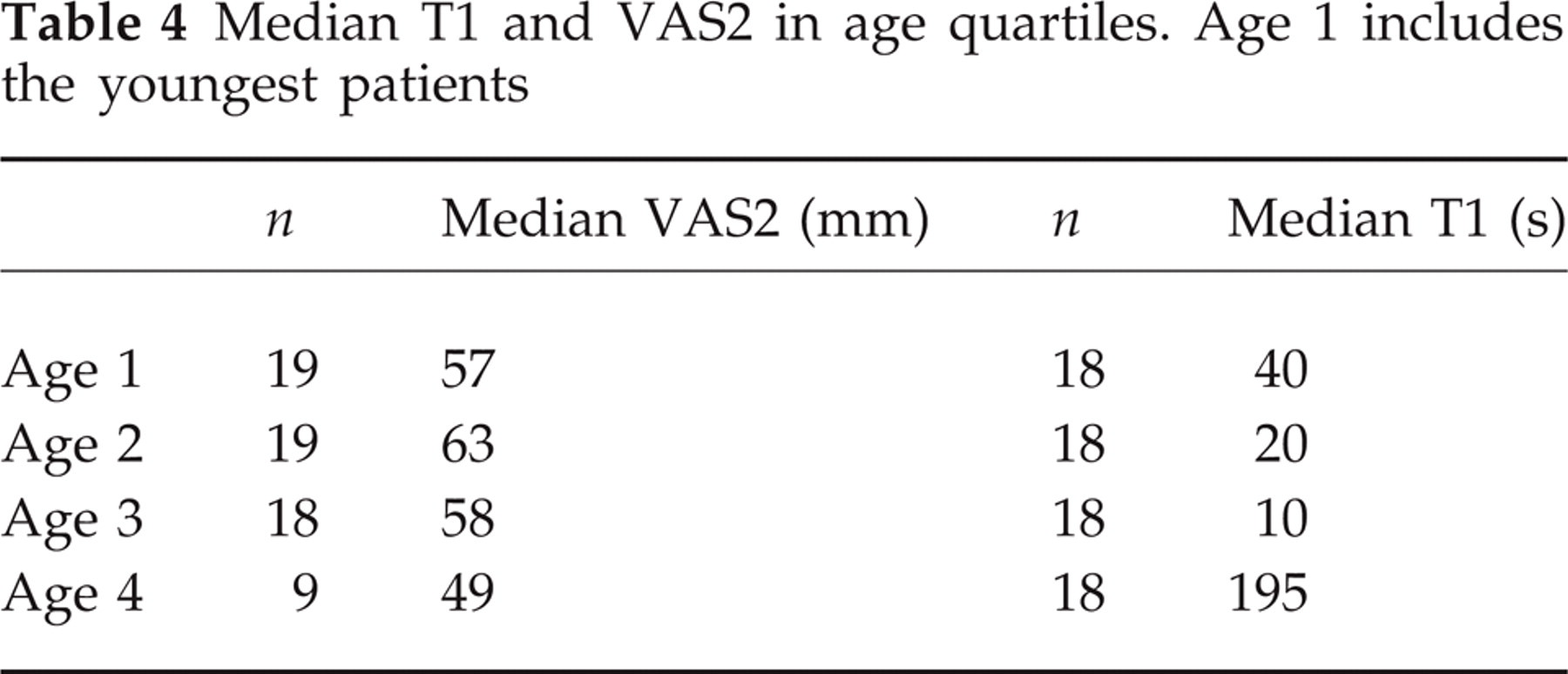
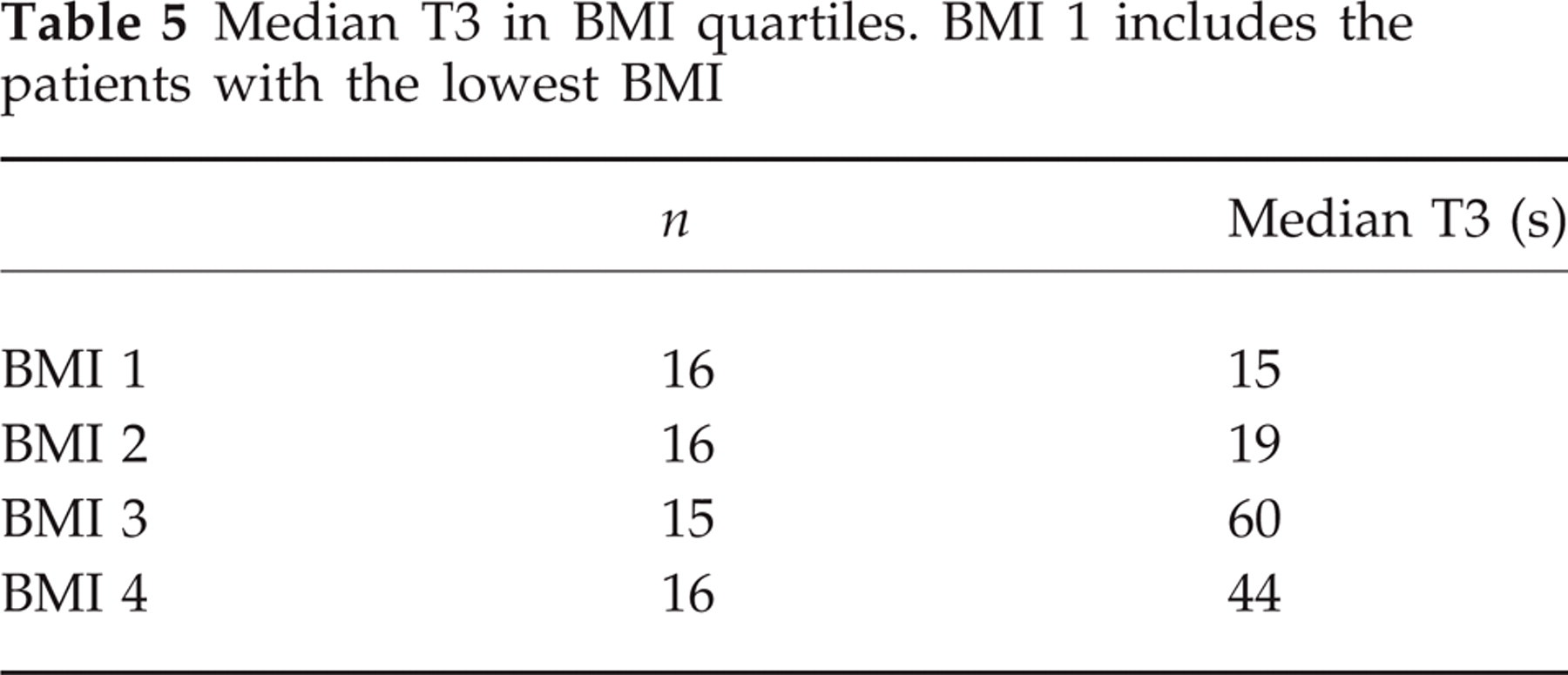
A logistic multiple regression analysis was performed with PPH (yes/no) as the dependent variable. The independent variables were sex, age, height, BMI and needle size. In this analysis, only sex and needle size were significantly related to the outcome. Female sex and the use of the thicker needle increased the risk of developing PPH (Table 3). A linear regression analysis was performed with median VAS2, Log median T1 and Log median T3 as dependent variables and sex, age, height, BMI and needle size as independent variables. The severity of pain in the upright position was positively related to female sex (P = 0.03) and young age (P = 0.03). The pain delay (T1) increased with age (P = 0.008) and the pain decrease time (T3) increased with an increasing BMI (P = 0.04). Tables 4 and 5 show BMI and age distributed in quartiles and related to T1, T3 and VAS2. The main assumptions of the applied multivariate statistical methods (e.g. linearity) were found to be adequately met.
Odds ratio (OD), 95% confidence interval (CI) and P-values for risk factors for PPH. Logistic regression

Median T1 and VAS2 in age quartiles. Age 1 includes the youngest patients
Median T3 in BMI quartiles. BMI 1 includes the patients with the lowest BMI
Discussion
The present study showed that PPH was most prevalent in females (46% vs. 21% in males), which is in accordance with several previous reports (5–10). The present study appears to have an appropriate test power regarding the difference between the sexes. For instance, it may be shown that if the true prevalences of PPH in females and males were 40% and 20%, respectively, the probability of detecting a difference between the sexes would have been 92%. Also, females were more frequently bedridden from their PPH, the headache severity was scored higher and their PPH was more frequently associated with nausea. No plausible explanation has yet been forwarded regarding this difference between the two sexes.
According to the leakage theory (1), PPH might be favoured by a decreased CSF production or an increased leakage of CSF after LP, and factors related to the latter theoretical aspect were investigated in the present study. A previous study showed that a rapid development of headache upon rising – which probably reflects a rapid leakage of CSF – often leads to severe pain (3). Thus, tall persons might be expected to experience PPH more rapidly and severely than smaller persons upon rising, since their CSF pressure at the level of the dural rent should be higher (A in Fig. 1). In the present study, height did not influence the prevalence of PPH, but tall persons developed PPH substantially more rapidly than small persons, although the difference was not statistically significant.
Tinnitus has been shown to exhibit different clinical characteristics compared with other associated symptoms in PPH. In contrast to other associated symptoms, the prevalence of tinnitus seems unrelated to PPH severity, is increasingly prevalent with increasing duration of the PPH period, and its intensity does not decline towards the end of the PPH period (4). Additionally, the present study indicates that tinnitus is most prevalent in tall patients. The aetiology of tinnitus in PPH may be different from the aetiology of other associated symptoms. Tinnitus and hearing loss may according to some authors be caused by a leakage of perilymphatic fluid from the cochlea to the cerebrospinal space through a cochlear aqueduct, which is functionally open in about 50% of adults (11, 12). One might speculate whether a rapid drainage of perilymphatic fluid in tall patients might predispose for tinnitus.
Since a large rent is supposed to leak more rapidly and extensively than smaller rents (B in Fig. 1), the use of a thick needle might cause a higher prevalence of PPH and a shorter pain delay upon rising than a thinner needle. As anticipated, PPH was more prevalent with the use of a 20- compared with a 22-gauge needle in the present study as in previous investigations (8, 13, 14). The pain delay tended to be shorter with the use of the thick compared with the thin needle in the present study, but this difference was not statistically significant.
Also, the resistance to outflow may be dependent on the structure of the fatty epidural connective tissue (C in Fig. 1) and the capacity of the escape route through the intervertebral foramina (D in Fig. 1), which get smaller with age due to osteochondrosis. As expected, the pain delay upon rising increased and the pain was scored less severe with increasing age. The negative correlation between age and PPH prevalence was not confirmed in the present study, but a number of previous studies conclude that PPH is most prevalent in younger persons (5–7, 15), and in particular in young females (16).
Little attention has been paid to the effect of BMI on the frequency of PPH. In one study (17) a high risk of PPH was reported for young females with a low BMI, but this has to our knowledge not been confirmed in other studies. Neither was this relationship seen in the present study, but patients with a low BMI tended to have a short pain delay upon rising and their PPH declined more quickly upon lying down compared with those with a high BMI. It is unclear why the change in pain intensity in response to rising and reclining should be slower in patients with a high BMI. Conjecturally, a high content of fat in the epidural tissue might constrict the subarachnoidal space and thereby prevent a swift flow of CSF in relation to change in body position, but this hypothesis is of course speculative, and this aspect of PPH has not been addressed in previous studies.
In conclusion, our study showed that PPH was more prevalent and seemed to be more severe in females than males. Some of the results were expected according to the leakage theory: the frequency of PPH was higher with the use of a 20- compared with a 22-gauge needle. Also, taller patients tended to record a shorter pain delay upon rising than smaller patients, which was also shown for young compared with old patients. A high BMI disposed for a slow change in pain intensity upon rising and reclining, which may reflect a constricted epidural space.
Footnotes
Acknowledgements
The authors wish to thank (in alphabetical order) Helge Nordal, Ottar Sjaastad and Bodvar Vandvik for their stimulating assistance.