
Abstract
Trigeminovascular activation is involved in the pathophysiology of migraine and cluster headache. The marker evaluated best for trigeminovascular activation is calcitonin gene-related peptide (CGRP) in the cranial circulation. It is unknown whether trigeminovascular activation plays any role in cervicogenic headache (CEH). The objective of this study was to investigate CGRP plasma levels in CEH patients in relation to headache state. To compare plasma CGRP levels between the peripheral and the cranial circulation. Blood from both external jugular veins and from the antecubital vein was drawn from 11 patients with CEH. Plasma CGRP levels were measured by radioimmunoassay. No difference was found between CGRP levels assessed on days with and without headache. There was no difference beween CGRP levels from the symptomatic and the asymptomatic external jugular vein and the antecubital vein. There is no evidence for an activation of the trigeminovascular system in CEH. In certain cases, clinical differentiation between CEH and migraine without aura is difficult. Plasma CGRP levels might serve as a biological marker to distinguish the two headache entities.
Introduction
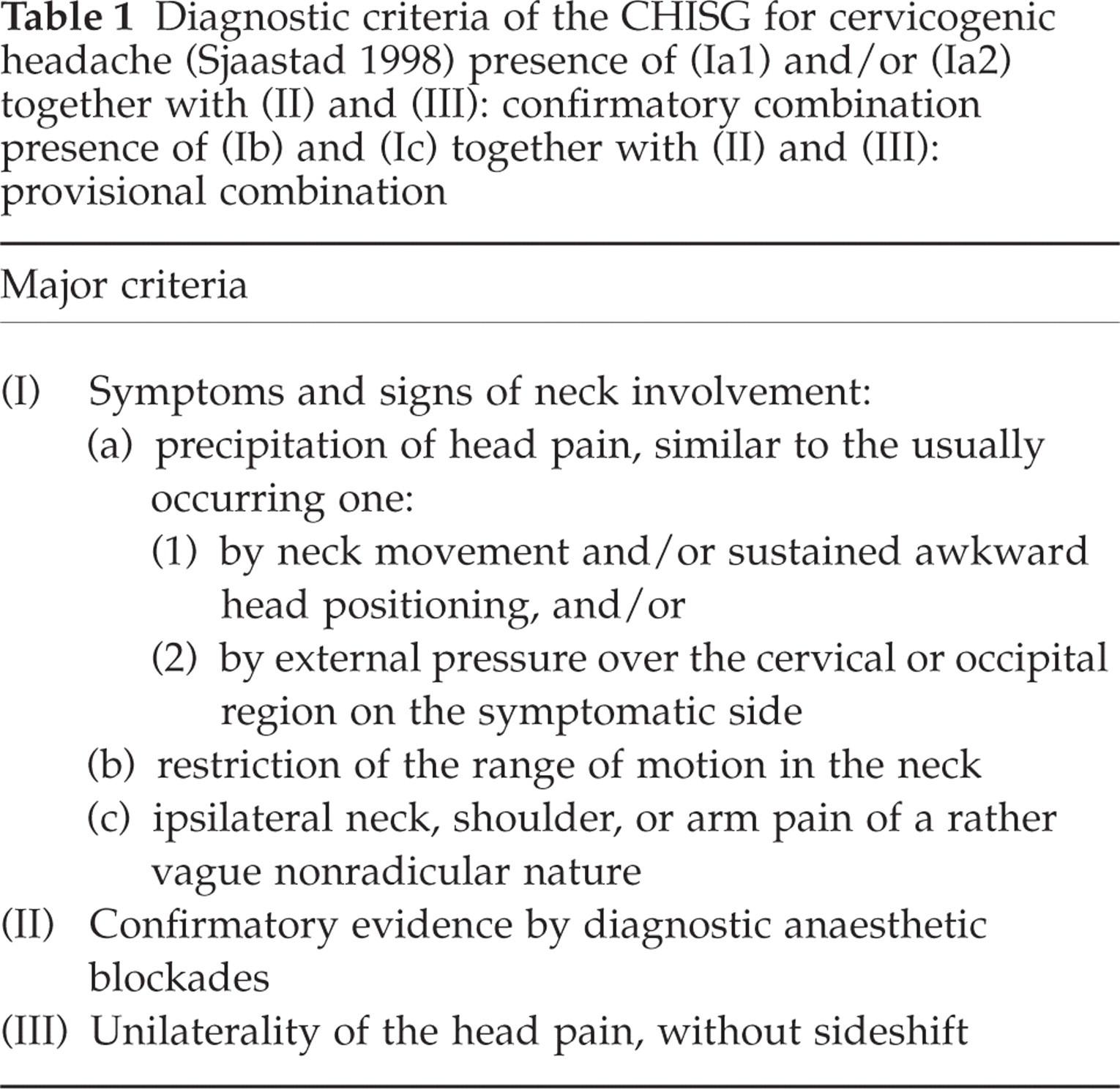
The relationship between the cervical spine and headache has been a matter of debate for decades (1). In 1983 and 1990, the term ‘cervicogenic headache’ (CEH) was defined, based on clinical observations of side constant hemicrania originating from primary sources in the cervical spine (2, 3). The obligatory symptom of CEH is a side-locked unilateral pain that is caused by particular movements of the cervical spine or external pressure applied to the ipsilateral neck or occipital region (2, 3). The current diagnostic criteria for CEH as proposed by The Cervicogenic Headache International Study Group (CHISG) are shown in Table 1 (4). CEH is characterized as a moderate-severe, nonthrobbing, and nonlancinating pain usually starting in the neck. There are episodes of varing duration or a fluctuating, continuous pain (4). Various anatomical structures innervated by the upper three cervical nerves have been shown to be potential sources of the headache (5). The physiological basis for this ‘referred pain’ is convergence between trigeminal afferents and afferents from the upper three cervical nerves (5, 6). Trigeminocervical convergence has early been demonstrated (7). Recent neurophysiological research in rats has disclosed the interaction of cervical and trigeminal input in accurate detail and this underlines its clinical relevance (8, 9).
Diagnostic criteria of the CHISG for cervicogenic headache (Sjaastad 1998) presence of (Ia1) and/or (Ia2) together with (II) and (III): confirmatory combination presence of (Ib) and (Ic) together with (II) and (III): provisional combination
During stimulation of the trigeminal ganglion, and during spontaneous attacks of migraine and cluster headache, there is a release of neuropeptides such as calcitonin gene-related peptide (CGRP) and neurokinin A from trigeminal sensory nerve endings into the cerebral circulation (10–13). The connections of the trigeminal system with the cranial vessels have led to the concept of the ‘trigeminovascular system’ being a crucial functional network involved in the pathophysiology of primary headache disorders (14, 15). Whether or not an activation of the trigeminovascular system via trigeminocervical convergence as a ‘final common pathway’ plays a role in the pathophysiology of CEH is an open question (16, 17). We investigated levels of CGRP in the external jugular vein (EJV) of CEH patients as the most intensively investigated marker for an activation of the trigeminovascular system.
Methods
Patients
Data were collected from 11 patients suffering from CEH according to the CHISG diagnostic criteria (4)(Table 1). Only patients with all symptoms and signs of neck involvement (Ia + Ib + Ic), a positive blockade of the greater occipital nerve (pain intensity ≤ 1 on a visual anlogue scale (VAS 0–10) 30 min after blockade), and unilaterality without sideshift were included. Exclusion criteria were a history of migraine or any other type of primary headache, and an intake of analgesics during the last 24 h prior to the examination. Ten patients were examined on two days: examination 1 with a typical episode of CEH and examination 2 without headache. One patient with a chronic CEH could be examined with headache only. On days with headache, the headache had been present for at least three hours. On days without headache, the patients had been headache-free for at least 24 h spontaneously or after manual therapy. The study protocol was approved by the local ethics committee of the University of Münster. All patients gave written informed consent following a detailed explanation of the procedure.
Procedures
The blood samples were taken between 1000h and 1600h Patients were rested supine, and a small ‘butterfly’-cannula was inserted into the ipsilateral and the contralateral external jugular vein and the anticubital vein on the nondominant side. Blood (9 ml) was collected into tubes prepared with 15% ethylenediaminetetraacetate and immediately decanted into cooled tubes prepared with aprotinin (Trasylol, 500 μl, Bayer, Leverkusen, Germany). The tubes were transported on ice and centrifuged at 2000 g for 15 min. Plasma for CGRP was aliquoted into polypropylene tubes for storage at −80°C until analysis. Samples were coded and all determinations were performed blinded.
Radioimmunosassay
Plasma CGRP concentrations were measured with a fully evaluated radioimmunoassay for human CGRP, as described previously (18). In brief, human α-CGRP was obtained from Peninsula Laboratories Europe (St. Helens, UK). Standards were prepared in 0.1 mol/l phosphate buffer (pH 7.5) containing 0.1% bovine serum albumin, 0.01% sodium azide, and 20 kIU/ml aprotinin (Trasylol). The tracer was prepared by iodination of [Tyr0]α-CGRP25−37 (Multiple Peptide Systems, San Diago, CA, USA) using the IodoGen method (Pierce, Rockford, IL, USA) and purified by high-performance liquid chromatography on a Merck-Hitachi system (E. Merck, Darmstadt, Germany). The antibody used was raised in rabbits against human α-CGRP and is specific for the C-terminal segment of CGRP. It was used in a final diluation of 1 : 600 000. The assay was performed at 4°C as a nonequilibrium assay incubating sample (100 μl) and antibody (200 μl) for 4 days prior to 2 days of incubation with tracer. Free and antibody-bound tracer were separated using a solid-phase separation system (SAC-CEL; IDS, Boldon, UK). The detection limit of the assay was 5 pmol/l. The intra-assay coefficient of variation was 2%, and the interassay coefficient of variation was 7%. The nonspecific binding was 3% to 4%.
Statistics
Results are presented as means ± SEM. For comparing CGRP-values, the nonparametric Wilcoxon-test was used. To test associations between variables, Spearman-rho correlation coefficient was used. All statistical analysis were performed using SPSS version 11.0 (SPSS, Chicago, IL, USA). The level of significance was set at P = 0.05.
Results
The mean age at examination was 35.7 (± 14.6) years. Two patients were men and nine were women. The mean history of CEH lasted for 6.7 (± 8.4) years. Ten patients suffered from episodic CEH, one from chronic CEH. In patients with episodic CEH, the pain had started 12.6 (± 9.6) hours before examination 1. On examination 1, mean pain intensity was 4.9 (± 1.2) on a visual anlogue scale (VAS 0–10). Quality of pain was sharp in five patients and dull in six patients. No patient had signs of autonomic activation (e.g. ptosis, lacrimation). The mean interval between examination 1 and examination 2 was 27.2 (± 21.5) days. On examination 2, patients were free of pain for 5.6 (± 2.5) days.
The concentration of CGRP was above the detection limit in all blood samples. There were no missing values. There was no significant difference between CGRP levels on days with headache and on days without headache (Fig. 1). For both time points, there were no significant differences between CGRP levels from the EJV of the symptomatic side, from the EJV of the asymptomatic side, and from the cubital vein (for all comparisons P > 0.1). On days with headache, there were no significant correlations between CGRP levels from the EJV of the symptomatic side and the age of patients, the duration of pain, and the intensity of pain (for all P > 0.6).

Mean CGRP levels (pmol/l) with and without pain.□ symptomatic EJV 35.2 ± 17 and 36.3 ± 13; asymptomatic EJV 34.0 ± 15 and 33.8 ± 12; ▪ cubital vein 35.5 ± 15.7 and 34.4 ± 12 (for all comparsisons P > 0.1).
Discussion
During the past 15 years, there has been a strong interest in the role of neuropeptides in primary headache disorders. CGRP is the most potent vasodilator peptide in the trigeminovascular system (19). Increased plasma CGRP levels have been detected in the cranial circulation (EJV of the symptomatic side) but not in the peripheral circulation during attacks of migraine and cluster headache (11, 12). A normalization of CGRP levels in the cranial circulation after successful treatment of migraine and cluster headache attacks with sumatriptan has been shown (12, 14).
In contrast, CGRP levels in the cranial circulation of CEH patients in our study were unaltered. A sample of at least 10 patients would provide 80% power to detect an effect size of 1.4 regarding the CGRP level. Previous studies in headaches with an activiation of the trigeminovascular system found an increase of at least 50% of CGRP levels during the pain (11, 12, 14). Therefore, our sample size of 11 subjects would have been able to detect an expected effect size of 1.5 with sufficient power.
To the best of our knowledge, this is the first study on neuropeptide changes in CEH in humans. In former animal studies, a stimulation of the greater occipital nerve as an important cervical afferent had caused a decrease of CGRP levels in the jugular blood (20). In summary, there is no evidence for a trigeminovascular activation in the origin or intensification of CEH. The results thus explain the lack of effect of sumatriptan which has been described as a characteristic of CEH (4).
Since its first systematic description in 1983 (2), there has been an extended controversy about the existence of CEH as a distinct headache entity (1, 21, 22). The International Association for the study of pain (23) gives various general descriptions of possible manifestations of CEH without providing clearcut diagnostic criteria. In its recently published second edition of The International Classification of Headache Disorders, the International Headache Society (IHS) also accepts the term ‘CEH’. Nevertheless, in these criteria, sufficient reliability and validity of clinical signs that implicate a source of pain in the neck are denied and evidence that the pain can be attributed to a neck disorder or lesion can be demonstrated only by a positive blockade (24). Our patients fulfilled the IHS criteria for CEH. However, since we additionally wanted to rely on precise clinical criteria, we used the CHISG criteria which provide operational clinical criteria for symptoms and signs of neck involvement which have been validated (Table 1) (25–28). From the clinical point of view, CEH is one of the most difficult differential diagnoses for migraine without aura due to a significant overlap of diagnostic criteria (4, 29, 30). However, exact application of the CHISG diagnostic criteria characterizes a headache entity biologically distinct from migraine. From the pathophysiological point of view, our study clearly demonstrates that CEH is not just a migraine variant because trigeminovascular activation is absent in CEH. Apparently, CGRP plasma levels from the cerebral circulation might serve as a useful biological marker to differentiate both headache entities.
Footnotes
Acknowledgements
The expert technical assistance of Alice Rudboel (Copenhagen) and Richard Holtmeier (Münster) is gratefully acknowledged. The investigation of cervicogenic headache at the University of Münster was supported by a grant of the Bertelsmann Stiftung, Gütersloh, Germany.