
Abstract
The objectives were to introduce a new method for controlled trials of acupuncture in the field of headache research and to examine the role of needling per se. Women with menstrually related migraine were randomized to three months of treatment with verum or placebo needles. Three standard size casts were moulded to secure the placebo needles in the head. No significant differences were found between the verum group (n = 15) and the placebo group (n = 13) during treatment or follow up three and six months later, either in the attack frequency or in the number of days per month with migraine, headache intensity or drug-use. The casts held the needles exactly in place despite movements of the head, and are validated as practical, hygienic and extremely durable. This method is satisfactory for controlled studies of acupuncture in headache. It is possible that the positive results in earlier clinical trials on acupuncture in migraine are attributable to other mechanisms than needling of subcutaneous tissue.
Introduction
Migraine is a common reason for acupuncture (1, 2). When reviewing the scientific basis for this, it is impressive to find positive results in all published reports. There are a few carefully designed studies of high quality where the effect of standard acupuncture has been compared with that of sham acupuncture (3) or prophylactic pharmacotherapy (4, 5), respectively. However, most studies do not live up to the standards of good clinical trial practice. The vast majority have fundamental methodological shortcomings, such as absence of appropriate control group and not using generally accepted diagnostic criteria. In a Cochrane review, it is concluded that acupuncture is effective and plays a role in the treatment of headache. Meta-analysis of specific outcome data in migraine is not possible owing to heterogeneity and insufficient reporting (6, 7). Acupuncture may be a choice for patients in need of prevention, when pharmacological prophylaxis is not suitable. The mechanisms underlying a positive effect of acupuncture in migraine have not been sought.
Clinical acupuncture research is complicated for several reasons, of which the placebo issue is the most intriguing (8–11). The placebo effect is considerable for any migraine treatment, and is probably greater for specialized and time-consuming therapies. Furthermore, sufferers are prone to begin treatment in a severe phase, from which spontaneous improvement can be expected. The American Headache Society (AHS) stresses the need for developing new methods for controlled studies of acupuncture in headache (12). Penetration of the skin is commonly thought of as the single most important mechanism. From a methodological point of view, false needles therefore seems to be the most appropriate choice of control at hand because it has the same credibility as true acupuncture but with weaker afferent stimulus than sham acupuncture. A blunted, telescopic placebo needle (13) fulfils these criteria and is regarded as a major advance in acupuncture research (14). The predictable recurrence of menstrually related migraine (MRM) allows for prophylactic therapy in short perimenstrual courses, which is why therapists commonly recommend acupuncture to women with MRM.
The main objective of this study was to investigate the role of the invasion of the needles per se in acupuncture as prophylaxis against MRM, taking into account experience from an open pilot study (15). A secondary aim was to introduce a practical, robust method for using the placebo needles in the head.
Materials and methods
Design
This is a prospective, randomized, single-blind, placebo controlled, parallell group study. Consensus guidelines for clinical trials in menstrual migraine (16, 17) and acupuncture (2, 7, 9, 11, 14, 18, 19) have been followed. The project was approved by the Ethics Committee at Göteborg University. Informed, written consent was obtained. Participants did not pay the customary fee for treatment.
Subjects
Forty-six female patients were consecutively enrolled at a specialist clinic. A diagnosis of migraine according to the criteria of the International Headache Society (IHS) (20) was confirmed by a neurologist.
Inclusion criteria were: age above 20 years, acupuncture-naïve, regular menstrual periods, a history of self-considered menstrual migraine of at least one year, effective contraception and no plan to become pregnant or change hormonal treatment during the study. Exclusion criteria were: Migraine prophylaxis or cycle-modulating hormonal drugs during the last 3 months, lack of time and/or motivation to participate, severe illness, bleeding disorder or anticoagulation, lack of effective acute treatment for migraine, overuse of analgesics and/or migraine-specific acute drugs (>10 days/month), ‘interval-headache’ > 6 days per month, difficulties in differentiating migraine from other headaches.
A relation between migraines and menstrual cycle was prospectively documented in diaries (17, 21). The criteria for MRM used were debut of attacks on the first day (± 2 days) of bleeding ± debut of attacks on the estimated day of ovulation ± occasional attacks at other times (≤ 10% of total). Thirty-one (n = 31) eligible subjects were randomized to either customary (verum) or placebo needles according to a method of lottery. Twenty-eight (n = 28) persons finished treatment and are included in the results.
The mean ages at initial visit for participants included in the results were 35.2 (± 7.5) years in the verum group and 37.4 (± 8.6) years in the placebo group. All had migraine without aura. In the verum group five (n = 5) patients had additional attacks with aura. The two groups are comparable in all other respects.
Three subjects (n = 3) did not complete treatment and were excluded. A further five patients (n = 5) did not complete the whole period of follow up. The reasons for drop-out/withdrawal (number, group/point of time given within parenthesis) were new oestrogen treatment (n = 4, verum/T2, verum/T3, placebo/T1b, placebo/T2), lack of time (n = 2, both verum/T1a), health problem (n = 1, verum T1a), discomfort (n = 1, verum T1a), pregnancy (n = 1, verum T3) and lack of motivation (n = 1, verum T3).
Experimental protocol
To confirm the study criteria for MRM prospectively, a baseline-registration (T0) was undertaken for a minimum of 2 months (in unclear cases 3–4 months) before treatment. The participants were instructed to keep diaries in which they entered days of migraine, drug use (doses, not type), average migraine pain on a 10-point visual analogue scale (VAS) and days of menstruation. Completed diaries were sent to the secretary. The period of treatment (T1a) lasted for three months (menstrual cycles). Needling was administered on the 8:th, 5:th and 3:rd days (±1 day accepted) before the estimated first day of menstruation, making a total of 9 sessions. Patients were regularly encouraged to continue keeping diaries. Long-term follow up (one month diary at each assessment point) was done twice, at three (T2) and six (T3) months after treatment. No restriction was placed on the use of concomitant acute medication, since it is considered unethical (17).
Procedures
Acupuncture was performed by the same experienced physiotherapist (AF) with an equally experienced stand-in (JC) when needed. Sessions were scheduled exclusively between 1500h and 2000h (22, 23). All patients were treated identically, and great emphasis was on the acupuncturist not behaving more or less enthusiastically. They were instructed not to discuss the needling technique or the effect, but side-effects were reported directly to and documented by the acupuncturist.
The following insertion points (Fig. 1) were used in all patients: GB8 (above apex of ear), GB20 (medial to mastoid process) locally along with LI4 (first dorsal interosseus of upper limbs), Liv3 = LR3 (first dorsal interosseus of lower limbs) and SP6 (above medial malleolus) peripherally. Depending on the site of usual maximum headache, one of GB14 (above middle of eye-brow, frontal pain), Taiyang = Extra 2 (between eye-brow and external canthus, temporal pain) or Bl10 = UB10 (insertion of trapezius at external protuberantia occipitalis, occipital pain) was chosen. The exact localization of these acupoints (used bilaterally) is described in textbooks (24, 25). An intial stimulation was given at insertion. Needles (n = 12) were left in situ for 30 min and rotated manually every 10 min.

Location of acupoints used (all bilaterally) and their relation to the traditional meridians.
Sterile Chinese disposable filiform needles (Huato®, dimensions 15 × 0.25 mm or 30 × 0.30 mm) were used in the verum group. The depth of insertion varied between 10 and 30 mm depending on location. Blunt placebo needles that touch but do not penetrate the skin (13) were purchased from the inventor. This control method was elaborated further with a cap for the head to fix the necessary plasters over acupoints richly covered with hair. Verum-needles, too, were inserted through these plaster holders. All participants were asked:
Do you feel the needle?
Do you feel anything when I rotate it?
How does it feel?
Verum needles were stimulated until the ‘de qi’ sensation was achieved, and stimulation of placebo needles was done for a corresponding amount of time.
Statistical approach
The analysis was conducted by a blinded investigator. The primary measure (frequency) was number of attacks per month. Secondary measures were days with migraine per month, mean headache intensity and amount of headache medication used (total sum of injections, tablets, nasal sprays and suppositories). Changes in all parameters as compared with the run-in period (T0) were calculated for the complete treatment period (T1a), last month of treatment (T1b, attack frequency only), three months (T2) and six months (T3) after treatment. For patients (n = 5, 18%) withdrawn during the period of follow up at three (n = 2) or six (n = 3) months after treatment, the last usable result was carried forward. Mann–Whitney's U-test for unpaired samples was used to compare the change from baseline in each parameter. Significance levels were set at 0.05. All analyses were performed using the Statistical Package for Social Sciences (SPSS) software program (version 11.0 for MacOSX, SPSS, Inc., Chicago, USA).
Results
All mean results are shown in Table 1. At no point in time did the change in any of the measured parameters differ significantly between groups. Boxplots of changes in the primary end-point (attack frequency) are shown in Fig. 2. By the last month of treatment (T1b) more individuals (n = 3, 23%) in the placebo group than in the verum group (n = 2, 13%) documented a significant (≥50%) reduction of attack frequency. During follow up, a large variation was seen for attack frequency in the verum group.

Change in attack frequency at different assessment points in the verum (shaded boxes) and placebo (unfilled boxes). Plots give the interquartile range (boxes), median (line within boxes), the highest and lowest values excluding outliers and extreme values (whiskers), ○ outliers, e extreme values.
Baseline recordings and follow-up results within the groups

An absolute majority of all participants (n = 21, 75%) decreased concomitant use of symptomatic medication during T1a. At T2 and T3, 50% had decreased and 50% had increased medication.
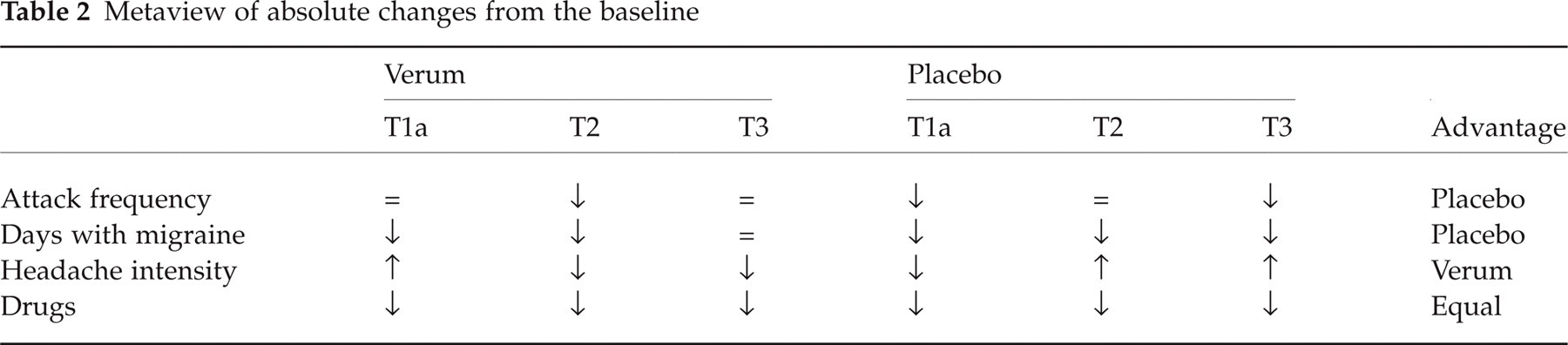
An overview of the ‘signs’ (positive, negative or no difference) for absolute changes in all measured parameters at the three points of time (Table 2) reveals no consistent difference between the two treatment groups (verum > placebo = 4, ties = 5, verum < placebo = 3).
Metaview of absolute changes from the baseline
The total number of side-effects reported was six in the verum group and three in the placebo group. These were bleeding at acupoint (one major in the verum group and one minor in the placebo group), subcutaneous haematoma (two in the verum group and one in the placebo group), tenderness at acupoint (one in each group), facial and cervical blush (n = 1, verum group) and vertigo (n = 1, verum group).
Discussion
It is not necessary to explain why a treatment is effective to approve of it in clinical practice. But it is due to successful mechanistical research that acupuncture has gained acceptance in medical science (2). Our findings suggest that the positive effect of acupuncture in migraine may not be owing to perforation of the tissues per se and are in line with an earlier study in tension-type headache (26). It cannot be concluded that placebo needles have an effect equivalent to true acupuncture, but it is the authors’ opinion that if there were a clinically relevant difference, it would have been revealed.
Since there was no knowledge of what variability of results could be expected, the required number of participants to achieve adequate power could not be calculated beforehand (11, 27). A sample size (n = 30) that could be managed (during weekdays between 3 and 8 pm) by one therapist for 18 months was chosen. This is in the same range as previous studies on treatment of MRM (median n = 20, 28), and acupuncture in migraine (median n = 40, 7). The major reason for withdrawal was that the subjects began using oral contraceptives (29, 30). The rationale for withdrawing pregnant women was the probable migraine-prophylactic effect of pregnancy.
It is impossible to have genuine double-blinding, since the therapist must have control of the patient's perception of the needles (10, 11, 31). A reasonable alternative is to randomize patients to one of two blinded therapies in combination with a blinded evaluator, which is sometimes referred to as ‘double-blind’ approach despite the unmasked therapist (2, 9–11, 13, 26, 32, 33). The choice of control is contingent on the objectives. Sham acupuncture has too many drawbacks (5, 9–11, 13, 31, 32). A better possibility – if the aim is to find a theraputic effect – is to use an active comparator, although divergent effects of expectation constitute a potential pitfall.
It is commonly maintained that the real acupoints are located subcutaneously, and there is support from human and animal studies for the idea that deep needling has certain neurophysiological effects, independent of cutaneous afferent impulses. Since the objective was to investigate whether the perforation with needles per se is clinically important, it was crucial to choose a nonpenetrating comparator indistinguishable from true needles but exerting an identical psychological impact. The placebo needle is a step in the right direction and the closest one can come to a ‘golden standard’ today (2, 8, 9, 13, 14, 34).
During the course of our study participants were not systematically asked if they could tell which treatment they received, since it was an important part of our research protocol to avoid discussions on the method of intervention during the period of treatment and for the whole 6 months period of follow up. After closing of the study, we have talked to the patients at different times – and no one could tell us which type of stimulation they had been given. One woman who withdrew (‘lack of motivation’) from follow up after verum treatment thought she had been given placebo. In Konrad Streitbergers original publication on the placebo needle, none of the participants (n = 60) suspected that the skin had not been punctured. The differences in the VAS rating between the two needles were too small to reveal which was the placebo (13). White et al. (35) recently reported a single-blind, randomized (n = 37), cross-over study on the validity of the ‘Streitberger’ needle. Intervention consisted of either 2 weeks of treatment with real acupuncture followed by 2 weeks on placebo, or vice versa. The primary outcome was a needle sensation questionnaire. No significant differences between groups or needle types were found for any of the sensations measured. Most patients were unable to discriminate between the needles by penetration, and no major differences in outcome between real and placebo needling could be found.
A problem has been that the plasters fixing the needles are impossible to fasten in thick hair covering cranial acupoints. One possibility is to use pieces of elastic foam (26), but our prototypes of needle-holders based on glue in the capillary matrix were abandoned either because they did not stay in place or because they triggered a strong afferent stimulus when removed. Instead, we moulded casts of durable plastic in alternative sizes (small, medium, large) and with a flexible strap for attachment. They secured needles in an exact place despite head movements and were practical, hygienic and extremely durable throughout the study.
There is no scientific evidence concerning how the needling should be administered and dosed. The custom of inserting needles in somatic segments corresponding to the pain and in addition to that distally is considered essential. Acupoints (Fig. 1) were selected by taking into account previous studies, recommendations in generally accepted manuals and personal advice from the University of Traditional Chinese Medicine in Shanghai. The classic ‘migraine points’ were included (2, 9, 24, 25, 36–38). A certain degree of standardization was necessary and does not violate traditional recommendations. Nine acupuncture sessions is common, and studies on migraine prophylaxis should be no shorter than three months (17).
Diagnostic groups in acupuncture studies should be homogenous, based on clear-cut criteria (9, 10). Although 60–70% of female migraineurs relate their headaches to the menstrual cycle, it cannot be categorically concluded that the results of this study are generalizable to all migraine. The scientific advantage of MRM is that the predictable temporal profile offers the possibility of studying effects of prophylaxis administered in a limited phase where the pathogenetic mechanisms are likely to be specific (16, 17, 21). There are no agreed definitions for terms such as ‘menstrual migraine’ and MRM, and there is little support for the idea that they constitute unique headache entities (20, 21, 28, 39–44). The time intervals and other restrictions used vary enormously (21, 45). Consistent ovulatory attacks tend to be reported, and this is compatible with the theory of oestrogen withdrawal being a trigger factor (39, 46, 47). We therefore decided not to exclude women with additional mid-cyclic attacks. No previous study has investigated the assertion that MRM is particularly responsive to acupuncture. Regarding other nonpharmacological treatment of MRM, the literature contains contradictory findings (29, 30, 45, 48).
In summary, we find it possible that effects of acupuncture in migraine are attributable to other mechanisms than perforation of subcutaneous tissue. Repetitive relaxation and being cared for may be just as important. From an ethical point of view it was intriguing to find that some patients were disappointed to find that the needles they considered effective were later revealed as ‘false’. After completion of the study we could only offer conventional acupuncture, but those who accepted (n = 2) perceived it as being too painful. Most participants’ drug use was reduced, often despite deterioration of their migraine, which suggests psychological mechanisms. The acupuncture therapeutic setting fulfils most criteria described for placebo effects, but it may be argued that this could be utilized in for example drug-detoxification (8, 9, 13, 31, 34). Many patients appreciate and prefer ‘low-tech-high-touch’ medicine, not because they reject drugs as is often thought, but because it is considered to activate endogenous, positive mechanisms, and because it offers ‘empowerment’– an opportunity to interact and influence the recovery.
Footnotes
Acknowledgements
We would like to thank Elisabet Stener-Victorin, RPT, PhD, and Christina Carlsson, RPT, for their valuable comments on the design of the study, Karin Drottz, ROT, MSc, for her assistance in constructing the needle holder and Martin Gellerstedt for his skilful help with statistical analysis. The placebo needle is an invention of Konrad Streitberger, MD. The study has received grants from Astrazeneca, Glaxo Smith Kline and Renee Eanders foundation.