
Abstract
The aim was to investigate the lifetime prevalence of headache and primary headache (diagnoses according to International Headache Society criteria) in multiple sclerosis (MS). The relationships between headache and clinical features of MS and MS therapy were also investigated. We studied 137 patients with clinically definite MS; 88 reported headache, 21 of whom developed headache after the initiation of interferon. The prevalence of all headaches in the remaining 116 patients was 57.7%. Migraine was found in 25.0%, tension-type headache in 31.9%, and cluster headache in one patient. A significant correlation (P = 0.007, Fisher's exact test) between migraine and relapsing-remitting MS was found. Primary headaches are common in MS patients. Further studies are needed to clarify the mechanisms underlying this association, particularly the association between migraine and relapsing-remitting MS, and the role of interferon in the development of new headache.
Introduction
The relationship between multiple sclerosis (MS) and headache is poorly understood. Headache is not generally considered a symptom of MS and studies investigating the relationship between the two conditions have produced conflicting results (Table 1). Thus, the lifetime prevalence of headache in MS patients is reported at between 4% and 58%(1–8) and the frequency of headache as an MS onset symptom is reported at between 1.6 and 26% (1, 2, 4, 6, 7, 9–11). Attention has been drawn recently to de novo headache and exacerbation of pre-existing headache in interferon-treated MS patients (8, 12).
Summary of results of studies of the relation between headache and multiple sclerosis (MS)

The primary aim of the study was to investigate the association between MS and headache. We estimated the lifetime prevalence of primary headaches in a clinical sample of MS patients, using a questionnaire based on International Headache Society (IHS) recommendations (13), in order to facilitate classification of different headache types. The secondary aim of the study was to evaluate the correlation between headache in general and different types of primary headache, and the clinical features of MS (illness duration, disability and clinical form). The onset of a new headache after initiation of MS chronic treatment was also evaluated.
Patients and methods
We prospectively recruited all patients presenting at the MS out-patient clinic of the C. Besta National Neurological Institute, Milan, between May and December 2001, in whom clinically definite MS (14) had been diagnosed.
The patients underwent a semistructured interview guided by an ad hoc questionnaire. The questionnaire sought information on lifetime occurrence of headache, frequency of attacks, location of pain, quality and severity of pain, duration of attacks, aggravation by movement and routine physical activity, and presence of autonomic symptoms. Patients were asked to recall the above-mentioned features referring to their usual headaches. This information was sufficient to diagnose headache type according to IHS criteria (13).
MS was diagnosed according to McDonald and Halliday (14) and was classified as relapsing–remitting, primary or secondary progressive according to Kalman & Lublin (15). Functional disability was scored using the expanded disability status scale (EDSS) (16). The patients were dichotomized as follows for the purposes of the statistical analysis: relapsing–remitting vs. progressive forms; EDSS score ≥ 3.5 vs. EDSS < 3.5; and illness duration ≥ 10 years vs. < 10 years. The χ2 test (or Fisher's exact test when one of the samples contained fewer than five subjects) was used to assess the significance of differences. We also collected information on headache onset in relation to MS onset, and on headache onset in relation to use of medication for MS.
Results
A total of 137 patients (95 females and 42 males) were recruited. Mean age was 40.6 years (SD 11.6, range 19–73); mean duration of MS was 13.4 years (SD 9.4, range 1–46). The relapsing–remitting form was present in 102 patients (74.5%) and the progressive form in 35 (25.5%): primary progressive MS in one patient, secondary progressive MS in the remaining 34. The mean EDSS score was 3.4 (range 0–8.5). Sixty-four patients were on long-term anti-MS medication: 51 were receiving interferon, nine azathioprine, and four copolymer. Eighty-eight of the 137 (64.2%) patients reported headache.
Among the 64 patients on long-term anti-MS medication, 21 developed headache only after the initiation of therapy; all were being treated with interferon. Headache was present in 21/51 (41%) of all patients using interferon (nine males, 12 females, mean age 36.9 years, SD 11.3); 10 of these (48%) had migraine (migraine without aura in six, migrainous disorder not fulfilling all the diagnostic criteria in four) and 11 (52%) had tension-type headache.
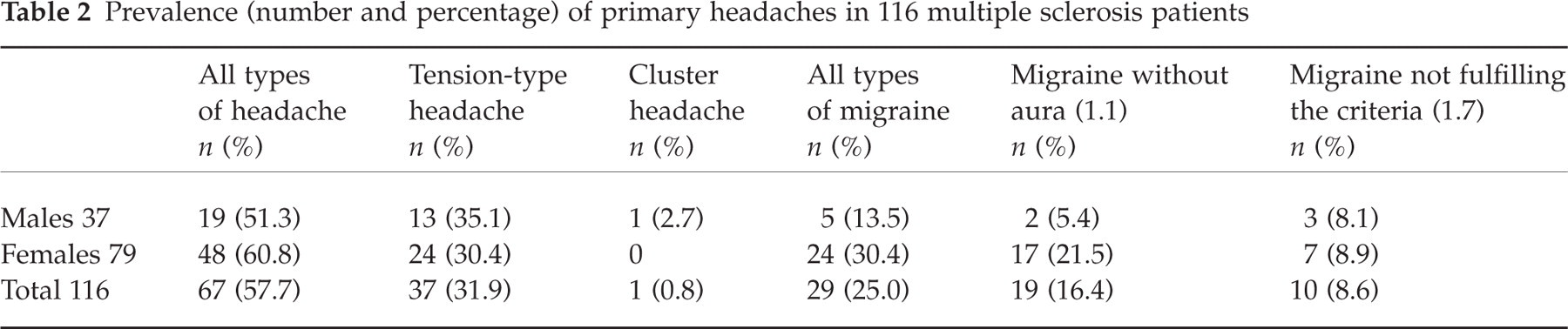
The lifetime prevalence of all types of headache according to IHS criteria, and correlations between headache and MS clinical features, were assessed in the 116 patients (32 males, 84 females, mean age 41.3 years, SD 11.5) remaining after excluding those in whom headache began only after the initiation of interferon. Sixty-seven (57.7%) of these patients suffered from headache (Table 2). Twenty-nine patients (25.0%) had migraine, 37 (31.9%) had tension-type headache, and one (0.8%) had cluster headache. Most migraine patients (19/29) had the form without aura; 10/29 were diagnosed with migrainous disorder not fulfilling all the diagnostic criteria; no cases of migraine with aura were diagnosed. Migraine (without aura) was more prevalent in female patients than in males. The prevalence of tension-type headache did not differ between the sexes. The single patient with cluster headache was male (Table 2).
Prevalence (number and percentage) of primary headaches in 116 multiple sclerosis patients
Correlations between headache in general, different primary headaches, and the main clinical features of MS are shown in Table 3. The prevalence of headache in general was not related to MS form, illness duration or disability score. Migraine was more frequent in patients with relapsing–remitting MS, while tension-type headache was more frequent in patients with the progressive form (P < 0.001).
Correlations between headache in general, and different primary headaches, and clinical features of multiple sclerosis (MS) patients
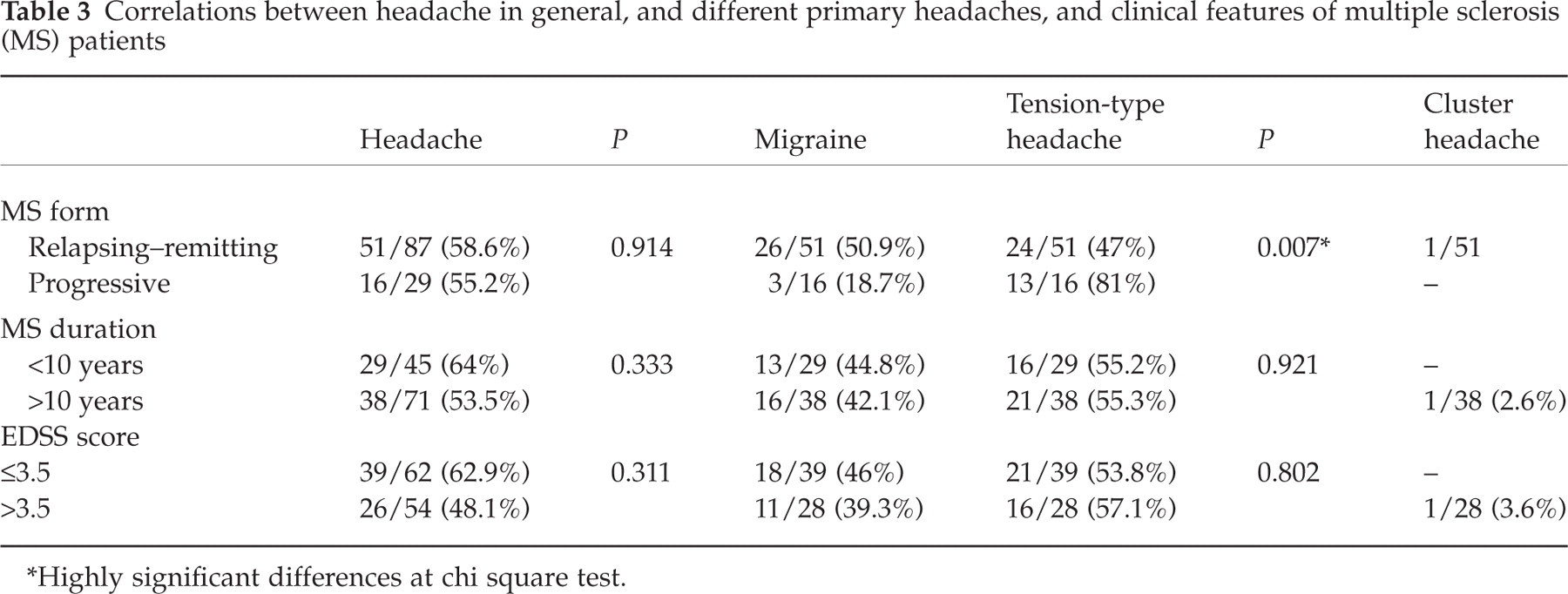
∗Highly significant differences at chi square test.
Two patients reported headache as a presenting symptom of MS, and in both cases the diagnosis was migraine.
Discussion
Our survey indicates that headache is common in patients with clinically definite MS (14). Considering only patients in whom headache onset was unrelated to anti-MS treatment, the prevalence of headache was 57.7%– a higher proportion than reported by most studies of the relationship between headache and MS, in particular, higher than all figures reported in studies published between 1950 and 1989 (1–6), but consistent with two recent studies (7, 8) in which the occurrence of different types of primary headaches was also investigated (Table 1). In the first of these recent studies (7) the obsolete categories of ‘vascular headache of the migraine type’ and ‘muscle contraction headache’ (17) were used; however, these are reasonably close to the migraine and tension-type categories we used. The proportions of these two primary headaches were similar to those of our study.
The second study (8) was the only one in which IHS criteria (13) were used. Although its primary aim was to determine the association between drug treatment for MS and headache, the prevalence of different headache forms before treatment was also assessed. The prevalence of pre-existing migraine in this study was higher than in our study, while the prevalence of tension-type headache was surprisingly low. As in our study, among migraine subtypes the commonest form was migraine without aura.
In our series, those with and without headache did not differ in terms of the proportions with relapsing–remitting and secondary progressive MS, illness duration or disability, as also found recently (7). However, the prevalence of different primary headache forms did differ according to MS form: migraine was the most frequent primary headache among patients with relapsing–remitting MS, while tension-type headache was more prevalent among patients with the secondary progressive form.
The role of MS treatments in exacerbating pre-existing headaches and triggering de novo headache syndromes has been emphasized recently (8, 12). Furthermore, the recent meta-analysis of interferon trials in relapsing–remitting MS reported that headache was investigated as a side-effect in five of the seven trials considered. It was found that headache was significantly more frequent in MS patients receiving interferon than in those receiving placebo (18). We found that headache started after the initiation of anti-MS therapy in 15.3% of our clinical series. All these patients in fact received interferons. About half developed migraine and half developed tension-type headache. We also found that 1.7% of our patients reported headache as an MS onset symptom, a figure that is lower than in most published estimates (1, 2, 6, 7, 9, 10).
The presence of other comorbidities which may correlate with the presence or the worsening of headache cannot be excluded. In particular, we did not screen patients for the presence of depression or other psychiatric comorbidities.
Our findings seem to have important implications for clinical practice and research. The fact that primary headaches are highly prevalent in MS implies that these disorders should be investigated in the clinical work-up of every MS patient. The main reason for this is that MS and primary headaches can have a marked impact on patients’ functioning and sense of well-being (19–22) which might be even greater when these conditions are associated in the same patient. Assessment of health-related quality of life was beyond the scope of the present study; however, we sought relations between disability, as assessed by EDSS score, and presence/absence of headaches in our sample. No significant correlation was found.
Finally, although it is possible that the MS–primary headache association is due simply to the fact that both disorders are more frequent in females and in young adults, our data suggest the possibility that there may be a causal relationship between the two conditions, and particularly between migraine and relapsing–remitting MS.
The following speculations may guide further studies in elucidating the nature of such a link. Since reduced numbers of T8 lymphocytes seem to characterize both conditions (23–25), it may be that both arise from shared immune mechanisms. Another possibility is that repeated demyelinization of brainstem structures can cause migraine-like headaches in MS (6, 26, 27). There is evidence that several brainstem areas are involved in the pathophysiology of migraine. Studies in animals and humans indicate that the trigeminocervical complex, the rostral brainstem and periaqueductal grey matter have primary roles in the complex mechanisms underlying migraine attacks (28–31). Further studies are also needed to determine the exact relationship between immunomodulatory therapy and headache in MS patients.
Footnotes
Acknowledgements
The authors thank Don Ward for help with the English language.