
Abstract
The purpose of this study was to examine the relationship between the patterns of functional organization of the brain, as evaluated by the number of anomalous brain conditions or phenomena (ABCP), and the prevalence of migraine in a group of 434 women with lifetime major depressive disorder. ABCP are conditions or phenomena which are clearly related to brain function whose prevalence significantly deviates from the statistical mean for the general population. Eighteen ABCP (e.g. mixed or left handedness, enuresis after age 5, learning and speech disorders) were used in this study as ‘markers’ for their associated patterns of functional brain organization. The relationship between the number of ABCP and the prevalence of migraine was highly significant. The correlation between the number of ABCP and the prevalence of migraine was 0.36 (P < 0.0001, confidence interval 0.26, 0.43). The prevalence of migraine in patients with no ABCP (n = 11) was 9%, while that of those with eight or more ABCP (n = 40) was 85%. This supports the hypothesis that there is a relationship between patterns of functional brain organization and migraine prevalence.
Introduction
There are a number of studies, using a variety of investigatory techniques, which suggest that the interictal central nervous system (CNS) of migraineurs is in a state of increased sensitivity (1–5). This ‘state’ appears to be characterized by a reduced stimulus threshold, an increased responsiveness to a variety of external stimuli, and a decreased tendency for the brain to habituate to repetitious stimuli. These and other studies strongly suggest that the CNS of migraineurs, in the interictal state, is different from the CNS of those who have never had this disorder. The present study presents data derived through a different approach which are consistent with the findings cited above.
The vast majority of investigators concerned with the phenomena of health and disease believe that differences in human health arise as a consequence of interactions between genetic and environmental factors. The author has proposed that in addition to these factors, differences in the patterns of functional, or physiological, brain organization play a significant role in the pathophysiology of disease and the maintenance of health (6). Evaluating the concept of ‘patterns of functional brain organization’ is clearly problematic. However, there are many methods of measurement currently available which provide the means by which this hypothesis might be tested indirectly.
On the basis of a number of reports in the literature (7–16) and observations made clinically and during a previous study (17), the author hypothesized that anomalous behavioural conditions or phenomena (ABCP), which are clearly related to brain function (e.g. learning or speech disorders, left-right differentiation difficulties, left or mixed handedness) might be used as ‘markers’ for the patterns of functional brain organization with which they are associated. Each of these anomalous behaviours or conditions was assumed to be associated with different patterns of brain organization. If this assumption is correct the number or pattern of ABCP reported by each individual could be used as a measure to distinguish, or define, different patterns of brain organization. While this method of measurement clearly provides a very tenuous or minimalistic evaluation of the pattern of functional organization of the entire brain, it has proven to be a fortuitous choice.
This is the case because when the 14 ABCP (two of which were common and classic migraine) used in the previous study (17) were intercorrelated, the relationships between these seemingly very divergent phenomena showed a strong tendency to be positively interrelated. This was true regardless of the diverse average age of onset of the various ABCP. Eight of the 14 ABCP were significantly correlated with classic migraine in this study (17).
Many studies have shown that mental and physical disorders tend to be co-morbid on a lifetime basis (18–25). It is generally accepted that mental disorders arise as a result of dysregulations in CNS functioning. Based on a number of observations from diverse areas of neurobiology, it was hypothesized that the changes in patterns of brain organization associated with the dysregulations assumed to underlie mental disorders might be similar, or related to, the changes in the patterns of functional brain organization which are hypothesized by the author to be an integral aspect of the pathophysiology of physical disorders. For example, it has been frequently noted that migraine and depression are co-morbid disorders on a lifetime basis (26).
The present study involves 434 female patients who were diagnosed as having had at least one lifetime major depression. It is a preliminary test of the hypotheses outlined above, i.e. different patterns of functional brain organization, as defined by an increasing number of ABCP, will be associated with a progressively increasing vulnerability to develop migraine headaches.
Methods
The subjects of this study were 434 female patients who had met the DSM-IV (27) criteria for major depression at some time during their lives. All of these patients were evaluated, and most were treated, by the author in his private psychiatric practice in New York City between 1961 and 2002. They represent all the non-bipolar I affective disorder patients seen during this period on whom all of the data used in this study had been obtained.
In 1980, the author began collecting data on the ABCP and family history of physical illness on a consistent basis. Most of the female patients with a lifetime diagnosis of major depression seen after 1980 are included in this study. However, initially the author did not collect information on all of the ABCP used in this investigation. Different ABCP were added gradually, as detailed in the report of the ‘bipolarity’ study (17), and only partial data were available on many of these patients. Those patients were not included in the present study.
An attempt was made in 1980–1982 to contact patients seen prior to that date and obtain these data. When this was successful they were included in the current investigation. The patients’ mean age at the time of the initial evaluation was 36.8 years, SD 11.1 (range 17–78). Their mean number of years of education was 15.1 years, SD 2.39 (range 7–20 years).
Of these 434 patients, 70% were judged to have had at least one lifetime co-morbid mental disorder severe enough to meet DSM-IV criteria: 80 (18.4%) abused alcohol; 72 (16.6%) abused drugs; 219 (50.5%) had anxiety disorders (excluding obsessive-compulsive disorder); 45 (10.4%) had obsessive-compulsive disorder; 61 (14.1%) had eating disorders; 41 (9.4%) had somatoform disorders; and 44 (10.1%) had personality disorders. One hundred and thirty-three patients (30.6%) had one co-morbid disorder; 104 (24.0%) had two co-morbid disorders; 50 (11.5%) had three co-morbid disorders; and l7 (3.9%) had four or five co-morbid disorders. As a group the patients had a mean of 1.29 co-morbid disorders. Ninety-eight (22.6%) of the patients had been hospitalized psychiatrically at least once. Two hundred and eleven (48.6%) had a positive family history of depression. This group of patients had a prevalence of migraine of 50.6%.
Migraine headaches with and without aura were diagnosed by the author according to the International Headache Society (HIS) criteria (28). None of the migraine headaches in this group appeared to have been precipitated by physical disorders. Using the notes from the interviews during which these data were gathered, reliability ratings for major depression, the two types of migraine and the number of ABCP were made on every fifth patient by J. Endicott (Department of Research Assessment and Training, New York State Psychiatric Institute, New York, NY, USA).
Anomalous brain conditions or phenomena are defined as conditions or phenomena which are generally accepted as being associated with CNS activity and the prevalence of which significantly deviates from the statistical mean of the general population. Eighteen ABCP were used in the present study: night-time enuresis after age 5, fingernail biting after age 5, thumb sucking after age 5, speech disorders, dyslexia, arithmetic learning disorders, left handedness, mixed handedness, left switched to right handedness, left–right discrimination difficulties, episodic neurological phenomena, episodic nausea and/or vomiting (which appear to be unrelated to physical disease), sleep walking, car sickness, Raynaud's phenomena, repetitious fainting, seizures, and relatively brief visual disturbances like scotomata which are not followed by a headache. All but six of these ABCP are defined in the previous paper (17) and these will not be repeated here except for ‘episodic neurological phenomena’, which is not a widely used concept.
Episodic neurological phenomena
Relatively brief recurrent unusual or abnormal physiological or psychological events which: (i) were not followed by a headache, (ii) did not appear to be associated with neurological or systemic disease, (iii) did not occur only during periods of major depression or anxiety, and (iv) did not follow extrinsic pressure to the affected part (as during sleep). Three types were specifically inquired about: (i) paresthesias (e.g. tingling or numbness), (ii) visual changes (e.g. intermittent blurred vision), (iii) psychological (e.g. feelings of depersonalization).
In the earlier paper (17) dyslexia and arithmetic learning disorders were scored together as ‘learning disorders’. A number of findings indicated that these two learning problems should be scored separately. Women most frequently reported ‘problems with arithmetic’. It proved very difficult to obtain a reliable evaluation of the severity of the arithmetic learning problems. In order to gain reliability in rating these disorders, individuals were judged to have ‘arithmetic learning problems’ when they reported being unable to memorize the full multiplication tables up to 10 × 10.
Repetitious vasomotor syncope
Sudden onset of unconsciousness which was not associated with seizures or other physical diseases and occurred two or more times during the subject's lifetime.
Seizures
Six types of seizures were reported by this group: complex partial seizures (previously called ‘temporal lobe seizures’) (n = 13); simple partial seizures (also ‘temporal lobe seizures’) (n = 9); generalized tonic-clonic seizure (grand mal seizures) (n = 8); myoclonic seizures (n = 3); absence seizures (n = 2); and childhood febrile seizures (n = 1).
Visual anomalies
Phenomena such as scotomata of various types, fortifications, tunnel vision, etc., which appear relatively suddenly, are recurrent, last a few minutes to several hours and are not associated with headaches. They were scored independently from ‘episodic neurological phenomena’. Visual anomalies which were found to be associated with physical disorders, such as retinal or vitreous detachment, were not included in this category.
Reported family history of migraine included reports of headaches in parents or siblings which had been diagnosed by a physician as migraine or were characterized by at least one or more of the criteria in the IHS criteria for migraine (28). On some occasions this had to be inferred from patient reports. For example, patients would report that their parents vomited during the headache, or tied a band around their head and went into a dark room to sleep, or the children were not allowed to make any noise while their parent was trying to sleep in a darkened room, etc.
Statistical analysis
The mean age at intake and education of subjects with and without migraines were compared using t-tests. The Pearson correlation coefficient was used to assess the relationship between total number of ABCP and the prevalence of migraine. Logistic regression analysis was used to assess the contribution of the number of ABCP to the prevalence of migraine, controlling for the presence and absence of family history of migraine. The reliability of the diagnosis of major depression and of migraine was assessed using the κ statistic, while that of the total number of ABCP used the intraclass correlation coefficient.
Results
Of the 434 patients, 220 (50.6%) reported experiencing migraine headaches at some time during their lifetime. The mean age of those reporting migraine was 35.1 years (95% confidence level (CL) 33.8, 36.3) and that of those denying migraine was 38.5 years (CL 36.9, 40.2). These ages are significantly different (P < 0.001). The mean years of education of those reporting migraine was 15.1 (CL 14.7, 15.4) and that of those denying migraine was 15.1 (CL 14.8, 15.4) (differences not significantly different).
The κ coefficients of reliability of the diagnosis of major depression on every fifth patient (n = 87) was 0.92 and for migraine was 0.90. The reliability evaluation (intraclass coefficient correlation) of the number of ABCP was 0.96. All these evaluations indicate a high degree of agreement on these variables.
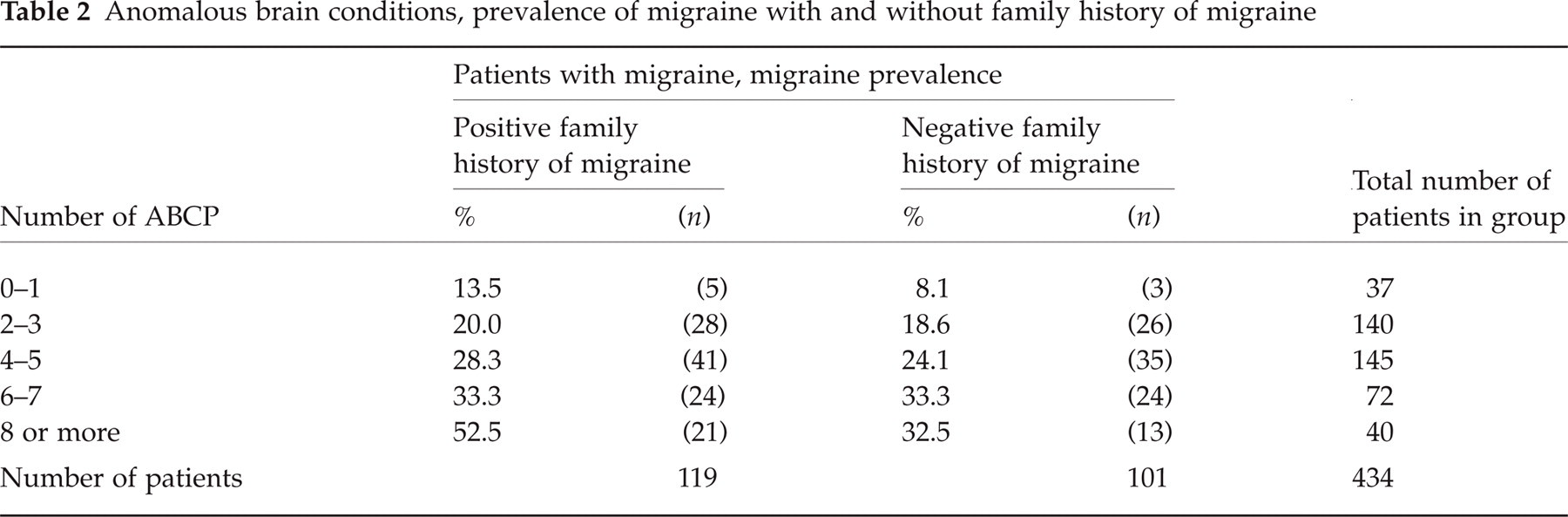
The Pearson correlation between the number of ABCP and the prevalence of migraine was 0.36 (P = 0.0001). These data are shown in Table 1. Logistic regression analysis indicated that the number of ABCP made a significant (P < 0.001) contribution to the prevalence of migraine, controlling for the reported family history of migraine. These data are given in Table 2.
Life time prevalence of migraine and patterns of functional organization of the brain

Anomalous brain conditions, prevalence of migraine with and without family history of migraine
Seventeen of the 18 ABCP used in the present study were positively correlated with the prevalence of migraine. Left handedness was negatively correlated (−0.09), but this was non-significant. Thirteen of the positive ABCP–migraine correlations were statistically significant: enuresis (r = 0.13, P = 0.006), speech disorders (r = 0.14, P = 0.003), dyslexia (r = 0.14, P = 0.002), mixed handedness (r = 0.13, P = 0.008), left handedness switched to right (r = 0.11, P = 0.02), left–right discrimination difficulties (r = 0.23, P < 0.0001), episodic neurological phenomena (r = 0.16, P = 0.0004), nausea and/or vomiting (r = 0.13, P = 0.007), sleep walking (r = 0.15, P = 0.002), motion sickness (r = 0.09, P = 0.048), Reynaud's syndrome (r = 0.25, P < 0.0001), seizures (r = 0.17, P = 0.0003), visual disturbances without headache (r = 0.11, P = 0.02).
Discussion
The finding of a highly significant relationship between the lifetime prevalence of migraine headaches in women and the number of their ABCP lends support to the hypothesis outlined in the Introduction, i.e. different patterns of functional brain organization are differentially associated with health outcomes, in this case migraine headaches.
Genetic (29, 30) and many environmental factors (31, 32) have been implicated in the pathophysiology of migraine attacks. By grouping patients according to their number of reported ABCP, as in Table 1, a ‘dimension’ is formed which can be interpreted as representing a measure (although a relatively inexact one) of an increasing vulnerability to one or more of the many factors which have been associated with the initiation of migraine attacks. This increasing vulnerability, evaluated by an increasing number of ABCP, is hypothesized to be a consequence of associated changes in the relative ease with which CNS dysregulations can be precipitated by genetic, environmental and/or other brain-related factors. A proportion of these CNS dysregulations, in turn, are hypothesized to constitute the CNS dysregulations which form an integral aspect of disease pathogenesis, in this case the pathogenesis of migraine headaches.
Seventeen of the 18 ABCP used in the present study (left handedness was the exception) were positively correlated with the prevalence of migraine. Since some of the diagnostic criteria for several of the ABCP used in this study (episodic neurological phenomena, motion sickness, nausea and/or vomiting, scotomata without headache) correspond closely to some of the IHS criteria for the diagnosis of migraine, their inclusion among the 18 ABCP used in this study may have spuriously inflated the reported relationship between the number of ABCP and the prevalence of migraine. The contention that the ABCP in question and the prevalence of migraine are not ‘independent’ of one another is almost certainly true. An underlying tenet of the hypothesis being tested in this investigation is that very few observable behavioural phenomena which deviate from the population norm (e.g. ABCP) will be ‘independent’ of one another; instead, it is hypothesized that there will be a strong tendency for these variables to be positively interrelated and thus, not independent.
From this point of view the primary issues to be addressed are not whether the ABCP, including the four ABCP in question, are independent of migraine, but rather the extent to which they are related exclusively to migraine as opposed to other disorders, and the nature of these relationships. These issues are extremely complex and the information necessary to resolve them adequately is not currently available. However, there are several observations which may help clarify them.
The ABCP were defined in such a way as to clearly differentiate them from migraine headaches and from one another. If an ABCP was ever associated with a headache it was not scored as an ABCP for that patient. This criterion was particularly important in defining ‘visual abnormalities without headache’, which will be labelled ‘scotomata without headache’ in this report. If a person ever had a headache associated with a visual abnormality this ABCP was not scored.
The author has treated one migraine patient (not included in this study) who reported episodes of blindness lasting approximately 3–10 min beginning in early adolescence. After several years of ‘scotomata without headache’ the patient's episodes of blindness began being followed immediately by migraine headaches, i.e. she had developed migraine with aura. Should this patient and patients like her have been scored as having ‘scotomata without headache’? Our knowledge regarding this condition is so minimal that the question can only be answered hypothetically. If ‘scotomata without headache’ was invariably eventually followed by development of migraine with aura, the inclusion of this ABCP in a study such as the present one would clearly, and at least from most investigators’ point of view spuriously, inflate the correlation between number of ABCP and the prevalence of migraine. However, in fact, among these 434 women this hypothetical sequence did not usually occur. Most of the patients in this group who were scored as having ‘scotomata without headache’ never developed migraine headaches and most of the individuals who did develop migraine never manifested ‘scotomata without headaches.’ In the present study the correlation between number of ‘scotomata without headache’ and migraine headaches was 0.11. While this is statistically significant (P = 0.02), it is a very modest relationship.
Space limitations preclude a more extensive discussion of this issue and questions involving the other three ‘questionable’ ABCP. In general, the discussion above applies to all of them, in that none of them was individually present in most patients who developed migraine headaches. In this group of 434 women the correlations between these three ABCP and migraine were: episodic neurological phenomena (r = 0.16), nausea and/or vomiting (r = 0.13), and motion sickness (r = 0.09). Again, while these correlations are all significant, they are relatively low. On the other hand, the relationships between left–right discrimination difficulties and Raynaud's syndrome with migraine (r = 0.23 and 0.25, respectively) are much more robust (P < 0.0001 for both). The diagnostic criteria for these ABCP and migraine are completely independent, i.e. free of shared criteria.
While the elimination of the four ABCP reduces the correlation between number of ABCP and migraine, this reduction is minimal and the relationship is still highly significant. They have been retained because they appear to be positively correlated with many other disorders and their elimination would hinder the investigation of their relationship to migraine and preclude comparisons of their correlations with migraine with the correlations between them and other conditions. For example, a correlation matrix was calculated using all of the ABCP in this study and a number of other variables. The relationships between these four ABCP and Raynaud's phenomena were: episodic phenomena (r = 0.14, P = 0.003), nausea and/or vomiting (r = 0.08, P = 0.10), motion sickness (r = 0.13, P = 0.008) and scotomata without headache (r =−0.01, P = 0.8). These data suggest that the ABCP tend to be positively interrelated, tend to be positively correlated with physical conditions other than migraine, and, not surprisingly, that ‘scotomata without headache’ is more highly related to migraine headaches than Raynaud's phenomena.
This tendency of anomalous phenomenological variables which are clearly related to CNS functioning to be positively interrelated is not confined to the present group of patients. The Collaborative Perinatal Project (NCPP) of the United States National Institute of Neurological and Communicative Disorders and Strokes avoids many of the methodological problems of the present study and presents a correlation matrix between behavioural phenomena and soft signs of neurological damage (33). This investigation followed 28 889 children from birth through the age of 8 years. Neurological examinations conducted at age 7 years revealed 2331 of these children to have one or more of 10 ‘soft signs’ of neurological damage (poor coordination, abnormal gait, impaired position sense, astereognosis, nystagmus, strabismus, abnormal reflexes, mirror movements, other abnormal movements, and abnormal tactile finger recognition).
Psychosocial evaluations were made at the same age and the children were rated on the degree to which they had seven behavioural anomalies: hyperactivity, hypoactivity, impulsively, short attention span, emotional lability, withdrawal and socioemotional immaturity. A correlation matrix including the seven behavioural anomalies and the 10 ‘soft signs of neurological damage’ was calculated. When the correlation between two mutually exclusive items (hyperactivity and hypoactivity) was eliminated, the remaining 17 items yielded 135 intercorrelations. Of these, 126 were positive (93%) and nine were negative. Correlations at the P < 0.001 level were considered significant in this study. One hundred of the 102 correlations which were significant at this level were positive and two were negative. One of the two significant negative correlations (hypoactivity and impulsivity, r =−0.04) might be considered to be between mutually exclusive items, but was included to preclude any question of bias on the author's part. All seven of these behavioural conditions and the 10 ‘soft signs’ can be considered to be ABCP, and hence ‘markers’ for patterns of functional brain organization with which they are associated. The results lend further support to the hypothesis that there will be a general tendency for ABCP to be positively related to one another. Although the degree to which the findings of either the authors (17) or the study described above (33) are generalizable to the general population is unknown, the data are consistent and appear to be of sufficient significance to justify further investigation.
The relationships between the ABCP which were found in the two studies noted above suggest that regardless of the age at which the ABCP become manifest, they tend to be positively correlated with one another. For example, a child of 6 who had one ABCP (e.g. enuresis) will be slightly more likely to develop migraine at some time in the future than a 6-year-old with no ABCP, and a 6-year-old with two ABCP will be more apt to develop migraine in the future than one with no or one ABCP, etc.
The data presented in Table 2 indicate that the number of ABCP, and presumably the patterns of brain organization for which they are ‘markers’, are significantly related to the prevalence of migraine both with and without a reported family history of migraine. As reported in Results, analysis of this data showed that there was a significant relationship between the number of ABCP and the prevalence of migraine, controlling for the influence of reported family history of migraine. A separate report will examine in more detail the relationship between the prevalence of migraine, the number of ABCP and a reported family history of migraine.
The relatively high rate of migraine in this group of patients (50.6%) is presumed to be a consequence of two factors: all patients were female, and all had been diagnosed as having had at least one lifetime major depression.
Epidemiological studies in western countries report a prevalence of migraine in women of 8–29%, with many studies having prevalences toward the high end of that range (34, 35).
Breslau et al. in studying a random sample, aged 21–30 years, of a Detroit HMO population, found a lifetime prevalence of migraine in females of 16.3% and a migraine prevalence of 32.6% in those women who had ever had a major depressive disorder (MDD) (36). Thus, the migraine prevalence in female depressives was roughly twice that in females in the general population.
While the prevalence of migraine among women in New York City is unknown, it is not known as one of the most ‘easy going’ places in the western world. It would appear reasonable to assume the New York City prevalence of migraine among women to be about 20–25%. If Breslau's finding that women with MDD had roughly twice as much migraine as that found in the general female population is generalizable to most other female populations, a rate of migraine of 40–50% is approximately what one would expect to find among the present group of women.
A major limitation of this study lies in the type of subjects involved, i.e. all of the women were drawn from a psychiatric practice and all had received a lifetime diagnosis of major depression. This may limit the relevance of these findings for women not similarly defined. While the degree of generalizability of the findings to other migraineurs is unknown, it appears unlikely that the results are totally irrelevant to other female migraine patients who have not had a major depression, because the underlying hypotheses were derived from, and appear to be applicable to, a wide range of ‘subjects’ including different clinical groups (8, 11, 33, 37, 38), animals (39, 40) and the general population (21, 26). However, definitive answers to questions regarding the generalizability of the present findings can only be obtained through attempts at replication utilizing different groups of migraine patients, especially population-based samples of women.
Another methodological problem stems from the method of diagnosis. The author made all of the determinations of depression, the ABCP and migraine. However, the κ coefficients of reliability given in Results indicate a high degree of agreement in the independent diagnosis of these conditions or phenomena.
It should also be noted that most of these diagnoses were made in the context of a study which was published many years prior to the author's conception of the hypothesis being tested in the present report (17). That investigation attempted to assess whether a psychophysiological dimension termed ‘bipolarity’ extended through all affective disorders. Fourteen of the ABCP used in the present study were the dependent variables in the earlier investigation. If a rating bias occurred, the direction of that bias would presumably have been toward increasing the relationship between ‘bipolarity’ and the number of ABCP. Such a bias would have little, if any, effect on the relationships being examined in the present report. None the less, future studies would be greatly strengthened by using independent evaluations of these variables.
Footnotes
Acknowledgements
Jean Endicott PhD completed ratings used to assess reliability of the measures. John Nee PhD completed the data analyses.