
Abstract
Cluster headache has not been fully investigated in Asians. One hundred and four patients (90M/14F; mean age 39.2 ± 12.2 years) with cluster headache were recruited from two major headache clinics in Taiwan. They filled out a structured cluster headache questionnaire. All participants were diagnosed to have episodic cluster headache. Mean age of onset was 26.9 years; mean latency of diagnosis was 8.1 years. A trend of decrease in male/female ratio with time was noted. Seventy-three percent were ex- or current smokers (M: 79%, F: 36%). Restlessness was reported by 51% patients. Only 1 patient (1%) reported visual aura. Patients responded well to standard acute and prophylactic treatment. The monthly incidence of cluster period was inversely related to sunshine duration. Compared to Western series, our patients were different in several aspects including the absence of chronic cluster headaches and a low prevalence of restlessness and aura. Racial and geographical factors might contribute to these discrepancies.
Introduction
Cluster headache is an excruciating headache syndrome. The distinctive features that are hallmarks of a cluster headache include male predominance, periodic occurrence with cluster attacks, and concurrence of autonomic features (1–4). Despite these well-known attributes, many cluster headache patients are either misdiagnosed or under-managed (1). These oversights may reflect the unfamiliarity with this syndrome of many physicians.
One reason for the lack of awareness may be the fact that cluster headache is much less common than other severe headaches such as migraine and tension-type headache. For example, one population-based study reported the prevalence of cluster headaches as only 0.069% (5). While most patients with cluster headache have episodic attacks, an estimated 10–21% of patients suffer from chronic cluster headache (1, 2, 6–8).
The bulk of our current knowledge and understanding of cluster headaches comes from Western-based studies. The clinical characteristics of cluster headache in other regions of the world are ill understood, and are based on only a handful of case reports or abstracts from African or Asian countries (9–10).
In order to characterize the clinical picture of cluster headache in Taiwanese citizens, we surveyed the registered patients with cluster headache in two major headache clinics in Taiwan.
Methods
Registered patients from two major headache clinics in Taiwan constituted the study population. The clinics were located in the Taipei Veterans General Hospital (VGH) and the Sin-Lau Hospital (SLH), Tainan. Only those patients who fulfil the 1988 classification criteria for cluster headache of the International Headache Society (IHS), (digit code 3.1) (11) were acceptable.
Hospital settings
VGH is a 2198-bed national medical centre that serves both veterans and nonveteran citizens. The hospital is located in Taipei, which is both the capital of Taiwan and a major urban centre with a population of approximately 2640000. Most of the patients of Taipei VGH come from northern Taiwan. The headache clinic has been operating since 1996.
SLH is an 828-bed community hospital located in the southern region of Taiwan, in the city of Tainan. Despite a population of 740000, Tainan is not as modern a city as Taipei, in terms of infrastructure and facilities. SLH serves both urban and rural patients. The headache clinic has been operating since 1991.
A referral system does not exist in Taiwan. Thus, all patients to these two hospitals are self-referred.
Target subjects
Headache registries – databases of headache patients – were established at VGH in 1997 and at SLH in 1994. We utilized these registries to contact all the registered cluster headache subjects via telephone or mail. Approval was sought from each subject to complete a questionnaire, either at home or at hospital, or via telephone.
Data collection
Information was compiled from a standardized cluster headache questionnaire to which all authors had agreed. To ensure the accuracy of the data, one author (Lin KH) reviewed all the completed questionnaires, and telephoned each patient to confirm uncertain or missing items.
Statistical methods
Descriptive and inferential statistics were computed with the use of SPSS for Windows, Version 11.0 (SPSS, Inc., Chicago, IL, USA). For continuous measures, Student's t-test or one-way analysis of variance (
Results
Participants
The headache registries produced a total of 10 934 headache patients(4634 from VGH and 6300 from SLH). Of these, 139 patients identified with cluster headache were contacted(100 patients from VGH and 39 from SLH). The questionnaire response rate was 81%, representing 113 patients. The questionnaire was completed at home by mail by 61% of respondents, at the hospital by 26% of respondents, and via telephone by 13% of respondents.
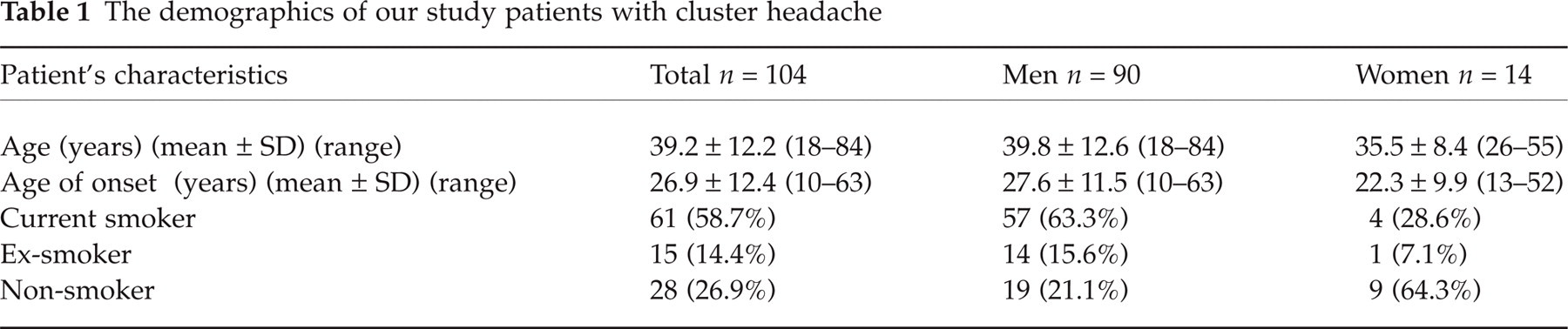
Two female patients presenting with chronic cluster headache had intracranial lesions, in the form of a parasellar meningioma and a pituitary adenoma, and so were excluded from further participation. A further 7 patients were found to have been misdiagnosed. Thus, a total of 104 patients(79 from VGH and 25 from SLH) fulfilled the IHS diagnostic criteria for cluster headache with a diagnostic accuracy of 92%. Their demographics are showed in Table 1.
The demographics of our study patients with cluster headache
Headache diagnosis
All patients fulfilled the criteria of episodic cluster headache (11), but none had chronic cluster headache. The mean duration from headache onset to diagnosis was 8.1 ± 8.0 years. The latency did not differ between female (9.7 ± 8.2 years) and male patients (7.8 ± 8.0 years, P = 0.403).
When patients were grouped according to their diagnostic years, no significant differences were evident in the mean latency to diagnosis (7.2 ± 7.1 years before 1997, n = 36; 9.4 ± 8.5 years during 1998–2000, n = 29; 7.9 ± 8.5 years after 2001, n = 36) (P = 0.563, one-way
Headache profile
Duration of cluster periods and cluster attacks
Fifty-five percent of the patients had a duration of the cluster period between 2 and 6 weeks, with a mean duration of 5.8 ± 5.0 weeks (range 0.4–35 weeks). The cluster attack lasted ≤ 1 h in 33% of patients, and 1–2 h in 34% of patients.
Sides and locations of headache
Strictly unilateral headache was the most frequent occurrence (80% of patients; right side 46%, left side 34%) followed by predominantly unilateral headache (17% of patients; right side 12%, left side 5%). The right side was more frequent than the left side(58% vs. 39%, z = 2.79, P = 0.005). Three (3%) patients reported equal attacks on shifting sides among different attacks.
The most commonly reported locations of cluster headache were temporal (76%) followed by retro-orbital regions (70%) (Table 2).
The locations of pain in study patients

Characteristics of headache
Most patients described their headache as pulsatile (56%), followed by compressive (34%), explosive (24%), and stabbing (24%). Cranial autonomic symptoms were all unilateral and lacrimation was the most frequent (83%). Other accompanied features included nausea (42%), vomiting (38%), photophobia (56%), and phonophobia (58%) (Table 3).
Comparison of the frequencies (%) of autonomic and other associated features between male and female patients
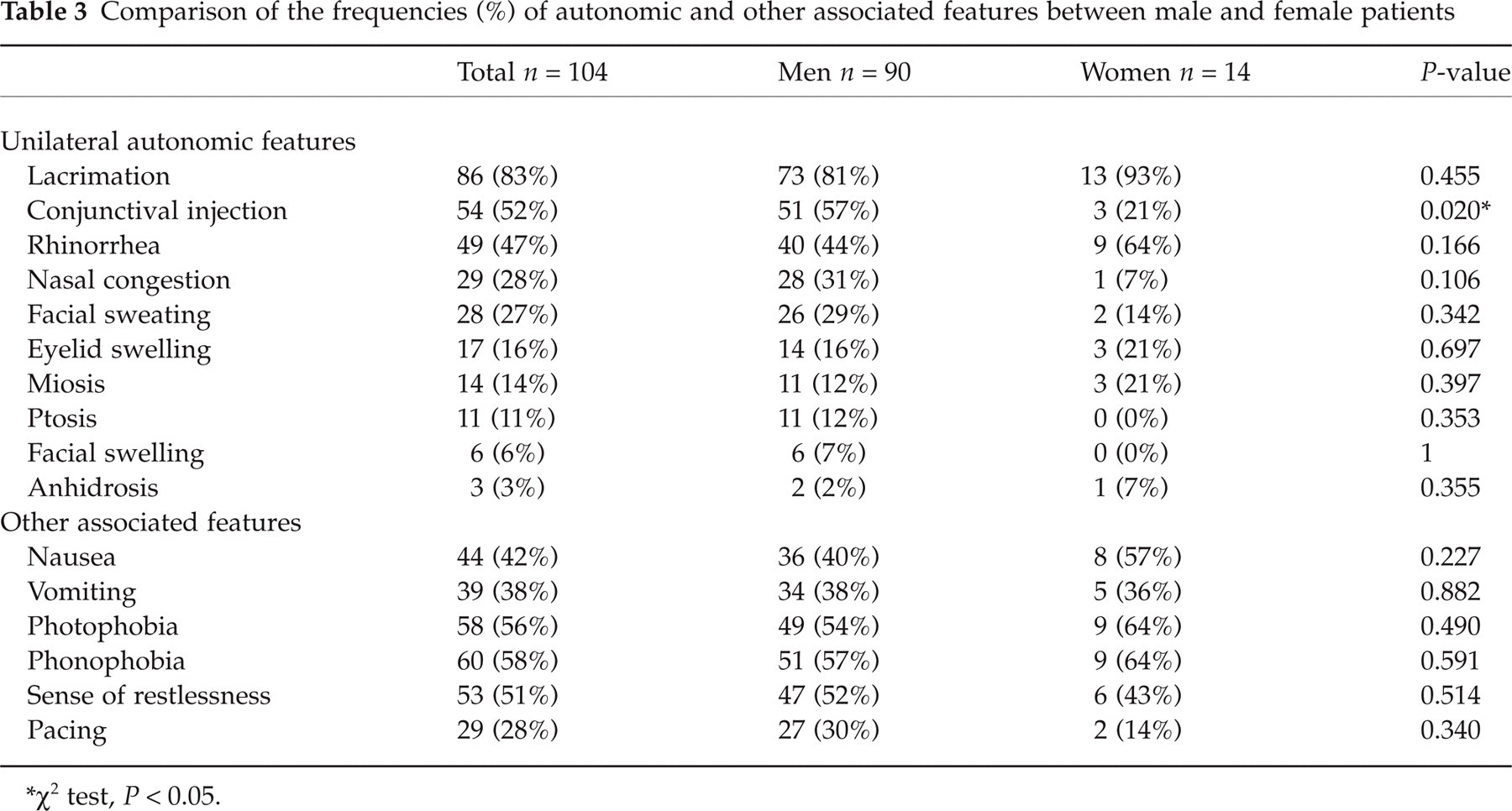
χ2 test, P < 0.05.
One 26-year-old female patient reported a visual aura prior to the cluster headache attacks. Not all attacks were accompanied by visual aura, which manifested as ‘moving waves’ and ‘blurred vision’ in her visual field for 5–10 min. Usually, 30 min after cessation of the aura, she began to suffer a cluster attack over her right orbital and temporal region. The patient denied any history of migraine.
Fifty-three (51%) patients experienced a sense of restlessness during attacks. Twenty-nine (28%) patients admitted that they preferred pacing about during the attacks (Table 3). Of the latter, two (7%) patients reported exacerbation of headache on pacing, 18 (62%) patients reported no relief and 9 (31%) patients experienced a decrease in discomfort.
Periodicity of headache
Forty-one percent of patients had one cluster period per year, 11.5% had one cluster period every 2 years and 11.5% had cluster periods twice per year. These periods occurred most frequently in December and March in both cities, as well as in September in Tainan (Fig. 1). The periods occurred least frequently in June (Fig. 1).

The relationship between the monthly incidence of cluster periods (no. of patients, • and monthly average sunshine (○) duration in (a) Taipei Veterans General Hospital (VGH) (northern Taiwan) and (b) Sin-Lau Hospital (SLH) (southern Taiwan).
Attempts to correlate the cluster periods with climate, including 5-year monthly averaged temperature, rainfall, atmospheric pressure, daylight hours and sunshine duration (12), revealed a possible relationship between the monthly incidence of cluster periods and duration of sunshine but not other climate variables. Two variables of the sunshine duration were tested, i.e. the number of monthly sunshine hours (amount) and the difference of monthly sunshine hours (change). The latter was arbitrarily calculated as the absolute difference between the sunshine duration in a month and the mean sunshine duration in the two previous months. The results showed the incidence of cluster periods was significantly and inversely related to sunshine hours (r = −0.774, P < 0.001) (Fig. 2). However, only a trend of significance was found between the change of sunshine duration and the incidence of cluster headache (r = 0.385, P = 0.06). A further multiple regression analysis showed that amount of monthly sunshine duration but not the change of sunshine duration was related to the incidence of cluster periods after controlling for the factor of geographical difference (Taipei vs. Tainan) (data not shown).

The correlation between the monthly incidence of cluster periods and monthly averaged sunshine duration. ○ Taipei; □ Tainan. Pearson's coefficient (r) =−0.771; P < 0.001.
During cluster periods, 56% of patients had one attack per day, 13.5% had one attack every other day and 10% had two attacks per day. Sixty-eight (65%) patients reported that the headache happened at about a fixed time, most frequently at midnight (28%) and in the afternoon (27%) (Fig. 3).
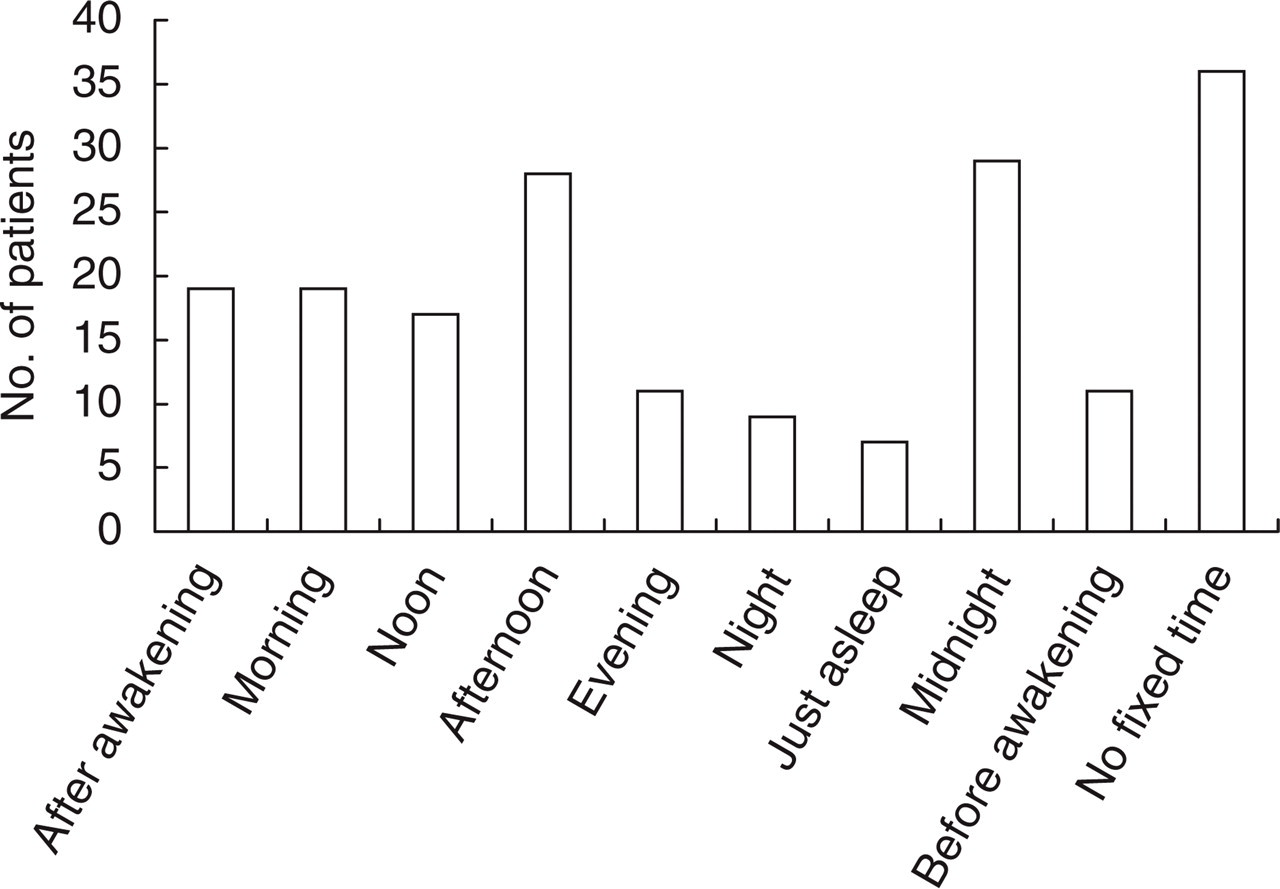
The frequencies of cluster attacks at different times of day.
Possible trigger factors
Of the 76 current smokers and ex-smokers, only six (8%) patients experienced headaches after smoking. However, 20 (24%) of 84 patients who had consumed alcohol reported headaches soon after alcohol consumption. Twenty-six patients reported that some special odour could induce headache attack. Forty-five (43%) patients experienced a headache attack when they had ‘not enough sleep’ or suffered from insomnia. Finally, 17 (16%) patients subjectively felt that increased body and weather temperature triggered their headache.
Family history of cluster headache
Six patients (in 4 families) had a family history of ‘physician-diagnosed’ cluster headache in their siblings. None of our patients reported cluster headache occurring with their parents.
Other types of headache
Four patients (4%, 2M, 2F) also had migraine headaches. Seventeen patients(16%, 13M, 4F) had tension-type headaches.
Characteristics in female patients
Five (36%) of 14 female patients were smokers (4 current and 1 ex-smoker) (Table 1). Except for a lower frequency conjunctival injection (men 57% vs. women 21%, P = 0.02, χ2 test) (Table 3), the female patients had a similar headache profile in comparison with male patients (data not shown).
Trend of decrease of male/female ratios
The number of patients diagnosed with cluster headaches increased with time. In contrast, the M/F ratio decreased from 11:1 (n = 36) during 1982 into 1997, to 8.7:1 (n = 29) during 1998 into 2000, and finally to 3.6:1 (n = 37) from 2001 to the report's preparation.
Northern vs. southern Taiwan
The involved hospitals were located in geographically different settings. Taipei is a metropolitan centre in a subtropical zone, while Tainan is a mixed urban/rural centre in a tropical zone. These differences prompted an exploration of the influence of these geographical factors on cluster headache.
The clinical features were similar in the two subgroups. However, the male-to-female gender ratio was lower in Taipei (5.1:1): than in Tainan (24:1). The proportions of cluster headache patients in the total pool of registered headache patients were lower at SLH (0.6%) than at VGH (2.5%).
Treatment efficacy of cluster headache
Acute therapy
Only one triptan (sumatriptan tablet 50 mg) was available in Taiwan during the period of the study. While only about 47% of the study population had ever used this therapy for acute cluster attacks, a high percentage (80%) of users reported the therapy to be effective. Inhalation of a high flow rate of oxygen had been used by 27% of the patients. Of these, 71% found the treatment effective (Table 4).
Frequencies (%) of usage and efficacy of treatment in study patients

Transitional therapy
For transitional therapy, 68 (65%) patients used prednisone (1 mg/kg). Of these patients, 42 (62%) used prednisone for up to 2 weeks, 5 (7%) for 3 weeks, 13 (19%) for 1 month, 5 (7%) for 2–3 months and 3 patients did not provide duration of prednisone usage. Fifty-seven (84%) of 68 patients considered the therapy to be effective.
Oral dihydroergotamine (10 mg/day) was used by 57 (55%) patients. Of these, 47 (83%) patients considered the therapy to be effective (Table 4).
Preventive therapy
Verapamil was used as a preventative therapy by 89 (86%) of patients. Seventy-eight (88%) of these patients maintained the treatment for no longer than 2 months. Of the total patient population who used verapamil, 72 (81%) patients reported the therapy as being effective.
Other treatments were markedly less used: lithium (4%), valproic acid (14%), tricyclic antidepressants (2%) and selective serotonin reuptake inhibitors (3%).
Alternative therapy
In our patients, several alternative therapies were tried but with unfavourable efficacy including: Chinese herbal medicine, n = 8 (8%), efficacy = 25%; acupuncture, n = 18 (17%), efficacy = 28% and massage, n = 39 (38%), efficacy = 28%.
Discussion
The present data comprise a clinic-based sample of cluster headache in Taiwan. Most clinical characteristics of cluster headache reported in this study are consistent with other studies involving larger patient populations in Western countries (1–4). These characteristics include:
similar age at onset: 26.9 years in the present study vs. 28.1–31.9 years (1, 7–8);
decreasing trend of M/F gender ratio;
most common area at the temporal and retro-orbital regions;
lacrimation as the most frequent autonomic symptom;
high frequencies of migrainous features such as nausea/vomiting, photophobia, and phonophobia;
once per day as the most common attack frequency;
about 5% of positive family history (1).
However, some discrepancies between the current results and previous results were also noted. The present patient population did not display chronic cluster headache, had a lower frequency of restlessness than reported elsewhere, and had a near absence of occurrence of aura as a prelude to a cluster attack.
The absence of chronic cluster headache is noteworthy. Chronic cluster headache either primary or secondary, consisted of 10–21% of all cluster headache patients in previous reports (1, 2, 6–8). The reason for this marked dichotomy is unknown. Some predictors for the evolution from episodic to chronic cluster headache have been suggested (2, 6, 13). Since our patient population displayed a similar clinical profile to those in the cited studies, the lack of patients with chronic cluster headache is perplexing. One Japanese study (9) also reported a low prevalence of chronic cluster headache (2/68, 2.9%). We do not know if Asians have a lower frequency of chronic cluster headache since the data from other countries in this region are very limited. It is of note that our two patients with symptomatic cluster headache presented with chronic course and were responsive to cluster preventive treatment. The headache subsided after removal of a tumour in one patient. Therefore, the presence of chronic cluster headache should alert the physicians of a possibly underlying structural lesion in Taiwan.
The present finding that only about half of those with cluster headache felt restless sharply contrasts with another recent report of a very high frequency of restlessness (93%) (1). The authors of the latter report suggested restlessness, agitation, and the absence of aggravation of pain with movement as revised criteria for IHS cluster headache (1). We cannot offer an explanation for the difference in the study populations concerning restlessness, other than that the suggested revised criteria might be less sensitive in our patients than in Western patients.
Cluster headache occurs much more frequently in men than in women. Reported M/F ratios range from 2.5:1 to 6.7:1 (1, 2, 6–8, 14–16). The ratio may be decreasing in more recent times (14–15). Our study is consistent with the latter findings. It has been suggested that major lifestyle changes, particularly relating to adoption of smoking and employment outside the home may be fueling the increasing prevalence of cluster headache in women (15). Consistent with previous studies (1–2, 7, 15), current smokers were much more prevalent in patient population (M: 63.3%, F: 28.6%) than the general population (M: 47.27%, F: 5.23%) (17). The smoking M/F ratio in the general population was 9:1 and the ratio of our cluster headache patients was 6.4:1. This relationship is similar to those in a Western study (15). In fact, the difference of smoking gender ratio between Taipei and Tainan might also be related to the difference of gender ratio of cluster headache between the two sampled hospitals. The M/F ratio of cluster headache was much lower in VGH (5.1:1) than in SLH (24:1), whereas the M/F ratio of smoking habits was 6.92 (50.01%/7.23%) in Taipei and 20.5 (48.38%/2.36%) in Tainan (15).
Similar to previous reports (1–2, 16), our patients reported high frequencies of migrainous features. We do not consider the contamination of migraine cases in our cluster patients as a major contributing factor for the high frequencies of migrainous features. Therefore, the presence of migrainous features cannot be used to rule out the diagnosis of cluster headache. In general, cluster headache was not considered to be associated with aura symptoms. As early as 1972, Graham (18) had reported visual aura as scintillating scotoma in their cluster headache patients. Silberstein et al. (19) reported on six cluster headache patients who had stereotyped auras preceding their individual cluster attacks. A recent study reported as high as 14% of aura in their cluster patients (1). However, we only found 1 (1%) female patient with visual aura before cluster attacks, evidently in the absence of a history of migraine headache.
The similar clinical picture of cluster headache between men and women in the present study echoes the findings of previous reports (1, 2). A recent study in a tertiary headache centre, which found some different characteristics in women with cluster headache (16), is contrary to the previous reports and the present study. However, the small sample size of our female patient population limits any comparison with the recent report.
The linkage of the incidence of the cluster periods and seasonal change noted presently is qualitatively comparable to Western studies, although the peak incident months varied (1–2, 20–22). The seasonal influence was noted in both of our study clinics. The variation of incidence among different months was more apparent in northern than in southern Taiwan, which was compatible to the degree of climate change between these two regions (Fig. 1). This seasonal influence appears to be focused on the monthly average duration of sunshine, and not other climatic variables. A previous study has mentioned a negative relationship between cluster period incidence and daylight hours (22). However, based on the different patterns of cluster period monthly incidence between Taipei and Tainan, we suggest that true sunshine exposure might be more important than total daylight hours as an influence to the occurrence of cluster headache. Sunshine exposure may influence the pineal gland and hypothalamus, which are considered as the centre for the pathophysiology of cluster headache (23, 24).
In theory, the brevity of cluster headache attacks precludes most oral abortive treatments. However, sumatriptan (50 mg tablet) and high flow oxygen were judged effective in our patients. Unfortunately, these two treatments were used in less than 50% of patients. Prednisone was used in 65% of our patients as transitional prophylaxis; whereas, verapamil was used in 85% patients as maintained prophylaxis. These two prophylactic agents also worked well in our study patients.
The time lag between the onset and the diagnosis of cluster headache has not decreased in recent years. This unexpected finding leads to the suggestion that physicians in Taiwan might not be alert enough in the diagnosis of cluster headache. Education of physicians about the diagnosis of this devastating and treatable headache is an important issue to address in the near future.
There are several potential limitations to the present study. Firstly, the extrapolation of the data obtained in just two headache clinics to the general population may be unwarranted. Arguing against this point is the fact that Taiwan has always lacked a referral system. Since all headache patients have been self-referred, the clinical data may in fact be representative of the more global community population than data that has originated from tertiary headache centres in Western studies. Secondly, because the data from the cluster headache questionnaire were collected retrospectively; a recall bias may exist in determining the exact months of the incident of cluster periods as well as the treatment efficacy. Therefore, these data should be interpreted cautiously.
Footnotes
Acknowledgements
This study was supported in part by a grant from Taipei-Veterans General Hospital (VGH 331).