
Abstract
We present a review of 22 cases of headache mimicking chronic paroxysmal hemicrania (CPH) (17 female and five male; F : M ratio 3.4), nine cases mimicking hemicrania continua (HC) (seven female and two male) and seven cases mimicking SUNCT syndrome (five male and two female) found in association with other pathologies published from 1980 up to the present. All case reports were discussed with respect to diagnostic criteria proposed by International Headache Society (IHS) for CPH, by Goadsby and Lipton for HC and SUNCT, and evaluated to identify a possible causal relationship between the pathology and the onset of headache. The aim of the present review was to evaluate if the presence of associated lesions and their location could help elucidate the pathogenesis of trigeminal autonomic cephalalgias (TACs).
Introduction
Chronic paroxysmal hemicrania (CPH) is a primary headache disorder described first by Sjaastad and Dale in 1974 (1) and is included in the International Headache Society (IHS) Classification of 1988 (2). Its main features are: frequent attacks of strictly unilateral, very severe pain localized in the orbital, supraorbital or temporal regions; attack duration from 2 to 45 min; frequency usually ranging from 2 to 40 attacks in a day. The pain is associated with prominent autonomic symptoms, such as tearing, conjunctival injection, rhinorrhoea, nasal stuffiness and ptosis of the omolateral eyelid (3). Among diagnostic criteria is listed a rapid and complete response to indomethacin, at a dose up to 150 mg (4). The chronic form does not have a recognizable temporal pattern, while episodic paroxysmal hemicrania (EPH), a more rare disorder, is characterized by bouts of frequent, daily attacks with the same clinical features as CPH, but separated by relatively long remissions, in a pattern similar to episodic cluster headache (5). A definitive classification of these forms is needed.
Hemicrania continua (HC) is another primary headache characterized by absolute response to indomethacin, which is considered a diagnostic criterion. It was described by Sjaastad and Spierings in 1984 (6). Its clinical features are: strict and unchanging unilaterality of the headache; continuous temporal pattern of the headache in its full-fledged form (but unremitting pain could be preceded by a remitting pattern); moderate to more severe headache; relative paucity of attack-related autonomic symptoms and signs and lack of precipitation mechanisms. In both these forms, a female preponderance (4–7), and some cases which are also responsive to other non- steroidal anti-inflammatory drugs (NSAIDs) (8–13), were described.
SUNCT syndrome is the acronym of Short-lasting Unilateral Neuralgiform headache attacks with Conjunctival injection and Tearing. This expression refers to another headache syndrome first described by Sjaastad et al. in 1989 (14) which is characterized by brief, strictly unilateral pain attacks without side-shift, stabbing or burning in quality, usually lasting 5–120 s, and accompanied by important ipsilateral autonomic manifestations. The patients, the majority males, experience up to 30 attacks per hour, but usually the frequency is 5–6 per hour (15). Some recent case reports (16, 17) have shown a responsiveness of this headache syndrome to lamotrigine .
These headaches, together with cluster headaches, have been grouped together in the chapter on trigeminal autonomic cephalgias (TACs) for inclusion in the forthcoming issue of IHS Classification. This is because these syndromes share various clinical features, mainly the presence of autonomic symptoms, although they, from a clinical and therapeutic point of view, appear as separate clinical entities.
In literature, from 1980 to the present day, we found some rare cases described by the authors as CPH, but associated with various intra- or extracranial pathologies. In addition, there are more recent observations of HC or SUNCT syndrome, also associated with other diseases.
The association of cluster headache with artero-venous malformations, pituitary
adenomas, aneurysms, infectious diseases and other pathologies has been well known for
more than 25 years and it is the topic of a recent literature review (18)
The association of these headaches with a structural lesion or a general disease gives rise to particular problems. Firstly, the inclusion of the case report, as stated above; in some cases, the diagnosis does not fulfil IHS diagnostic criteria for CPH, or diagnostic elements are not sufficient for the diagnosis. Secondly, there is a pathogenetic link between the lesion and the headache, or the possibility of a coincidental association, as stressed by many authors.
A review of these reports is now needed and may be an aid in the search for future cases and a contribution to the pathogenetic exploration of TACs.
Case material
We reviewed a wide search of the literature from 1975, 1984 and 1989, respectively, to June 2001, to identify all the relevant case reports presented by authors as CPH, HC and SUNCT syndrome, in association with intracranial or extracranial pathologies, using MEDLINE/Index Medicus, Current Contents/Clinical Medicine and EMBASE/Excerpta Medica. We not only carefully reviewed the reference lists of all papers found, but also, in some instances, contacted one of the authors to obtain further information about a case.
The first case presented was published in 1980. We considered all the cases presented as CPH and critically reviewed the diagnoses following IHS criteria (2). As far as HC and SUNCT cases are concerned, the diagnosis was discussed following the criteria set forth by Goadsby and Lipton (19). In the literature, other diagnostic criteria for HC have been more recently proposed by Pareja et al. (20). A comparison between these criteria was made by Bigal et al. (21), with the conclusion that the Goadsby and Lipton criteria would be more clinically useful. The search was restricted to papers written in English, French, German, Italian and Spanish. The evaluation did not include case reports lacking important information (i.e. sex, age of the patient or features of the headache). This is sometimes the case when Abstracts, Letters, etc. (22) are concerned.
Although every effort was made to include all patients in the literature, it is possible that some reported cases were missed.
Chronic paroxysmal hemicrania (23–40)
Sex ratio and age at onset
The review includes 22 cases presented as CPH, 17 female (77.3%) and five male (22.7%), demonstrating a female preponderance (F : M ratio of 3.4), approximately the same as in idiopathic CPH. The cases included in the review are listed in Table 1.
Chronic paroxysmal hemicrania in association with other pathologies
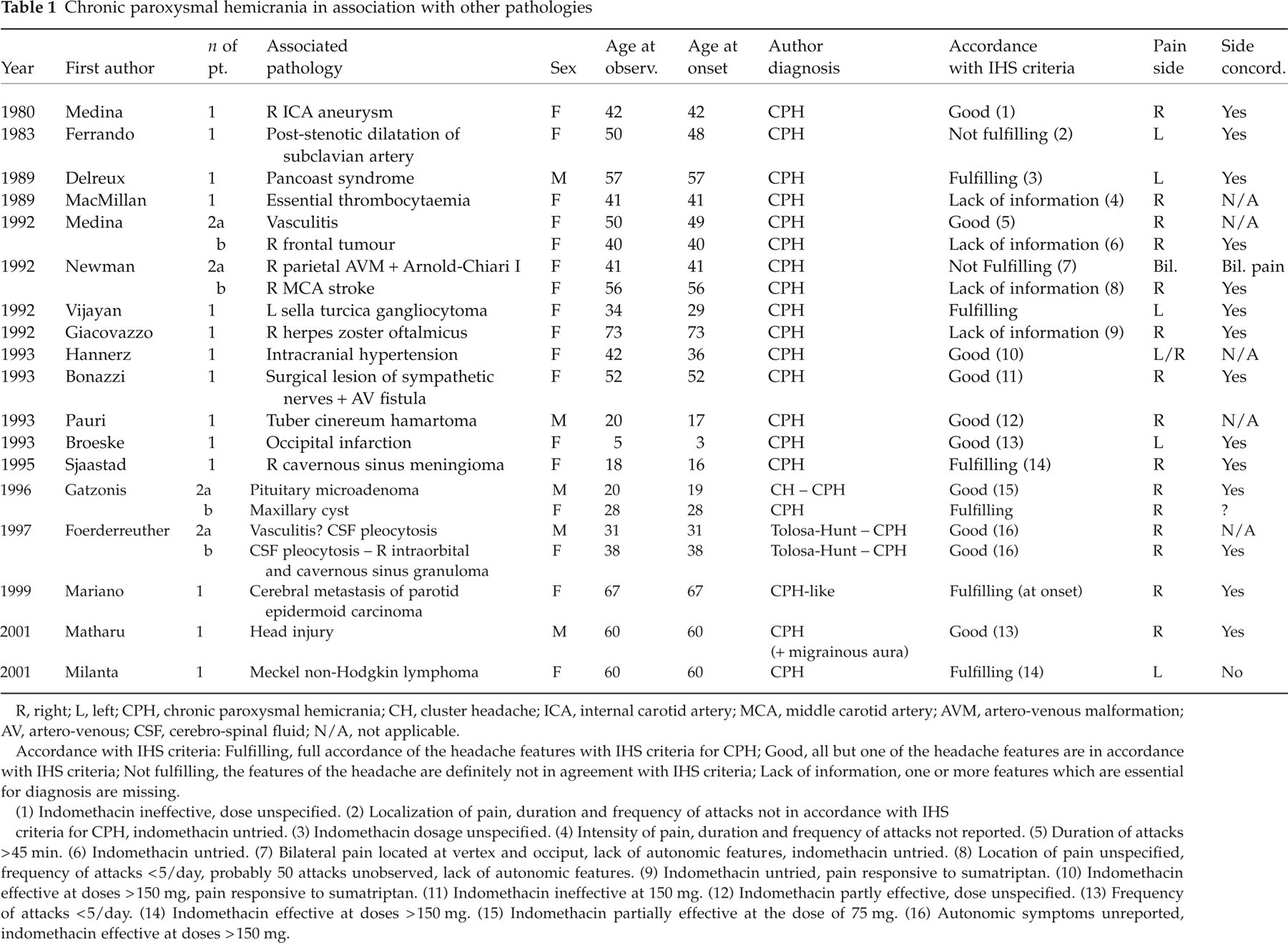
R, right; L, left; CPH, chronic paroxysmal hemicrania; CH, cluster headache; ICA, internal carotid artery; MCA, middle carotid artery; AVM, artero-venous malformation; AV, artero-venous; CSF, cerebro-spinal fluid; N/A, not applicable. Accordance with IHS criteria: Fulfilling, full accordance of the headache features with IHS criteria for CPH; Good, all but one of the headache features are in accordance with IHS criteria; Not fulfilling, the features of the headache are definitely not in agreement with IHS criteria; Lack of information, one or more features which are essential for diagnosis are missing. (1) Indomethacin ineffective, dose unspecified. (2) Localization of pain, duration and frequency of attacks not in accordance with IHS criteria for CPH, indomethacin untried. (3) Indomethacin dosage unspecified. (4) Intensity of pain, duration and frequency of attacks not reported. (5) Duration of attacks > 45 min. (6) Indomethacin untried. (7) Bilateral pain located at vertex and occiput, lack of autonomic features, indomethacin untried. (8) Location of pain unspecified, frequency of attacks < 5/day, probably 50 attacks unobserved, lack of autonomic features. (9) Indomethacin untried, pain responsive to sumatriptan. (10) Indomethacin effective at doses > 150 mg, pain responsive to sumatriptan. (11) Indomethacin ineffective at 150 mg. (12) Indomethacin partly effective, dose unspecified. (13) Frequency of attacks < 5/day. (14) Indomethacin effective at doses > 150 mg. (15) Indomethacin partially effective at the dose of 75 mg. (16) Autonomic symptoms unreported, indomethacin effective at doses > 150 mg.
The age at onset of symptoms varies con-siderably (range 3–73
years)
Symptomatology
The clinical picture of each patient is presented according to IHS diagnostic criteria for CPH in Table 1. In six patients, the symptoms definitely fulfilled IHS criteria (except for the effective dosage of indomethacin in three patients); in 10 cases, there was good accordance, except for one criterion; in two cases the original description definitely did not fit IHS criteria, and in four cases some information was lacking.
Localization of pain
The pain was strictly unilateral in all but one case [see reference 28 (case A)] (localized at the vertex and radiating to the occiput), and in another case (31) a side-shift was observed (but the pain remained unilateral). The areas in which the pain was felt were frequently multiple; for this reason, the indicated areas exceed the number of patients. The main sites of pain were retro-periorbital in 14 cases, fronto-temporal in 14 cases, with radiation to the homolateral ear, maxillary, cervical or scapular region in seven cases. In one case, the pain is reported only in the ‘hemiface’, with widespread radiation, and in two cases the information was missing.
Associated pathologies
The associated pathologies are listed in Table 1. There are four cases with vascular pathologies (including an aneurysm), seven with intracranial and two with extracranial space-occupying processes, four with inflammatory or infectious diseases, one with a parietal MAV and Arnold-Chiari malformation, one with anamnesis of a head injury, one with a finding of intracranial hypertension, one with essential thrombocytaemia and one with a post-surgical lesion of sympathetic nerves plus A-V fistula.
Treatment
Absolute efficacy of indomethacin is one of the diagnostic criteria of CPH, so is not surprising that all patients diagnosed as such were treated with this drug. Also, the patients diagnosed as CPH-like, whose clinical picture was strongly similar to CPH and was in association with other pathologies, must not only take indomethacin but be responsive to it to formally carry out the diagnosis. However, as the effect of indomethacin in CPH can be exerted at different doses, IHS criteria require an absolute effect at a dose of 150 mg daily or below. This is not the case in all reports presented in this review: in two cases (23, 32), indomethacin was ineffective; in five cases [31, 35 (case B), 37 (cases A and B), 40] the dose of indomethacin needed to obtain therapeutic effect was higher than 150 mg, ranging from 200 to 350 mg; in one case [36 (case A)] the dose of 75 mg was partly effective (but the higher dose was not tested), in two cases (25, 33), the dose of indomethacin was unspecified, and in four cases [24, 27 (case B), 28 (case A), 30] indomethacin was not administered. It is of interest that in two cases sumatriptan was effective (30, 31), unlike in genuine cases of CPH (41).
Hemicrania continua (35, 42–46)
Sex ratio and age at onset
The nine cases presented as hemicrania continua associated with other pathologies are seven female (77.8%) and two male (22.2%), showing a female preponderance (F : M ratio 3.5) as in idiopathic HC. The mean age at onset of symptoms was 32.78 ± 10.87 (range 16–53), and at observation 36.89 ± 8.62 (range 28–53). These patients are on average younger than those affected by CPH. The duration of the illness before diagnosis was, on average, 4.11 years (range 6 weeks−18 years). These cases are listed in Table 2.
Hemicrania continua in association with other pathologies
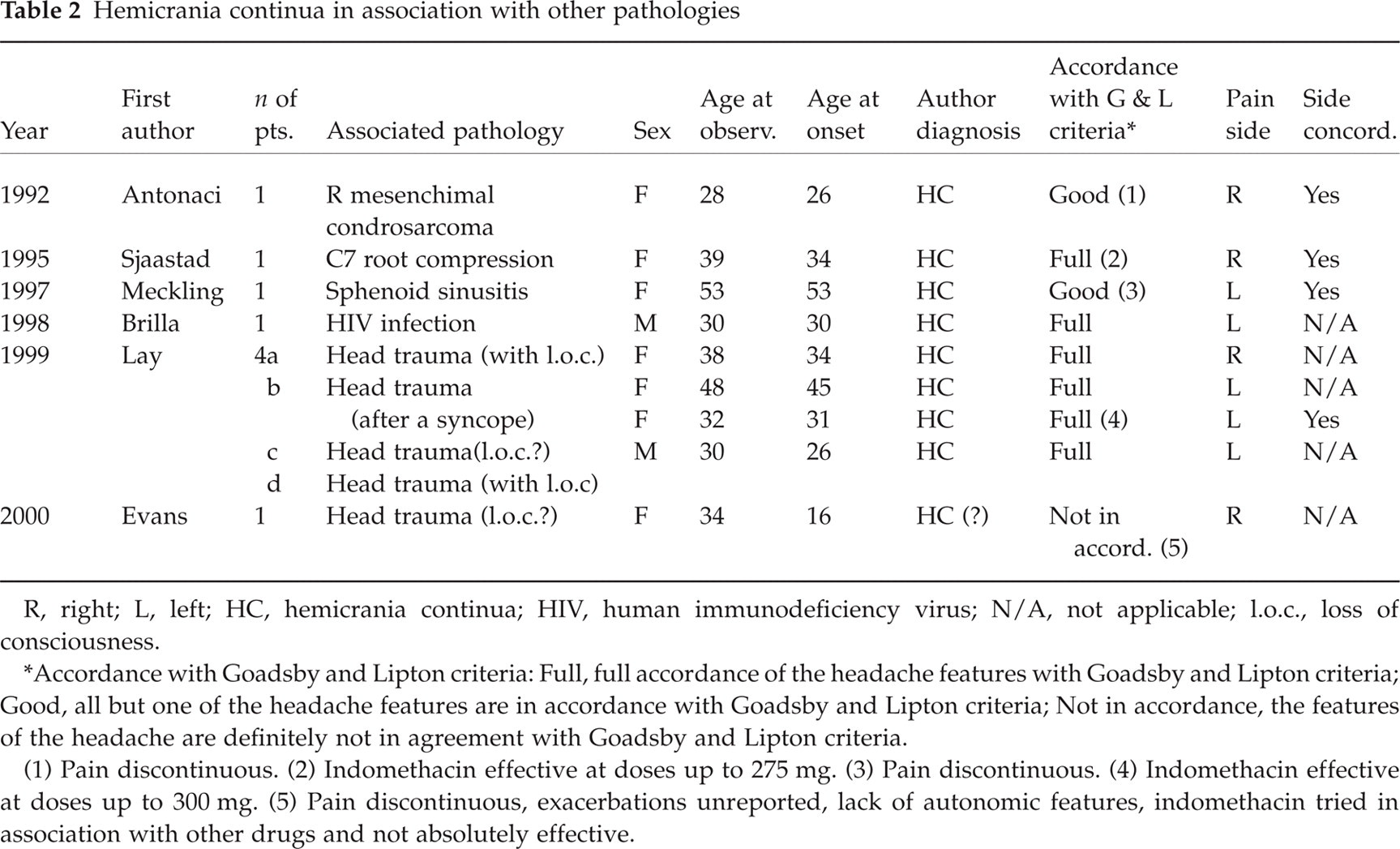
R, right; L, left; HC, hemicrania continua; HIV, human immunodeficiency virus; N/A, not applicable; l.o.c., loss of consciousness.
∗Accordance with Goadsby and Lipton criteria: Full, full accordance of the headache features with Goadsby and Lipton criteria; Good, all but one of the headache features are in accordance with Goadsby and Lipton criteria; Not in accordance, the features of the headache are definitely not in agreement with Goadsby and Lipton criteria.
(1) Pain discontinuous. (2) Indomethacin effective at doses up to 275 mg. (3) Pain discontinuous. (4) Indomethacin effective at doses up to 300 mg. (5) Pain discontinuous, exacerbations unreported, lack of autonomic features, indomethacin tried in association with other drugs and not absolutely effective.
Symptomatology
HC-like diagnosis is discussed with respect to the Goadsby and Lipton (19) diagnostic criteria for HC. We have listed six cases in full accordance (in two of them the dose of indomethacin was higher than in idiopathic cases), two cases with good accordance (all but one criterion fulfilled) and one case definitely not in agreement.
Localization of pain
In the majority of cases, the pain is located in the temporo-orbital area, but sometimes it starts or radiates in the frontal or occipital region.
Associated pathologies
The associated pathologies are listed in Table 2. In HC-like cases, there is a definite preponderance of head traumas (five); there is also one case of intracranial tumour, two cases of infectious diseases and one with C7 root compression.
Treatment
As in CPH, one of the original diagnostic criteria for HC is the absolute effect of indomethacin. Goadsby and Lipton criteria consider the possibility of otherwise genuine HC, but which is unresponsive to indomethacin (47). In HC, the adequate dosage of the drug, as a diagnostic criterion, is up to 150 mg per day for 3 days (48). In most of the papers concerning this disease, it appears generally lower than for CPH, only occasionally reaching 150 mg. In the papers we reviewed, the dose ranged from 50 to 300 mg; in one case indomethacin 75 mg lost its efficacy in 2 months (42) and in two cases [35 (case A), 45 (case C)] indomethacin 150 mg was ineffective, requiring higher dosages. Even in HC-like headaches, as in CPH-like headaches, there seems to be a trend towards a higher dose requirement than in idiopathic cases.
SUNCT syndrome (49–55)
Sex ratio and age at onset
We found seven ‘symptomatic’ cases of SUNCT syndrome: five male (71.4%) and two female (28.6%). In these cases, a male preponderance was observed (M : F ratio 2.5 : 1). They are listed in Table 3.
SUNCT syndrome in association with other pathologies

R, right; L, left; SUNCT, shortlasting unilateral neuralgiform headache attacks with conjunctival injection and tearing; AVM, artero-venous malformation; HIV, human immunodeficiency virus; N/A, not applicable.
∗Accordance with Goadsby and Lipton criteria: Full, full accordance of the headache features with Goadsby and Lipton criteria; Good, all but one of the headache features are in accordance with Goadsby and Lipton criteria.
(1) Some of the attacks exceeded 120-s duration. (2) Duration of the attacks > 120-s.
Gender ratio in idiopathic SUNCT syndrome is still a matter of debate. Pareja and Sjaastad reported an M : F ratio of 4.25 (15), but other authors (56) report a female preponderance (F : M 9 : 2).
The mean age at onset was 43.71 ± 18.61 (range 14–63), and at observation was 47.86 ± 17.18 (range 24–70). These patients are, on average, older than those affected by CPH or HC, as in idiopathic SUNCT syndrome. In these cases, the delay between the onset of headache and the diagnosis was on average 4.14 years, ranging from 7 days to 10 years.
Symptomatology
All these cases fulfil Goadsby and Lipton diagnostic criteria for this syndrome, except two cases (52, 54) characterized by a longer duration of the attacks.
Localization of pain
In all case reports, the pain is located unilaterally in orbital or fronto-orbital area.
Associated pathologies
The pathologies found in association with SUNCT-like syndrome (Table 3) were three artero-venous malformations (in the posterior fossa), one brain-stem ischemic lesion, one HIV infection and two congenital bone malformations, mainly concerning the posterior skull (one with seborrheic dermatitis). It is remarkable that most of the lesions found in association with this syndrome involve the posterior fossa or, in general, the posterior part of the brain.
Treatment
Up until a few years ago, SUNCT syndrome has been considered an intractable headache disorder. Only in 1999, lamotrigine was proposed as an effective treatment for this clinical entity. In the case reports presented in this review, various treatments have been used, but generally without result. Only carbamazepine is reported in two cases as effective; in other cases it is only reported as not very effective or its efficiency fades away in a short time. In one case spontaneous improvement of the headache is reported.
Treatments used in SUNCT-like cases are reported in Table 4.
Treatments used for seven cases of SUNCT-like headache
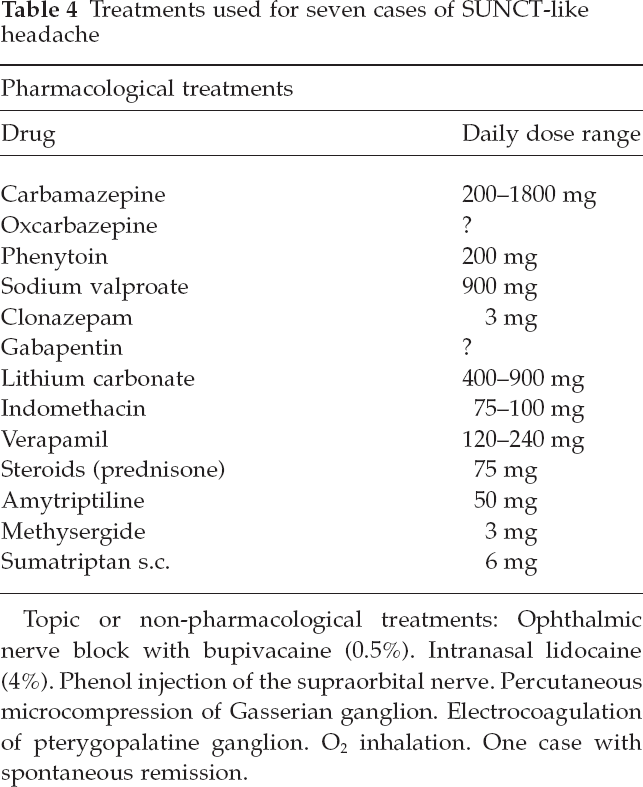
Topic or non-pharmacological treatments: Ophthalmic nerve block with bupivacaine (0.5%). Intranasal lidocaine (4%). Phenol injection of the supraorbital nerve. Percutaneous microcompression of Gasserian ganglion. Electrocoagulation of pterygopalatine ganglion. O2 inhalation. One case with spontaneous remission.
Figure 1 summarizes the age at onset of symptoms separately for the three headaches.

CPH-, HC-, and SUNCT-like headaches. Age at onset.
Comparison
The associated pathologies are grouped and listed separately for the three headaches in Table 5.
Associated pathologies in 40 TAC-like cases

Discussion
We have identified a number of case reports presented by the authors as CPH, HC or SUNCT syndrome in association with other pathologies, in order to critically review them with respect to diagnostic criteria and a possible pathogenetic link between the associated pathology and the headache. In two reviews on CPH (4) and HC (7), various cases of the headaches are reported as associated with or following other pathologies (e.g. head trauma, systemic diseases, etc.). We preferred to restrict the search only to case reports in which the authors fully describe and discuss the associated diagnosis, as a possible cause of the headache.
The number of published cases is rising yearly, probably due to the spreading knowledge of these uncommon headaches, along with the wide diffusion of neuroimaging techniques. On average, medium age at onset is older than for idiopathic cases as far as CPH is concerned, while among HC and SUNCT cases, medium age at onset is about the same as in primary headaches.
Although a limited number of patients is concerned, gender ratio in ‘secondary’ cases approximately reproduces the ratio seen in idiopathic cases.
The most commonly associated pathology with CPH-like headache is by far the neoplastic
one, but also inflammatory/infectious diseases are well represented. In HC-like
headache, post-traumatic cases are predominant; likewise, head trauma is also reported
as relative frequent (22%) in the review by Bordini et al. (7). In SUNCT-like cases, vascular and
bone malformations in the posterior fossa are most commonly observed. These data are
somewhat different from those seen in cluster-like cases, where the most frequently
observed pathology in association with the headache was the vascular one, in particular
aneurysms and vascular malformations. What is also of interest is the predominance of
general inflammatory processes, in comparison with the finding of only two infectious
localizations (
As stated before, the agreement with IHS criteria for CPH is incomplete in some cases. Among the cases reported as CPH, we have recognized six cases in which the diagnosis was not acceptable or at least questionable: (i) in the case reported by Ferrando et al. (24), the maximum frequency of the attacks were two in a week, the duration of the attack exceeded 12 h and could reach 48 h, the localization of pain was wider than in genuine CPH and indomethacin was not administered; (ii) in the first case by Newman et al. (28), the pain was not unilateral (located at vertex, occiput and base of the skull) and was unaccompanied by autonomic symptoms. Furthermore, indomethacin was not tried in this case.
In other reported cases there is a lack of important information: (iii) in the case by MacMillan and Nukada (26), the intensity of pain, duration and frequency of attacks were not reported; (iv) in the second case by Medina in 1992 (27), the author states that indomethacin was not used; (v) in the second case by Newman et al. (28), the localization of pain is not reported, accompanying symptoms were absent, the frequency of the attacks was low and it is likely that 50 attacks were not observed; (vi) Giacovazzo et al. (30) did not use indomethacin, but sumatriptan (effective).
In other cases, only one IHS criterion is missing: for example, in the first case by Medina (1992) (27), the pain lasted for about 1 hour; in the case described by Hannerz and Jogestrand (31) there was a side-shift after 5 years of strictly left-sided pain; in the case by Broeske et al. (34) the frequency of attacks was low; both patients reported in the paper by Foerderreuther et al. (37) did not present autonomic symptoms associated with the headache.
In other cases, pharmacological responsiveness is a matter of question. As far as CPH or
HC are concerned, indomethacin response is a crucial point. Antonaci et al. (57) proposed the
‘Indotest’ with a single dose of parenteral indomethacin as a standard diagnostic
criterion for these headaches. This test was not performed in any of the papers
reviewed; moreover, the effect of the drug was not the same in all cases, because in
some of them a higher dose than 150 mg (as stated by IHS criteria for CPH) was needed to
achieve a therapeutic result. In HC, diagnostic dosage of indomethacin was recently
stated as 150 mg (20,
58). In a clinical
review of the first 18 published cases, Bordini et al. (7) report doses of 150 mg or less; Newman
et al. (59) report 10
cases in which HCs were resolved with doses of 75–200 mg, and in a recent report on 26
CPH and HC cases (48)
the initial doses ranged between 25 and 150 mg/day. In one of the papers considered
(35), Sjaastad
suggested that continuous need of high indomethacin dosages both in CPH and HC could be
regarded as a sign of an associated serious disease. In fact, this was the case in five
of the 22 CPH patients [31, 35,
37 (cases A and
B), 40] and three of
the nine HC patients [35, 45
(cases B and C)]. Finally, in the paper by Medina (1980) (23), and in the one by Bonazzi et al.
(32) indomethacin
was ineffective [Medina (1980) did not report the dosage, Bonazzi tried indomethacin 150
mg/day]
When indomethacin is totally ineffective, the possibility of another diagnosis cannot be ruled out. For example, in the original paper of 1980, Medina (23) diagnosed the case as cluster headache; in the paper of 1992 (27) the same author revised the diagnosis to CPH. Due to the high frequency of the attacks, a diagnostic hypothesis of SUNCT syndrome could be advanced. Nevertheless, the reported duration of the attacks (5 to 6 min) does not fit the Goadsby and Lipton criteria for SUNCT syndrome and is more in accordance with an ‘atypical’ CPH.
Regarding hemicrania continua, in the case reported by Evans (46), baseline headache and autonomic symptoms are not mentioned; furthermore, indomethacin was tried with amitryptiline and verapamil, and the effect of this association was not absolute.
Some cases of idiopathic CPH and HC were reported as responsive to NSAIDs other than indomethacin, such as piroxicam-β-cyclodextrin, ibuprofen, rofecoxib and celecoxib (8–13). In our series, many drugs, such as ASA, paracetamol, prednisone and methisergide were used, but generally they were of little or no value, except in cases in which they were used for the associated disease (i.e. methilprednisolone for vasculitis). Further, there were two cases of CPH-like headache in which sumatriptan was effective (30, 31).
Here, we also mention a paper by De Angelis and Payne (60) concerning a case of lymphomatous meningitis associated with atypical cluster headache, in which a case of hemicrania continua is clearly recognizable (61). This article will be analysed in another paper on cluster-like headache.
Recently, D’Alessio et al. presented a poster (62) describing two cases labelled as ‘indomethacin-responsive hemicrania’, one in association with an extracranial venous malformation and another in association with a subcutaneous angiolipoma. The first case reported strictly unilateral, right-sided, dull and continuous pain, worsened by frequent exacerbations (4–5 daily), lasting up to 5 min, with autonomic symptoms. Indomethacin was absolutely effective at 50 mg daily. The second case presented bilateral pain with nausea, photo- and phonophobia, responsive to indomethacin 200 mg daily. The diagnosis of the first case is, in fact, questionable, ranging from paroxysmal hemicrania (with continuous background pain) to hemicrania continua (with frequent and severe exacerbations of the pain). The second case does not fit the diagnostic criteria for hemicrania continua because of bilateral pain. We have not included these cases in the review because of the lack of a definite diagnosis by the authors.
On the contrary, all reported cases described as SUNCT syndrome fit well with diagnostic criteria of this headache syndrome, except Penart and ter Bergh cases (52, 54), because of the longer duration of the attacks. However, some observations describe otherwise genuine cases of SUNCT with attacks lasting up to 300 s (15).
Another interesting problem is the causal relationship between the associated pathology and the headache, or the possibility of a coincidental association. To put forward such hypotheses in individual cases, some criteria have to be considered:
Close temporal relationship between the associated disease and the onset of pain.
Side concordance between the unilateral pain and the lesion, if localized.
Surgical remission, if the patient was operated on, or prompt remission after aetiological medical therapy, if indicated, without need of constant indomethacin administration.
Prolonged post-treatment follow-up, in order to exclude a relapse of the headache attacks or improvement due to spontaneous remission.
In the cases reviewed, a close temporal relationship is clearly recognizable only in cases in which an acute illness was diagnosed (i.e. stroke, herpes zoster, surgical lesion, vasculitis, head trauma). In other cases, i.e. where a space-occupying lesion is present, it is likely that the lesion preceded the headache, but it is impossible to argue a direct causal relationship only on this basis. In these cases, it is important to pay attention to the side concordance and to the treatment outcome.
In Tables 1, 2 and 3 we have reported the side concordance between the lesion and the pain in all case reports examined. In one CPH case, the concordance was not applicable [28 (case A)] because of the reported bilateral pain (case not fulfilling IHS criteria); in other cases, because the patient was suffering from an unlocalized disease such as thrombocytaemia (26), vasculitis [27 (case A), 37 (case A)], intracranial hypertension (31), HIV infection (44, 53), not localized trauma [45 (cases A, B and D), 46], median intracranial lesions (33) or bone malformations (54, 55).
A well-defined post-treatment remission, followed by a prolonged follow-up, is present
only in the cases by Giacovazzo (30), Gatzonis (36, two cases) and Milanta (40)
Concerning HC cases, we underline the attempts to treat the majority of patients with a wide series of drugs, mostly ineffective, before a correct diagnosis was established. In most cases, the headache was triggered by a minor head injury, so a close temporal relationship is recognizable, but an aetiological treatment was not applicable. Complete relief of the headache, followed by a sufficient follow-up without need of further indomethacin intake, is reported only in the case by Antonaci et al. (42). In the Sjaastad (35) case, the treatment of the associated disease was followed by only partial clinical remission; in the Meckling (43) case, the effect of medical treatment was good, but the follow-up is lacking. In other cases, prolonged indomethacin administration (sometimes at high doses) was needed.
In SUNCT cases, a well-defined temporal relationship between the associate disease and the onset of pain is generally questionable, except in the case by Penart (52), in which a spontaneous remission of pain is also described. Medical improvement was observed only in the patient reported by Morís et al. (55), with a 2-year follow-up.
Taking the above into consideration, we believe that, in most of our reported cases, it is difficult to establish a well-defined causal relationship between the associated disorder and the headache. Except in the specifically mentioned cases, the most probable hypothesis is a coincidental association between an established case of TAC (sometimes with atypical symptoms) and a lesion.
An important question is if these observations could help elucidate the pathogenesis of TACs, i.e. by stressing the importance of a specific localization of the associated and perhaps causal lesion. The aim of the present study was to present an almost complete review of the literature. However, because of the limited number of cases, we prefer not to draw definite conclusions. Our objective, therefore, was to focus attention on the constant involvement of the posterior fossa by the lesions associated with SUNCT syndrome, and on the anterior localization of the lesion, in the vicinity of the midline, or within cavernous sinus in some cases of CPH-like headache.
We also stress the importance of performing a full neuroradiological investigation in cases of TACs that are in some ways atypical, i.e. older age at onset, clinical features (bilateral pain, side-shift, duration of the attacks) and/or, in CPH or HC, atypical response to indomethacin (ineffectiveness or need for higher doses than usual to achieve a therapeutic result).
Final note
After the temporal limits decided on for inclusion of cases in the review (June 2001), but before the publication of the paper, we read of one new case report of hemicrania continua with an underlying occult lung cancer (63), and two cases of SUNCT syndrome in association with prolactinomas (64). These case reports are only quoted and therefore not included in the discussion.