
Abstract
Headache research in Denmark started with the description in 1949 by Dalsgaard-Nielsen of the percutaneous nitroglycerin test. In 1976 Jes Olesen started The Copenhagen Acute Headache Clinic and from that time modern headache research began in Denmark. Specific changes in regional cerebral blood flow during attacks of migraine with aura, spreading oligaemia, were described for the first time in 1980. The first headache classification with operational diagnostic criteria was published in 1988 and used in a Danish population study from 1989. The lifetime prevalence of migraine was 8% in men and 25% in women. An intravenous nitroglycerin test was introduced in 1989 and has been developed as an experimental headache model. In 1993 it was suggested by Jes Olesen et al. that NO supersensitivity could be a possible molecular mechanism of migraine pain. Recent genetic studies have supported the distinction between migraine with aura and migraine without aura. From the middle of the 1980s the pathophysiology of tension-type headache has been investigated and recent results indicate central sensitization in patients with chronic tension-type headache.
Early headache research in Denmark
Headache research in Denmark started with the description by Thorvald Dalsgaard-Nielsen (1896–1975) in 1949 of the percutaneous nitroglycerin test (1, 2). In this test migraine attacks were provoked with ointment of nitroglycerin, which was applied to the forehead and to the temporal region (2). In controls the threshold for headache (6 mg) was higher than in migraine patients (1–2 mg) (2). This observation was confirmed in 1970 in a double-blind clinical trial where migraine patients reacted with headache significantly more often (19/25) than other headache patients (8/25) after nitroglycerin 6 mg (3). Later nitroglycerin-induced headache and nitroglycerin-induced migraine attacks were developed as an experimental headache model (see below). Dalsgaard-Nielsen described in 1957 his hypnocephalea clinostatica and suggested it be treated with ergotamine at bedtime (4). Later he studied serotonin in blood platelets (5) and the effect of the amine-depleting drug, reserpine, in migraine patients (6).
Axel Klee (1933–1982), in his 1968 thesis (7), describes in detail the symptoms of 150 severely afflicted migraine patients admitted by the Disablement Insurance Tribunal to the Department of Neurology, University Hospital, Copenhagen. A correlation between severity and number of symptoms was found.
Until approximately 1980 the theory of the pathophysiology of migraine was based on H.G. Wolff's thinking (8): ‘The neurological symptoms are due to cerebral vasospasms and the headache is caused by a subsequent reactive hyperaemia with dilatation of the arteries’.
The major precondition for the progress in pathophysiological investigations in migraine was the pioneering development of measurements of regional cerebral blood flow (rCBF) by Niels A. Lassen (1926–1997, 9–14). In addition, Lassen also developed methods for measuring local blood flow with the 133Xenon wash-out method (15, 16) which were used for measuring extracranial blood flow (see below).
Jes Olesen (1941-), who had written a thesis on regional cerebral blood flow (rCBF, 17) under the supervision of Niels A. Lassen and Erik Skinh⊘j (1918–1983), started in 1976 The Copenhagen Acute Headache Clinic at the University Hospital in Copenhagen (18), where patients could admit themselves with any acute headache. From this clinic, headache patients were recruited for pathophysiological research and randomized clinical trials. In addition, young physicians, working in this clinic, were also quite naturally recruited for headache research. Later the headache research programme moved to the County of Copenhagen and is now at the Glostrup Hospital, University of Copenhagen.
Skinh⊘j had in 1972 shown decreased rCBF and increased spinal lactate during migraine attacks (19) and these findings supported Wolff's theory of cerebral anoxia as the cause of the aura symptoms (8). In patients in whom carotid angiography triggered a migraine attack with aura, studied with a multidetector scintillation camera with 254 channels (12), Jes Olesen et al. reported, in the early 1980s, that the decrease in rCBF did not reach the ischaemic threshold and that the decrease in rCBF spread slowly from behind forwards over the cerebral hemisphere, not respecting the territories of the larger cerebral arteries (see Fig. 1) (20, 21). The speed of the spreading oligemia was 2–3 mm/min, the same speed that had been observed for the neurophysiological phenomenon, Spreading Depression of Leao (22). Based on Lasley's calculations of the speed of progression of the process in the occipital cortex responsible for scintillating scotomas, it had previously been proposed (23) that the primary process underlying the migraine aura could be Leao's Spreading Depression (SD). Against this hypothesis, however, was the fact that SD increased CBF (22).
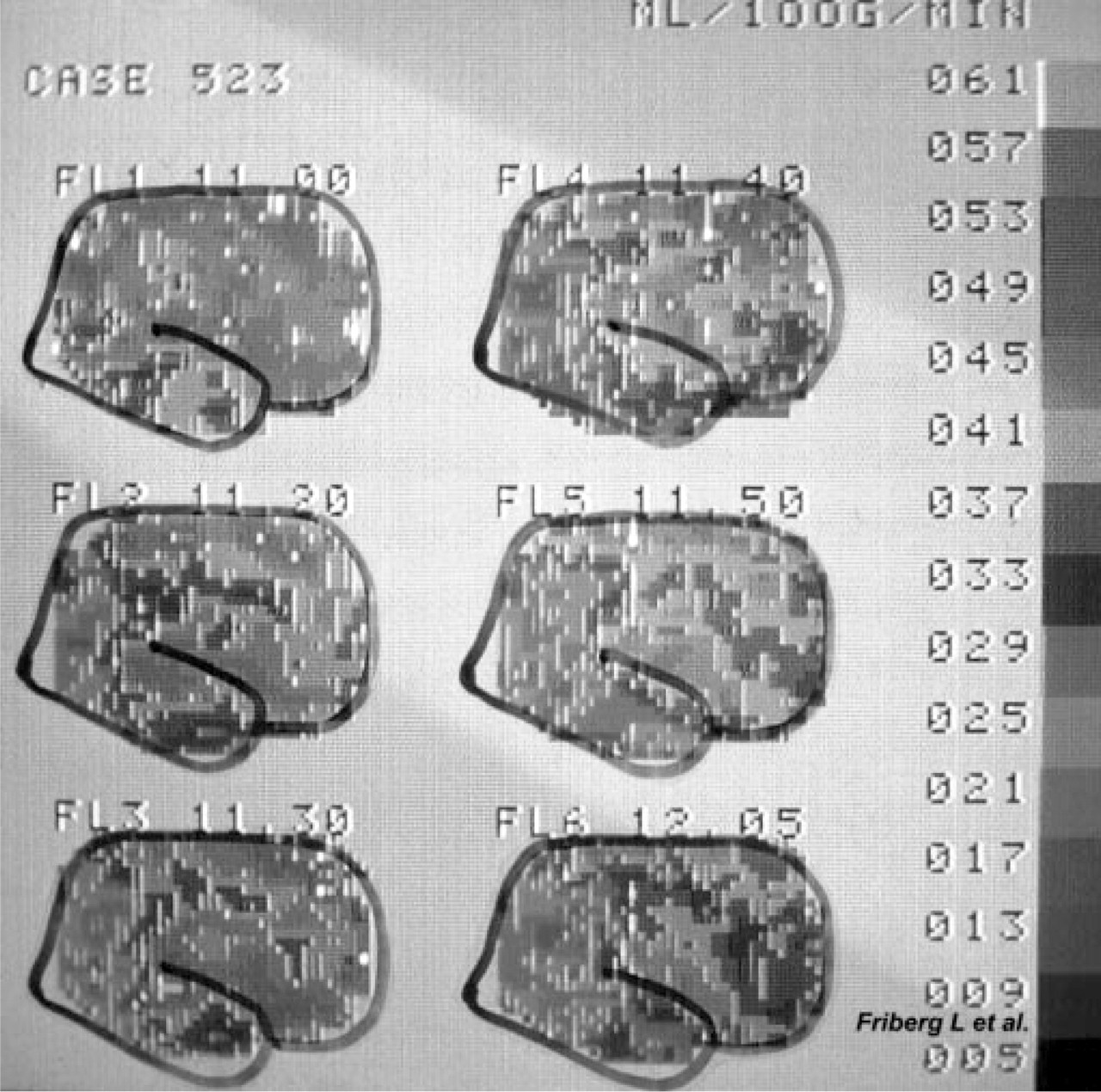
Spreading oligaemia in an attack of migraine with aura triggered by carotid angiography. The patient was examined with repeated measurements, with 10–20-min intervals, of regional cerebral blood flow (rCBF) with a multidetector scintillation camera with 254 channels after intracarotid injections of 133Xenon (12). Note the slow spread of decreased rCBF from behind forwards over the right cerebral hemisphere (courtesy of Lars Friberg).
Inspired by the rCBF changes observed in connection with the aura phase, Martin Lauritzen could now, in rat studies, show that after an initial hyperaemia, as found previously, a decrease in rCBF of 20% was observed for up to 1 h (24). The combination of the changes in rCBF during the aura phase and the rat experiment demonstrating prolonged oligaemia, resulted in world-wide acceptance of SD as the most likely candidate for the underlying pathophysiological event causing the aura phase. In 1987 Martin Lauritzen wrote his thesis on the relationship between migraine and SD (22). In the first rCBF studies using the intracarotid method (20, 21) repeated examinations were extended until 0.5–1 h into the headache phase, at which time rCBF remained depressed. With the atraumatic SPECT method with 133Xenon inhalation (13) it was shown in six patients with spontaneous attacks of migraine with aura that an initial posterior hypoperfusion was followed after 3–8 h by a hyperperfusion in the previous hypoperfused areas (25). There was no temporal relationship between the changes in rCBF and headache and the hyperperfusion often extended beyond the duration of the clinical headache (25, 26). Before and during attacks of migraine without aura no changes in rCBF were observed in attacks provoked by red wine or specific food (27), a finding later confirmed during spontaneous attacks of migraine without aura studied with SPECT (28). For a review of rCBF changes during migraine attacks, see (26, 29).
In 1962 an ad hoc committee had suggested criteria for headache classification (30). The criteria were, however, so non-specific that they were not suitable for headache research. After the founding of the International Headache Society in 1984 a new classification for headaches was suggested on a Danish initiative and this international teamwork, with Jes Olesen as chairman of the committee, resulted in the first headache classification with operational diagnostic criteria in 1988 (31).
Many ergotamine abusers consulted the Copenhagen Acute Headache Clinic and it was shown that these patients had sub-clinical ergotism as measured with strain gauge plethysmography (32). It was demonstrated in a thesis by Tfelt-Hansen in 1986 that a single dose of ergotamine had a prolonged effect on peripheral arteries, at least 24 h (33).
Extracranial blood flow was investigated with the 133Xenon wash-out technique (15, 16) in migraine patients recruited from the Copenhagen Acute Headache Clinic. As shown in the thesis by Kai Jensen in 1993, temporal muscle blood flow and subcutaneous blood flow were found unchanged during migraine attacks (34), thereby challenging the traditional concept of extracranial vasodilation based on measurements of arterial pulsation (8, 35).
Based on the Glostrup Population Study the epidemiology of headache, using the new diagnostic criteria of IHS (31), was studied from 1989. This resulted in a thesis in 1995 on the epidemiology of headache by Birthe Krogh Rasmussen (36). The lifetime prevalence of migraine was 8% in men and 25% in women (36).
The reactions of the temporal artery during migraine attacks had previously been studied extensively, by recording the pulsations, by Wolff's group (8, 35). From 1986 high-frequency ultrasound equipment, originally developed for dermatological examination, was used for measuring directly the diameter of the temporal artery; it was shown in 1990 that the artery is dilated relatively on the headache side during a migraine attack, although only to a minor extent (37). In 1991 it was shown with transcranial Doppler and simultaneous rCBF measurements that the middle cerebral artery is dilated on the headache side and that this dilatation is reversed by sumatriptan, most likely due to a constrictive effect of the drug (38). These two papers have contributed to the trend for concentration on intracranial vessels as the pain source in migraine.
In 1989 it was shown that intravenous (i.v.) nitroglycerin induced a dose-dependent and reproducible headache response in healthy volunteers (39) and i.v. nitroglycerin was further developed as an experimental headache model. It was suggested in 1993 by Jes Olesen et al. that NO could be involved in the pathogenesis of migraine pain (40), for a review see (41). It was shown in Lars Lykke Thomsen's thesis in 1997 that migraine patients are more sensitive to NTG than controls and that NTG induces genuine migraine attacks in migraine patients (42). The NTG-induced headache is effectively treated with sumatriptan and this experimental headache has been suggested as a human model for development of migraine drugs (43).
A major point in the headache classification, argued from the Danish members and scientifically based on the difference in rCBF changes, see above, was the separation of migraine into two major types: migraine with aura and migraine without aura (31). This distinction allowed Michael Bj⊘rn Russell to conclude in his thesis from 1997 that migraine without aura depends on both genetic and environmental factors, whereas migraine with aura mainly depends on genetic factors (44). Later studies in patients recruited from the Danish Twin Registry has confirmed and expanded these results (45, 46). For genetic epidemiology of cluster headache and chronic tension-type headache, see (47).
Tension-type headache
Whereas migraine, especially migraine with aura, always has been a fascinating neurological disease to study, the even more common tension-type headache has been a somewhat scientific stepchild. From the middle of the 1980s tension-type headache patients, especially in its chronic form, have been investigated, first with standarized palpation of pericranial muscles and tendon insertions (48), and later with examination of pain physiology in these patients. This resulted in three theses on tension-type headache in 1999. Rigmor Jensen described, on the basis of the Population Study in Glostrup, the epidemiology of tension-type headache, its relation to muscle tenderness, EMG activity and temporomandibular dysfunction (49). Michael Langemark examined 50 patients with severe chronic tension-type headache with an extensive test battery. He observed increased muscular tenderness but normal blood flow and only marginally increased EMG activity. Pain perception thresholds were decreased (50). Lars Bendtsen used an instrument for controlling the palpation pressure and demonstrated a qualitatively changed stimulus-response function in tender muscles in patients with chronic tension-type headache, indicating central sensitization (51). Recently, it was shown that NO synthase inhibition is moderately effective in the treatment of chronic tension-type headache (52).