
Abstract
Introduction:
Congenital heart disease is one of the most common congenital disorders, affecting between 0.8% and 1.2% of live births worldwide. The treatment of children with congenital heart defects is highly specialized and includes, among others, surgical treatment as the first-choice approach and postoperative care in intensive care units. The aim of this review is to explore nursing care plans for post-cardiac surgery children during their stay in intensive care units.
Methods:
An integrative review was performed to obtain articles from the online databases SCOPUS, ScienceDirect, Scielo, PubMed, EMBASE, and Redalyc. The synthesis of information was performed based on diagnoses and interventions. In addition, complications and associated factors were identified.
Results:
Nursing diagnoses and interventions focus on problem-centered care to respond to cardiovascular and ventilatory needs, sedation and analgesia, infection control, and nutrition. The main complications identified were increased time on mechanical ventilation, postoperative infection, renal failure, and mortality. Complications were associated with intrinsic conditions such as age, gender, or type of malformation and clinical and procedural conditions such as extracorporeal circulation, mechanical ventilation, or higher postoperative risk index.
Discussion:
This review identified problem-focused nursing diagnoses and interventions with a strong focus on the physiological conditions of the child. Although the results of this study show the conceptual level of nurses for specialized care, it denotes the need to complement the nursing process through diagnoses and interventions that promote the transversality of care beyond the problem-centered approach based on the possibilities of the response of the child and the family.
INTRODUCTION
Congenital heart diseases (CHDs) are structural abnormalities of the heart and/or great vessels present at birth. They are one of the most common congenital disorders and affect between 0.8% and 1.2% of live births worldwide. In 2017, the incidence rate of CHD was 17.9/1,000, and the most common subtypes were ventricular septal defect and atrial septal defect. However, other entities such as single ventricle and single ventricular pathway congenital heart anomalies, critical malformations of great vessels, congenital valvular heart disease, and patent ductus arteriosus integrate into the spectrum of heart disease affecting the infant population, causing a mortality rate of 3.9 per 100,000 inhabitants, mainly in children under 5 years of age (Wu et al., 2020).
Treating children with congenital heart defects is highly specialized and includes imaging, surgical, interventional, and supportive care techniques. The management of CHD begins before birth and involves the organization of perinatal care. Surgical treatment depends on complex intracardiac procedures, and it is currently the first-choice approach with acceptable risk and satisfactory long-term results. In most cases, these procedures require opening at least the right atrium and support of extracorporeal circulation (ECC; Seghaye, 2017).
Consequently, postoperative care requires hospitalization in intensive care units because of low cardiac output, arrhythmias, vasoactive instability, sedation, and pain relief management. In addition, the postoperative stage requires invasive cardiovascular and respiratory monitoring, fluid balance monitoring, venous support, inotropic support, afterload reduction, and pulmonary vasodilators (Seghaye, 2017).
In this context, pediatric cardiac critical care by nursing professionals is essential to achieve positive outcomes and depends on highly specialized knowledge. The breadth of interventions by an interdisciplinary team in intensive care units focuses on cardiopulmonary stabilization and management of unstable hemodynamics, continuous critical thinking and decision-making, and intensive intervention (Peterson & Evangelista, 2017). In this order, nursing care has become a subspecialty that requires knowledge of cardiac anatomy and physiology, the effects of mechanical ventilation, mechanical circulatory support, and vasoactive drugs. In addition, the nurses need to develop skills in physical examination of the child, interpretation of hemodynamic and laboratory data, active participation in patient rounds, communication, meticulous care of invasive devices, and support of families and caregivers (Jones & Tucker, 2016).
In this sense, to integrate this combination of knowledge and establish comprehensive care through a nursing process, different diagnostic systems have been developed, the most widely used of which are the North American Nursing Diagnosis Association (NANDA) system and its European counterpart developed by the International Council of Nursing Practice. NANDA defines a nursing diagnosis as a clinical judgment about the experiences or responses of the individual, family, or community, providing the basis for establishing interventions and evaluating outcomes (Chiffi & Zanotti, 2015).
The above definition affirms that the nursing diagnosis goes beyond a clinical judgment and integrates social and humanistic components framed in a behavioral or attitudinal description of the individual that goes beyond the correlation between cause and effect. Consequently, nursing diagnosis and interventions involve methods of care aimed at promoting individuals and communities to their maximum potential based on their actual state of health (Chiffi & Zanotti, 2015).
The care of children undergoing cardiac surgery in intensive care units requires a conscious and quality nursing process that encompasses the full spectrum of the discipline. Therefore, recognizing nursing interventions under taxonomic principles to broaden knowledge and make visible the risk and protective factors associated with established interventions is fundamental. Furthermore, discussing and promoting nursing approaches that respond to the needs of the child’s macroecology is a priority in providing comprehensive and humanized care.
METHODS
Design and Aims
An integrative review, according to Whittemore and Knaf (2005) was conducted to explore nursing care plans for post-cardiac surgery children during their stay in intensive care units. The literature synthesis provides an overview of nursing care by identifying diagnoses and interventions. In addition, complications and associated factors are presented.
Search Methods
Research articles were identified in the SCOPUS, ScienceDirect, Scielo, PubMed, EMBASE, and Redalyc databases using the search descriptors (DeCS–MeSH– EMTREE) in Spanish, English, and Portuguese. Appendix A in the supplementary material (available at http://links.lww.com/JPSN/A98) provides an example of the search strategy performed for PubMed. We also hand-searched the reference lists of the articles included in the review.
Inclusion Criteria
The following inclusion criteria will be defined: (a) cross-sectional, experimental, or quasi-experimental studies describing nursing care plans in children after cardiac surgery during their stay in intensive care units; (b) studies summarizing the outcome at the discharge of children hospitalized for cardiac surgery in intensive care units associated with the nursing outcomes proposed; (c) studies presenting the complications identified for nursing professionals during the attention process; and (d) studies in English, Spanish, and Portuguese, published between 2005 and 2020.
Exclusion Criteria
The following exclusion criteria will be defined: (a) studies that included intervention outcomes from other professions/individuals that did not allow identification of outcomes associated with nursing practice; (b) articles that do not report limitations, letters to the editor, and short communications; (c) theoretical articles; (d) articles presenting nonvalidated assessment tools; (e) gray literature; and (f) quality criteria on the Newcastle–Ottawa Scale below 5.
Search Outcomes
A total of 275 articles were retrieved from the database search. Twenty duplicate articles were removed. The title and abstracts of 255 articles were read. Two hundred twenty-three articles were eliminated according to the inclusion and exclusion criteria. The full text of the remaining 33 articles was reviewed. Nineteen articles were selected according to the inclusion and exclusion criteria. Sixteen of the studies were observational, and three were experimental. Seven studies included comparison groups. The PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses; Page et al., 2021) flowchart shows the search process in Figure 1 in the supplementary material (available at http://links.lww.com/JPSN/A99).
Quality Appraisal
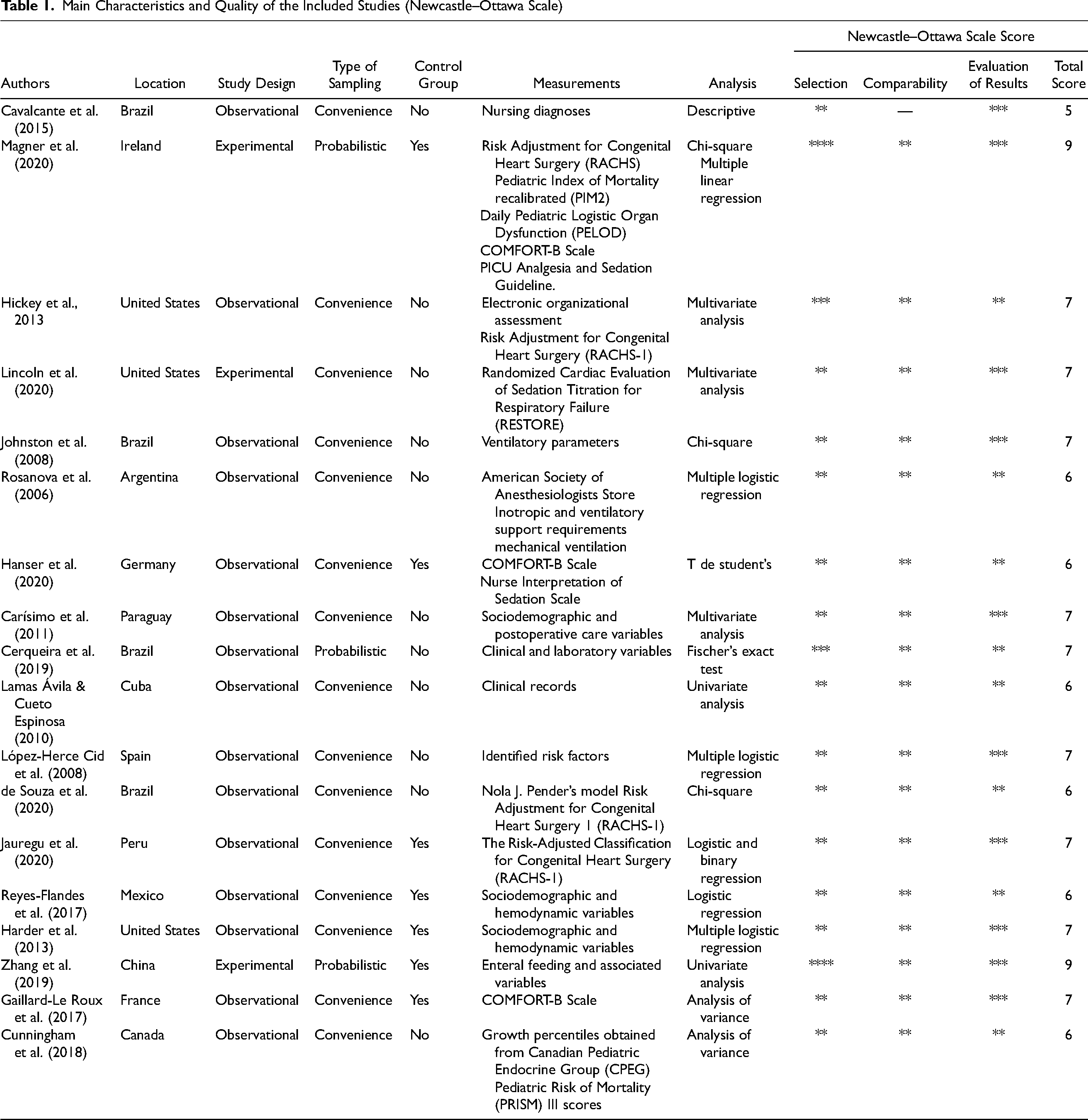
The quality of the articles was assessed using the Newcastle–Ottawa Scale, which establishes and rates the level of evidence of the articles by the number of stars according to three criteria: selection, comparability, and results. An article was considered high quality if it had between 7 and 9 stars, moderate if it had between 5 and 6 stars, and poor if it had between 1 and 4 stars (Table 1). Articles with scores above 5 were included in this review. According to the quality criteria of the Newcastle–Ottawa Scale, 10.5% of the reports obtained a high-quality score of 8 or more, and 89.5% obtained a score between 5 and 7.
Main Characteristics and Quality of the Included Studies (Newcastle–Ottawa Scale)
Data Analysis
A thematic analysis was conducted to identify the key results of the included articles. The analysis was carried out manually per this review’s objectives by tabulating each study’s methodology and results. The lead author conducted the thematic analysis, and the two co-researchers checked the analysis to reduce bias. The analysis focused on nursing diagnoses, interventions, and outcomes, including quantitative data reporting statistical tests and significance values.
RESULTS
Two main themes were identified: diagnoses and nursing interventions, and potential complications and risk factors for children undergoing cardiac surgery during intensive care unit stay.
Nursing Diagnoses and Interventions for the Care of Children in Intensive Care Units Post-Cardiac Surgery
Cavalcante et al. (2015) reported on the proposed NANDA nursing diagnoses for nursing care based on assessing a post-cardiac surgery child with their defining characteristics and related factors (see Table 2).
Nursing Diagnoses
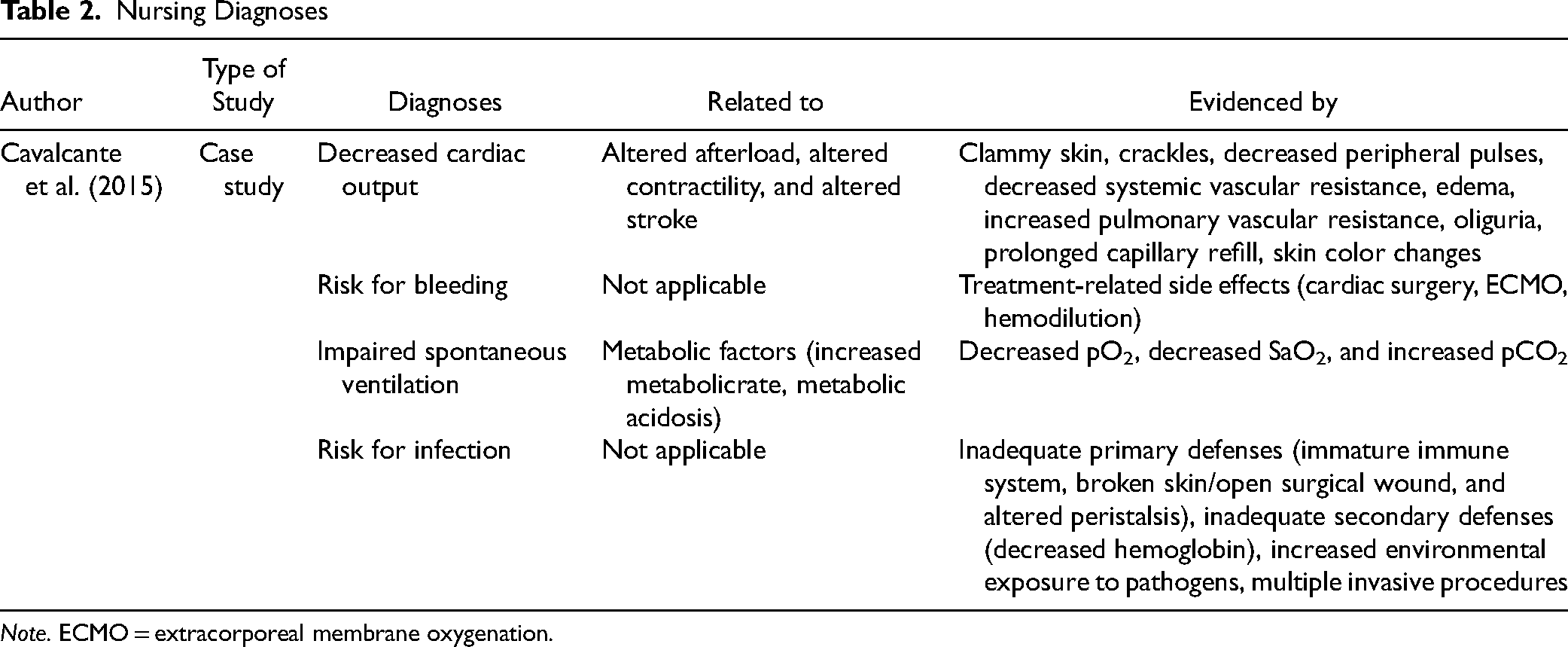
Note. ECMO = extracorporeal membrane oxygenation.
Eight articles reported on interventions and their detailing of activities in children post-cardiac surgery. Four studies identified the importance of a nurse-led analgesia and sedation protocol showing a decrease in the use of these medications. Magner et al. (2020) evaluated 125 children in two groups, 61 children before and 64 after introducing the analgesia and sedation regimen showing decreased use of paracetamol, morphine, and clonidine. Lincoln et al. (2020) collected data from 1,243 post-cardiac surgery pediatric patients in discontinuous pre- and post-intervention periods, identifying decreased use of sedation in the follow-up periods. Hanser et al. (2020) assessed children post-cardiac surgery in two pre- and post-protocol implementation periods, showing decreased peak doses of midazolam and morphine administration with acceptable sedation parameters assessed with the Nurse Interpretation of Sedation Scale and CONFORT B scale. Finally, Gaillard-Le Roux et al. (2017) included 235 post-cardiac surgery patients, 97 in an intervention group and 97 controls, showing statistically significant differences in decreased sedation use with protocol implementation (p = .02) according to sedation levels.
Three studies evaluated adherence to and implementation of feeding protocols for the care of children post-cardiac surgery. Newcombe and Fry-Bowers (2017) identified the importance and impact on anthropometric measures of implementing an early nursing-led feeding protocol with follow-up at birth, surgery, and discharge. Zhang et al. (2019) assessed 59 infants divided into two groups: 30 intervention and 29 control infants, applying a high-energy nutrition protocol for weight gain, showing less weight loss than infants receiving standard formula.
Cunningham et al. (2018) reported on adherence to a feeding protocol and the importance of this in reducing hospital stay, time to initiation of nutritional support, time without nutrition, mortality rates, and reduction of feeding interruption in 142 pediatric intensive care unit (PICU) admissions for cardiac surgery. See nursing interventions in Table 3.
Nursing Interventions: Main Results and Proposed Nursing Care
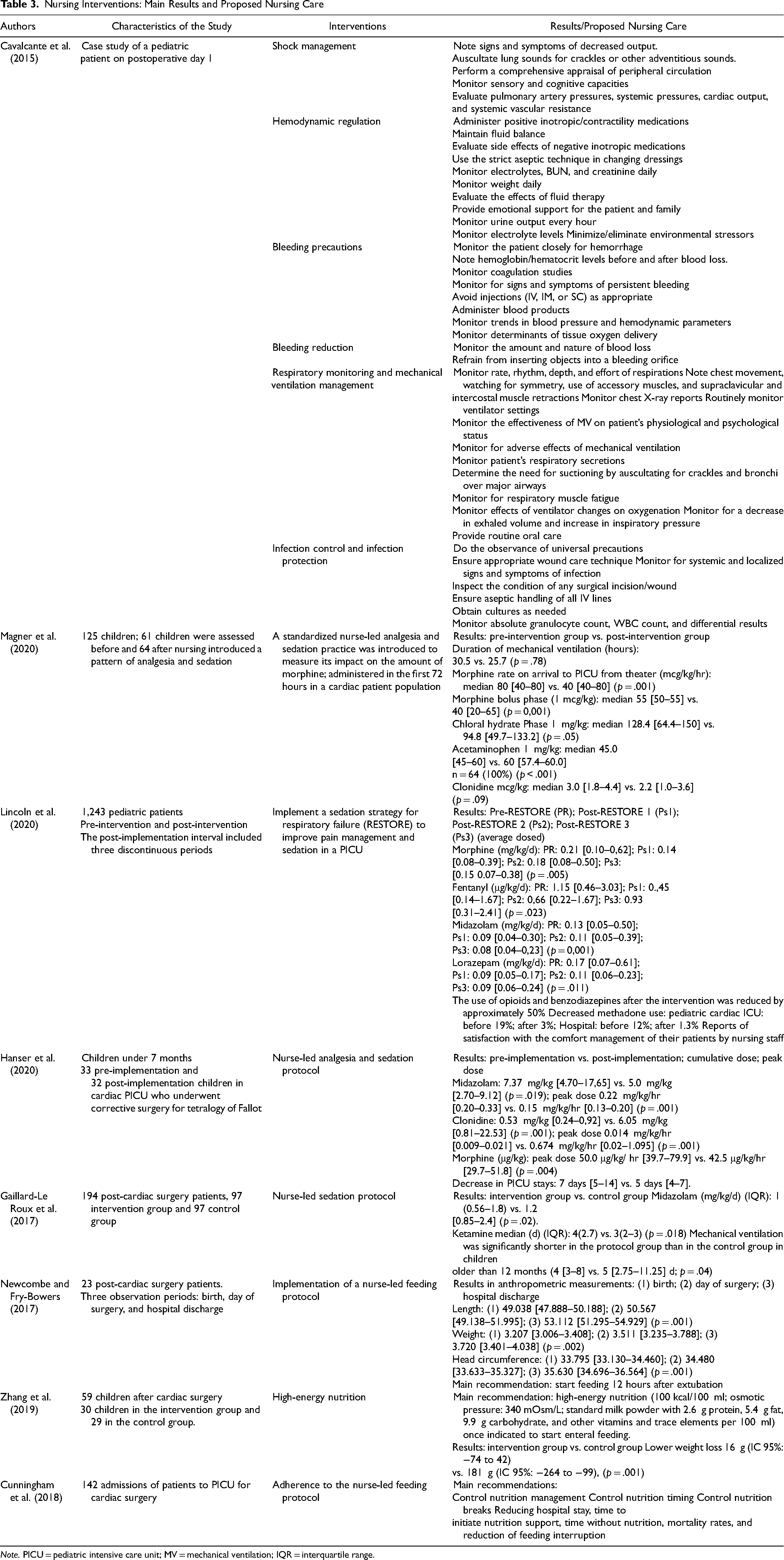
Note. PICU = pediatric intensive care unit; MV = mechanical ventilation; IQR = interquartile range.
Potential Complications and Risk Factors for Children Undergoing Cardiac Surgery During Intensive Care Unit Stay
Eleven articles reported postsurgical complications in children with CHD.
Ventilatory Complications and Associated Factors
Johnston et al. (2008) evaluated mechanical extubation failures by identifying the ventilatory parameters 1 hour before and after the procedure in 58 children under cardiac surgery. The study compared patients with extubation failure (19%) and patients with successful extubation (81%). The characteristics of the individual patients, their pathologies, and the parameters ventilatory with oxygen index and blood oxygen pressure influenced the success rate.
López-Herce Cid et al. (2008) studied postoperative factors influencing the prolongation of mechanical ventilation in 59 children aged 2 months to 14 years who had undergone cardiac surgery. Factors evidenced during the 24 hours postprocedure associated with mechanical ventilation were age, extrapulmonary complications, airway disturbances, nitric oxide treatment, sedation, and administration of continuous infusion muscle relaxants. In addition, the study showed clinical outcomes of importance to risk factors for mechanical ventilation. Risk factors >7 days of mechanical ventilation presented the same clinically significant variables as in >3 days, with the difference that the p value presented a lower strength of association than the evidence of risk. Consequently, it was found that weight less than 7 kg increases the presence of extrapulmonary complications in the PICU, behaving as a predictive factor for the increased hospital stay, with ventilation requirements >3 days in 82.8% of the cases and >7 days in 87.9% (López-Herce Cid et al., 2008).
Infection
Three studies reported the prevalence of surgical and nonsurgical site infections and associated factors. The population characteristics associated with infection were age, underlying pathology, gender, weight, and history. Intervening variables influencing the presence of infection were days of PICU stay, inotropic requirements, mechanical ventilation, invasive techniques and devices such as ECC time, chest tube, and urinary catheter.
Acute Kidney Injury
Reyes-Flandes et al. (2017) studied the risk factors associated with acute kidney injury (AKI) in children undergoing cardiac surgery with ECC. The results showed that AKI is related to renal blood hypoperfusion, associated with different ischemia phenomena, loss of pulsatile flow, and the severe systemic inflammatory response provoked by ECC (greater than 140 minutes, OR = 8.84, CI [2.54, 30.72]). Consequently, 25.8% of patients who developed AKI were identified as dying during their PICU stay.
Mortality
The prevalence of mortality in children undergoing cardiac surgery ranged from 3% to 13.3%. Studies showed factors associated with organizational characteristics of PICU, high-risk assessment scores, complex CHD, and especially cyanotic heart disease: type of surgery (elective or emergency); mechanical ventilation, dialysis, and clinical variables such as age; arterial gas bicarbonate level; creatinine level; infants; potassium level; calcium level; 24-hour temperature and mean arterial pressure; neurological complications; total perfusion time exceeding 45 minutes; and nutritional status (Carísimo et al., 2011; da Silva et al., 2018; de Souza et al., 2020; Hickey et al., 2013; Lamas Ávila & Cueto Espinosa, 2010). Complications and associated factors are presented in Table 4.
Complications and Associated Factors
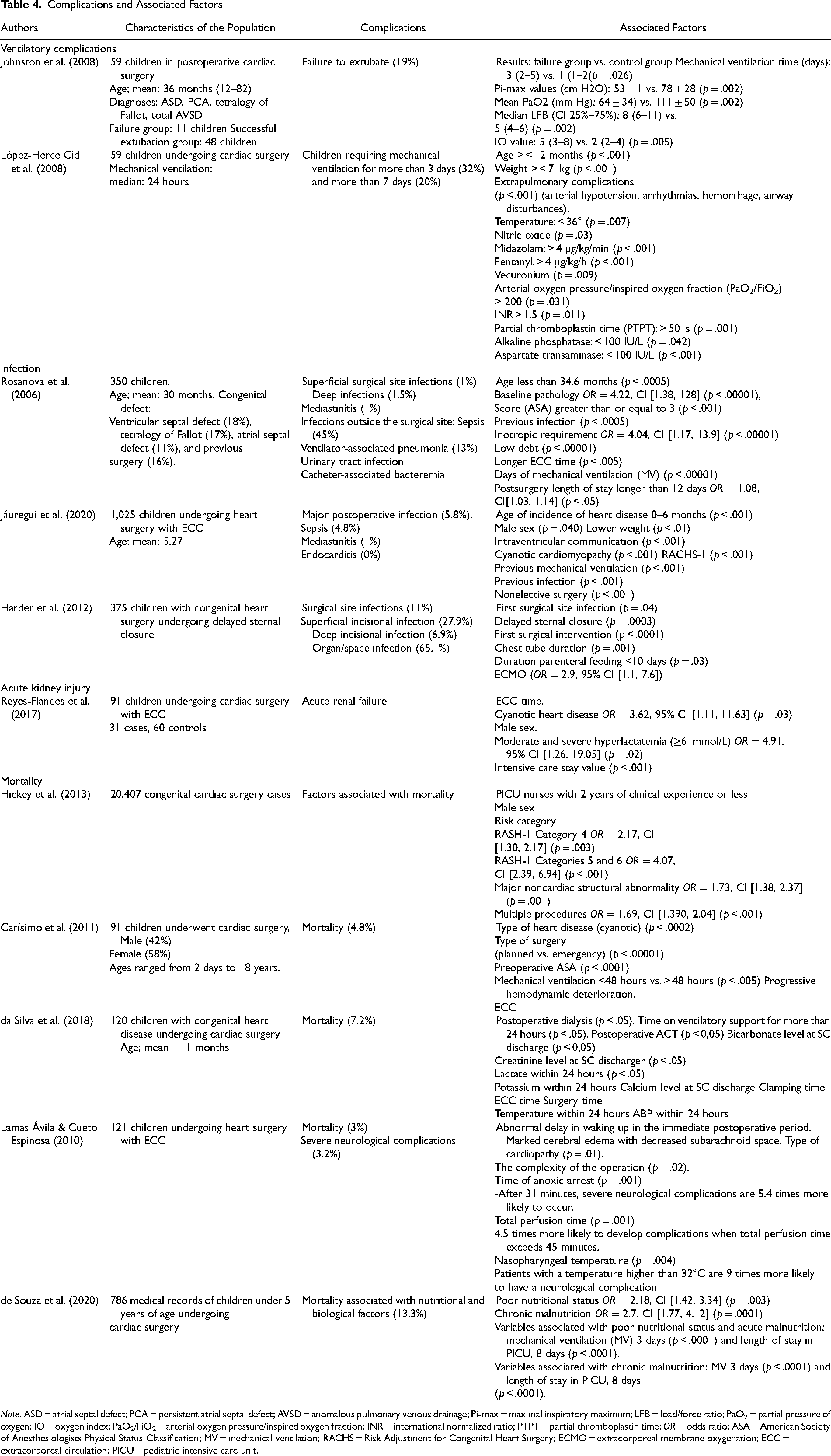
Note. ASD = atrial septal defect; PCA = persistent atrial septal defect; AVSD = anomalous pulmonary venous drainage; Pi-max = maximal inspiratory maximum; LFB = load/force ratio; PaO2 = partial pressure of oxygen; IO = oxygen index; PaO2/FiO2 = arterial oxygen pressure/inspired oxygen fraction; INR = international normalized ratio; PTPT = partial thromboplastin time; OR = odds ratio; ASA = American Society of Anesthesiologists Physical Status Classification; MV = mechanical ventilation; RACHS = Risk Adjustment for Congenital Heart Surgery; ECMO = extracorporeal membrane oxygenation; ECC = extracorporeal circulation; PICU = pediatric intensive care unit.
DISCUSSION
Based on a diagnostic taxonomy and interventions, this literature review explores nursing care plans for children exposed to cardiac surgery during their stay in intensive care units. It also proposed the identification of possible complications and associated factors as a conceptual basis for a comprehensive nursing care approach.
The nursing diagnoses identified in this review are mainly oriented toward the child’s care in the face of possible postsurgical alterations associated with decreased cardiac output, risk of bleeding, impaired spontaneous ventilation, and risk of infection. Consequently, the nursing interventions identified focused on clinical stabilization related to the preservation of hemodynamics, bleeding control, respiratory and ventilation monitoring, infection control and protection, analgesia, sedation, and nutrition.
This review showed that nurses caring for the child under complex health conditions develop a nursing process under problem-focused diagnoses and interventions. The assessment and control of signs and symptoms of shock, hemodynamic monitoring of circulatory, ventilatory and infectious variables, nursing interventions in pain management, and nutritional care have been highlighted in previous studies to identify early any alterations that the patient may present that lead to possible complications. In addition, the nursing care identified in this review represents a potential impact on the child’s recovery because of the exceptional attention to the management of advanced devices and the use of knowledge, guidelines, and protocols, which have repercussions on the reduction of hospital stay, the maintenance of relatively satisfactory anthropometric measurements in the postsurgical phase, pain management, and rehabilitation (Cavalcante et al., 2015; Newcombe & Fry-Bowers, 2017; Zheng et al., 2020).
Nevertheless, this review makes visible the strong focus of care oriented to the physiological needs of the child exposed to cardiac surgery. Understanding the integrity of nursing care and mentioning the meaning of nursing diagnosis, which is based on uniquely human response, are essential. Although the care of a child with cardiac pathology is immersed in several contexts of care (prehospital stage, surgery, postoperative care, hospital discharge, and home care), the intensive care nurse has a unique opportunity because of their level of conceptual depth to establish diagnoses and interventions that consider the macroecology of the child. In this sense, we consider it pertinent to establish nursing diagnoses that include activities aimed at holistic care with the integration of the family. Health promotion diagnoses and interventions in intensive care units favor a greater understanding of the health process of the intervened child, and by extension, better spiritual well-being increased coping capacity and greater knowledge of care guidelines on the part of the family and the child during the hospital stay and on discharge. Previous studies have identified the importance of family care in caring for PICU patients, with respectful and timely communication, emotional support, and education (Richards et al., 2017). In that sense, nursing professionals can play a pivotal role in establishing care using a multimodal approach through family integration and education, addressing their concerns and beliefs.
Concerning the postsurgical complications and related factors presented in this review, the findings accounted for the need to recognize the multidimensionality of care for children exposed to cardiac surgery in intensive care units. Furthermore, the related multisystemic complications highlight the importance of the transversality of care in all axes of care and the early identification of risk factors and associated complications. In this sense, a differentiated approach to care based on recognizing possible response mediators such as age, weight, and clinical and procedural variables is a priority to reduce the risk of complications. Under this premise, the nursing profession must be trained to recognize the patient’s hemodynamic parameters, their alterations, and the best approach to care (Hernández-Ruiz et al., 2022; Johnston et al., 2008; López-Herce Cid et al., 2008).
Nurse–patient interaction can identify these complications by assessing signs and symptoms related to hemodynamic instability, ventilation, infection, nutritional collapse, pain, and multiorgan damage. In addition, it is necessary to implement predictive scales for risk estimation validated in the pediatric population before the surgical procedure, especially during the first 24 hours postoperatively, because of the hemodynamic complexity of children undergoing surgery and their potential physiological alterations. Using scales can be beneficial for identifying and managing complications that may impact a possible reduction of hospital stay and the probability of death (Barker et al., 2010).
Although this review allowed us to identify diagnoses and interventions that reflect everyday nursing practice, as well as complications and associated factors that can be used as inputs for analysis to develop robust nursing plans, we believe that three significant challenges currently prevail in providing specialized care in intensive care units to the study population:
First, it is essential to recognize that the consolidation of evidence-based practice requires integration with the multidisciplinary work demanded by the complexity of care for children exposed to cardiac surgery. Specifically, it is necessary to define the individual scope of care actions and the collaborative problems resulting from the interdependence that exists in the care of children in complex healthcare settings, considering that there is no codified scientific framework for nursing knowledge as is often the case with medical diagnoses (Chiffi & Zanotti, 2015).
Second, it is essential to integrate into specialized care, diagnoses, and health promotion interventions as the essence of nursing care and comprehensive care mechanisms based on the recognition of the macroecology of the child, the assessment of the family support network, the resilience of children and caregivers, and the resources available to respond to patients’ needs by health care services.
Finally, it is essential to consolidate risk diagnoses that may become useful in planning nursing care to identify, assess, and manage possible complications that may affect the short- and long-term recovery of children exposed to cardiac surgery.
A few limitations of the integrative review methodology should be noted. First, the review included only peer-reviewed articles and was limited to those written in English and Spanish. Second, a librarian was not involved in developing the search strategy. Third, excluding gray literature and qualitative studies may have excluded valuable information from diagnoses related to health promotion and care strategies for families and caregivers.
CONCLUSION
This review identified problem-focused nursing diagnoses and interventions with a strong focus on the physiological conditions of the child in the postoperative period. There is a clear need to include diagnostics that promote aspects of family-centered care strategies to strengthen child and caregiver responsiveness. In addition, the complications and associated factors identified are input for recognizing the interdependence of care and applying risk diagnoses that lead to interventions to limit harm and promote early recovery.
Footnotes
Declaration of Conflicting Interests
The authors declare no conflict of interest
Funding
No funding was received for the completion of this review.
Supplemental Material
Supplemental digital content is available for this article. Direct URL citations are provided in the HTML and PDF versions of this article.