
Abstract
Introduction:
Gastrostomy tube (G-tube)-related problems, including dislodgements, are a frequent cause for emergency department (ED) visits in pediatric patients. We aimed to reduce G-tube-related ED visits at our children's hospital.
Methods:
An interprofessional team was formed including a family advisor, nurse practitioners, discharge coordinators, a pediatric surgeon, surgical residents, nurses, and quality improvement coaches. A number of interventions were put into place intended to improve caregiver preparation for G-tube placement, improved communication during the hospitalization, and postoperative interventions, including a new family education pathway and mechanical barriers to prevent tube dislodgment.
Results:
Overall, tube dislodgment accounted for 64% of G-tube-related ED visits: 14% in tubes less than 3 months from insertion and 86% in tubes older than 3 months. Our rate of ED visits for G-tube dislodgement had an initial baseline of nine visits per month. In the 3 years after the intervention, ED visits decreased from a median of 9.5 per month to 8 per month.
Discussion:
An interprofessional team implemented a quality improvement project that reduced G-tube-related ED visits in pediatric patients. Further efforts are needed to better understand the contributing drivers of G-tube-related ED visits and ways to minimize these events. Grant monies have been obtained from URMC Quality Institute and Vermont Oxford Network NICU Follow Thru Health Equity to continue our family-led quality improvement efforts.
INTRODUCTION
Case Study
For the fourth time in several months, a 12-month-old girl has come to the emergency department (ED) because of her gastrostomy tube (G-tube) either dislodging or malfunctioning. In past visits, it was noted that she presented with the G-tube not in the established tract and that her mother had not attempted to replace the G-tube at home. It is essential for this patient to have the G-tube in place to receive nutrition and lifesaving medications, as she has several chronic medical conditions preventing her from taking anything orally. At each ED presentation, the G-tube was easily replaced by the care team without complication. When inquiring on what the home plan was when the G-tube became dislodged, the patient's mother explained that she did not have any extra supplies at home and no one had showed her how to insert a new tube if one came out or became broken.
Background
G-tube placement in the pediatric population plays an important role in providing nutrition, hydration, and medication administration in many medically complex patients. Children requiring nutritional support through an enteral feeding tube include patients with oral aversion, swallowing difficulties, neurological deficits, failure to thrive, head and neck abnormalities, and chronic conditions, such as cardiac anomalies or cystic fibrosis. G-tube placement is common and is the third most common noncardiac inpatient surgical procedure performed in children in the United States (Behr et al., 2015). Complications associated with G-tube placement can range from minor (granulation tissue, minor infection, tube dysfunction) to serious (intraperitoneal leakage, bowel perforation, gastric outlet obstruction, and dislodgement). Severe complications range from 1% to 17%, depending on technique used, and minor complications including granulation tissue can occur in up to 68% of all cases (Arca et al., 2017; Correa et al., 2014; Goldberg et al., 2010). Several institutions have tracked emergency room visits 30 days after patient discharge from the hospital for G-tube-related problems and have found the revisit rate ranged from 8.6% to 20% (Cameron et al., 2020; Ruffolo, McGuire, et al., 2021; Saavedra et al., 2009). Complications from G-tube placement put a significant burden on the health care system and are stressful for the patient and family.
A major complication with G-tubes is that they can become dislodged. When the child is dependent on a G-tube to provide nutrition and medications, some families will panic when the tube becomes dislodged and go directly to the nearest ED to seek care to replace the tube. To prevent unnecessary ED visits, families need to be educated on how to prevent dislodgement and replace G-tubes when come they come out or malfunction.
EDs are overcrowded; with the congestion of these departments, patient safety is in jeopardy (Barata et al., 2015). The crowding of an ED increases medication errors, increases length of stay for a patient, decreases patient satisfaction, impedes the health care staff from providing quality care, and, most importantly, threatens the safety of the patient (Barata et al., 2015). Traditionally, it is thought the problem of ED overcrowding is the fault of the ED itself—staff shortage, lack of space, incompetence in patient throughput, and so forth—but in reality, the problem of ED overcrowding is much larger than one department and is, indeed, a health care issue where all aspects of the medical institution are involved (Jeanmonod, 2018). Prior research has shown that including interdisciplinary care, including nurse-practitioner-led clinics, can reduce ED utilization (Maselli et al., 2021).
To help reduce ED overcrowding at our institution and to better care for children and families with G-tubes, an interdisciplinary team from pediatric emergency medicine, pediatric surgery, and pediatric gastroenterology convened and formed a performance improvement (PI) team. This interprofessional PI team included a family advisor, nurse practitioners, nurse educators, discharge coordinators, a pediatric surgeon, a surgery resident, nurses, and quality improvement coaches. From chart review, it was soon discovered that a significant number of patients from the pediatric surgery and pediatric gastrointestinal services were presenting to the pediatric ED with G-tube-related events.
In reviewing the charts of these patients, it was noted that most of these visits were preventable and could have been treated at home or within the outpatient subspecialty clinics. Further review was completed to understand why the patients and their families were coming to the pediatric ED and what interventions could be put in place to reduce the number of unnecessary evaluations in the ED. Our smart aim was to reduce G-tube-related ED visits at our children's hospital by 25% over 1 year.
MATERIALS AND METHODS
Setting and Sample
A retrospective evaluation of electronic medical records from a convenience sample of pediatric patients (0–18.99 years old) who presented to the University of Rochester Medical Center's pediatric ED for a G-tube-related complaint between January 2017 and July 2021 was completed. This pediatric ED provides care to approximately 30,000 children annually. Patients who are in need of further care beyond what the ED can provide are admitted to this institution's children's hospital, a 124-bed children's hospital located within a large academic, teaching hospital.
The electronic medical records for each of these patients were reviewed to obtain basic demographic data (age, race, and ethnicity). We also reviewed the reason for presenting to the ED, type and size of G-tube, which subspecialty service placed the tube (pediatric surgery, gastroenterology, interventional radiology), actions taken in the ED (reinsertion of the G-tube, reassurance, subspecialty consult), and the disposition of the patient after ED evaluation. Baseline data concerning ED visits for G-tube-related concerns were abstracted from medical records between January 2017 and March 2018. On the basis of the baseline data, the PI team implemented initiatives in April 2018 to reduce ED visits. Retrospective data collected from April 2018 through July 2021 reflect the intervention phase.
Over a 6-month period, numerous interventions were put into place to help reduce the number of patients visiting the ED for a G-tube dislodgement or malfunction (Ruffolo, Pulhamus, et al., 2021). Education packets were updated with improved information, instructional videos were reviewed and updated to reflect current practices, stocking of replacement tubes on the units increased to improve access for immediate needs and to supply emergency G-tube replacement kits for home, and a new educational pathway was introduced to enhance and standardize the education the patient and their families received. Further descriptions of each intervention follow.
Education Packets
On the basis of prior data, the PI team believed that most visits to the ED could be avoided if the patient and family had the appropriate education to care for complications that may arise with the G-tube, along with having the necessary supplies at home to correct such problems. To initiate change in our patient population who currently have G-tubes, the interdisciplinary team at our institution evaluated the inpatient education received by caregivers to determine what changes could be made to enhance the education and increase caregiver preparedness at discharge. Before the implementation of this quality improvement project, families received brief, generic information concerning G-tubes and how they function.
The current general G-tube packet was revised to include information on the specific G-tube placed, potential complications with improved photographic examples, securement advice, emergency contact information, and emergency replacement instructions. Education points covered in the packet are similar to what was included before (i.e., cleaning the tube, feeding through the tube, troubleshooting). The specific details were now focused on the specific G-tube the child received.
Although pointed efforts have been targeted to educate families about how to replace the G-tube if one becomes dislodged, prevention of dislodgement is preferable. A significant part of caregiver teaching stresses how to keep the tube intact in the stoma. Education in the hospital focused on securement devices, clothing choices (onesies, avoiding loose-fitting shirts), removal of any extension tubing and disconnecting from the feeding pump when the feeding tube is not in use, and use of abdominal binders to prevent tugging or pulling on the external portion of the tube. During the admission, nursing staff work closely with caregivers to determine the most effective securement methods for the child to help increase success at home.
Education also focuses on care that needs to be taken when transitioning the child from a car seat, chair, or bed to prevent tubing from getting caught and pulled; for example, caregivers are encouraged to detach extension tubing before transfers. The improvement team interviewed families that had prior dislodgements and found (a) the extension tubing is usually connected when dislodgements occur and (b) patient transfers are a frequent antecedent event for dislodgements.
Instructional Videos
In the past, caregivers watched standard G-tube videos through the Get Well Network. The Get Well Network videos are not able to be viewed by families who are not inpatients. The interprofessional team closely examined these videos and determined that an opportunity for improvement existed with the creation of videos specific to each type of G-tube, as well as a video illustrating the steps in G-tube replacement. These videos are viewed by caregivers before their child is discharged home as part of the educational process, and the families will also have access to them outpatient for ongoing reference. The videos can be found at the following website: https://www.urmc.rochester.edu/childrens-hospital/gastroenterology/g-tube-home-care/videos.aspx.
Equipment
The interprofessional team examined G-tube securement methods and established a more robust protocol to help prevent dislodgements. Our revised standard of care include the use of a securement device (hook-and-loop adhesive to anchor the tubing) attached to the abdomen, an abdominal wrap around the G-tube, and removal of the G-tube extension tubing when the G-tube is not in use. We also cover the balloon port of the G-tube with a cap or tape to prevent unintentional access. Nursing leadership partnered with the interprofessional team to increase supply stock of both G-tube equipment and securement devices on the hospital inpatient units to ensure patients would have the needed supplies.
A key component of safe discharge with a G-tube is the emergency replacement kit. Caregivers are provided with step-by-step instructions for replacement of a G-tube, along with all necessary supplies in a resealable bag. Contents of the kit include a 12-French-long G-tube and a 10-French Foley catheter to place in the stoma in the event that the G-tube will not fit, along with the syringes, tape, and lubricant needed to complete the procedure. Caregivers are educated that the replacement kit must be with their child at all times, and a second kit is provided to those patients who attend a daycare or school program.
Before discharge, caregivers are given the opportunity to practice tube replacement on a teaching doll. Education is focused not only on the specific technique to replace the tube but also on what to expect including formula leaking from the stoma, what the stoma looks like without the tube in place, and potential complications when reinserting the tube. Caregivers are able to see pictures of G-tube stomas during the teaching session to decrease anxiety and increase comfort.
Caregivers do not replace the tube at home for the first 3 months as the tract heals. The child is seen by either the surgeon or a pediatric surgical advanced practice provider at 1 and 3 months. The outpatient gastroenterology and surgical teams have caregivers show emergency G-tube replacement at both visits to ensure the skill is achieved and retained. At the 1-month postoperative visit, caregivers practice emergency replacement on an education doll. The first G-tube change is done in the surgery clinic after 3 months. A caregiver is coached through the first change with a new button type. At the 3-month visit, caregivers are provided education that the tract is now mature and it is safe and acceptable to change the tube at home. Achieving the first G-tube replacement with supervision and guidance allows caregivers to gain confidence for emergency replacements at home, potentially reducing the need for visits to the ED.
Education Pathway
While the patient remains hospitalized after initial G-tube insertion, the education that is delivered by the health care team regarding how to care for a G-tube and what intervention should take place if a complication arises is documented in a standardized education record in the patient's electronic medical record. In addition to the electronic medical record, a single-page education pathway was developed to help guide families and nurses with education to be completed in a stepwise manner (Figure 1). The pathway is framed as a stop light, with each hospital day encompassing a different color of the pathway. A single-page print of the pathway is placed in the patient's room for caregiver and nursing reference, to provide transparency in the education that needs to be completed, and to set expectations related to patient and caregiver involvement in the education process.
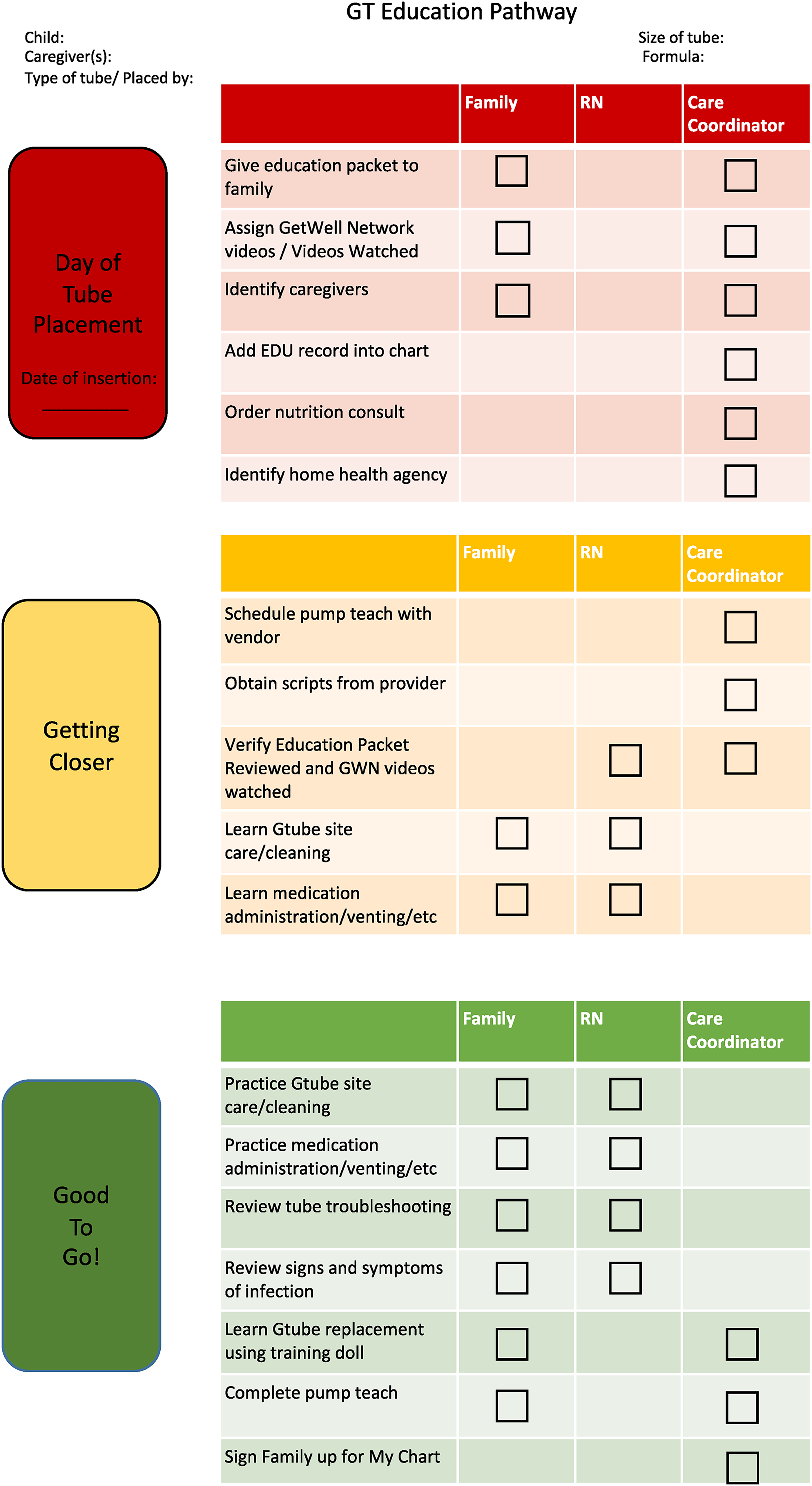
Discharge education pathway for caregivers of a child after gastrostomy tube (GT) insertion.
Part of the discharge protocol at our institution is establishment of community health nurse visits to provide support for the transition from hospital to home as well as an ongoing resource for patients and caregivers. Community health nurses work closely with the outpatient gastroenterology and surgical providers to ensure high-quality care is delivered to the patients at home. It is emphasized to the patient and families that, in addition to the surgery and gastroenterology clinics, these nurses are a resource caregivers can contact in case of a question or concern (including G-tube dislodgement) to help prevent an ED visit or hospital readmission.
As a component of this quality improvement bundle, in addition to the community health nurse support, education is continued at follow-up appointments in the outpatient clinic. Caregivers are asked to show securement techniques and emergency replacement procedure with reinforcement education provided as needed. Providers also check for the presence of an emergency replacement kit at each visit and ensure an ample amount of home supplies have been received.
Data Analysis
To help manage the data abstracted, information was entered into and analyzed using Microsoft Excel Version 2010 (Microsoft Corporation, Richmond, WA). Descriptive statistics (frequencies, mean, and median) were used to analyze the quantitative data.
RESULTS
During the 65-month period where data were collected, 587 pediatric patient encounters occurred in the pediatric ED because of a G-tube-related concern. Most of the patients were male (61%), White (57%), and non-Hispanic (88%; see Demographic Data in Supplemental Material, Table 1, available at http://links.lww.com/JPSN/A95). There were no significant differences regarding the day of the week patients presented to the ED. Seventy-six percent of G-tube-related ED visits occurred during nonbusiness hours of the subspecialty clinics. The number one reason for seeking care in the ED was because of the child's G-tube becoming dislodged (64%; i.e., child pulled it out, it was accidently pulled out during transfer, the balloon deflated and fell out; Figure 2).
G-Tube-Related ED Visits (N = 587)
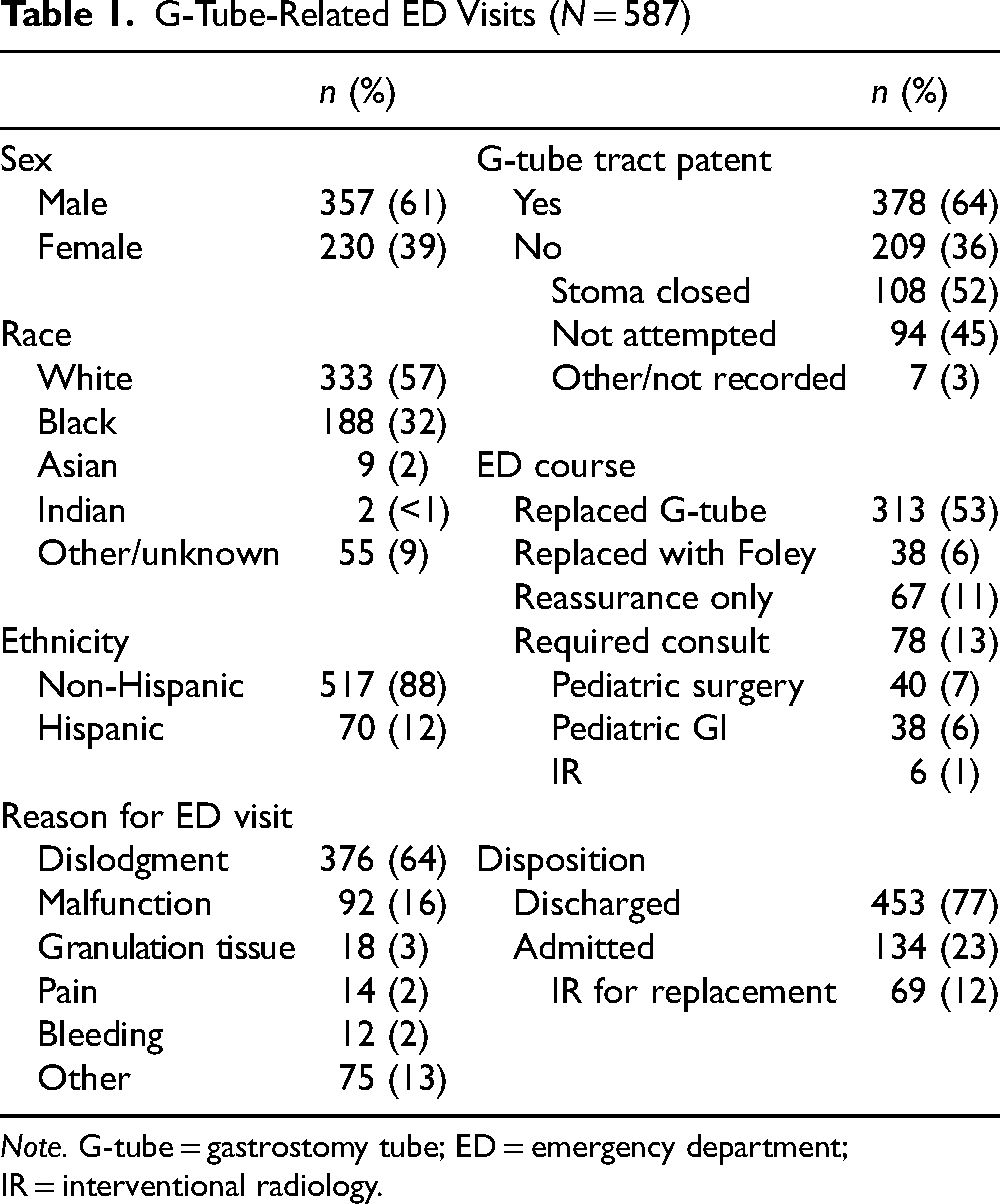
Note. G-tube = gastrostomy tube; ED = emergency department; IR = interventional radiology.
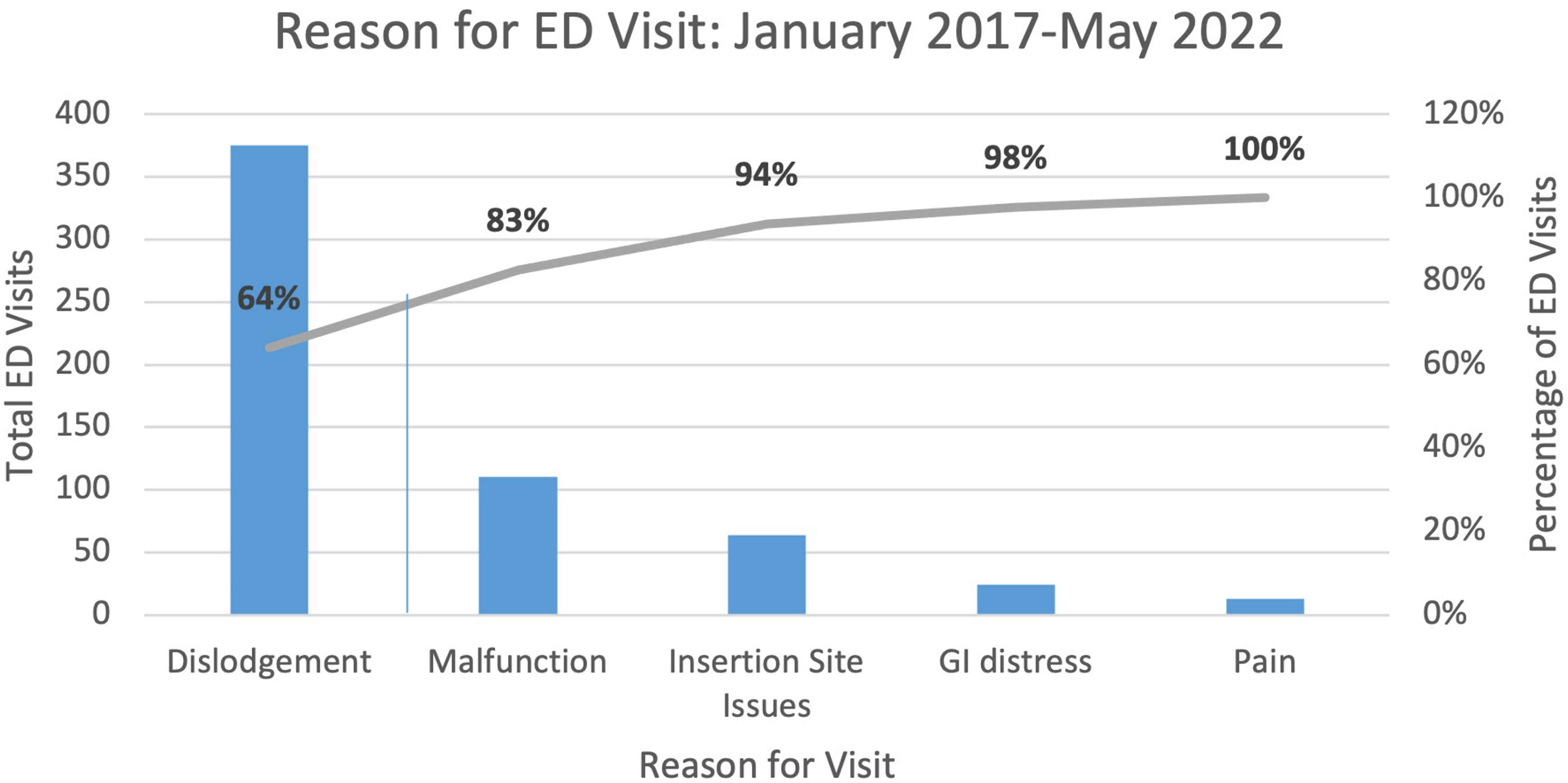
Pareto chart of reasons for emergency department (ED) visits.
The next most common reason for coming to the ED was because of the G-tube malfunctioning (16%; i.e., the G-tube was obstructed and fluids could not be flushed through, the tube itself was leaking, or a piece of the G-tube became broken). Other reasons for ED visits included granulation tissue, pain, or bleeding at the G-tube site (Table 1). Notably, the distribution of most common reasons for ED visitation did not change significantly over the study period.
Upon arrival to the ED, 64% of the patients still had the G-tube or another tube (Foley catheter) within the stoma to keep the tract patent. For those who did not replace the G-tube, the reasons parents cited were that they were unable to pass the tube because of the stoma closing (52%) or that they did not attempt to replace the tube (45%) because of not knowing how to and/or not having equipment to do so (Table 1).
While in the ED, most of the patients had their G-tube replaced with a new G-tube (53%) or a temporary Foley (6%) until they could be seen the following day in the subspecialty clinic (Table 1). Eleven percent of visits required only reassurance. Some patients who had a gastrostomy–jejunostomy tube had to be admitted for interventional radiology replacement the following day (12%).
Only 13% of children required consults from the pediatric surgical, pediatric gastrointestinal, or interventional radiology teams while in the ED to reinsert the G-tube because of difficulty in replacing the tube by the emergency medicine team or because of an immature tract. Our hospital considers the tract mature 3 months after insertion; there is a formal policy to consult pediatric surgery for any dislodgement within the first 3 months. The remainder of the patients seen in the ED either received an examination to reassure the family that the G-tube was indeed in the appropriate tract and could be used, prescriptions to treat skin or abdominal concerns such as cellulitis and constipation, or intravenous fluids to treat dehydration because of the G-tube not functioning properly. Of the children seen in the ED for G-tube-related concerns, 77% were discharged home from the ED (Table 1).
After implementation of the improved and enhanced education including updated education packets, educational videos, hands-on G-tube reinsertion demonstrations, and follow-up instruction in the outpatient setting, the number of patient visits to the ED started to decline (Figure 3). Before the quality improvement project, the median number of G-tube-related visits to the ED per month was 9.0. After the implementation of the PI project in April 2018, the following 7 months showed that the number of patients presenting to the ED with G-tube-related complaints was below the baseline median indicating special cause variation in the data. In association with this quality improvement initiative, the median number of G-tube-related ED visits decreased from 9.5 to 8, with special cause variation noted on a run chart (see Supplemental Data in Figure 3, available at http://links.lww.com/JPSN/A96).
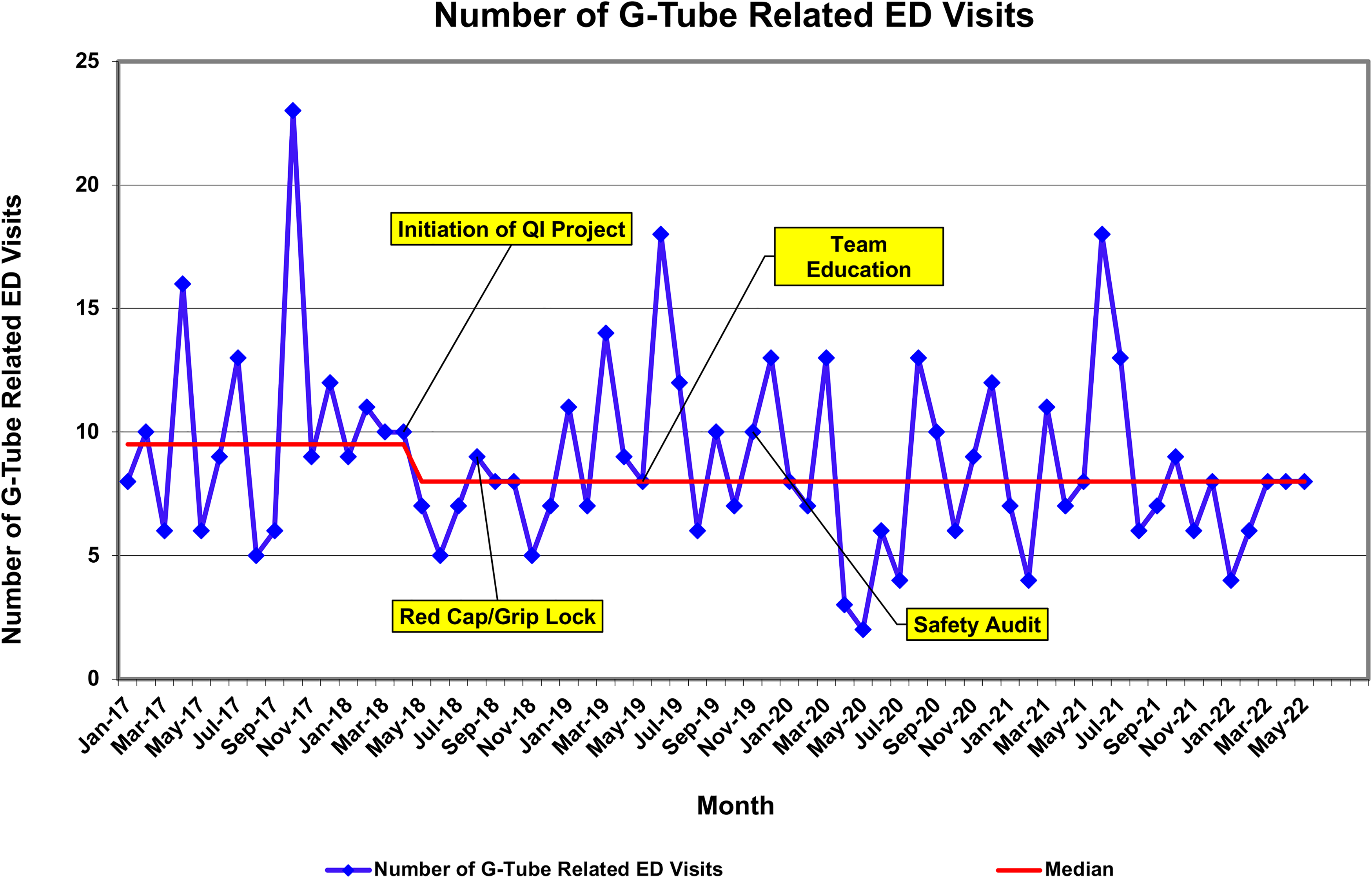
Run chart of monthly gastrostomy tube (G-tube)-related emergency department (ED) visits. Numbers decreased after the intervention began in March 2018, although the interventions exhibited a waning effect on ED visits.
One other metric evaluated was the performance of a call to a provider office before presentation at the ED. Before the conclusion of the project in October 2018, 10.3% of caregivers called the pediatric surgery or pediatric gastroenterology office. After implementation concluded in October 2018, 27.3% of caregivers called the office before presentation. This was calculated with a chi-square test to be significant to p < .05.
DISCUSSION
We presented a common case of a 12-month-old girl with a G-tube who had recurrent visits to the pediatric ED after tube dislodgment, which were attributable to the family not having extra supplies at home or the training necessary to replace the G-tube. These visits are preventable. Avoiding unnecessary ED visits is beneficial for patients, caregivers, providers, and health care systems.
Providing our patients and families with the appropriate education and instruction on how to care for their G-tube when a problem arises is critical in reducing ED-related visits. If caregivers feel comfortable knowing how to manage the G-tube and have the equipment to do so, it is very likely that they may not need to visit their local ED.
Interpreting the nature of this effect in the context of both the intervention and the larger societal context is important. It is possible that, after the initial implementation of the project, the effect of our initiative waned. In addition, most of our interventions were targeted to children with a new G-tube. Because the total vulnerable population of children with G-tubes includes children who had their G-tube placed before our intervention, our interventions only reached a subset of the total number of children with G-tube in our community. Therefore, it could take more time before a more dramatic effect on G-tube-related ED visits is manifested.
Given that there was another shift toward fewer ED visits starting in August 2021, the cumulative effects of our interventions may contribute to the positive effect over time. The lower ED utilization in 2020 may also be partially attributable to the global COVID-19 pandemic when overall ED utilization was reduced, particularly in April and May 2020.
Although further research and exploration may help define useful future interventions, some interventions are already planned to enhance the impact of this longitudinal project. First, a phone number is now provided to caregivers explicitly to call before an ED visit for a tube dislodgment, with a goal of diverting some of these visits. From 2011 to 2018, only 8% of patients coming to our ED for a G-tube-related problem called the clinic before presenting to the ED (Ruffolo, McGuire, et al., 2021). When data began to be collected for this project in January 2017 to the conclusion of the intervention in October 2018, that number increased to 10.3%.
The 2018 intervention did markedly improve both of these numbers, with more than double the number of caregivers placing calls before presenting to the ED (27.3%). An update to the emergency replacement kits is planned based on caregiver feedback, which will include improved securement devices, improved packaging, and individualized psychosocially informed crisis plans. A caregiver-facing website was also developed, which offers education videos and guides for patients with G-tubes. These interventions will, hopefully, continue to improve the care of patients with G-tubes and reduce unnecessary ED visits.
The current study does have limitations, which are important to consider when considering generalizability to other institutions. As many interventions were implemented simultaneously, we do not know which interventions are the most important. Retrospective data were utilized, which may contain inaccuracies in accounting. It is notable that visits decreased significantly beginning immediately postintervention, when it may be expected that there would be a delay to impact after the intervention. We were not able to directly discern which intervention may have provided immediate impact and which had deferred impact. In addition, although we collected demographic information for GT-related ED utilization, we did not analyze etiologies for demographic outcome disparities, as this was outside the scope of this specific study. We are currently conducting research to better understand these disparities and hope that our findings here will inform that work.
CONCLUSIONS
It is imperative that all patients receive consistent educational materials and readily accessible support across care settings—ED visits, inpatient admissions, outpatient clinic visits, and, most ideally, when patients are home. There are still times where an ED visit may be unavoidable, but if standardized instruction is offered and reiterated, it is likely that unnecessary G-tube-related ED visits can be reduced.
Footnotes
Acknowledgments
We thank Angie Pizzo, Family Advisor, for sharing her lived experiences and providing invaluable insight as we designed and evaluated this intervention.
Supplemental Material
Supplemental digital content is available for this article. Direct URL citations are provided in the HTML and PDF versions of this article.