
Abstract
Background
Contact dermatitis to hair dyes remains a health concern. Regulations in many countries require consumer self-testing for hair dyes, but no standardized procedure exists.
Objective
The aim of this study was to develop a self-test protocol for an allergy alert test (AAT) that can elicit a self-noticeable alert signal in p-phenylenediamine (PPD)–allergic consumers.
Methods
Simulating consumer use conditions (open application for 45 minutes after mixing with a developer), PPD-positive hair dye–allergic subjects and PPD-negative control subjects were tested on the forearm and behind the ear with experimental products containing 0.05%, 0.25%, 0.75%, and 2% PPD. Reactions were self-evaluated by subjects and independently assessed by dermatologists.
Conclusions
The AAT caused a reaction self-noticeable on the forearm in 90.5% (38/42) and behind the ear in 93% (39/42) of the PPD-positive subjects. This was objectified by a dermatological evaluation. The strength of the AAT response and the number of responding subjects increased with increasing PPD concentrations. Allergy alert test responses were also dependent on the reaction strength of the diagnostic patch test to PPD before the study; in subjects with (+++) patch test reactions, 19 of 19 were positive. All 48 control subjects were negative to the AAT. Therefore, the AAT protocol provides a signal indicative of an allergic reaction in PPD-allergic hair dye consumers.
Contact dermatitis to hair-coloring products remains a concern and is mainly related to p-phenylenediamine (PPD) and p-toluene-2,5-diamine. They are known allergens, and occlusive patch testing with PPD in the standard series and with p-toluene-2,5-diamine in the hairdressing series has been used for many years in dermatological practice to establish a diagnosis of contact allergy.1–4
To prevent elicitation in sensitized consumers, regulations in many countries, for example, the United States,5,6 Australia, 7 Canada, 8 India,9,10 Japan, 11 and some Latin American countries,12–14 require instructions for consumer self-testing.
Current instructions recommend application of the hair colorant to the skin for a defined period followed by an observation period throughout the next 48 hours, the average time required for contact dermatitis symptoms to develop.15,16 The intent is to alert the user not to apply the hair dye when experiencing any sensory or physically noticeable deviation from normal skin conditions and to seek medical advice.
Some self-testing protocols have been investigated by dermatologists, indicating that noticeable skin reactions are likely to occur.17–19 No standardized procedure has yet been described, and no harmonized instructions among hair dye manufacturers exist20–24 ; protocols vary regarding exposure dose, site, and duration as noted by the EU scientific advisory board (Scientific Committee for Consumer Products, now Scientific Committee for Consumer Safety). 20 The concern for an increased sensitization induction risk to colorants has been raised.20–23,25,26 Furthermore, it should be ensured that the consumer can perform and understand the alert signs of the test.22,23,25,26 It was recommended to create a uniform protocol with an exposure time and test preparation that reflect the actual use conditions. 23
For setting up a screening test, sensitivity and specificity have to be addressed.22,24,25 Before a large-scale study on asymptomatic hair dye consumers is considered, there must be demonstration of feasibility of a defined protocol addressing consumers' capability of self-reading and suitability of the chosen test site.
Consequently, the rationale of this study was to assess whether a defined self-test, referred to as an allergy alert test (AAT), can elicit a self-noticeable alert signal to a hair dye when performed by a hair dye–allergic consumer.
For this purpose, PPD-allergic subjects with a history of allergic reactions to hair dyes were recruited, and their AAT response to experimental hair dye products applied under simulated use conditions (open application for 45 minutes after mixing with a developer) on the forearm and behind the ear was analyzed.
By comparing with dermatological evaluation, it was further assessed whether self-evaluation by the subjects is feasible to indicate an alert for an allergic reaction to the product.
Comparing the response rates of subjects with different levels of patch test reactivity to PPD, we evaluated whether subjects with stronger reactivity (indicating a higher risk of severe reactions to hair dyeing) are adequately alerted.
We want to emphasize that the focus of the present work is investigating the suitability of the AAT to provide an alert signal to laypersons. The AAT is not intended for diagnosis of contact allergy because no dermatological analysis of the reaction to a single ingredient is performed under the standardized conditions of the diagnostic patch test.20,27
MATERIALS AND METHODS
p-Phenylenediamine–positive subjects with a history of allergic contact dermatitis to hair dyes and PPD-negative control subjects were recruited in 5 dermatological departments in 5 countries (the Netherlands, Germany, Austria, Great Britain, and Italy). The study protocol was approved by the respective ethics committees. Informed consent was obtained from all subjects.
Test Materials
The PPD concentrations in commercial products were reviewed, and 3 groups of shades were defined: light (typical range, 0.02%–0.2% PPD after mixing with a developer), medium (0.07%–0.48% PPD), and dark (0.37%–2.0% PPD). Accordingly, 3 experimental test products were formulated: product A (0.05% PPD after mixing with a developer, for light shades), product B (0.25% PPD, for medium shades), and product C (0.75% PPD, for dark shades). Product D (2.0% PPD) corresponded to the highest allowed concentration in Europe.
Products contained 2 additional hair colorants, resorcinol and 2-methyl-5-hydroxyethylaminophenol, each at concentrations of 0.03%, 0.15%, 0.46%, and 1.22% after mixing with a developer, respectively, in products A to D. The matrices consisted of water, surfactants (<30%), solvents (<25%), ammonium hydroxide (<3.5%), and perfume (<1%). These formulas were mixed extemporaneously with a developer containing 6% hydrogen peroxide (1:1).
The control (Y) did not contain any colorant.
Subjects
p-Phenylenediamine–positive subjects had self-declared clinical manifestations of nonoccupational contact dermatitis to oxidative hair dyes. Subjects reported the shade of commercial hair-coloring products that had elicited contact dermatitis reactions. The group comprised 46 subjects after subtracting the 4 subjects who dropped out (Fig. 1A).
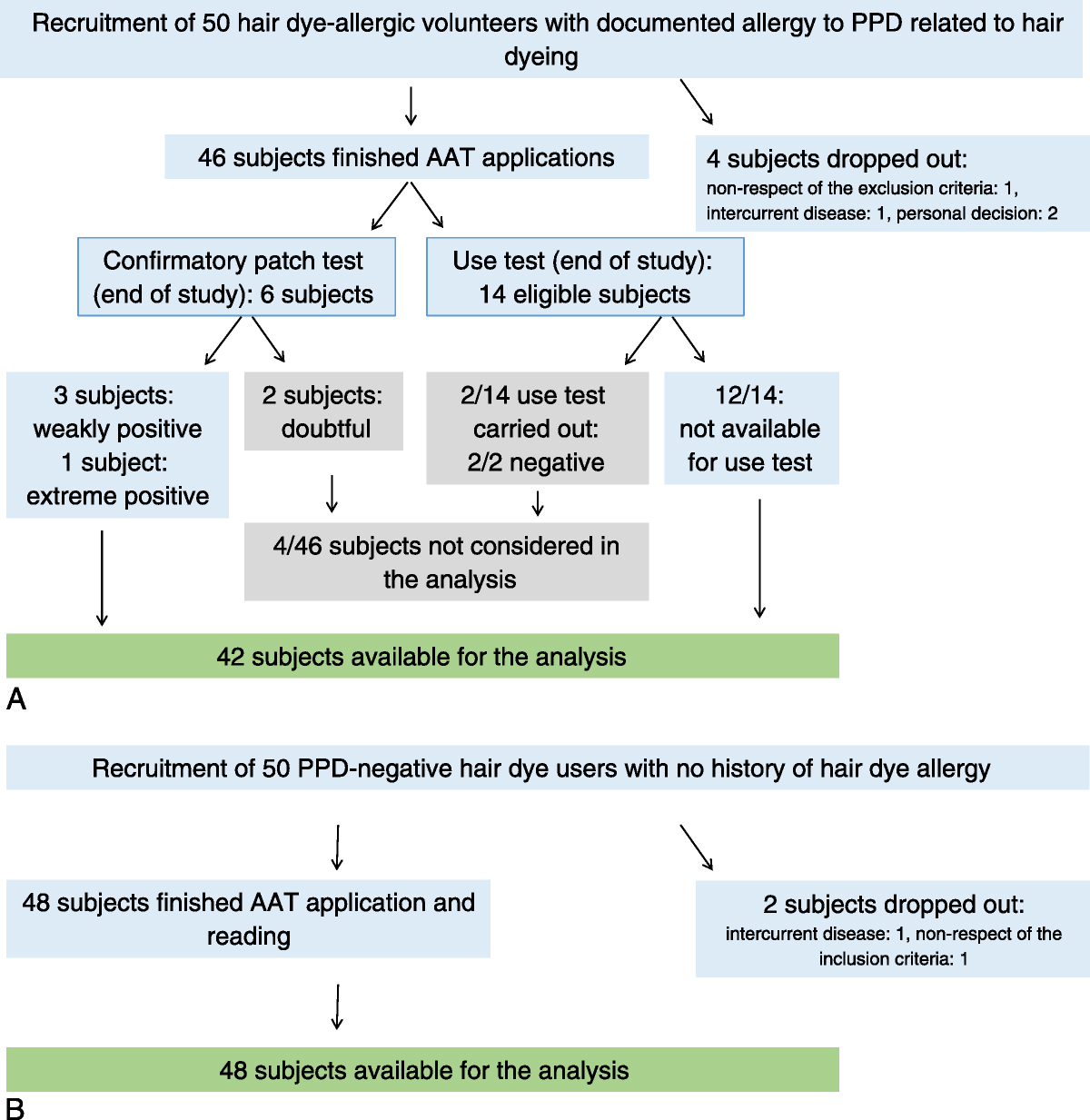
Overview of study subjects from the recruitment to the end analysis. A, Experimental group of PPD-positive subjects with a history of allergic reactions to hair dyes. B, Control group of PPD-negative subjects without manifestations to hair dyes.
Further 2 subjects were excluded because they were not patch test positive to the confirmatory patch test with PPD at the end of the study, and 2 additional subjects were excluded because the use test was negative (see Results). Therefore, the comparative analyses were carried out on 42 subjects (Fig. 1A).
p-Phenylenediamine–negative control subjects were hair dye users with no history of adverse reactions to hair dyes. The group consisted of 48 subjects after subtracting the 2 subjects who dropped out (Fig. 1B).
Study Design
p-Phenylenediamine–positive subjects were tested consecutively with experimental products containing rising concentrations of PPD (A–D); the control product Y was applied simultaneously. When a product produced a definite allergic reaction by dermatological grading accompanied by self-perception of a positive reaction by the subject, the AAT was confirmed as positive, and testing with products containing higher PPD concentrations was not done. A doubtful reaction was considered as objectified only if a clear positive reaction was elicited by the higher-concentration experimental product.
p-Phenylenediamine–negative control subjects were tested with 1 experimental product only and with the control product Y.
The products (0.15 mL) were applied by a study nurse or the investigator using a micropipette after placing circular adhesive devices (3M, Monaderm) on the volar area of the forearms and behind each ear. They were spread over the surface surrounded by the adhesive device (3.6 cm2) (Fig. 2). The applications of experimental and control products were not blinded because the colorants colored the skin.
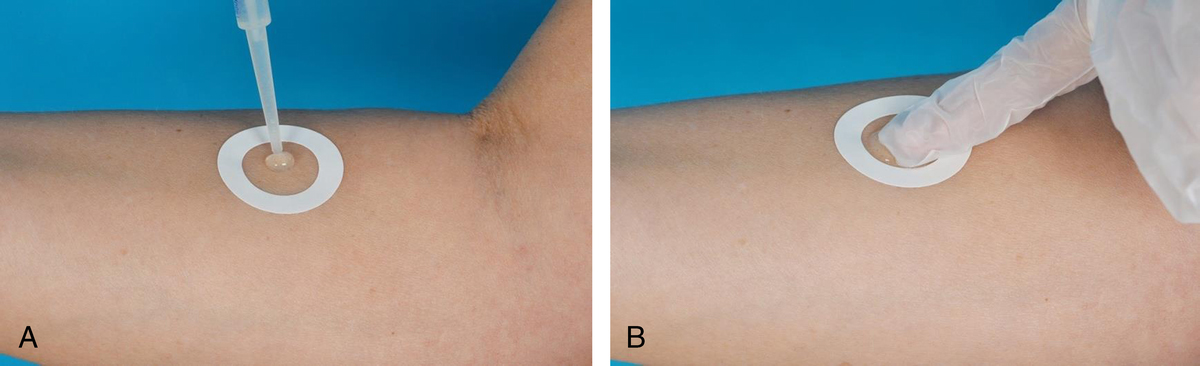
Application of the experimental product on the forearm. A, The products (0.15 mL) were applied by a study nurse or the investigator using a micropipette after placing circular adhesive devices (3M, Monaderm) on the volar area of the forearms and behind each ear. B, Products were spread manually over the surface surrounded by the adhesive device (3.6 cm2).
The adhesive devices were removed 45 minutes after application, and the test products were washed off. Reactions were recorded on day 0 (15–20 minutes after removal), day 2, and day 4. Further readings were carried out where necessary.
Self-evaluation based on sensory and tactile perception and/or a mirror was carried out at least until day 6 using diaries in which the subjects filled in daily all manifestations and their onset.
A high weighting was given to the self-evaluation of the reactions, because in real life, the consumer decides about proceeding or not to hair coloring. To independently evaluate the feasibility, AAT reactions were also assessed by dermatologists. In the absence of a universally accepted method for grading open test results, a published scoring was used. 28 It included a global evaluation of the severity of the reaction and an objective evaluation using a set of objective parameters (maximal score, 19).
Therefore, the evaluation of the reactions was done from several perspectives:
Consumer perspective: AAT self-perceived by the subject; reaction present 6 hours post-application and not later than 48 hours Dermatologist's perspective: reaction objectified by the dermatologist as doubtful or positive at day 2 and, possibly, day 4 Broader perspective: AAT self-perceived by the subject and objectified by the dermatologist.
The PPD-positive subjects with no reaction or a doubtful reaction to product D (highest PPD concentration) underwent a confirmatory diagnostic patch test to PPD.
A confirmatory challenge test (use test on a large strand of occipital hair with the shade considered to have caused historical dermatitis) was proposed to all PPD-positive subjects who did not react to the AAT with the corresponding experimental product. The control product was applied on the contralateral side. Each contact area on the scalp had a surface of 10 cm2. The hair-coloring products were rinsed off using shampoo after 45 minutes, and skin reactions were scored 20 minutes, 2 days, 4 days, and later if needed. The reactions were graded using the same method as the AAT.
Sample Size and Statistical Analysis
Prestudy and interim sample size calculations under different scenarios showed that enrollment of 45 PPD-positive subjects and 45 PPD-negative control subjects would have sufficient power to demonstrate a significant difference between the 2 groups.
Charts and 2 × 2 tables with descriptive statistics were constructed; McNemar χ2 test was used to test for statistically significant differences within the PPD-positive subjects.
RESULTS
The PPD-positive subjects consisted of 3 males and 43 females, aged between 17 and 71 years (mean, 41 years). Five of 46 subjects reported reactions to light shades; 19 of 46 subjects, to medium shades; and 22 of 46 subjects, to dark shades. Nine of the 46 subjects reported mild scalp dermatitis after hair dye use, 22 of 46 reported involvement of the scalp and edema on neighboring skin, 10 of 46 also reported facial eczema, and 5 of 46 reported hospitalization. All reactions were compatible with allergic contact dermatitis; no contact urticaria or manifestations of type I reactions after hair dye use were reported. The grade of positive patch test reactions to PPD within 5 years before the study was weakly positive (+) in 8 of 46, strongly positive (++) in 19 of 46, and extreme (+++) in 19 of 46 subjects.
The PPD-negative subjects recruited from the dermatological departments consisted of 2 men and 46 women, aged 20 to 71 years (mean, 41 years).
Reactivity to the Experimental Products
Cumulative reactivity to all products was, respectively, 93% behind the ear and 90.5% on the forearm. Thirty-eight (90.5%) of 42 PPD-allergic subjects reacted to at least 1 experimental product on day 2 on both test sites. These reactions were both perceived by the subjects and objectified by the dermatologists.
One subject (2.4%) reacted only behind the ear with a perceived and objectified reaction. Three subjects (7.1%) did not react to any experimental product. They were followed up with a diagnostic patch test to PPD: 2 were negative on day 2 and weakly positive (+) on day 3; 1 subject had an extreme positive reaction (+++). For details on the reactivity, see Table 1.
Characteristics of Subjects Who Did Not React to Any AAT Test Concentration (Products A–D) and/or Did Not React to Use Testing With Self-declared Shade Level Causative of Historical Allergy Symptoms
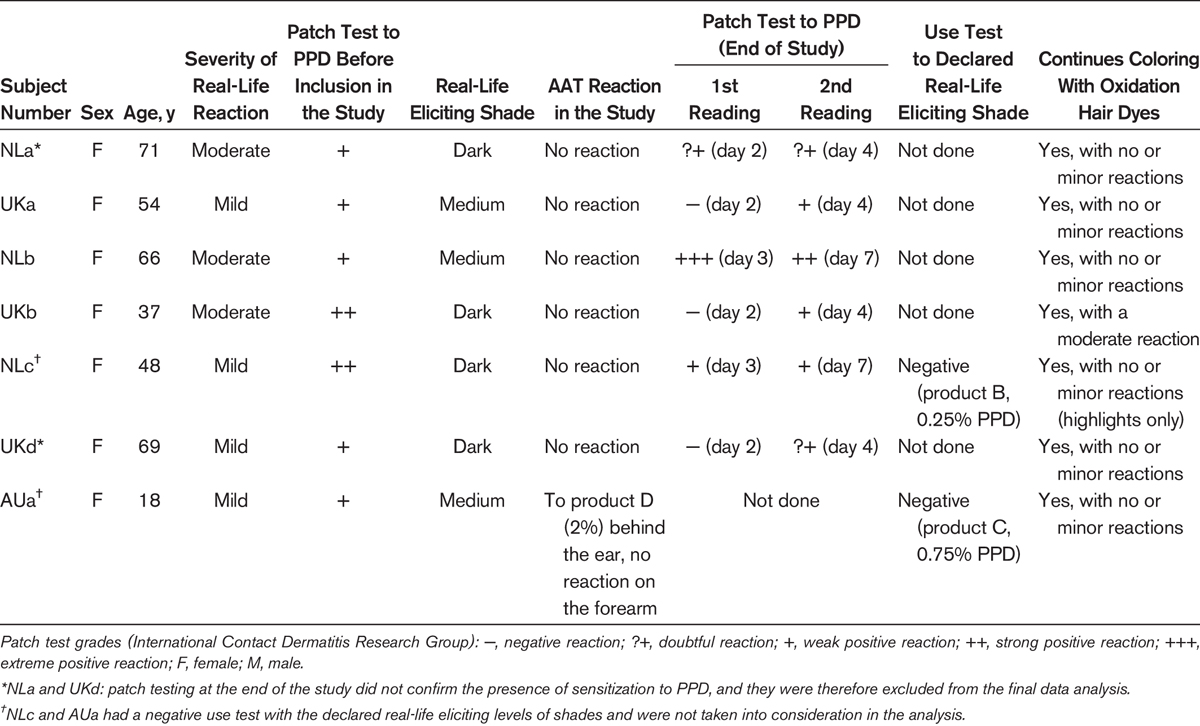
Four subjects were not included into our analysis because, in 2 of them, a clear proof of current sensitization was absent (negative confirmatory patch test to PPD [Table 1, subjects NLa and UKd]). In the other two, a proof of current reactivity to the PPD concentration considered to have caused their dermatitis was not obtained (negative use test to the declared shade level [Table 1, subjects NLc and AUa]).
Concentration Dependency
The strength of the AAT response and the number of responding subjects increased with increasing concentrations on both test sites, both from consumer perspective (reaction self-perceived) and from a broader perspective (reaction self-perceived and objectified by a dermatologist; Fig. 3). Product A (0.05% PPD) elicited a positive AAT, by both self-evaluation and dermatologist's reading in 19 (45%) of 42 subjects behind the ear compared with 14 (33%) of 42 positive by self-evaluation and 15 (36%) of 42 with objectified reactions by dermatologists on the forearm (Fig. 3). Thus, product A elicited an AAT reaction in a greater number of subjects compared with those who remembered light shades as the cause of their dermatitis (5/42 [12%]). No statistically significant differences in the reactivity on the 2 test sites could be observed.
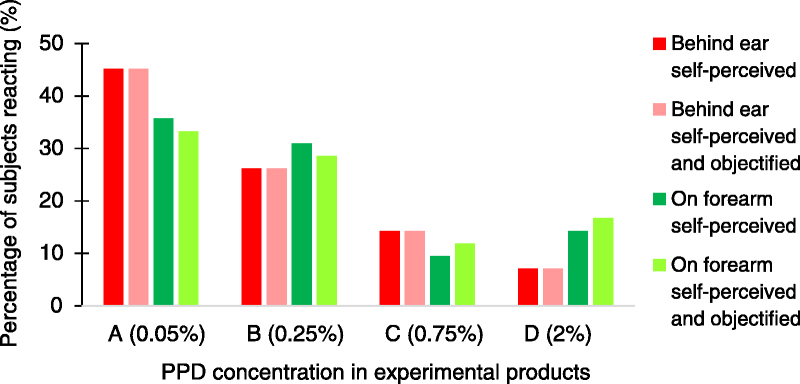
Concentration dependency of positive AAT in 42 subjects available for the analysis.
The 4 subjects who did not react to any experimental product on 1 or both sites were not available for the use test; therefore, their reactivity to the experimental products in real-use conditions at the time of the study is unknown (further details are given in Table 1).
The AAT reactivity (proportion of positive responders) on the 2 test sites was analyzed in subjects with different grades of diagnostic patch test reactions to PPD (Fig. 4). Allergy alert test reactivity rate increased on both test sites with the increase in the past patch test grade to PPD for all experimental products (Fig. 4A). This is also seen for the lightest test shade (product A) with which all subjects were tested (Fig. 4B). All subjects with extreme positive patch test reactions (+++) to PPD reacted to the AAT (Fig. 4A).
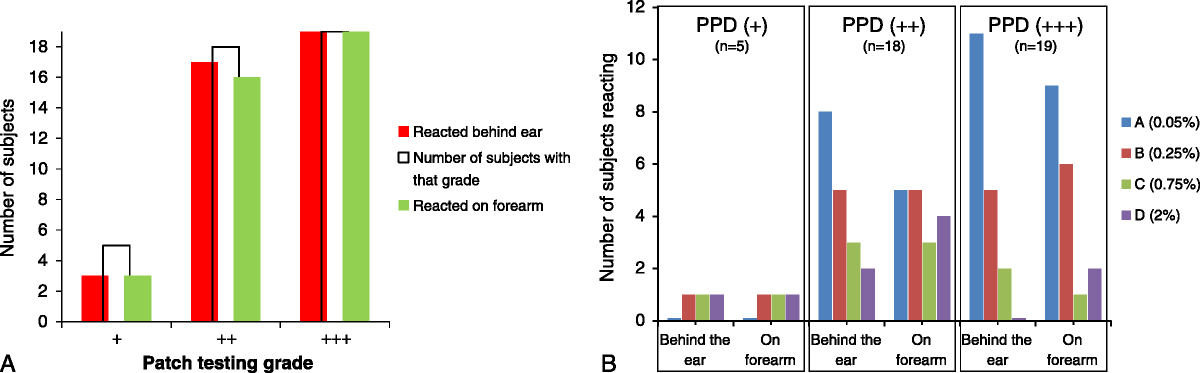
Stratification of AAT reactivity by past patch test grade. Reactions self-perceived by subjects and objectified by dermatologists at day 2 (N = 42 subjects). A, Reaction to any product (PPD concentration, 0.05%–2%). B, Allergy alert test reactions to increasing PPD concentrations in experimental products compared with subjects' reaction strength in diagnostic patch test before the study; no higher PPD concentration was tested when a positive response was obtained.
Time Course of the AAT Reaction
The time course of the AAT reaction was studied in the reactive subjects (broader perspective, n = 38 on the forearm and n = 39 behind the ear).
Subjects reported reaction onset from a few minutes to 48 hours after rinsing on both test sites (mean, 23 ± 15.4 hours on the forearm and 24 ± 14.4 hours behind the ear). Reddening, swelling, and itching were reported as the first symptoms. All reactions were self-evaluated as positive at day 2 in these subjects.
The strength of the reaction peaked at the 48-hour reading (mean score, 10 ± 3.7 on the forearm and 11.2 ± 3.6 behind the ear) and decreased thereafter (Fig. 5).
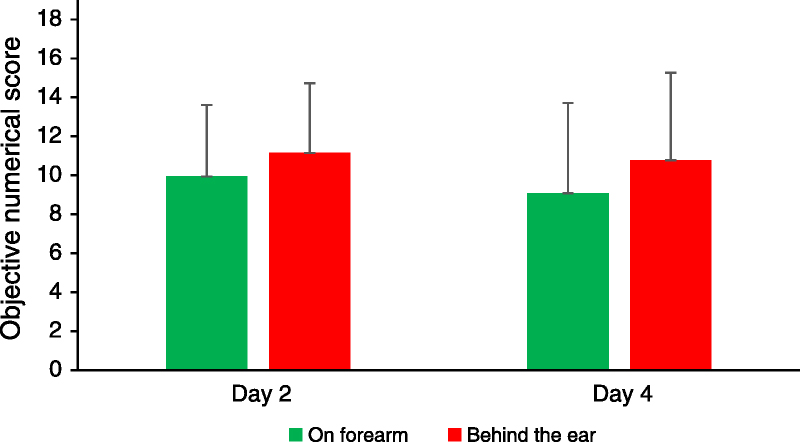
Numerical scores (±SD) of AAT-reactive subjects at days 2 and 4 readings (n = 38 on the forearm, n = 39 behind the ear). Reactions positive by self-evaluation and dermatologist's reading.
Specificity of the AAT Reactions
Doubtful reactions to the control product were recorded in 4 of 42 PPD-positive subjects: weak spotty erythema on less than 25% of the test site; these reactions were self-evaluated as positive. They occurred chiefly on day 0 and were considered as irritants. All 48 control subjects evaluated the AAT to the PPD-containing products as negative.
Reliability of Subject Self-evaluation (Consumer Perspective)
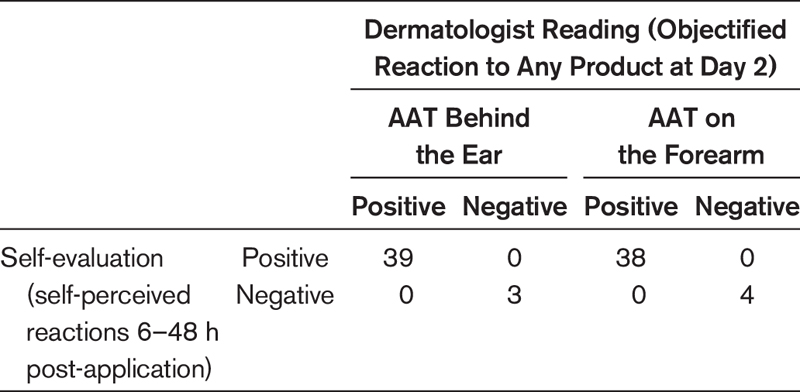
Evaluation of the AAT reactions by the subjects and by the dermatologists was in good agreement for both test sites, and no meaningful differences were observed (Table 2).
AAT Reactivity on the 2 Test Sites: Comparison of Subjects' Self-evaluation to Dermatologist's Evaluation
Adverse Events
No safety issues related to the AAT procedure were observed. None of the PPD-negative subjects reported manifestations compatible with active sensitization after participating in the study.
DISCUSSION
Contact allergy is a major concern to hair dye–allergic individuals, dermatologists, and the industry. Alerting the consumer of a potential health risk by a limited allergic reaction on a small skin area is considered beneficial because it can prevent an allergic reaction on the scalp, face, and neck if the entire product would be applied.5,6 This is particularly relevant for consumers who do not know that they are allergic and for allergic consumers who disregard their dermatologists' diagnosis and advice to stop hair dyeing.29,30
The current study assessed whether the applied AAT protocol is suitable to provide the basis for a harmonized test recommendation that can sufficiently alert hair dye–allergic consumers about their risk to develop contact dermatitis symptoms and thus not to apply the hair dye product.
The AAT was efficient to cause a reaction noticeable to most study subjects on the forearm (38/42) and behind the ear (39/42) within 48 hours. This was objectified by a dermatological evaluation. Therefore, a self-evaluation period of 2 days is considered adequate.
As in studies on self-testing for nickel and fragrance allergy, a high agreement was observed between self-reading and dermatologist reading.31,32 There were no relevant differences between self-evaluation and dermatological evaluation indicating that consumers can be adequately alerted by self-testing (Table 2, Fig. 3). Being alerted not to apply the hair color by an overinterpretation of irritant reactions as seen in 4 control subjects is not considered a limitation from a consumer protection perspective. 23 In the unlikely situation where these early reactions are indicating type I sensitivity, the consumers would be protected because they evaluate the test as positive.
Our findings are in line with another study indicating that hair dye consumers are able to correctly interpret alert signs. 18 The strength of the AAT response and the number of responding subjects increased with increasing PPD concentrations. Allergy alert test responses were also dependent on the reaction strength of the diagnostic patch test to PPD before the study; in subjects with (+++) patch test reactions, 19 of 19 were positive. These subjects reacted already to PPD concentrations between 0.05% and 0.75% in the AAT, indicating that they would be adequately alerted to avoid hair dyeing. A similar relationship between the patch test grade and the reactivity rate to open applications has been reported for other allergens.33,34 Conversely, individuals with weak positive reactions are less likely to be alerted (Fig. 4). In line with this, it has been described that such individuals continue hair dyeing because they are likely to experience milder symptoms. 29
As in previous studies with PPD applied either open17,18,35 or under a patch test, 36 a good dose-response relationship was observed on both test sites. For the first time, PPD concentrations as low as 0.05% were tested open, for 45 minutes, in a hair dye formulation. This concentration could elicit, before day 2, self-noticeable reactions, which were objectified by the dermatologists in 33% of tests applied on the forearm and in 45% of tests applied behind the ear (Fig. 3). These rates are comparable to a study in which 0.05% PPD (petrolatum) tested 48 hours under occlusion elicited positive reactions in 53% of subjects, both on the arm and behind the ear. 36
Comparison of the 2 test sites did not reveal statistically significant differences, both by self-assessment and when combined with a dermatological assessment (Fig. 5), indicating that both sites are suitable for AAT testing. Taking into consideration that application and reading on the forearm are more intuitive and consumer-friendly, we consider the forearm as more convenient for an AAT protocol.
Forty-two of 46 were considered for the current analysis, which stipulates a restriction to subjects with a clear evidence of current reactivity to PPD. Therefore, 4 of 46 were excluded because of a negative confirmatory patch test to PPD and/or a negative use test with the PPD concentration considered to have caused their dermatitis. Even when these 4 subjects are taken into account, the overall AAT reactivity would decrease by only 8%.
Among the 42 subjects included in the analysis, 3 did not react to any PPD concentration in the AAT, despite evidence of current reactivity to PPD shown by confirmatory patch testing. These subjects continued to use oxidative hair dyes with no or minor symptoms (Table 1). This rate is in line with the reported variation in the reproducibility of the diagnostic patch test, 37 both over time38–40 or applied simultaneously, 41 with Finn chamber technique38,41 or TRUE Tests.39,40
Induction of sensitization by the AAT was not investigated here. The risk of sensitization by self-testing in hair dye consumers was addressed in only 1 study, which found no association with the positive patch test results to PPD. 4
Our results demonstrate feasibility of a defined protocol addressing consumers' capability of self-reading and suitability of the chosen test site. This study does not address sensitivity and specificity in a “real-world” population of hair dye users. Investigating sensitivity and specificity in a study on asymptomatic hair dye users22,24,25 would pose considerable challenges regarding feasibility. In view of the background prevalence of PPD sensitization in the general or consumer population 3 and in view of the sensitivity derived from our test, after inclusion of the 4 excluded subjects, such a study would need enrollment of more than 5000 consumers for a precision estimate of the sensitivity of 10% and more than 19,000 for a precision estimate of 5%. 42
In conclusion, the dose-response observed and the high response rate in subjects with higher severity of the positive patch tests to PPD provide confidence that the AAT performed as described is suitable to provide a signal indicative of an allergic reaction in individuals likely to react to a hair dye.