
Abstract
Significance:
Despite 20 years of research and new treatment methods, diabetic foot ulcer (DFU) remains a common problem with frequent recurrences and complications.
Recent Advances:
There are reports that nerve decompression (ND) surgery has been observed to produce significantly fewer DFU recurrences than standard of care (SOC). The explanation of this apparent superiority has not been understood.
Critical Issues:
Microcirculation is understood to be involved in diabetic peripheral neuropathy (DPN) and DFU. There is an underappreciation of the participation in DPN of entrapment neuropathy (EN) due to nerve swelling and impingement in fibro-osseous tunnels. Reducing c-fiber compression in EN by ND generates recovery of subepidermal capillary flow. ND studies have found improved neuromuscular function and epidermal microcirculation phenomena, including chronic capillary ischemia (CCI) and pressure-induced vasodilatation (PIV). There is no current therapy recommended for impaired microcirculation. Clinical and animal evidence has demonstrated that release of locally compressed peripheral nerves improves the epidermal microcirculation which is under sympathetic control.
Future Directions:
Using epineurolysis to relieve nerve compressions is a physiology-based therapeutic intervention and provides the scientific foundation clarifying how ND reduces DFU recurrence risk. Incorporating ND with current SOC treatments could improve DFU recurrence risk, hard-to-heal ulcers, neuroischemic wounds, amputation risk, and the resulting costs to society. More studies using ND for DFU, especially evidence-based medicine Level I studies, are needed to confirm these preliminary outcomes.

SCOPE AND SIGNIFICANCE
Care for the diabetic foot ulcer (DFU) continues to be a frustrating challenge. Standard of care (SOC) methods are plagued by regrettable levels of delayed healing, failures to heal, recurrence risk, and association with amputations and early mortality. 1 We hope to bring attention to the clinical reports observing that diabetes is frequently accompanied by nerve trunk enlargement. Local sites of compression can then occur that cause neural dysfunction and pain but respond to surgical nerve decompression (ND) and recover a degree of normal function.
TRANSLATIONAL RELEVANCE
Nerve compression affects autonomic function, as well as sensorimotor processes. Microcirculation to the skin is under A-delta and c-fiber sympathetic control. Two microcirculation phenomena, chronic capillary ischemia (CCI) and degraded pressure-induced vasodilatation (PIV), are known to be present in diabetes yet can be revived by ND.
CLINICAL RELEVANCE
Laboratory and clinical evidence suggest that ND is effective for improving microcirculation in these patients with diabetic peripheral neuropathy (DPN) where any effective treatments are lacking. Clinical and preclinical ND studies over the past 20 years have provided a plausible and logical scientific rationale for the highly significant surgical successes in minimizing DFU complications. Recognition that ND improves neurovascular control of microcirculation offers hope of minimizing the totality of DPN, to the benefit of preventing DFU, DFU recurrence, and associated infection, amputation, and early mortality complications. Addition of improved microcirculation to the successes of SOC is likely to allow better DPN and DFU outcomes.
BACKGROUND
The problem
Etiology of the DFU is strongly related to the presence of DPN. The metabolic defects of diabetes produce both direct neural dysfunction and a secondary nerve swelling with potential for multiple local nerve entrapments. The neural defect, described as “dying back of axons” or “length-dependent axonopathy” (LDA), is progressive, irreversible, and resistant to pharmaceutical interventions. 2,3 But the secondary entrapment neuropathy (EN), caused by metabolically determined axonal enlargement, 4 responds well to surgical external epineurolysis producing ND. Current DFU etiology theory focuses nearly entirely on LDA, but some neurologists find ENs to be so frequent at any stage of the diabetic disease that “they may be considered a neurophysiological hallmark of peripheral nerve involvement in DM”. 5 The use of ND to relieve EN has exposed unexpected objective benefits for DPN, DFU, and their complications.
It has been known for 40 years that microcirculation deficit is involved in skin ischemia and epidermal death, which leaves an open DFU wound. 2 Wound debridement, infection control, unloading of skin pressure, and restoration of macrocirculation in peripheral artery disease (PAD) are effective SOC treatments. But with SOC there remains a 20% necessity of amputation to achieve DFU healing and >10% incidence of demise unhealed. 6 Wound healing carries an ongoing 10% risk of 1-year mortality and a 20–40% expectation of DFU recurrence within a year. 6 –9
Addressing the problem
Microcirculation is not addressed by SOC therapies, while ND has shown benefits. Animal and clinical studies indicate that phenomena related to microcirculation are rejuvenated by relief of nerve compression. 10 –13 We review 7 studies correlating ND and DFU recurrence. ND for EN is a little-acknowledged opportunity which appears to offer hope of much better outcomes.
Literature search and study inclusion criteria
Comparing ND and SOC in the DFU situation is a bit complicated. Recommended criteria for ND in DPN candidates include adequate circulation. 14 So ND use in DFU has been applied almost entirely to the neuropathic (nDFU) situation. Conversely the large literature of DFU SOC treatment and outcomes combines both nDFU and neuroischemic ulcers (n-iDFUs) in varying proportions, which have changed over time.
For our analysis, a literature search was conducted from June 1, 2022, to September 1, 2022, and the following databases were screened: PubMed, Cochrane Library, Google Scholar. For clinical trials: Clinicaltrials.gov and Cochrane Central Register of Controlled Trials were screened. The following terms were used in various combinations: “diabetic foot”, “diabetic neuropathy”, “compression neuropathy”, “impingement neuropathy”, “entrapment neuropathy”, “nerve decompression”, “nerve release”, “tunnel release”, “surgical release”, “epineurotomy”, “external neurolysis”, “incidence”, “prevalence”, “epidemiology”, “ischem*”, “meta-analysis”, “systematic review”, “ulcer recurrence”, “clinical trial*”, “clinical stud*”, “Eurodiale”, “standard of care”, “SOC”, “IWGDF”, “International Working Group”. Studies were removed that were older than 20 years, SOC studies with fewer than 500 subjects, or those that used the following terms: “quality of Life”, “QOL”, “carpal tunnel”, “CTS”, “ulnar tunnel”, “guidelines”, “protocol”. Based on our screening of the literature, the seven ND studies cited here are the only published studies that include DFU recurrence data. No other ND reports study DFU recurrence risk.
PERIPHERAL NERVE ENTRAPMENT
In diabetes, hyperglycemia saturates the hexokinase metabolic pathway that produces glucose-6-phosphate for cellular energy, and the alternate aldose reductase pathway becomes invigorated (Fig. 1). Aldose reductase, which catalyzes the reduction of glucose to sorbitol, is found in all target tissues that develop diabetic complications, including peripheral nerves. 15 Fructose and the sugar alcohol sorbitol are intraneural metabolic end products of this alternate path. Since there are no sorbitol or fructose transporters in the axonal membrane, like the family of GLUT and aquaporin transporters for glucose and water, 15,16 intra-axonal sorbitol and fructose are trapped within the axon and accumulate over time, similar to what has been shown in the eye in diabetes. 17 –19 This accumulation raises osmolarity, adjacent tissue fluid is transported across the epineurium attempting to achieve intraneural normotonicity, and nerve trunks become larger than normal. 4 As shown in Figure 2, in areas like periarticular fibro-osseous tunnels, the increased nerve size cannot be accommodated, and an external compression results with measured pressures of 60–105 mm Hg in the tibial nerve branches at the tarsal tunnel. ND reduces those pressures to <10 mm Hg. 20 Nerve entrapments at the carpal tunnel, tarsal tunnel, fibular neck, and ulnar tunnel are known to be common in diabetes. 21 When symptomatic, they are appropriately treated with external neurolysis surgery. Both autonomic and somatic sensorimotor functions are measurably affected by compression and relieved by ND. With the microcirculation to skin being under sympathetic control, the secondary EN can be of great consequence to development of the DFU wound. These EN changes appear to be directly related to the presence of diabetic neuropathy. 22
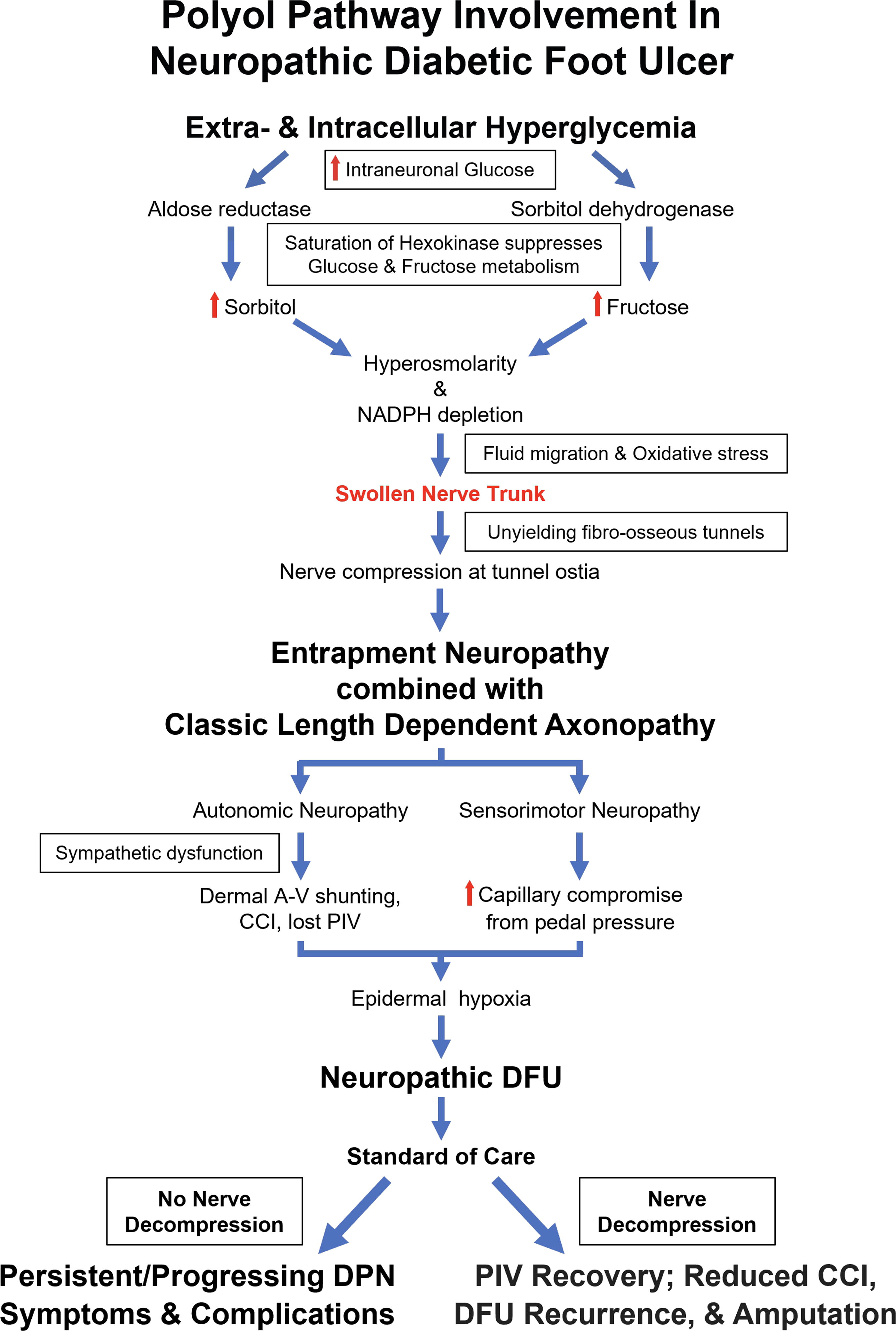
Hyperglycemia saturates the hexokinase pathway for glucose energy production. The alternate aldose reductase path continues to function and accumulate sorbitol and fructose within the neuron and axon. Transport and diffusion of extracellular fluid into the axon attempt to balance osmolarity and a larger size of the peripheral nerve and axon bundle results. Misfit between the enlarged nerve and its anchoring fibro-osseous tunnel produces compression, and entrapment neuropathy is the result.
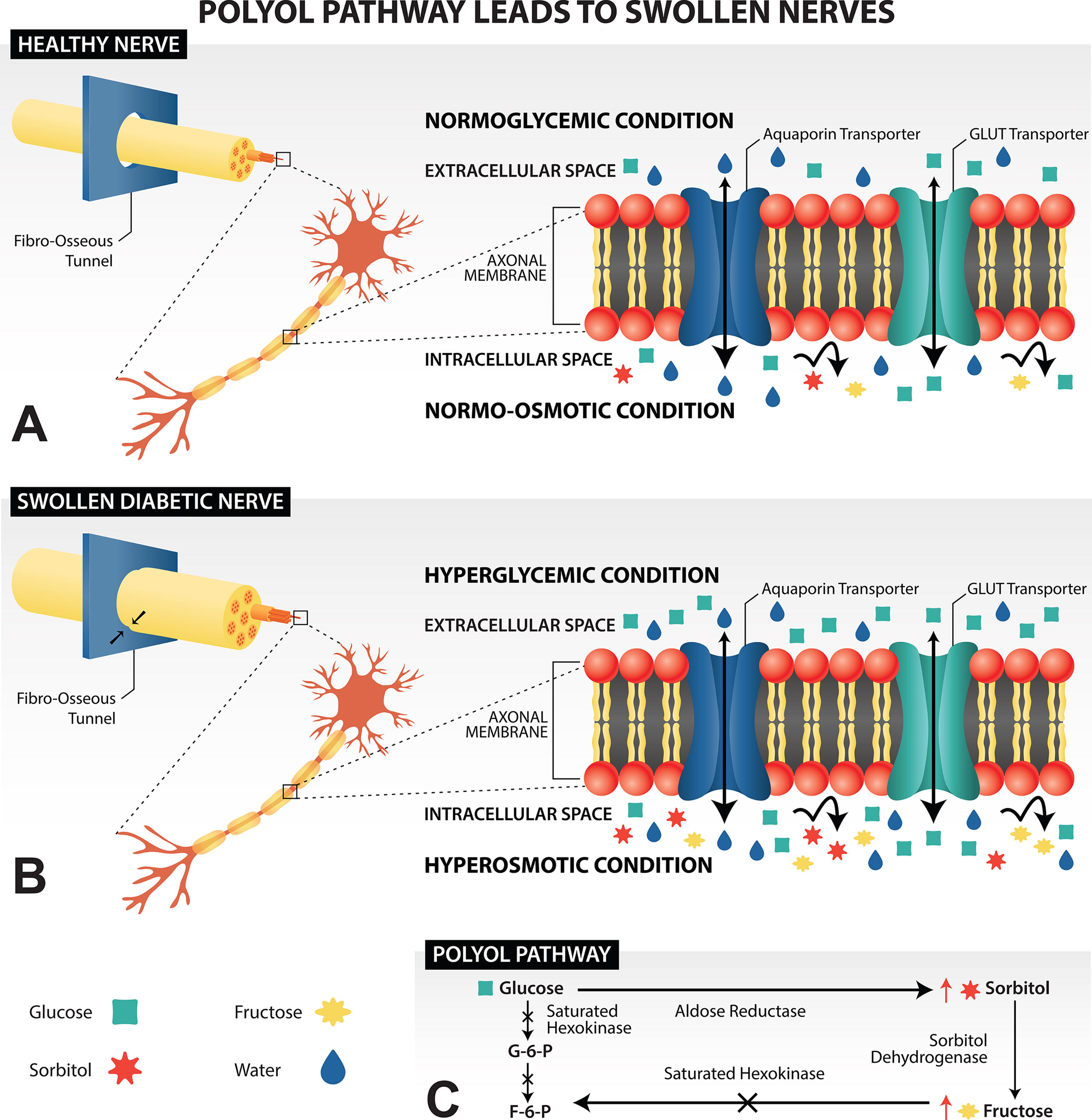
Tissue fluid, glucose, sorbitol, and fructose are sorted differentially by the axonal membrane. Sorbitol and fructose cannot diffuse across the membrane and have no transporters. Water and glucose move freely and bidirectionally by diffusion and/or transport. Glucose concentrations equilibrate across the axon membrane, but osmolarity does not, due to the sorbitol and fructose accumulation. Water must be pulled into the axons to equalize osmolarity, enlarging the nerve size.
SURGERY AND THE ENTRAPMENT NEUROPATHY DIAGNOSIS
EN is clinically demonstrated with the Tinel test, which generates a tingling or electric sensation radiating distally or proximally with fingertip percussion at a nerve compression site. A positive result is found in 45% of patients with diabetes 23 and is considered to indicate active, ongoing nerve compression, irritation, regeneration, or repair. In patients with Tinel-positive, painful DPN, Azsmann et al. in 2004, first reported an apparent protection from subsequent DFU or toe amputation after unilateral ND. 24 Ensuing DFU and minor amputation events all occurred in the nonoperated contralateral feet. Those complications occurred in 15 of their 50 cases (30%) during the mean 4.5 years follow-up, while the decompressed legs remained intact. This initial report focused attention on the potential of ND to modify DFU risk and its complications. Since that report, the seven other studies in Table 1 have shown very low risk of DFU occurrence or recurrence after a DPN leg has undergone ND. Nonoperated legs were not protected from new DFUs or amputation.
Risk of nDFU recurrence after ND surgery
ND, nerve decompression; nDFU, neuropathic diabetic foot ulcer; DFU, diabetic foot ulcer.
Seven ND studies all show nDFU annual recurrence rates <5%. The mean risk of recurrent DFU after ND is 1.39% per year. Different follow-up periods for some cohort members are included in these references. The highest annual recurrence rate in the seven studies was 4.3%.
bilateral ND surgery.
Surgical candidates, procedure, aftercare, and risks
Historically, candidates for ND in diabetes and DPN have had symptoms of pain and/or a healed nDFU. They should demonstrate failure of pain treatment, good glycemic control, a palpable foot pulse or ABI >0.8, a positive Tinel sign at a leg fibro-osseous tunnel site, minimal pedal edema, and weight <300 lb. Known lower limb peripheral nerve compression sites include the following: the common peroneal nerve at the fibular neck, superficial peroneal nerve in the distal third of the leg, deep peroneal nerve over the dorsum of the foot, tibial nerve proximally at the soleus arch and distally in the tarsal tunnel itself, the medial plantar tunnel, the lateral plantar tunnel, and the calcaneal tunnel. 25 ND studies report addressing 1–4 of these sites. Multiple sites (3 or 4) were decompressed in 465 of 526 subjects. The Viswanathan study (n = 61 patients) operated only the tarsal tunnel, releasing just tibial nerve and its branches.
ND is an outpatient open surgical procedure, an external neurolysis, usually performed without intraneural dissection. A few experienced surgeons safely accomplish this endoscopically. 26 Anesthesia can be local, regional, spinal, or general. Most surgeons use a tourniquet, but a few do not. Recommended aftercare is a bulky, compressive “Robert Jones” dressing with protected weight-bearing ambulation using walker or crutches. Sutures are retained for 3 weeks to minimize risk of medial ankle wound dehiscence. Recognized risks include iatrogenic nerve injury, wound dehiscence or infection, or local skin loss of anterior medial malleolar wound skin. The seven ND articles do not specifically report adverse events post treatment. Optimum timing is unknown. Zhong found better results in those with <5 years of known diabetes duration. 27 However, Anderson et al., demonstrated significant EMG improvement in ND cases as remote as the third decade from initial diabetes diagnosis. 28
SKIN MICROVASCULAR FLOW IN DIABETES
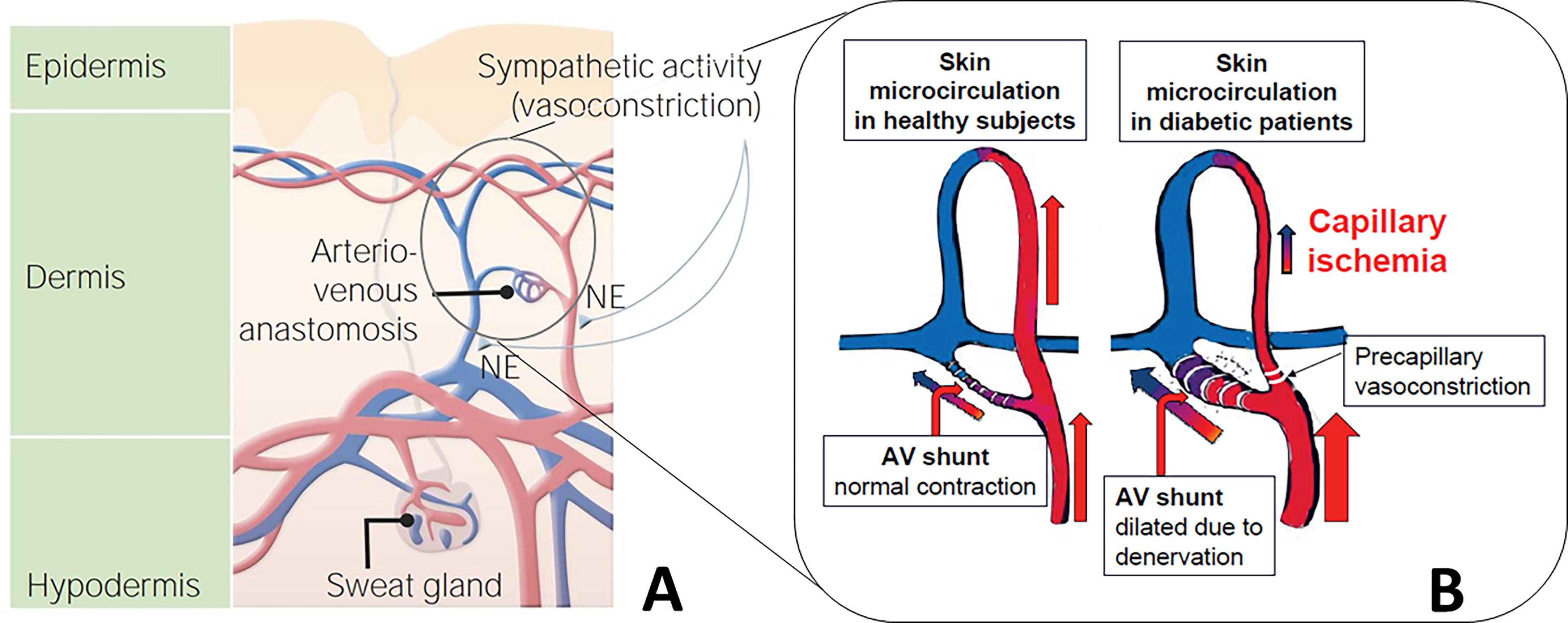
It has long been known that total foot circulation is increased in DPN, yet the crucial subepidermal capillary flow is diminished. 22,29 Figure 3 of normal skin shows the epidermal capillary plexus immediately deep to the epidermal papillae. The arterioles which feed the capillary system lie just deeper in the dermal reticular layer where sympathetic control of distribution to venules or capillaries occurs. In the normal microcirculatory state of skin, efferent sympathetic messaging curtails dermal arteriole–venule (a-v) shunting. Epidermal capillary blood flow is maintained and, thus, oxygenation and nutrition. DPN abolishes that autonomic control, opening the shunt and allowing an a-v vascular “steal” to develop in dermal and subcutaneous tissue with increased flow directly from arteriole to venule. Shunting events restrict both flow into and pressure drop across the more superficial subpapillary capillary plexus. The result is that total diabetic foot blood flow is maintained or increases while epidermal capillary flow decreases.
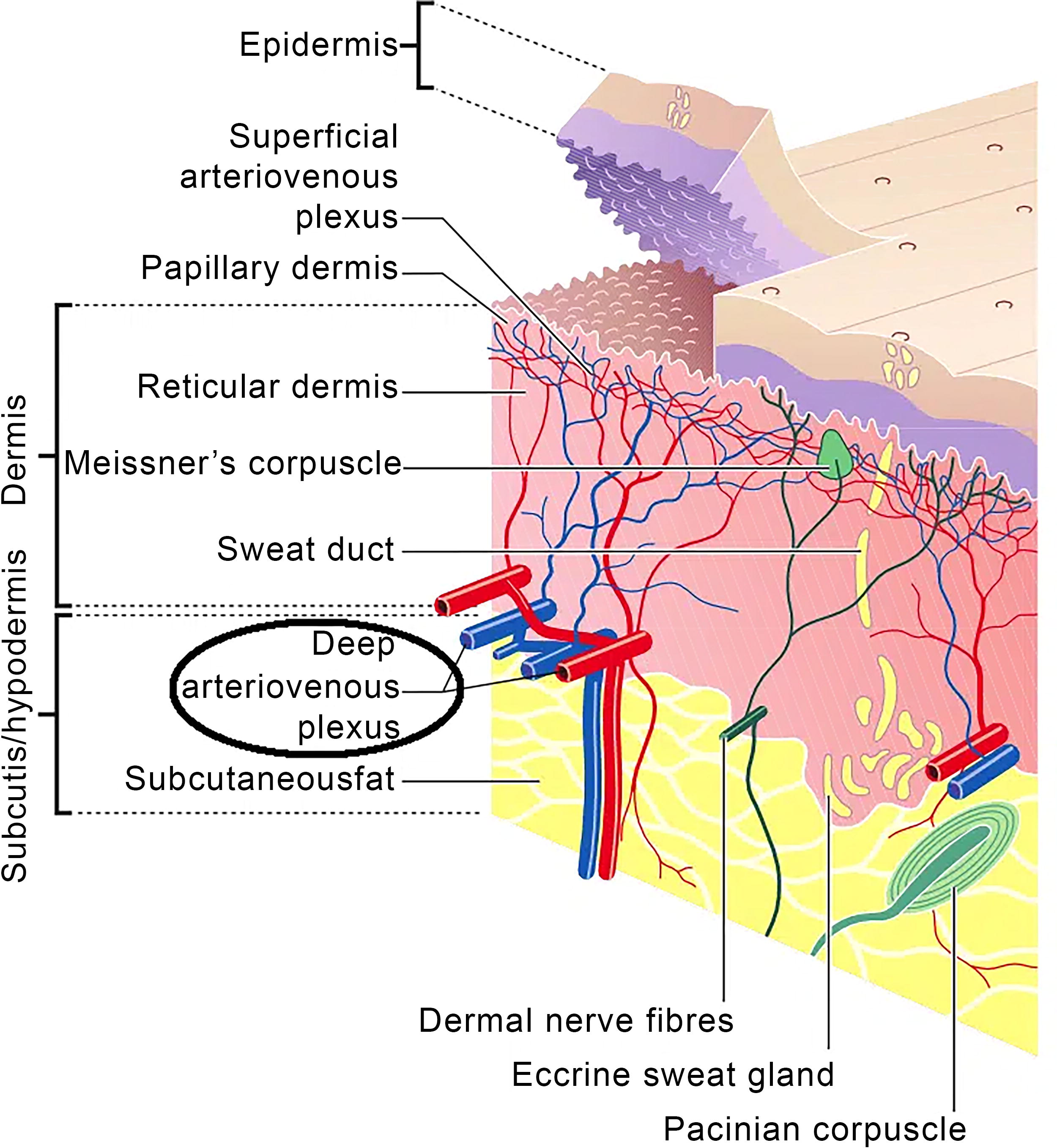
Overview of normal skin circulation. Sympathetic management of microcirculation occurs in the reticular layer with changes in a-v shunting controlling flow onward into the subpapillary capillary network. (From TeachMe Physiology website https://teachmeanatomy.info/the-basics/ultrastructure/skin/). a-v, arteriole–venule.
PIV AND CCI MICROCIRCULATION PHENOMENA
Laser Doppler flowmetry measures oxygenation in the most superficial 1 mm of skin and confirms that transcutaneous partial pressure of oxygen (tcpO2) decreases in diabetes. Such diminished epidermal capillary vascular flow is involved in two known skin circulation phenomena, namely, PIV and CCI.
PIV is an increased epidermal blood flow in response to afferent messaging of incident skin pressure and is also found to be diminished or lost in diabetes (Fig. 4). 30 –32 When moderate pressure increases are gradually applied to healthy skin, oxygenation as measured by laser Doppler tcpO2 typically increases about 45%. Much of the PIV work has come from Prof. B. Fromy and associates in Lyon, France. 12,31,32 Clinical research on PIV has concerned laboratory animals and better survival of skin transfers when they are innervated. Recovery of PIV after ND in DFU is yet to be evaluated in humans.
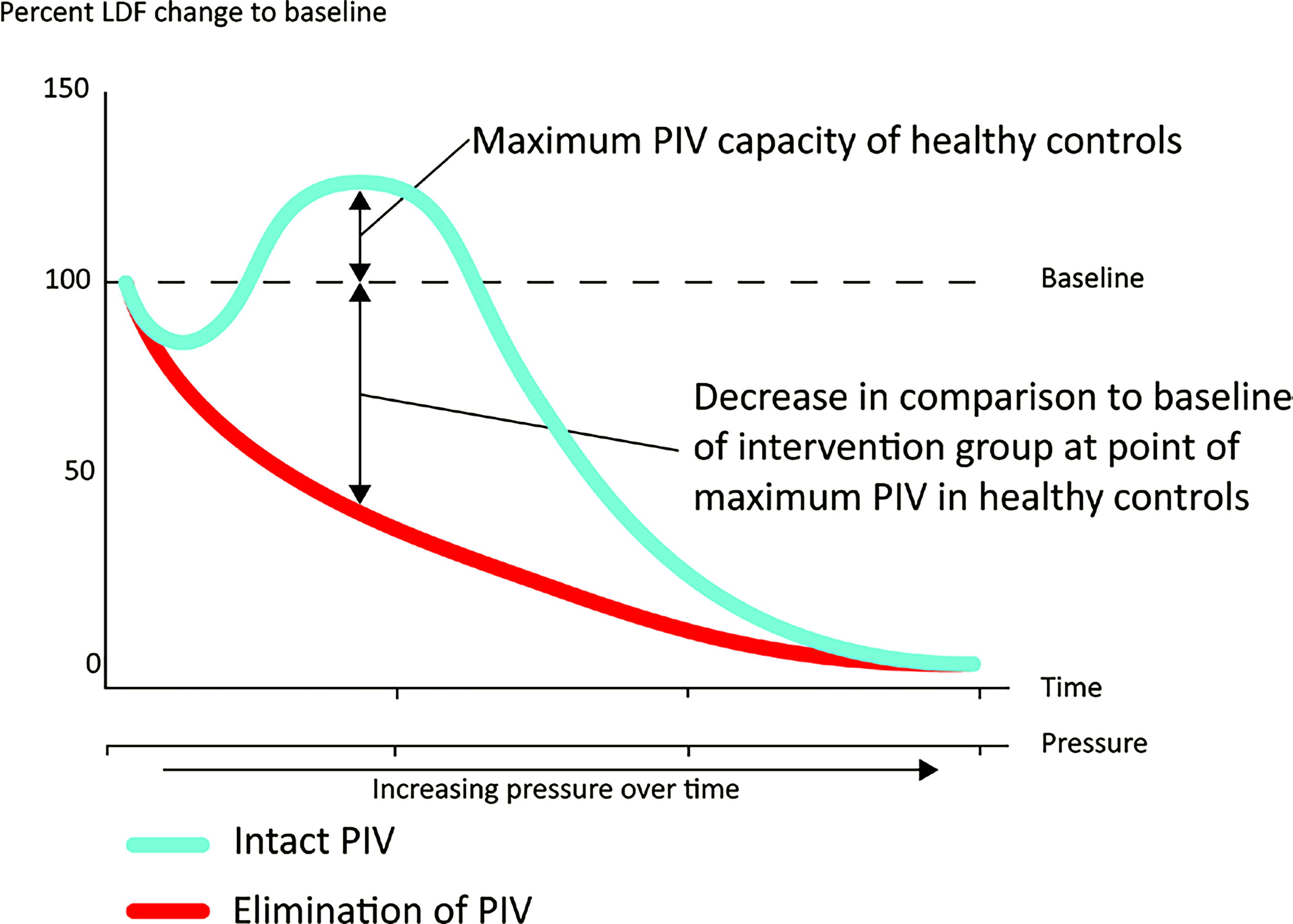
Quantitative example of PIV showing a drop in epidermal blood flow in subjects with a loss of pressure-induced vasodilation as a result of diabetic neuropathy (From Zwanenberg 23 ). PIV, pressure-induced vasodilation.
CCI has been studied primarily at the Karolinska Institute in Sweden. 29,33 –35 The said work has established that a state of “chronic capillary ischemia” is present in the skin capillaries of diabetic feet due to an increased shunting of blood through arteriovenous channels prior to passage into the subepidermal capillary system, as in Figure 5. Therefore, while the diabetic foot has normal or increased total circulation, the epidermis is hypoxic and starved of nutrition. This CCI is related to the diabetic disease per se and not only to presence or absence of late diabetic complications. 36 Understanding that a microcirculation defect is present means that critical limb ischemia may be occurring in diabetes, while toe pressure or ABI is not markedly abnormal. 37
Both CCI and PIV defects are exacerbated in DPN and DFU situations and can be reduced in diabetic laboratory animals by ND. 12,13 Balasubramanian et al. review the importance of microcirculatory interactions in diabetes and the DFU, with particular attention to the PIV phenomenon. 38 The contribution to the diabetic foot problem of autonomic small fiber neuropathy and deficient microcirculation is recognized, and a quest for interventions to improve function is implored. CCI is not specifically mentioned in that review, although several reports relating to this microvascular deficiency in diabetes, DPN, and DFU are published. Recognition that ND has therapeutic potential for deficient microcirculation has largely not been appreciated nor investigated to date.
DFU RECURRENCE AFTER ND
Since the 2004 Azsmann report several studies in surgical and podiatric journals have reported that epineurolysis ND surgeries have produced very low risk of DFU development, recurrence, and subsequent complications in DPN. Table 1 shows that seven DFU cohorts treated with ND had a combined 13 DFU recurrences across 526 subjects (2.47%) in 859 legs (1.51%). The 13 DFU recurrences that averaged across 937 patient follow-up years yielded an annual recurrence rate of 1.39%.
The 1.39% recurrence risk per year of these observational recurrence studies is striking. Two meta-analyses from Fu et al. and Armstrong et al. advise an expectation for all-cause DFU recurrence risk of 22.1% and 40% annual recurrence, respectively. 7,8 . The z-score for a comparison of ND versus Armstrong is less than −4 (i.e., more than 4 standard deviations less than the Armstrong mean). The Fu international study has no cohort number, which is required to calculate a z-score. We presumed a cohort size in their 49 articles of between 500 (10 patients/study) and 100,000 (2,040 patients/study) and found z-scores for each assumption to be less than −4, showing that the study size was not critical in comparison with ND. z-Scores of this magnitude, representing 4 standard deviations from the mean, indicate statistically that achieving this result by chance is extremely unlikely (p < 0.0001).
Animal laboratory studies verify that CCI and PIV loss both develop as diabetes is induced and are exacerbated when nerve compression is present. These phenomena improve after decompression. 11,12,39 These rat and mouse studies provide strong evidence confirming the associations between diabetes, EN, impaired sympathetic function, and microvascular deficit, and find that ND allows significant although incomplete recovery. The recovery of microcirculation after ND is consistent with the observed protection from initial ulceration and DFU recurrence in the human diabetes studies shown in Table 1. Minimizing recurrence after DFU healing by using ND offers an important prospect for controlling the complication cascade of recurrences, subsequent amputations, and early mortality in DPN.
Adding ND to SOC as initial treatment for nDFU is described by a prospective randomized study from India. 40 It relates to a superb and unusual 90% healing at 3 months and 100% healing within 6 months after adding initial ND to SOC in >60 initial DFU wounds as large as 3 cm in diameter. We suggest that explanation for the unmatched success rates in Table 1 likely lies in the unparalleled and durable ability of ND to rejuvenate microcirculation through relief of EN-associated sympathetic dysfunction.
DISCUSSION
Standard of care treatment
Multiple factors that can lead to DFU recurrence after SOC have been identified, including poor glycemic control, off-loading regimen, patient compliance with wound care regimens in the case of active ulcers, and tobacco use. ND for relief of EN addresses none of these, but it is the only therapy for DPN and DFU that addresses microcirculation.
SOC for DFU prevention, treatment, and aftercare primarily addresses restoration of PAD macrocirculation and local wound concerns like peri-ulcer skin pressure relief, wound debridement, control of infection, and improving the local wound environment using cellular, acellular, or matrix-like surface dressings. No effective microvascular interventions are presently known and being used in SOC for DPN and DFU. The Viswanathan ND article from India compares favorably to the skin construct therapy report which healed 70% nDFU of similar size in 3 months, whereas SOC controls achieved closure in 34%. 40,41 Both minimizing recurrence and accelerated initial healing may be possible through adding ND to SOC. Restoration of neurovascular control of epidermal microcirculation is the new etiology insight that justifies ND and explains its efficacy. By failing to address the swollen nerves, EN, and resulting impingement-induced neurovascular and neuromuscular dysfunction, SOC is limited in effective treatment of the entire metabolically induced dysfunctions of DFU.
Electrophysiology and objective measures after ND
The ND literature describes improvement in both sensory and motor nerve function in DPN after EN is decompressed. Meta-analyses have found subjective pain relief, as well as recovery of sensibility. 42,43 Several reports describe durable objective increase in NCV with significant recovery post ND compared with diabetic controls either without DPN or with DPN but not operated. 27,28,44,45 Anderson et al. showed immediate improvement of motor evoked potential EMG amplitude in 82.6% of 46 treated legs, with an average improvement of 73.6%. Notably, this recovery occurred immediately, intraoperatively, and within 60–90 s of the common peroneal nerve release (pre-ND, 3017 ± 2739 µV; post-ND: 5238 ± 4225 µV, p < 0.0001). 28
Motor evoked potential or NCV restitution is consistent with medium-term animal studies demonstrating that ND improved autonomically controlled tcpO2 microcirculation and reversed histologic changes in myelin thickness, axonal density, and diameter. 11,12 Improved neural and pedal arterial circulation may be important collateral benefits to the improved epidermal capillary flow and PIV recovery. 46 The immediate 30% improvement in tibial nerve vasa nervorum flow assessed by indocyanine green fluorescence during endoscopic tarsal tunnel ND may be supportive of neural function. 26 ND has reduced peripheral resistance and improved arterial pulsatility index and flow volumes at 3-month postoperative evaluation. 46
ND value in neuroischemia
Most clinical ND cohorts comprise only nDFU cases and exclude patients with n-iDFU because recommended surgical selection criteria advised that a palpable foot pulse or ABI > 0.7 be present before ND. 47 But one human study has demonstrated objective, measurable clinical benefit despite presence of neuroischemia. Trignano et al. used bilateral ND to treat 20 patients with DPN, all with bilateral leg tcpO2 values below the critical healing threshold of 40 mm Hg. 13 Eight of this neuroischemic cohort also had an open DFU at the time of surgery. At 18 months after ND, all DFUs had healed, none recurred, and no leg developed a new DFU. All 40 legs had improved oxygenation, with 38 of them having final tcpO2 values at or above the critical threshold of 40 mm Hg. Macrovascular PAD deficits were not present in this cohort nor were arterial revascularizations performed. So ND surgery has nicely demonstrated clinical benefit to microvascular CCI in this prospective DPN study. Use of ND in desultory, hard-to-heal wounds is being contemplated. Whether adding routine ND could improve outcomes of revascularization for PAD in diabetes is an interesting speculation worthy of investigation.
Strengths and weaknesses of ND
Weaknesses of ND therapy
A major weakness of ND surgery is lack of published Level I studies, although one completed Level I study with positive subjective outcomes has been published only as an abstract. 48 Another weakness is the paucity of ND studies. Based on a screening of the literature, the seven studies cited here are the only known published ND studies that include DFU recurrence data. Furthermore, the ND studies have all had relatively small enrollment sizes, varying from 8 13 to 206 49 for a total of 526 patients. Another weakness of ND is that while it alleviates some of the symptoms of DPN and mitigates the onset and recurrence of DFUs and amputations, it does not treat the metabolic components of DPN. Mechanical compression is resolved, but the neuropathy remains after ND. In addition, it is not possible to statistically compare the results of ND in nDFU and n-iDFU populations because of the patient selection criteria for the surgery. Six of the seven studies report on nDFU, and only Trignano et al. have studied ND in the n-iDFU population. 13
Strengths of ND
The association of diabetes and microcirculation has been known for 40 years. 50 ND is the only therapy that addresses the microcirculation dysfunction. ND also relieves compression of the accompanying blood vessels in the treated tunnels, which presumably improves blood flow in the vasa nervorum and in the microcirculation similar to what is seen in carpal tunnel release. It directly and acutely improves neuronal function as demonstrated by Anderson et al. 28 This would improve not only the motor axons but also sensory and autonomic fibers, including the sympathetic postganglionic fibers.
ND may have great relevance to the general framework of DFU care. The strongest evidence of benefit is for use in healed nDFU. In the six nDFU reports, the ND surgery has achieved 90% reduction in recurrence risk. Evidence is limited but suggestive that this would benefit patients with n-iDFU as well. Preliminary results of ND use in the indolent, recalcitrant, hard-to-heal DFUs are being studied and are encouraging. Microvascular improvements may be of additional value combined with PAD revascularization. 51 Confirmation of the observed 90% reduction in nDFU recurrence risk in future Level I studies would have huge economic impact on societal costs, particularly if it also applies to n-iDFU. 52
In 2005, Ioannidis published his essay “Why Most Published Research Findings Are False.” 53 This was instrumental in the rise of evidence-based medicine (EBM) categorizations and its implications of relative scientific strength and validity. For EBM, the most reliable evidence comes from the randomized, blinded controlled trial (RCT). This has led to a relative devaluation and denigration of evidence having lesser EBM degrees. But clinical observation and scrutiny of unexpected results can provide the initial clues that dogma may be incomplete or incorrect. Deprecation and belittlement of such evidence mean the pace of validating new and improved understandings is obstructed or greatly delayed. David Sackett, another EBM pioneer, was humble enough to observe that, “Half of what you’ll learn in medical school will be shown to be either dead wrong or out of date within five years of your graduation. 54 Thus, expert opinion and practice guidelines should always be viewed as evolving. Evidence trumps consensus. At times, this takes years.
Might the use of ND in DPN and DFU complications be such a situation? Ioannidis notes several conditions that militate for a lesser likelihood of being misled by research. These include the following: more teams involved, lesser prejudice, fewer financial incentives, larger study size, large effect size with p ≪ 0.05, well-defined outcomes, and absence of negative results. Scrutinized against such attributes, the observational studies of ND evidence for reduced nDFU recurrence risk measure up rather well. The literature shows that effect size for reduced nDFU recurrence risk is large with z-score <−4 and p value < 0.0001; no commercial interests benefit; current prejudice opposes ND; outcome is binary, visual, and objective; animal research parallels clinical outcomes; and only data-free, theoretical negative opinion has been published. 55 The recognition of EN existence, peripheral nerve compressions, and resultant impaired sympathetic control of microcirculation complete a scientific rationale for ND benefiting DPN and DFU recurrence.
The generally small study sizes of the published ND studies and the observational or prospective protocols would be improved by a Level 1 RCT. The study would not need to be huge because the apparent effect size of the ND studies already at hand is so great. Considering the severity and extent of the DPN/DFU problem and minimal evidence of ND surgical complications, some wound care practitioners have decided that the risk/benefit analysis already favors their use of this surgical approach. Others will hesitate, requiring the EBM process to be more complete and waiting for expert opinion to catch up. Some will be motivated to plunge into research to test and verify or debunk the ND approach.
SUMMARY
If the DFU problem was considered to rest upon three morbidities, they would be DPN, macrovascular PAD, and impaired microvascular circulation. PAD therapy aims to decrease macrovascular insufficiency with stents, atherectomy, thrombectomy, or bypass, i.e., a direct approach. Current SOC aims to directly optimize the local wound environment for healing, but the DPN and microcirculation are left unaltered and dysfunctional. Improving DFU microcirculatory dysfunction requires acting more indirectly, reducing total DPN by curtailing the contribution of the EN and local compressions to autonomic dysfunction. ND treats EN directly, whereas SOC fails to address it. ND can address both sensorimotor and neurovascular DPN impairments to the extent that EN and peripheral nerve compression are involved, and it does so at highly significant levels. This line of attack appears to be sufficient to regularly avoid the initial or recurrent DFU and thereby its complication cascade. Nobody believes or advocates that DPN is reversed in totality or cured surgically. But objective evidence shows that relieving the EN component due to physical nerve entrapment reduces serious DPN sequelae significantly. The evidence that ND for relief of EN compressions minimizes DPN and DFU complications needs considerably broader appreciation and research attention. Much benefit seems possible and probable.
Footnotes
ACKNOWLEDGMENTS
Graphics for Figure 1 and ![]() were developed by Nicole Ferola and Samantha Hueber, respectively.
were developed by Nicole Ferola and Samantha Hueber, respectively.
AUTHOR CONTRIBUTIONS
ABOUT THE AUTHORS
DISCLOSURE
No competing financial interests exist.
FUNDING
No funding was received for this article.