
Abstract
Significance:
Since the introduction of the first commercial negative pressure wound therapy (NPWT) system nearly three decades ago, several key technological innovations have led to the wide adoption of the therapy. This is a review of the history and innovation of commercial NPWT systems for adjunctive management of open wounds.
Recent Advances:
Technical modifications have broadened NPWT options to include innovative dressing interfaces, tubing configurations, power sources, capability of topical wound solution instillation or irrigation, canister versus canister-free configurations, smart technology, and disposable versus larger reusable therapy units. While these options complicate product selection, they have greatly expanded the potential to manage a wide variety of wounds in patients who previously may not have been candidates for NPWT.
Critical Issues:
Basic yet mandatory requirements of NPWT include delivering an accurate level of negative pressure to the wound bed, maintaining a seal, removing wound surface exudate through the dressing interface, and patient adherence to prescribed therapy. Meeting these requirements is challenging in the face of variable wound types, wound locations, exudate levels, and exudate viscosity. While there are a growing number of marketed NPWT systems, each may have different characteristics and performance. Evaluating the functionality of each system and relevant accessories is complicated, especially as additional manufacturers enter the market. Understanding the key innovations and specific challenges they are intended to solve may aid health care providers in selecting appropriate NPWT technologies for patients.
Future Directions:
Evolving technology, including artificial intelligence, will likely play a major role in redefining NPWT safety, simplicity, and reliability.

SCOPE AND SIGNIFICANCE
Since the first availability in the mid-1990s of commercially available negative pressure wound therapy (NPWT) systems, many iterations have been introduced, some of which have had a major impact on advancing the technology. This is a review of the history and innovation of NPWT systems for the management of open wounds.
TRANSLATIONAL RELEVANCE
To date, more than 1,939 clinical or basic research studies have been published regarding commercial NPWT use in open wounds. Basic research has focused on expanding the understanding of NPWT mechanisms, including its effect on various cells and tissues, blood flow, bioburden, exudate removal, lymphatic flow and edema, angiogenesis, and granulation tissue formation. 1 –5 Research has produced evidence that both expands upon and contradicts original findings of Morykwas and Argenta. 3,5 It has also revealed differences among individual NPWT systems and components. 6 –11 We review several NPWT system challenges, as identified through basic research, and resulting innovations that have improved clinical usefulness.
CLINICAL RELEVANCE
As of 2023, more than 25 companies worldwide are manufacturing NPWT systems with varying characteristics. It is difficult to judge the functionality of each system since standard performance criteria are not established. Despite the outward simplicity of NPWT system components, achieving negative pressure conditions that benefit patients with a wide variety of wound types involves optimization of a complex network of interactions. 12 Ongoing research and clinical use have prompted many technological innovations in the past three decades. Understanding major innovations that have occurred in certain NPWT systems may help inform product selection to fit patient/wound requirements and positively influence outcomes.
BACKGROUND
Use of negative pressure for wound management dates to the earliest Roman civilizations with use of the human mouth. 13,14 The first modern-day recorded application occurred in the 19th century, 15 and, fueled by the Soviet–Afghanistan War, Russians advanced negative pressure wound care in the 1980s. 16 The “vacuum sealing” technique was introduced into clinical practice in the early 1990s by Fleischmann et al., 17 and commercialization of scalable NPWT systems began in the mid-1990s, predicated by the works of Morykwas and Argenta. 18,19
The first commercial version of NPWT consisted of a reticulated open-cell foam (ROCF) dressing sealed by an acrylic adhesive drape and connected via single-lumen tubing to a suction device. The system was manufactured and marketed by one company (V.A.C.® Therapy, KCI, San Antonio, TX). Patent protection supported KCI’s position as a leading supplier of NPWT for the first 15 years after the introduction of V.A.C.® Therapy. Therefore, much of the history and innovation discussed in this publication concerns NPWT systems manufactured by KCI, although all attempts have been made by the authors, all of whom are former or present employees of 3M, to include influential innovations contributed by other NPWT system manufacturers.
Limitations of the original single-lumen NPWT system prompted numerous key technological innovations over time, including different tubing configurations, dressing interfaces, power options, integration with topical wound solutions, therapy unit sizes, exudate storage options, and software (Table 1). 20,21 While these options may have complicated product selection, they have greatly expanded NPWT utilization across surgical disciplines.
NPWT, negative pressure wound therapy.
Today, commercially available NPWT has been widely adopted for the treatment of acute and chronic open wounds and across most specialties, including plastic, 22 orthopedic, 23,24 trauma, 25 cardiac, 20 abdominal, 26 and gynecological, 27 as well as in outpatient wound centers. 28 NPWT utilization has also expanded to help manage closed postsurgical incisions or as a method of temporary abdominal closure in the open abdomen, but product descriptions and publications supporting these indications are outside the scope of this review.
In their original research, Argenta and Morykwas observed that application of controlled suction through an open-cell foam created an environment conducive to healing and enhanced granulation tissue formation. 18 Their clinical observations in addition to animal studies suggested that stimulation of perfusion, reduction of edema, and the response of surrounding tissues to mechanical forces were interrelated mechanisms of action of NPWT with ROCF. 19 Subsequent research has focused on the concepts of macro- and microdeformation to further elucidate the effects of NPWT. 3,29 Macrodeformation is the visible contraction of the wound that occurs when negative pressure is applied to an open-cell foam. 3 The effects of macrodeformation are seen on the wound tissue edge where negative pressure mechanically pulls the wound edges toward the center while facilitating wound exudate removal. 30
With negative pressure applied at the wound–foam interface, the struts in the reticulated polyurethane foam push down on the cell surfaces, while stretching cells upward, thus applying strain to the cells. 3 This interaction is termed micro-deformation, and this mechanical stretch/strain stimulates a cascade of activated molecular responses. 3 These responses may include cell division, 4 granulation tissue formation pathways, 3 and angiogenesis. 31,32 However, the specific mechanisms by which these occur continue to be debated. 33 Microdeformational wound therapy systems also remove fluids, including potentially infectious materials, away from the wound site and into a canister. 29 It has been reported that soft tissue wound exudates removed during NPWT comprise a significant loss of protein, immunoglobulins, and electrolytes, which should be considered when assessing protein requirements. 34
Numerous factors should be assessed before instituting NPWT. These include, but are not limited to, type, size, and location of the wound, patient comorbid conditions, and treatment goals, as well as the experience level of the treating clinician. However, the focus of this review is on the history and innovation of NPWT systems themselves.
Basic yet mandatory requirements of NPWT include delivering an accurate and prescribed level of negative pressure to the wound bed, maintaining a seal application for a minimum number of hours per day, and removing exudate through the dressing interface. All components of the system—the therapy unit, software, tubing, dressing, and sealing drape—play a critical role in NPWT outcomes. Ongoing testing of the functionality of each of these components over the past three decades has expanded usage of commercial NPWT to adjunctively manage a wide variety of wound types, wound locations, exudate levels, and exudate viscosities.
Continued research and clinical usage have revealed limitations for all original components of commercial NPWT, leading to many iterations of the system over time. While some innovations appear to have been subtle tweaks, other innovations have been quantum leaps in solving problems of usability and reliability, allowing for significantly larger subsets of patients to use NPWT (Fig. 1). We review what are arguably the most influential technological innovations for commercial NPWT system use in open wounds, and the impetus and implications behind each of the changes.
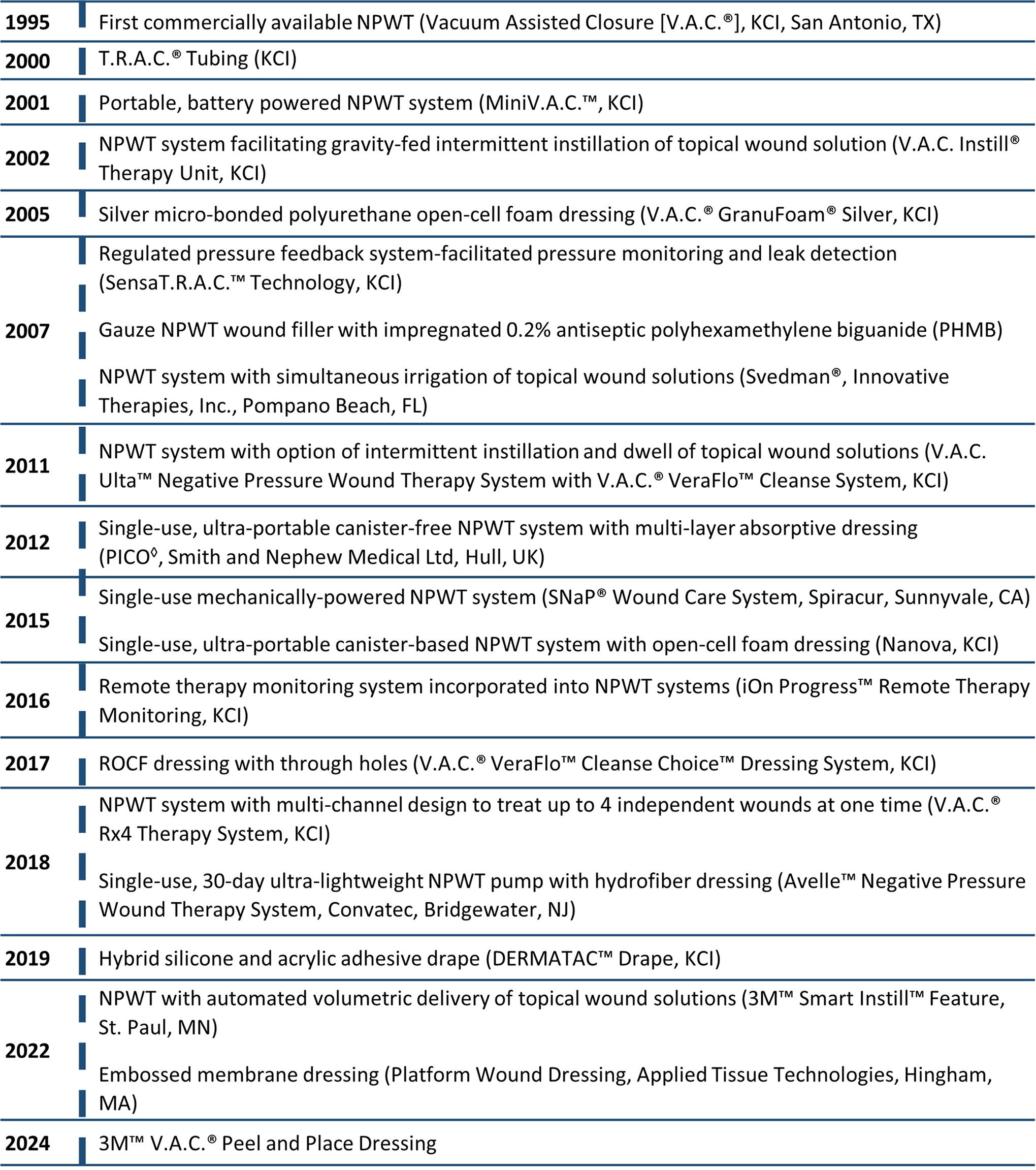
Time line of influential commercial negative pressure wound therapy innovations.
DISCUSSION
Challenge #1: Application of consistent, accurate negative pressure at the wound site
Maintaining a controlled and accurate level of negative pressure across the wound bed is necessary for effective NPWT, 35,36 as it impacts the magnitude of microdeformations at the cellular level that stimulate fibroblasts to proliferate, migrate, and produce collagen for wound closure. This is particularly critical for hard-to-heal wounds. 37,38 In order for NPWT to be effective, a sufficient level of mechanical stimulation is required for both angiogenesis and maturation of the microvasculature in the wound and periwound to facilitate tissue growth through neovascular supply. 12,31,39
A finite element computer model showed that most simulated tissue elements stretched by NPWT with the original ROCF experienced deformations of 5–20% strain, similar to in vitro strain levels shown to promote cellular proliferation. 4 However, this model was based on a sealed system with a consistent application of −125 mmHg. Drops in absolute negative pressure delivered to the wound will slow or halt the healing process. 36,40 –42 Orlov and colleagues 36 reported that pressure below −40 mmHg at the wound bed adversely decreased periwound stimulation around a 120 mm × 70 mm wound to less than one-third of the baseline stimulation. Further decreases to −20 mmHg or lower resulted in complete lack of periwound mechanostimulation. 36
In 1996, reports indicated that NPWT systems that used a single-lumen tube to connect the dressing to the NPWT therapy unit did not consistently provide pressure at the wound site. Clinicians reported that the therapy unit displayed the programmed level of negative pressure, even when the tubing was clamped closed or kinked. In those situations, no therapy was applied to the wound as there was no capacity for a safety alarm to alert the clinician of the blockage. Resolving this problem involved re-engineering single-lumen tubing to a multilumen tubing, utilizing four “pressure sensing” pathways incorporated in isolation from the large centrally located lumen through which exudate is removed (Fig. 2). 35 The reconfiguration coupled with the new therapy unit software enabled detection of pressure disruptions and blockages while providing appropriate alarms. This multilumen innovation to the original NPWT system (V.A.C.® Therapy, KCI, San Antonio, TX) is yet to be adopted in all commercially available NPWT systems.
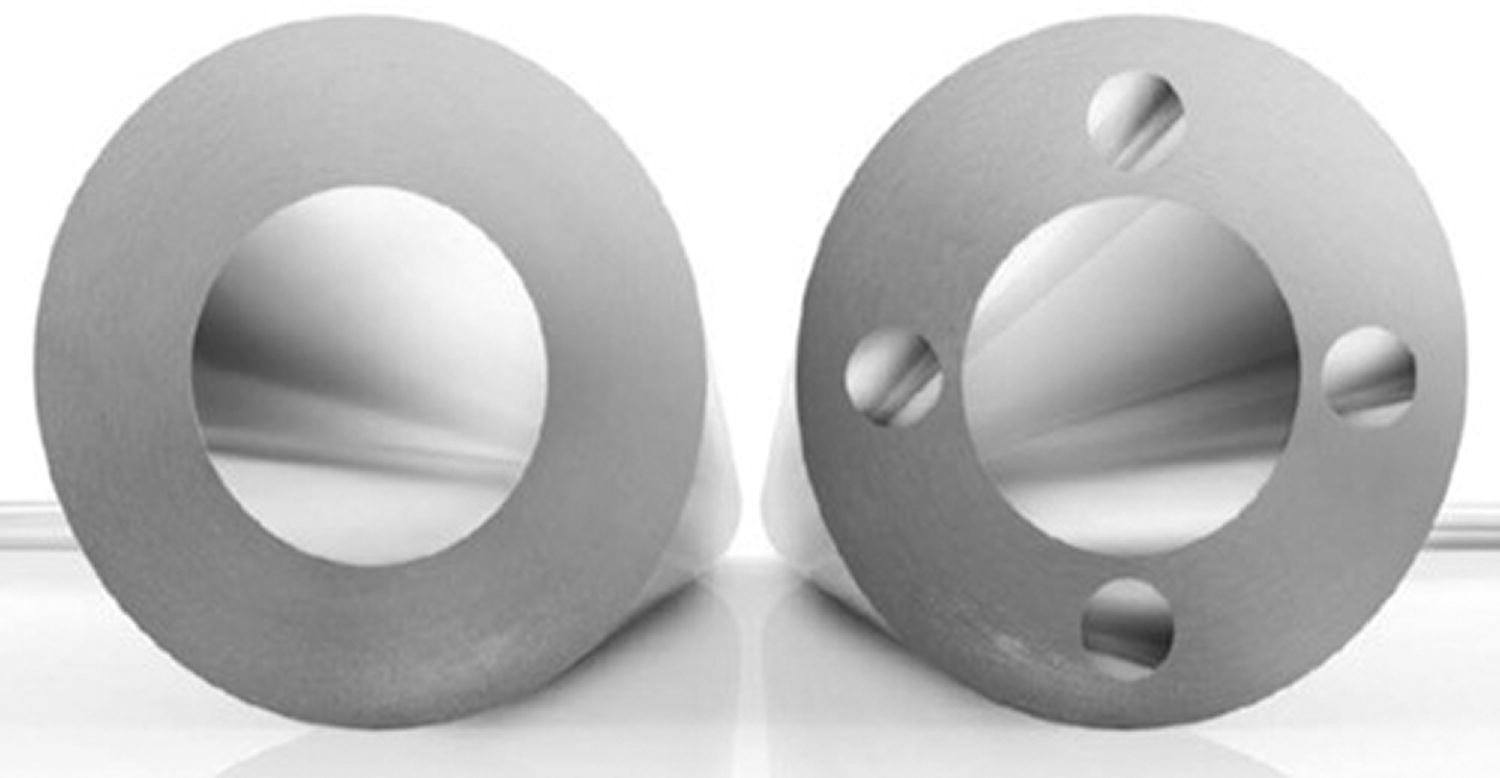
Single-lumen tubing (left) and multilumen tubing (right).
Researchers also observed that air leaks, changes in wound exudate characteristics such as volume and/or viscosity, and variability in NPWT unit placement relative to the wound location could also impact the system’s ability to deliver the programmed negative pressure to the patient’s wound. 35 Sensors in the V.A.C.® therapy unit were then interfaced with the pressure sensing and exudate transporting lumens to continuously monitor the actual pressure applied and adjust pump output to compensate for changes in wound and NPWT unit height as well as exudate characteristics. 35
Soon afterward, the multilumen tubing was integrated with a novel pad that greatly simplified the process of connecting the NPWT unit to the wound dressing. The previous single-lumen tubing had a blunt end that was physically embedded into the foam dressing and required the creation of an adhesive drape mesentery to be carefully wrapped around the tubing to obtain an airtight seal. 19 The new pad was designed with small “feet” to be placed over a hole cut in the adhesive drape where it touched the foam, to allow better negative pressure distribution to the foam and wound bed. 35,43
Therapy unit software was revised to complete the regulated pressure feedback system between the therapy unit, pad and dressing. The first version of this feedback system was incorporated into certain NPWT systems (V.A.C. Freedom™, KCI, San Antonio, TX) in 2002. This tracking technology was officially named SensaT.R.A.C.™ (KCI, San Antonio, TX) in 2007 with the subsequent redesign of the pad that replaced the “feet” or pegs with a more flexible flat design of the SensaT.R.A.C. pad, incorporating integral pathways to help guide exudate to the center lumen (Fig. 3). Dual-lumen pressure feedback systems have since been incorporated into some other commercially available NPWT systems. 36,44

Negative pressure and blockage sensing pad as a low-profile dome with channels to guide fluid away from the sensing ports (V.A.C. SensaT.R.A.C.™ Pad, KCI).
When the first commercial NPWT system (V.A.C.® Therapy, KCI, San Antonio, TX) received United States Food and Drug Administration (FDA) 510(k) product clearance in 1995, the original U.S. FDA product code description for an NPWT device listed it as a “powered suction pump intended for wound management and reduction of wound complications via application of negative pressure to the wound, which removes fluids, including wound exudate, irrigation fluids, and infectious materials.” Following the improved accuracy of the new pressure feedback system and subsequent peer-reviewed evidence of positive clinical outcomes, the FDA indications were changed in 2006 to: “intended to create an environment that promotes wound healing by secondary or tertiary (delayed primary) intention by preparing the wound bed for closure, reducing edema, promoting granulation tissue formation and perfusion, and by removing exudate and infectious material.” At present, only a few NPWT systems are equipped with accurate pressure sensing systems and are thus labeled with this new FDA indication, while most NPWT system manufacturers use labeling with the original FDA wording.
Another important engineering feature, introducing air into NPWT systems either via multiple lumens or through dressings with a high moisture vapor transmission rate (MVTR) outer film, has been recognized as vital to efficiently move exudate out of the wound and augment fluid movement into the canister. The air pathway lumens are intended to be free of wound exudate. Air pathway lumens are required to accurately measure and manage pressure at the wound site. McNulty et al. (2010) established in a benchtop model that a system with single-lumen tubing did not compensate for changing fluid properties at the wound; a −22.4 mmHg pressure drop could occur for every 30.5 cm that exudate travels against gravity. 35
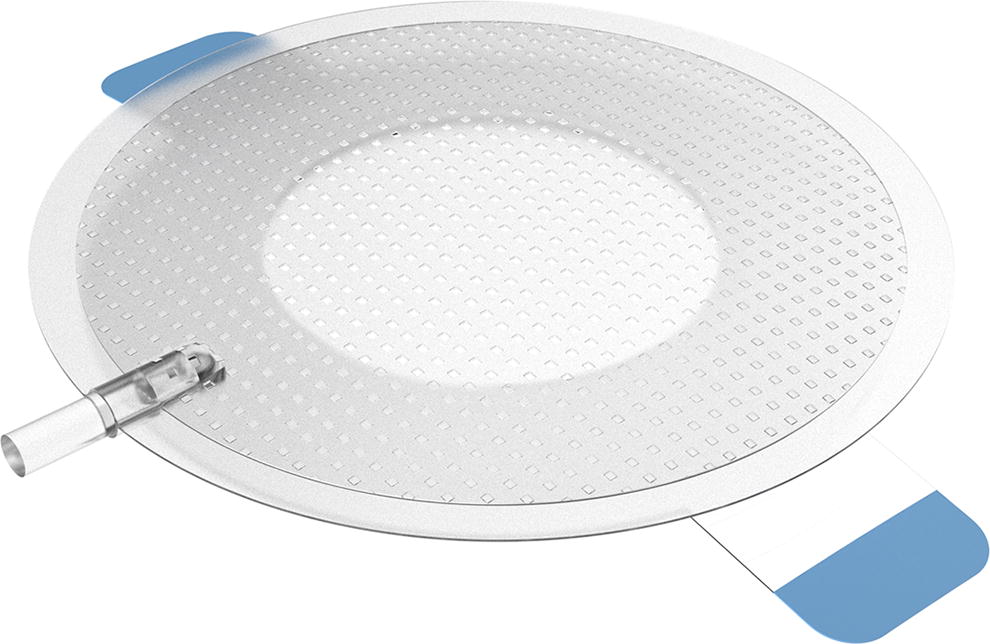
Under certain conditions, difficulties in maintaining consistent, intended negative pressure have also been observed with ultralightweight, canister-free NPWT systems. 36 Canister-free systems, compared with canister-based systems, are intended to simplify NPWT and are easiest to apply. This innovative technology is available from several manufacturers but was originally marketed by Smith and Nephew (PICO◊, Smith and Nephew Medical Ltd, Hull, UK). Most use a multilayer absorbent dressing with a high MVTR top film that allows transpiration of exudate vapor; delivery of negative pressure depends on continuous evaporation of wound fluids from the dressing (Fig. 4) using a disposable pump set at nominal −80 mmHg. 11

Multilayer absorbent dressing used with canister-free NPWT device (PICO◊ Fluid Management Pack, Smith and Nephew Medical Ltd, Hull, UK). NPWT, negative pressure wound therapy.
While an initial porcine study reported similar therapeutic levels of negative pressure between a canister-free, single-use system and a traditional NPWT system, 11 these results were contradicted in a recent computational finite element porcine model, where investigators observed significant drops in target wound bed pressure when the canister-free system multilayer dressing was saturated. 36 Investigators concluded in two different studies that a greater absolute negative-pressure level and its continuous, consistent delivery through controlled fluid management technology provided superior biomechanical performance by removing excess fluid from the dressing. The investigators noted that the canister-free technology negatively affected the delivery of consistent negative pressure over time. 10,36 Comparative clinical studies are needed to accurately determine the continuity of negative pressure applied to the wound bed and the associated clinical benefits under varying conditions and across different NPWT system models.
Challenge #2: Removal of high-viscosity exudate
Removal of exudate away from the wound is a fundamental mechanism of action of NPWT, prompting a cascade of events, including a reduction of edema and stimulation of blood flow. 3 The contact dressing launched with the original commercial NPWT system consisted of a hydrophobic polyurethane ROCF with a pore size between 400 and 600 µm. 19 Initial bench and animal testing and a vast majority of subsequent preclinical testing have been performed using ROCF that meets similar specifications, and this is the same foam predominantly used on NPWT patients today. Morykwas et al. determined from animal studies that these foam characteristics helped provide uniform distribution of negative pressure at the wound site. 19 The hydrophobic construction was selected to facilitate exudate removal. 19
Over time, however, numerous clinicians noted challenges in efficiently drawing copious or high-viscosity exudate through this ROCF, and this was also noted when gauze or PVA foam was used. 20,45,46 With traditional NPWT, thick exudate may remain pooled in the wound or coated on the wound-side of the dressing upon removal. To address this limitation, NPWT with instillation/irrigation (NPWTi) of a topical wound solution (including saline) was used to help dilute and thin out the exudate as well as solubilize devitalized tissue for removal. 47 NPWTi therapy units provide a mechanism for intermittent instillation and dwelling of topical wound solutions alternating with cycles of NPWT (NPWTi-d) or continuous irrigation of topical wound solutions during NPWT (NPWTi-c).
Significant changes to the original ROCF were also devised for effective removal of thick exudate and slough into the canister. A specialty ROCF (V.A.C. VeraFlo™ Dressing, KCI, San Antonio, TX), with similar density and pore size but less hydrophobicity than the traditional NPWT foam, was introduced with one commercially available NPWTi-d system (V.A.C.Ulta™, KCI, San Antonio, TX) in 2011 with a goal of enhancing fluid distribution properties down to the wound bed. The foam allowed the chosen topical wound solution to better cover the wound bed and dwell for a period of time, which improved removal of viscous exudate without the need to remove the dressing. 48 A porcine model also showed significantly increased thickness of granulation tissue after seven days with NPWTi-d/specialty ROCF compared with traditional NPWT. 48,49 However, clinically, it was noted there were still limitations to removal of some fibrinous debris with NPWTi-d and the less hydrophobic specialty ROCF. 50
An important breakthrough came in 2017 with a specialized ROCF that contained an array of “through holes” in addition to its reticulated pores (V.A.C. Veraflo Cleanse Choice™ Dressing, KCI, San Antonio, TX). The 1.0-cm-diameter holes spaced 0.5 cm apart created larger channels to allow the exudate and fibrinous debris to pass through and be removed from the wound surface (Fig. 5). 51,52 In the first published observational case series, Teot et al. reported that after 3 days of NPWTi-d with the holed foam, most of the nonviable tissue had been nonsurgically removed. 45 In the subgroup of 10 nonsurgically debrided wounds with a necrosis/fibrin cover, a rapid decrease in the amount of the nonviable/fibrinous tissue was observed at each dressing change. 45 Other authors concluded that NPWTi-d with ROCF with through holes provided efficient and rapid removal of thick exudate, fibrinous nonviable debris, and infectious materials. 53,54 Research is needed to validate the mechanisms of action of this newly configured ROCF dressing.

Reticulated open-cell foam with through holes (V.A.C. Veraflo Cleanse Choice™ Dressing, KCI).
Challenge #3: Bacterial clearance with NPWT
Chronic wound bioburden is typically polymicrobial, abundant, and extremely diverse, with staphylococci and pseudomonas species frequently identified in hard-to-heal wounds. 55,56 This complexity of microbial flora in chronic wounds has complicated the study and understanding of the relationship between bacterial load and wound healing. 5,57,58 Both planktonic and biofilm-protected bacteria can induce chronic inflammation in a local wound environment 59 and the quantitative reduction of bioburden has historically been considered important for chronic wounds to proceed to the proliferative phase of healing. However, multiple studies, including NPWT-treated 60 –62 and antimicrobial agent-treated 5,63,64 wound studies, have reported no apparent effect on wound healing despite quantitative increases in bacterial load.
In their earliest work, Morykwas and colleagues 19 investigated change in bacterial counts in acute artificial wounds in a porcine model after inoculation of gram-positive cocci. A significant decrease in bacterial counts was observed on the fifth day of NPWT treatment compared with controls. However, these results have not been prospectively replicated in human wounds, 65 and subsequent studies measuring bacterial load during NPWT have shown mixed results. 5 Some studies have shown a significant decrease in nonfermenting gram-negative bacilli, including Pseudomonas spp, after NPWT, 66,67 while other studies have shown no significant difference 66,68 or enhanced proliferation of gram-positive cocci, including Staphylococcus aureus, when the wound was cleared of gram-negative bacteria. 60,69 It has been postulated that NPWT may exhibit species selectivity, suppressing the growth of gram-negative bacteria, which in turn could allow for greater exploitation by gram-positive cocci. 5
There is also evidence that while bacteria and fungi may be removed from the wound surface during NPWT, accumulation of bacteria occurs within the foam. 6,70 While a sealed dressing helps protect against outside contaminants, the foam dressing itself can serve as a medium for bacterial colonization, particularly if the therapy unit is turned off for extended periods with the dressing in place. 71
In a systematic review of the influence of NPWT on bacterial bioburden, Glass et al. concluded that the earlier assumption that NPWT suppresses bacterial proliferation is oversimplified; rather, the studied mechanisms are complex and multifactorial. 5 Results of meta-analyses are complicated by the diverse variables, wound types, and characteristics studied, as well as differences in measuring methodology. 5 Experience with DNA-based molecular methods for microbial detection supports a comprehensive approach for controlling infection, including ongoing consideration of patient and wound factors that may contribute to increased vulnerability to microbial invasion. 57
Throughout this ongoing debate about NPWT and the associated bacterial bioburden clearance, several innovations have been aimed at reducing bacterial load during NPWT. In 2005, ROCF dressings with microbonded silver distributed throughout the dressing (V.A.C. GranuFoam® Silver, KCI, San Antonio, TX) were introduced for use with V.A.C.® Therapy systems. Results of an in vitro study investigating the antimicrobial effect of the dressing against pathogens commonly found in clinical settings, including Staphylococcus aureus and Pseudomonas aeruginosa, showed the silver ROCF dressing to be effective during antimicrobial testing with a 99.99% reduction in colony forming units, remaining effective after 72 h of simulated NPWT. 72 However, the lack of clinical studies evaluating bioburden reduction with the use of silver ROCF dressings with NPWT bars any definite conclusion regarding their clinical effectiveness.
The beneficial relationship between irrigation and healing has been recognized for centuries, and in fact, antiseptic solution instillation via syringe during intermittent pauses of negative pressure was used throughout the 1990s in the original vacuum sealing technique by Fleischmann and colleagues in Germany. 73 While this technique helped reduce orthopedic wound infection in Fleischmann’s series, their methodology was manual and time-consuming. The comparative effectiveness of various solutions for irrigation also remains controversial. 74 Nevertheless, instillation of topical wound solutions during early adoption of NPWT served as the impetus for future innovation. 75
One manufacturer began the process of engineering a timed, controlled method of intermittent instillation of topical wound solutions during NPWT. The first commercially available NPWTi system was introduced in 2002 (V.A.C. Instill® Therapy Unit, KCI), and initial studies showed reduced bacterial loads with NPWTi versus NPWT alone. 75 An NPWT system with simultaneous irrigation of topical wound solutions was introduced in 2007 (Svedman®, Innovative Therapies, Inc., Pompano Beach, FL). 76 Instillation technology was upgraded in 2011 (V.A.C. Ulta™, with V.A.C.® Veraflo™ Therapy, KCI) to allow delivery of the topical solution to the wound at a preset volume and dwell time (NPWTi-d) during intervals of paused negative pressure.
Contrary to traditional NPWT, reduction in bacterial load has been consistently reported across studies of NPWTi-d. 77 –80 This has redefined the subset of patients that can be treated with NPWT to include patients with infected wounds. 47 Reduced bacterial bioburden has been reported with instillation of saline 81 as well as antiseptics such as polyhexanide (concentration 0.005–0.04%) 82 and acetic acid (concentration 0.25%–1%) 83 in acute and chronically infected wounds. 84 According to the manufacturer’s guidelines, however, NPWTi-d systems and FDA-cleared topical wound solutions are not indicated to treat wound infection. They are to be used in conjunction with good clinical practice for treating the infection, such as systemic antibiotics and debridement as appropriate. Although prophylactic use of topical antiseptic agents has been recommended in certain situations, 47,84 it is important to acknowledge that extended use of topical antiseptic solutions may be toxic to tissues and may impede acute wound healing. 85
In 2022, NPWTi-d therapy units were re-engineered with “smart” technology (3M™ Smart Instill™), consisting of upgraded software that automatically determines the volume of solution needed, with a goal of preventing over and under filling of the dressing, and reducing guesswork and setup time for staff. Commercial availability of NPWT systems that provide automated volumetric delivery of topical wound solutions at customizable time intervals has been a major leap toward applying the benefits of NPWT to cyclic cleansing. These innovations have occurred over a long period, and well-designed research studies are needed to further elucidate the comparative clinical effects of NPWTi-d with various topical wound solutions.
Challenge #4: Presence of necrotic tissue
When NPWT was first cleared for marketing by the FDA in 1995, “necrotic tissue with eschar” was listed as a contraindication. One reason for this contraindication was that NPWT was intended to draw wound edges together and remove exudates. The presence of necrotic tissue with eschar prevents optimal wound macrostrain and is known to delay wound healing. Therefore, eschar would need to be removed before application of NPWT via mechanical, enzymatic, autolytic, or sharp debridement. This excluded a large subset of patients with wounds that could not be debrided for a variety of reasons.
This requirement for a wound to be free of eschar and largely free of other nonviable tissue remains for traditional NPWT. However, studies have recently demonstrated removal of slough and other nonviable tissue during NPWTi-d with the previously mentioned ROCF with through holes. 45,52 –54 Following publication of study results in 2023, the FDA cleared a new claim of “hydromechanical removal of infectious materials, nonviable tissue, and wound debris, which reduces the number of surgical debridements required, while promoting granulation tissue formation, creating an environment that promotes wound healing.” Subsequently, “necrotic tissue with eschar” was removed by the manufacturer from the list of contraindications, but solely with respect to NPWTi-d use with two types of ROCF dressings with through holes (3M™ V.A.C. Veraflo Cleanse Choice™ and 3M™ Veraflo™ Cleanse Choice Complete™, 3M, St. Paul, MN). Instructions for the ROCF dressings with through holes do advise that clinicians should consider removing or cross hatching eschar to optimize therapy.
Challenge #5: Maintaining adequate drape adhesion and avoiding skin damage
Macro- and microdeformation with NPWT must occur within a vacuum environment by extracting air from the foam or gauze dressing, allowing for a reduction in the size of the dressing and the ensuing resultant mechanical forces to be applied. This is accomplished by using an adhesive outer film dressing, often referred to as the “drape.”
The most common configuration of NPWT involves creating a hermetically sealed chamber at the periwound/wound surface via ROCF that is covered by a flexible adhesive drape, extending from the wound to 3–5 cm of the intact periwound skin, and then connected to a negative pressure therapy unit. To function optimally, the system must be able to achieve and maintain an airtight seal, which requires secure attachment of the dressing to the skin. 86 Seal leaks with loss of negative pressure can lead to wound dehydration, periwound maceration, necrosis, and delayed wound healing, and pain and discomfort for the patient, as well as take additional nursing time. 87 Elimination of air leaks and resulting leak alarms can help reduce patient and clinician anxiety and encourage effective continuation of NPWT. 88,89
Dressing kits of nearly all NPWT system manufacturers contain a flexible polyethylene drape with a tacky side, coated with the same acrylate adhesives that have been used in medical tapes and devices for decades. 86 While use of an acrylic adhesive drape often results in a tight seal, application of the drape can be cumbersome, and the drape cannot be repositioned after placement. There is added complexity in problematic areas such as in moist skin folds, over previously damaged periwound skin, or in the presence of ongoing incontinence. Application time can be extensive and many “work arounds” may need to be made to not only obtain the initial seal but maintain it for 48–72 h. 90 This can lead to increased time, material waste, and cost.
Unfortunately, the benefits of a strong adhesive can morph into a challenge, as the adhesive cures over time and can be painful for the patient as well as time-consuming for the staff to gently remove in a time-efficient manner. As with removal of any adhesive drape, a certain number of epidermal cells will be removed from the skin, increasing the risk of medical adhesive-related skin injury (MARSI), which can further harm surrounding skin and cause pain and discomfort for patients. 91
Lack of skin preparation and incorrect removal of acrylate adhesives further increase this risk. 91 If the adhesive is removed quickly, abruptly, or at a steep angle versus more parallel to the skin (“low and slow”), or if the skin is fragile, as with the very young, very old, or the immune suppressed, skin stripping or blister formation can occur. The clinical requirement for repeated dressing changes also predisposes the patient to increased risk of periwound complications. Adhering to correct dressing application and removal techniques, as well as other recommendations for preventing MARSI, is critical in reducing potentially preventable related morbidity. 91
Skin-friendly drape technologies have been introduced to enhance drape usability and reduce MARSI risk. In 2012, a single-use ultralightweight negative pressure device (PICO◊, Smith and Nephew Medical Ltd, Hull, UK) was launched with the first 100% silicone drape. Silicone adhesives are quite different in how they interact with the skin to adhere. Compared with the acrylate, this type of adhesive is very gentle to the skin upon removal. While gentle to the skin, silicone adhesives can be limited in their ability to adhere well and maintain a seal, especially over moist skin areas, in diaphoretic patients, or in areas with high friction due to patient movement. As a result, this single-use NPWT system requires the four outer edges to be sealed with precut acrylic adhesive fixation strips to assist dressing adhesion.
The need to balance skin adhesion, usability, and patient comfort led to the development in 2018 of a new hybrid drape with a pattern of silicone adhesive interspersed with acrylic adhesive (3M™ V.A.C. Dermatac™ Drape 3M, St. Paul, MN) (Fig. 6). Published data regarding this new silicone/acrylic hybrid drape are positive but limited to small case series. 9,92 Fernandez et al. reported that the drape was easy to reposition during initial application and maintained a negative pressure seal. 92 No periwound skin irritation was observed in any of the patients. The authors found that the hybrid drape had similar adhesive capabilities compared with the standard polyurethane drape system. The ability to reposition the hybrid drape while retaining adhesion saved time and waste. Patients also reported less discomfort and irritation in the area surrounding the wound versus the standard acrylate drape. 92

Hybrid drape made of silicone (outside of the circles) and acrylic (within circles) adhesives (3M™ V.A.C. Dermatac™ Drape).
However, concerns remain with the use of circumferential dressings with NPWT, regardless of the drape material. Difficulties may include achieving a seal during application and preventing circulatory compromise from the circumferential compression on the extremity. 93 If a circumferential application is considered, extreme care should be taken to not stretch or pull the drape when securing it, but to attach it loosely, and to perform systematic palpation of distal pulses and regular distal circulatory status assessments. 90
Challenge #6: Patient adherence to keep therapy on
For NPWT to be successful, negative pressure must be applied to the dressing while the dressing and sealed drape are in place. Most manufacturers’ instructions state that if the NPWT unit is turned off for more than two hours, the dressing needs to be removed and a new dressing applied. 90 Infection is one of the most common adverse events reported with NPWT, 94 and it can result from prolonged periods of interrupted therapy with the dressing in place. 7,8
Throughout the history of commercial NPWT, there have been reports of NPWT being turned off for prolonged periods of intentional or unintentional interruptions of therapy (Table 2). 7,8 Patients in unmonitored settings may disconnect from or turn off the therapy unit, not fully understanding the risks associated with this decision. It can be difficult to determine the value of NPWT due to wide fluctuations in patient adherence.
To help assist patient adherence in maintaining negative pressure while the dressing is in place, a remote therapy monitoring system (iOn Progress™, KCI, San Antonio, TX) was developed and installed on certain NPWT systems in 2016 to provide real-time monitoring of patient adherence to the prescribed therapy. 95 The system includes a network of trained professionals who call patients when their NPWT usage is lower than prescribed and provide education to assist with therapy adherence. A study performed within two years after introduction of the remote monitoring system determined that of 979 calls to 198 patients, 157 (16.0%) of the calls were due to low patient adherence (therapy unit turned off). 95 The day following an educational patient phone call, adherence increased 73% of the time by an average of 8.5 h. The authors concluded that patient adherence could be influenced through active engagement. 95 A subsequent review of payer claims data from 1,105 patients showed that, compared with patients with NPWT and no remote therapy monitoring, patients with NPWT and remote therapy monitoring had higher NPWT costs ($3,757 vs. $3,289; p = 0 .0035) but lower wound-related non-NPWT costs ($7,361 vs. $11,462; P = 0.0045), resulting in overall wound cost savings. 96 Future combinations of real-time monitoring of patient adherence and wound characteristics could be valuable tools for measuring therapy effectiveness.
NPWT, negative pressure wound therapy.
Challenge #7: Limiting tissue ingrowth into foam
In a 2003 porcine study, Morykwas et al. 97 evaluated histological infiltration of tissue into the ROCF dressing. Two days post application, no ingrowth was noted. On days 3 and 4, however, increasingly organized granulation tissue matrix formation was noted as proteins and cells migrated into the foam. 97 Similar results were reported in 2019, in a different porcine study performed to evaluate the impact of dressing change frequency on the peel force of NPWT ROCF dressings at removal on days 3, 4, or 7. 98 As the number of days between dressing changes increased, the peel force needed to remove the dressing increased. On day 4, not only was the peel force increased, but remnants of foam were also noted in the wound. At 7 days, removal caused bleeding and required surgical removal of the foam dressing. The authors concluded that these results underscored the need for a standard dressing change frequency of every 2–3 days for ROCF dressings. 98
In addition to adjusting dressing change frequency, clinicians have used various techniques, such as placing a nonadherent dressing interface on the tissue beneath the ROCF, to limit tissue ingrowth in situations of robust cellular response during NPWT with ROCF. In cases of exposed vital structures, such as bowel, heart, or vessel, it becomes even more important to protect tissue to reduce the potential for damage at the ROCF-vital structure interface. If natural tissue is not available, multiple layers of a nonadherent material may be considered to provide a complete barrier between the structure and the ROCF. 90
Although ROCF is the predominant dressing used with NPWT, some clinicians use other dressing materials, such as gauze (with or without a nonadherent layer), to limit tissue ingrowth and to fill irregularly shaped wounds, due to ease and conformability to the wound bed. 20,99 PVA foam has also been used to limit tissue ingrowth, 11,25,100 and in Europe, some clinicians use a polymeric membrane dressing (PolyMem WIC®, Ferris Manufacturing Corp, Ft. Worth, TX) to minimize the ingrowth issue with NPWT. 101 Soaking the wound bed underneath the ROCF with sterile normal saline has also been shown to facilitate dressing removal. 90 If using NPWTi-d, a soak feature option is available for applying the topical wound solution to the wound bed before dressing removal.
An alternative to both ROCF and gauze is the embossed membrane Platform Wound Dressing (Fig. 7) (PWD®, Applied Tissue Technologies, Hingham, MA), 102 however, this dressing has just recently entered the market and its utility is yet to be thoroughly investigated. In addition, preclinical results of an all-in-one peel and place dressing, which may be left in place up to seven days without tissue ingrowth, have recently been published. 103,104 This dressing uses a multilayer construction with a polyurethane manifolding core, and a fenestrated hybrid silicone-acrylate adhesive drape as the periwound interface. 103 Significant reductions in force needed to remove the novel dressing after seven days of treatment compared with ROCF were noted and no foam fragments were observed in the wounds in the study arm compared with control. Greater re-epithelialization levels and faster wound fill with a corresponding decrease in wound area were also evident with the novel dressing versus control. 103 The results of this study are promising, but the dressing is not yet widely commercially available. Notably, these dressings have specific instructions pertaining to wound depths, geometries, and wound fillers. 101,103,104
Platform wound dressing with no foam or gauze (PWD®, Applied Tissue Technologies).
SUMMARY
While the application of negative pressure to treat wounds is not new, the commercialization of NPWT systems for clinical use has stimulated innovation and resulted in numerous new applications. Major technical innovations, including different dressing interfaces, tubing configurations, power options, allowance for hydromechanical removal of nonviable tissue, canister versus canister-free configurations, smart technology, and disposable versus reusable devices, have expanded the options for managing a wide variety of diverse wounds and patients, both in and out of acute care settings. Managing a wide variety of wound types, wound locations, exudate levels, and exudate viscosities using NPWT can be challenging. Reducing these challenges and improving outcomes have led to many design changes to all components of the original commercial NPWT system—the therapy unit, software, tubing, dressing, and sealing drape.
Today, the product selection process can be complex due to the growing number of options in commercial NPWT systems, each with multiple features that continue to evolve. New technologies have been aimed at enhancing healing through various means, including ensuring delivery of the target negative pressure to the wound bed, reducing tissue ingrowth into dressings, removing high viscosity exudate, impacting bacterial clearance, balancing drape adhesion with avoidance of skin damage, and improving patient adherence to prescribed therapies. Awareness of some key innovations that have occurred may assist clinicians in selecting NPWT systems to fit patient and clinical requirements. In the interests of brevity, these authors have highlighted innovations that have addressed several key challenges with use of NPWT, but this is by no means an exhaustive list of all NPWT challenges and shortcomings. Ongoing developments to enhance NPWT system simplicity and mobility are needed, but reliability and safety must be inherent in the design. Well-designed clinical research is crucial to determine the effects of each innovation in the context of specific wound conditions and to establish performance criteria for NPWT system comparisons.
TAKE-HOME MESSAGES
Commercial NPWT has become an integral tool for managing a wide variety of acute and chronic wounds. All original components of commercial NPWT—the therapy unit, software, tubing, dressing, and sealing drape—have undergone significant advances over the past three decades to improve functionality, usability, and reliability. NPWT innovations have been aimed at enhancing healing through various means, including ensuring delivery of the target negative pressure to the wound bed, reducing tissue ingrowth into dressings, removing high-viscosity exudate, impacting bacterial clearance, balancing drape adhesion with avoidance of skin damage, and improving patient adherence to prescribed therapies. A basic understanding of the history of commercial NPWT system development may help establish comparison or testing criteria to guide product selection in terms of functionality, efficacy, and reliability.
Footnotes
ACKNOWLEDGMENTS AND FUNDING SOURCES
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
AUTHOR DISCLOSURE AND GHOSTWRITING
C.M. and K.B. are employees of 3M. All authors contributed to the design and writing of this article and no ghostwriters were used.
ABOUT THE AUTHORS