
Abstract
Significance:
The incidence of chronic wounds is increasing due to our aging population and the augment of people afflicted with diabetes. With the extended knowledge on the biological mechanisms underlying these diseases, there is a novel influx of medical technologies into the conventional wound care market.
Recent Advances:
Several nanotechnologies have been developed demonstrating unique characteristics that address specific problems related to wound repair mechanisms. In this review, we focus on the most recently developed nanotechnology-based therapeutic agents and evaluate the efficacy of each treatment in in vivo diabetic models of chronic wound healing.
Critical Issues:
Despite the development of potential biomaterials and nanotechnology-based applications for wound healing, this scientific knowledge is not translated into an increase of commercially available wound healing products containing nanomaterials.
Future Directions:
Further studies are critical to provide insights into how scientific evidences from nanotechnology-based therapies can be applied in the clinical setting.

Scope and Significance
This review highlights new nanoplatforms created for the treatment of chronic wounds, specifically diabetic wounds. We briefly introduce the despaired wound healing of chronic wounds and drugs/biomolecules that are being used and particularly discuss the use of nanoparticles (NPs), nanofibers, and liposomes in the treatment of diabetic wounds, emphasizing their mechanisms of action.
TRANSLATIONAL RELEVANCE
Nanotechnology driven therapeutics can influence a specific biochemical event within the impaired healing process, being able to change one or more wound-healing phases.
This offers unique opportunities compared to dressing-based conventional wound care products.
A major advantage of these nanoplatforms is their adaptability and tunability. For instance, nanotherapeutics can be used in controlled and sustained released of the active ingredient over a period of days or weeks, while conventional delivery systems such as dressing films or gels can sustain the release of the therapeutic agent over 1 to 2 days.
CLINICAL RELEVANCE
Chronic wounds have an important economic impact in developed countries, and it is expected to increase as the population ages. Current therapies cannot fully address the impaired healing, provoking wound complications like infections and poor wound closure. Thus, new biomolecules and therapies that promote wound healing, prevent wound infections, or inflammation, among others, are needed. Several nanotechnological approaches with multiple functions and different mechanisms have proved their potential in wound animal models and could be the next generation of wound nanotherapies.
BACKGROUND
Chronic wounds
Chronic wounds exhibit a disturbed repair process, provoking that wounds would not heal within 3 months. 1 Among them, nonhealing pressure ulcers (NHPUs), venous ulcers (VUs), and diabetic foot ulcers (DFUs) are the most common ones. VUs are caused by dysfunctional blood valves or obstructed veins, mainly in legs. In contrast, NHPUs are skin and underlying tissue injuries caused by prolonged skin pressure in people confined to bed or with limited mobility for long time periods. DFUs often start from several diabetes complications such as foot deformity, peripheral arterial diseases, and peripheral neuropathy. Diabetic neuropathy is the result of nerve damage caused by uncontrolled glucose blood levels, and it reduces the skin sensitivity. Foot deformation leads to the formation of keratosis and callus, resulting in wound aggravation and even gangrene. Diabetic patients have also alterations in the capillary system (thickening of basement membrane, reduced capillary size, etc.). Over time, alterations in the glucose levels contribute to vasoconstriction and plasma hypercoagulability, developing occlusive arterial disease, ischemia, and ulcer formation (peripheral arterial disease).
Nonhealing ulcers have a considerable impact for patients and their families. These types of wounds cause loss of function, morbidity, severe pain, infections, hospitalization, and in some cases amputations.
Chronic wounds mostly arise associated to population aging, obesity, and diabetes, increasing the health costs. 2 This disease is often not regarded as a high priority compared to other conditions because it is not considered to be life-threatening. 3 Chronic wounds prevail as a silent epidemy affecting the well-being of over 40 million people in the world. 4
Most of the common features of chronic wounds include an extended inflammatory phase, existence of persistent infections, formation of bacterial biofilms, as well as higher levels of proteases and reactive oxygen species (ROS). 5 Furthermore, dermal and/or epidermal cells residing in chronic wounds fail to respond to reparative stimuli. These cells present phenotypic abnormalities such as lower expression of growth factor (GF) receptors, as well as lower mitogenic potential, preventing their response to external environmental cues. 6 The higher levels of proteases in chronic wounds promote the destruction of extracellular matrix (ECM), GF receptors and GF like platelet-derived growth factor (PDGF), vascular endothelial growth factor (VEGF), keratinocyte growth factor (KGF), and transforming growth factor-beta (TGF-β). 6
The higher ROS levels observed in chronic wounds also stimulate the ECM destruction and cell damage. All these cellular abnormalities do not allow the formation of granulation tissue and ECM deposition, resulting in the formation of nonhealing wounds. Another feature of chronic wounds is impaired angiogenesis. Angiogenesis is a physiological process required for wound healing. In normal wound healing this process depends on the balance between the growth and proliferation of vessels and their maturation and quiescence. In diabetic patients, this balance is disrupted. Endothelial cells exposed to elevated glucose levels have been reported to become senescent leading to integrity loss and eventually apoptotsis. This decreased angiogenesis is also due to macrophage deficit present in these wounds, since these cells produce high levels of VEGF and other pro-angiogenic mediators. 7
Current treatments of chronic wounds
Current treatment of chronic wounds depends on the wound etiology. In all cases, an adequate wound cleaning and debridement, a control of possible infections, and the use of wound dressings are needed. NHPU treatments include dressings that accelerate the wound healing and relieve the tissue pressure. However, DFUs and VU focus on dressing that maintains the moist environment conducive to wound healing and on compression. 8 Specifically, compression leg bandages are used in VUs to improve the vein circulation. Conventional dressings, such as gauze or gauze-woven cotton composite dressings, provide wound protection from bacterial contamination and allow gaseous/fluid exchange. They are used as secondary dressings to cover complex dressings or for the treatment of superficial and noninfected wounds. Specifically, compression leg bandages are used in VUs to improve the vein circulation. 9
These materials are characterized for their easy use and low cost. However, disadvantages such as frequent change needs, lack of control of moisture levels, and adherence to the wound bed have restricted their usage in wound management. 10
Nowadays, new synthetic dressings, capable of providing a suitable moist environment, are available.
These dressings are semiocclusive or occlusive. They can be in the form of film, foam, hydrogel, or hydrocolloids. They are fabricated using a variety of synthetic materials such as poly(vinyl alcohol) (PVA), poly(lactide-co-glycolide) (PLGA), polyurethanes, polyethylene glycol (PEG), polycaprolactone (PCL), nylon, or silicone. Among them, hydrogels are seen as promising biomaterials suitable for wound dressings due to their high-water content. Hydrogels can maintain the moist environment at the wound interface while absorbing excessive exudate, allow gaseous exchange, act as barrier to microorganisms, and do not adhere to the wound bed.
Generally, hydrogels are made of natural polymers such as collagen and chitosan and synthetic polymers (PVA, PEG, etc.) to achieve optimal mechanical properties.
New therapeutics in the treatment of chronic wounds
Within the last decade, significant improvements in the development of new therapies have been done, like integrating additives such as antimicrobial molecules, immunomodulatory cytokines, GF, microRNA (miRNA), or exosomes. 11 Advanced devices releasing antimicrobial agents, such as iodine or silver, are effective in reducing the bacterial load in the wound bed.
Some commercially available examples in Europe and United States are Actisorb™ Silver220 and Iodosorb®.
Antimicrobial peptides are able to control both inflammation and bacterial infection, acting as wound-healing peptides. These properties are highly desired in novel topical formulations for treatment of chronic wounds. 12
Regarding GFs, several studies have demonstrated that their use improves all aspects of tissue repair in animal models. 13 The success of topically administered GFs in chronic wounds is limited. Due to their short in vivo half-life, low absorption rate through the outermost skin later around the wound, as well as rapid elimination by exudation before reaching the wound bed, might limit the efficacy of GF topical application. Current strategies using GF may not provide the needed time for GFs in the wound area to interact with the target cells, due to their high degradation rate. 14
Conventional medications containing GFs need to be applied in high doses and/or be repeatedly administrated over a long period, leading to important side effects and increasing the cost of the therapy. GF delivery systems that improve their stability in the wound area and control their release provide more effective and secure treatment alternatives. Presently, PDGF, fibroblast growth factor (FGF), and epidermal growth factor (EGF) are widely studied for their application in GF-mediated wound repair. 15
Several approved products that include GFs are supplied as medications for external use in the form of solutions, gels, creams, and ointments. Clinical trials of topically administered GF have reported contradictory evidence for therapeutic outcomes. 16 There are some commercially available formulations containing GFs such as recombinant human platelet-derived growth factor (rhPDGF; Regranex® Gel), recombinant human basic fibroblast growth factor (bFGF; Fiblast® Spray), and recombinant human EGF (Heberprot-P®, Regen-D™ 150, and Easyef®). Regranex Gel is an aqueous-based sodium carboxymethylcellulose gel containing 0.01% becaplermin (rhPDGF) approved for topical use by the Food and Drug Administration (FDA). Fiblast Spray is a recombinant human bFGF product commercialized in Japan.
Another characteristic of biological dressings is their ability to interact with cells or matrix proteins in the wound bed to promote healing. The ECM is a combination of structural and functional proteins. These proteins are produced by skin cells and arranged into specific patterns, which are responsive for the physiologic and biomechanical requirements of skin. The three-dimensional (3D) ultrastructure of ECM also provides a scaffold that promotes cell organization, proliferation, and differentiation during the process of wound healing. Today, commercially available acellular ECM scaffolds include porcine-derived small intestinal submucosa (e.g., Oasis® wound matrix), porcine urinary bladder matrix (e.g., MatriStem UBMTM), bovine dermis (e.g., PriMatrix® and MatriDerm®), and equine pericardium (Matrix Patch™). Devitalized ECM scaffolds are also commercially available (EpiFix®).
These acellular biological products function as temporary substrates into which cells can migrate and proliferate in a well-organized and controlled manner. In this way, they promote granulation tissue formation and tissue regeneration.
Since the use of ECM-based scaffolds alone seems to be limited for chronic wound care due to an absence of interaction with cells and tissues, autologous cellular elements have been included in these scaffolds. 17
These living skin equivalents address the damaged ECM by adding a collagen matrix and also provide immune-privileged living cells that proliferate and actively synthesize GFs, cytokines, and ECM components, creating an optimal wound healing environment. 6
Some examples of skin equivalent substitutes commercially available are: Apligraf®, Dermagraft®, and Alloderm™. Apligraf is an FDA product containing an epidermal keratinocyte layer and a dermal layer of fibroblast-seeded collagen. Dermagraft, also FDA approved, is formed by a polymeric scaffold seeded with neonatal allogeneic fibroblasts. These cell-based biological dressings offer an enormous potential in the field of chronic wound management, acting in several ways to improve wound healing. 18
miRNAs are highly conserved endogenous small noncoding RNA molecules participating in various biological processes, including diabetic wound healing. miRNAs regulate post-transcriptional gene expression by binding to their target messenger RNAs (mRNAs), leading to mRNA degradation or translation suppression. 19 miRNAs are known to be altered in chronic wounds indicating that these molecules are also implicated in impaired angiogenesis. 20 In vivo studies using diabetic mice reported that miRNAs were differently expressed in skin cells and that their levels of expression changed during the wound healing process. 21
Other studies have demonstrated the in vivo upregulation of miR-129 and -335 enhanced wound closure through the inhibition of Sp1-mediated matrix metalloproteinase-9 (MMP-9) expression in a diabetic wound model. 22
RNA delivery techniques have improved in the last years, leading to the creation of functionalized wound dressings carrying stable miRNA or anti-miRNA molecules for skin wound healing applications. 23
This has led to an increase in available anti-miRNA-based strategies parallel to that of the functional miRNA transfection approach. For example, light-inducible synthetic antimiR-92a and Locked Nucleic Acid-antimiR-26a show progress made in this respect. 24
In another study, synthetic miRNA-92a inhibitor 25 reported increased angiogenesis and wound healing in different animal models such as diabetic mice and normal pig. 25
Although their effect in chronic wounds has not been reported yet, exosomal miRNAs obtained from umbilical cord mesenchymal stem cells (MSCs), human amniotic epithelial cells, and human umbilical cord blood plasma have demonstrated to be useful in wound healing. 26
DISCUSSION OF FINDINGS AND RELEVANT LITERATURE
Needs of new delivery systems in chronic wound: nanotechnology
Current therapies to treat chronic wounds are intended to cover the wound, protect against bacterial infection, remove dead tissue, provide moistening, and absorb excess of fluid. 27 Nanotechnology platforms, due to their characteristics, have demonstrated new promises and benefits in the field.
Recent progress in nanotechnology have opened new areas in the field of drug delivery applications allowing the delivery of biomolecules such as DNA/RNA or GFs that can be applied in chronic wound healing. Their small size and physicochemical properties allow the intracellular delivery of these biomolecules or drugs, protect these agents from degradation, and enhance the drug penetration into the wound. All together allow the topical administration and increase the half-life of these agents, lowering the number of applications and costs. In addition, the encapsulation of drugs and biomolecules inside nanocarriers enables different drug release profiles that can match the wound healing requirements. In the next sections, we will review the NPs, nanofibers, and self-assembled nanocarriers used for the treatment of chronic wounds (Fig. 1), specifically those that have proved positive results in wound healing in diabetic animal models.
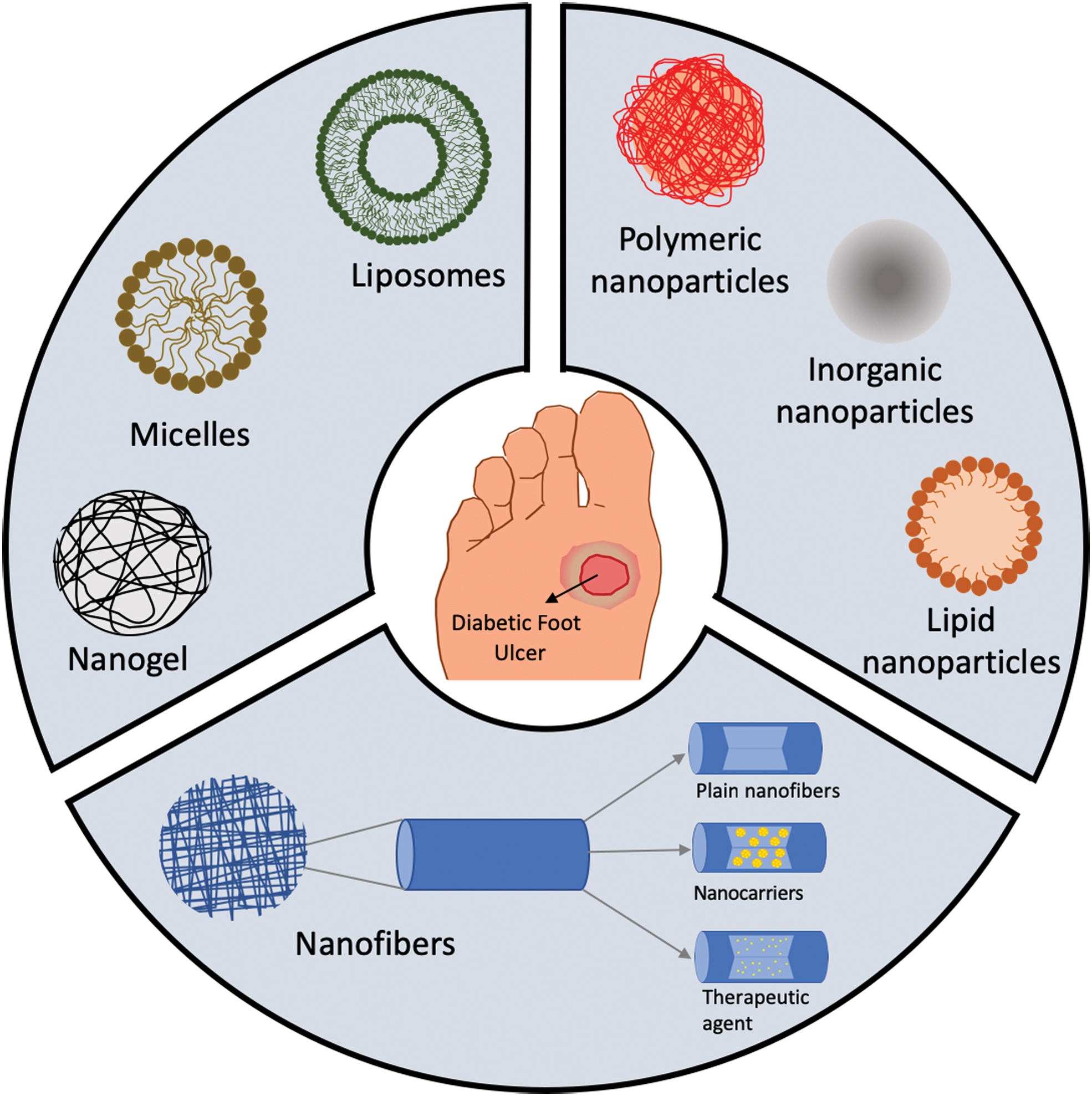
Schematic representation of nanocarriers used for chronic wound healing: self-assembled nanocarriers (liposomes, micelles, nanogels), NPs (polymeric, inorganic, lipid), and nanofibers (plain and encapsulating nanocarriers or therapeutic agents). NP, nanoparticle. Color images are available online.
Nanoparticles
NPs, with a diameter of 1–100 nm, are highly explored in the field of biomedicine and tissue engineering. In wound healing, they can be subdivided in two main categories: NPs with intrinsic properties positive for wound healing and NPs as drug delivery systems. Their main advantages are the controlled and sustained release, increase in drug half-life, and bioavailability.
NPs with intrinsic activity for wound healing
When developing strategies to address the healing of chronic wounds, technologies not using drugs or biologics are attractive to lower product fabrication costs and reduced time to market. Metallic NPs made of silver, copper oxide, gold, iron oxide, zinc oxide (ZnO), aluminum oxide, titanium dioxide, and gallium have proved their antibacterial properties. 28 –32 Its activity is caused by the production of ROS 33 and the interaction with RNA, DNA, and enzymes (inhibitory), which all together provoke bacterial death (Fig. 2). Other materials with intrinsic activity are cerium, bioactive glass (BG), and carbon-based and -bearing nitric oxide (NO) NPs.
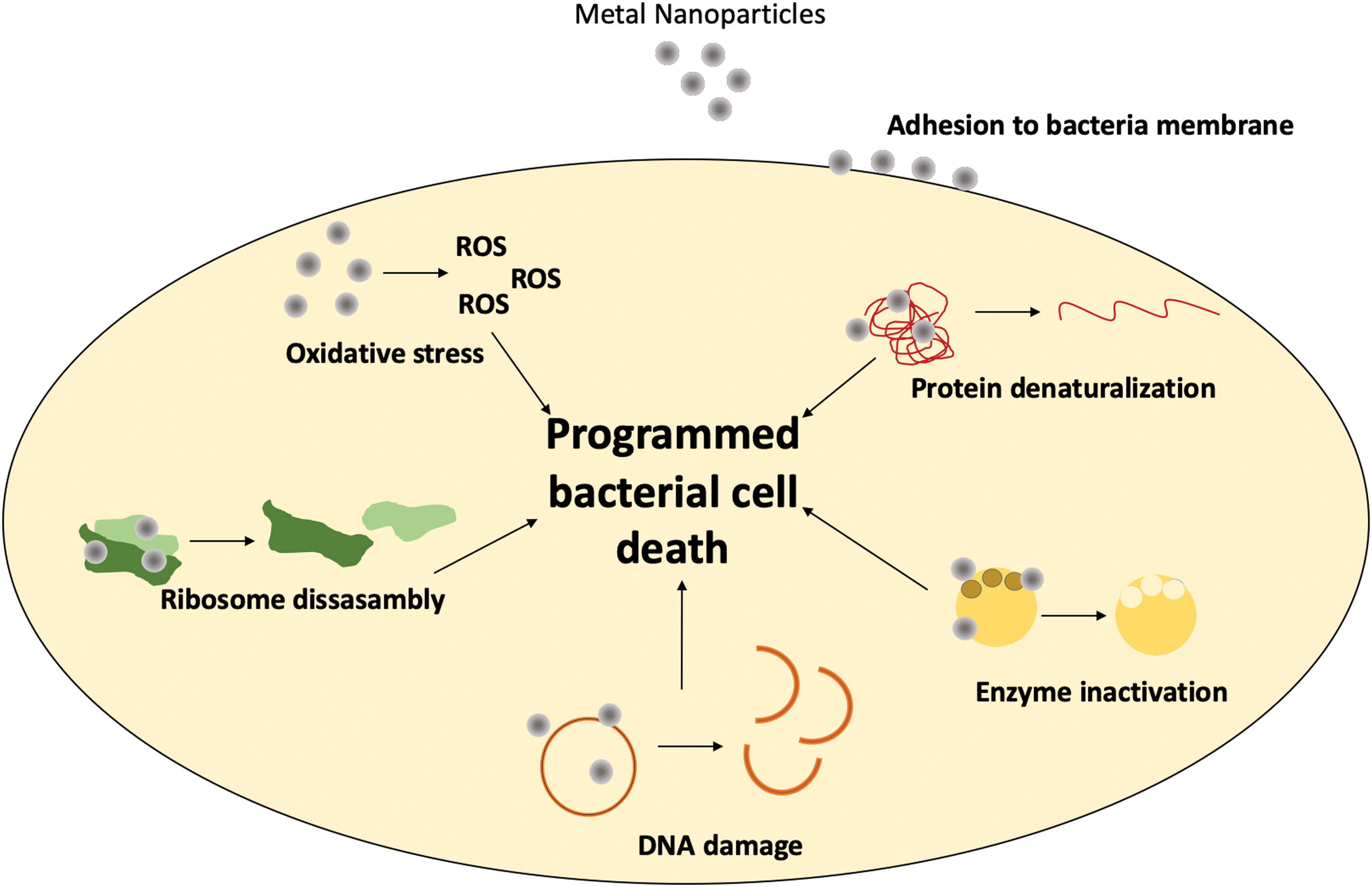
Antibacterial mechanism of action of metallic NPs. Metal NPs provoke protein denaturalization, enzyme inactivation, DNA damage, and the disassembly of ribosomes, as well as ROS generation. Altogether, promote the programmed bacterial cell death. ROS, reactive oxygen species. Color images are available online.
Although these NPs have useful properties, therapies that use metals are limited because excessive levels of metals, especially heavy metals, may damage human cells. Table 1 summarizes the NP formulations that have been tested in diabetic wound healing in animal models and have proved its activity in wound healing and as antibacterial agents. Among heavy metals, silver has been used as an antimicrobial agent due of its relatively low toxicity to human. 34 Recently, in response to issues concerning antibiotic resistance, topical application of medicals containing silver has become popular. 35
Nanoparticles with intrinsic activity for wound healing for the treatment of diabetic wounds in animal models
Diabetes type 1 was inducted with aloxan (rabbits) or streptozocin (mice and rats) (*times for complete wound closure or more than 90% of full thickness wounds).
AgNPs, silver nanoparticles; AuNPs, gold nanoparticles; BG, bioactive glass; EGF, epidermal growth factor; NP, nanoparticle; PCL, polycaprolactone; PDGF, platelet-derived growth factor; PEG, polyethylene glycol; PLGA, poly(lactide-co-glycolide); PU, polyurethane; PVA, poly(vinyl alcohol); VEGF, vascular endothelial growth factor.
Silver nanoparticles (AgNPs) are probably the most used NPs in wound healing due to its antimicrobial, anti-inflammatory, and wound healing properties (inducing myofibroblast differentiation from fibroblasts and stimulating keratinocyte proliferation/relocation).
36
Moreover, no bacterial resistance and toxicity were observed. Nevertheless, silver ions released from the NPs can lead to toxicity,
37
through oxidative stress by the generation of
Thus, its inclusion in other formulations to control ion release is needed to reduce its cytotoxicity. AgNPs have been incorporated in gels, such as hyaluronic, 39 PEG-chitosan, 40 polyacrylic acid, 41 and foams, 42 among others, that had proved their efficiency in diabetic wound healing and in the reduction in bacteria count. For example, Shi et al. prepared hydrogels made of maleic acid-grafted dextran and thiolated chitosan impregnated with AgNPs. 43 This hydrogel behaves as antifouling materials, improving the performance of AgNPs. They provided a slow Ag+ release that promoted the wound healing due to its antibacterial activity, inhibition of inflammation, and modulation of the immune response. Zhao et al., fabricated conductive hydrogels mimicking skin made of polydopamine decorated with AgNPs, polyaniline, and PVA with potential as epidermal sensors and wound healing agents. 44
The resulting hydrogels had adequate self-healing properties, repeatable adhesiveness, antibacterial activity and promoted angiogenesis and collagen deposition. The impregnation of cellulose nanocrystal matrix with AgNO3 NPs has also shown interesting results in diabetic wound healing. 45,46
A reduction in inflammation and an increase in collagen deposition, reepithelialization, and angiogenesis were observed, promoting wound healing. 46
In terms of clinical trials, however, there are not enough evidences to establish whether AgNP-containing dressings or topical agents promote wound healing or prevent wound infection. 47 –49
For DFUs, as well, no randomized trials or controlled clinical trials exist that analyze their clinical effectiveness, 50 although new devices are developed that suggest that more clinical trials are needed. Gold nanoparticles (AuNPs) have inherent antibacterial activity and promote the process of wound healing through hemostasis and inflammatory phases. 51
AuNPs have recently been used by various research groups for their wound-healing applications. AuNPs have been combined with biomolecules like antioxidants 52 to enhance the wound healing activity of the formulation. Martinez et al. fabricated a nanocomposite made of Au NPs functionalized with chitosan and calreticulin, 53 a calcium-binding protein of the endoplasmic reticulum that has shown wound healing activity. 54
When administered into diabetic mice wounds, improved healing was observed compared to untreated mice. Randeira et al. made AuNP conjugates with a spherical nucleic acid of ganglioside-monosialic acid 3 synthase (GM3S) dispersed in Aquaphor (Fig. 3). This enzyme is overexpressed in diabetic mice and impedes wound healing. Treated wounds in diabetic mice decreased the local enzyme expression and fully healed in 12 days, with an increase in granulation tissue formation and vascularity (Fig. 3). 55
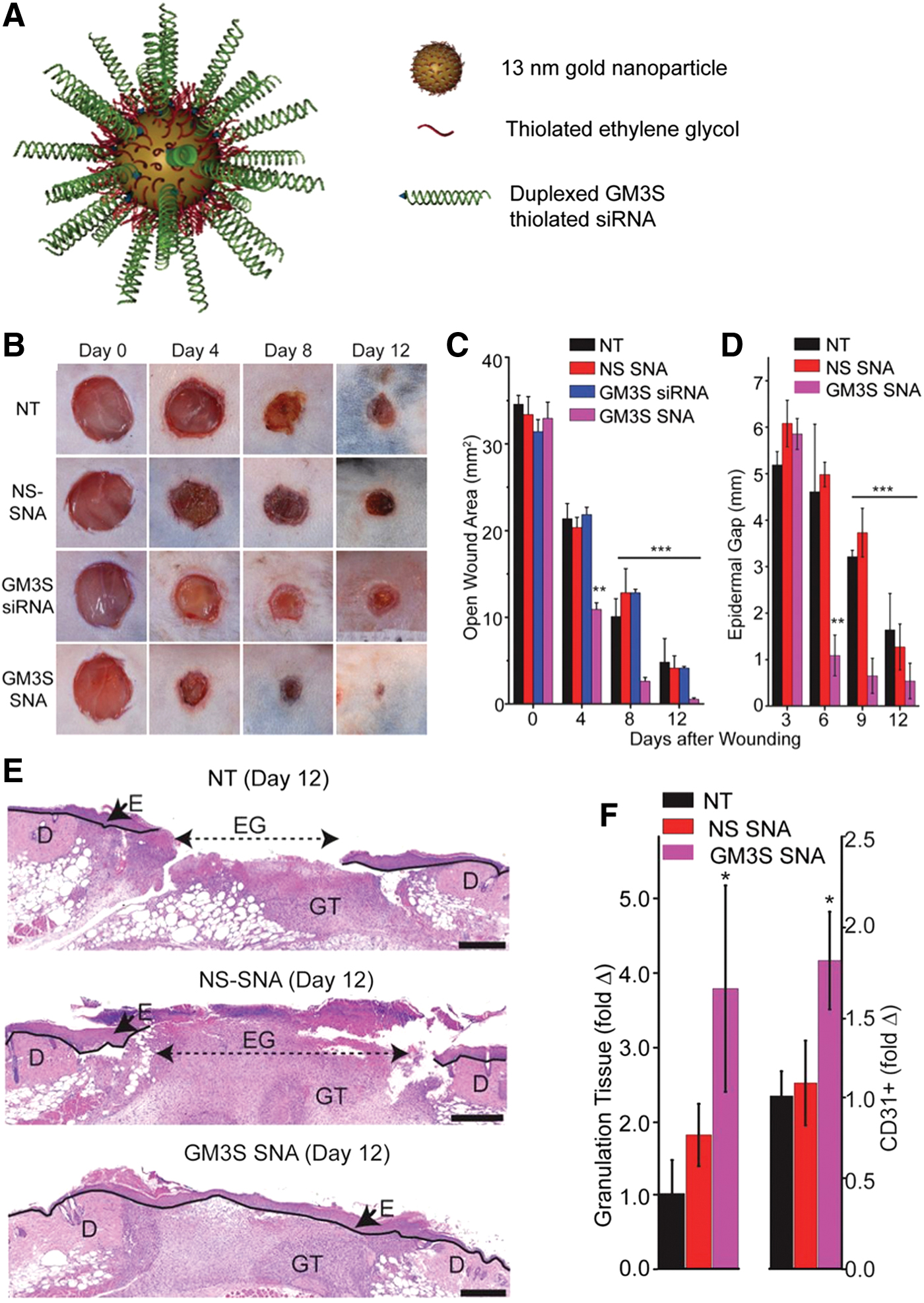
The topical administration of AuNPs conjugated to spherical nucleic acid for GM3S shows a reduction in local GM3S expression and heals the wound in 12 days in diabetic mice wounds. An increase in granulation tissue, new blood vessel formation, and IGF-1 and EGF receptor phosphorylation is observed.
Copper ions (Cu2+) also promote wound healing in diabetic mice 56 –58 due to its pro-angiogenic properties. 59 Cu2+ stabilize the expression of hypoxia-inducible factor and promote the secretion of VEGF, mimicking hypoxia, that plays a role in cell recruitment, cell differentiation, and blood vessel formation. 60
In addition, Cu2+ have antimicrobial activity. 28 However, multiple applications are necessary, 61 provoking copper toxicity. Slower ion release can reduce its toxicity. Metal−organic frameworks (MOFs) are a type of crystalline porous coordination polymers composed by inorganic metal ions and organic ligands that interact to form clusters with tunable release rates, being also efficient in diabetic wound healing. 62,63 Xiao et al. prepared MOFs modified with folic acid that released slowly Cu2+ and improved the wound closure by inducing angiogenesis, collagen synthesis, and reepithelialization. 62
Copper-based MOFs, however, might be unstable in physiological protein containing solutions, making difficult their direct use in wound healing. 62
ZnO NPs also exhibit activity in wound healing. 64 So far, zinc promotes reepithelialization, pro-angiogenesis, and it is anti-inflammatory. 65 Other metallic NPs such as graphene oxide, 66 iron oxides, or titanium have been also included in wound healing alternatives with positive results. 67 However, further studies need to be performed to ensure their efficacy in diabetic wound healing. Cerium oxide nanoparticles (CeONPs) have been proven to have antioxidant and pro-angiogenic activity, enhancing diabetic wound healing, 67,68 being even effective in the treatment of DFUs. 69 BGs have also been reported to be successful in wound healing applications due to their high biocompatibility and positive biological responses of their ionic products. 70
Several reports indicate that BG NPs can efficiently enhance diabetic wound healing. Lin and coworkers reported an accelerated wound healing in diabetic rats probably due to an increase in angiogenesis related factors such as VEGF and FGF-2. 71
Silicon (Si) ions have also been used for the treatment of diabetic wounds. Jiang et al. prepared a spaced-oriented scaffold for Si ion release. The scaffolds were coated with silicon-doped amorphous calcium phosphate NPs coating its surface to promote angiogenesis. 72 The Si ions released promoted wound healing by enhancing angiogenesis, collagen deposition, and reepithelialization of the diabetic wound. Porous Si NPs loaded with Flightless I neutralizing antibodies showed a significant improvement in healing compared to controls and the antibody alone in diabetic wounds. 73
NO is a potent anti-biofilm in wound healing and it has been proved that diabetic wounds have a low NO level in the wound bed. 74
NO has been formulated in NPs to improve wound healing in diabetic animal models. 75 NO-releasing NPs prepared by doping PLGA NPs with polyethylenimine/diazeniumdiolate have been reported to accelerate healing of methicillin-resistant Staphylococcus aureus biofilm-infected wounds in diabetic mice together with biofilm clearance and reduced bacterial count. 76
Overall, we must highlight that mostly bioactivity and mechanism proposed in the literature are related to the ion species rather the metal or oxide. That means that features that affect degradability and dissolution such as particle size, crystallinity, and solubility should be strongly controlled.
NPs as drug delivery systems
NPs can also be used in wound healing as encapsulation platforms (Table 2). Polymers such as polyesthers, polysaccharides, peptides, and lipids can be used for their preparation. PLGA can release lactate into the wound bed to promote neovascularization and wound healing. 77 PLGA has been used to encapsulate a variety of molecules, such as insulin, 78 ferulic acid, 79 and GFs, 77,80,81 showing accelerated wound healing in diabetic rodent models. For example, wounds treated with NPs encapsulating VEGF have an increase in collagen deposition, reepithelialization, and angiogenesis in diabetic wounds. 77 Compared with free VEGF, wounds required only 19 days to be completely closed in the case of VEGF encapsulated in the PLGA NPs compared with the 28 days for free GF. 77
Nanoparticles for drug delivery of wound healing drugs or biomolecules for the treatment of diabetic wounds in animal models
Diabetes type 1 was inducted with aloxan (rabbits) or streptozocin (mice and rats) (*times for complete wound closure or more than 90% of full thickness wounds).
bFGF, basic fibroblast growth factor; ELP, elastin-like protein; KGF, keratinocyte growth factor; STF-1, stromal cell-derived factor-1; TNFα, tumor necrosis factor alpha.
Lipid nanoparticles (LNPs) are generally prepared with physiological lipids or lipid molecules in processes that do not require any potentially toxic organic solvents. Generally, for wound healing applications, LNPs are loaded with specific siRNAs. Topical application of LNPs formulated with an ionizable and degradable lipid and a siRNA specific for tumor necrosis factor alpha (TNFα) have shown a decreased TNFα mRNA expression in the wound bed by 40–55% in diabetic mice compared to untreated wounds. 82 Another example of LNP application in chronic wounds is lecithin-based NPs. Topical application of these NPs complexed with deferoxamine in a model of wound healing in diabetic rats showed an increased wound closure along with an improved collagen deposition and neovascularization compared with free deferoxamine. This suggests that the NPs encapsulating the therapeutic have a better healing outcome than the free therapeutic. 83
NPs made of peptides have also shown their utility in the field of wound healing. Elastin-like protein (ELP)-based fusion proteins, by forming NPs, have been shown to protect biomolecules from proteolysis and can act as “drug depots” that supply the biomolecules over an extended period. Recently, self-assembling elastin-like peptide GF chimeric NPs have been used to treat chronic wounds. These NPs of ELP and KGF 84 or ELP and stromal cell-derived factor-1 (SDF-1) 85,86 were applied to excisional wounds on the back of diabetic mice. These treatments showed accelerated wound closure and increased vascularization compared to free GF, ELP alone, or vehicle (Fig. 4). Other peptide, such as the cationic antimicrobial peptide protamine, has been reported to be suitable for the development of treatments for chronic wounds. Wang et al. developed protamine NPs and hyaluronan oligosaccharide loaded in alginate hydrogels. Using a diabetic mouse-skin defect model, these authors demonstrated that this composite reduced bacterial-induced chronic inflammation at the wound site and accelerated the wound-healing process by promoting angiogenesis. 87
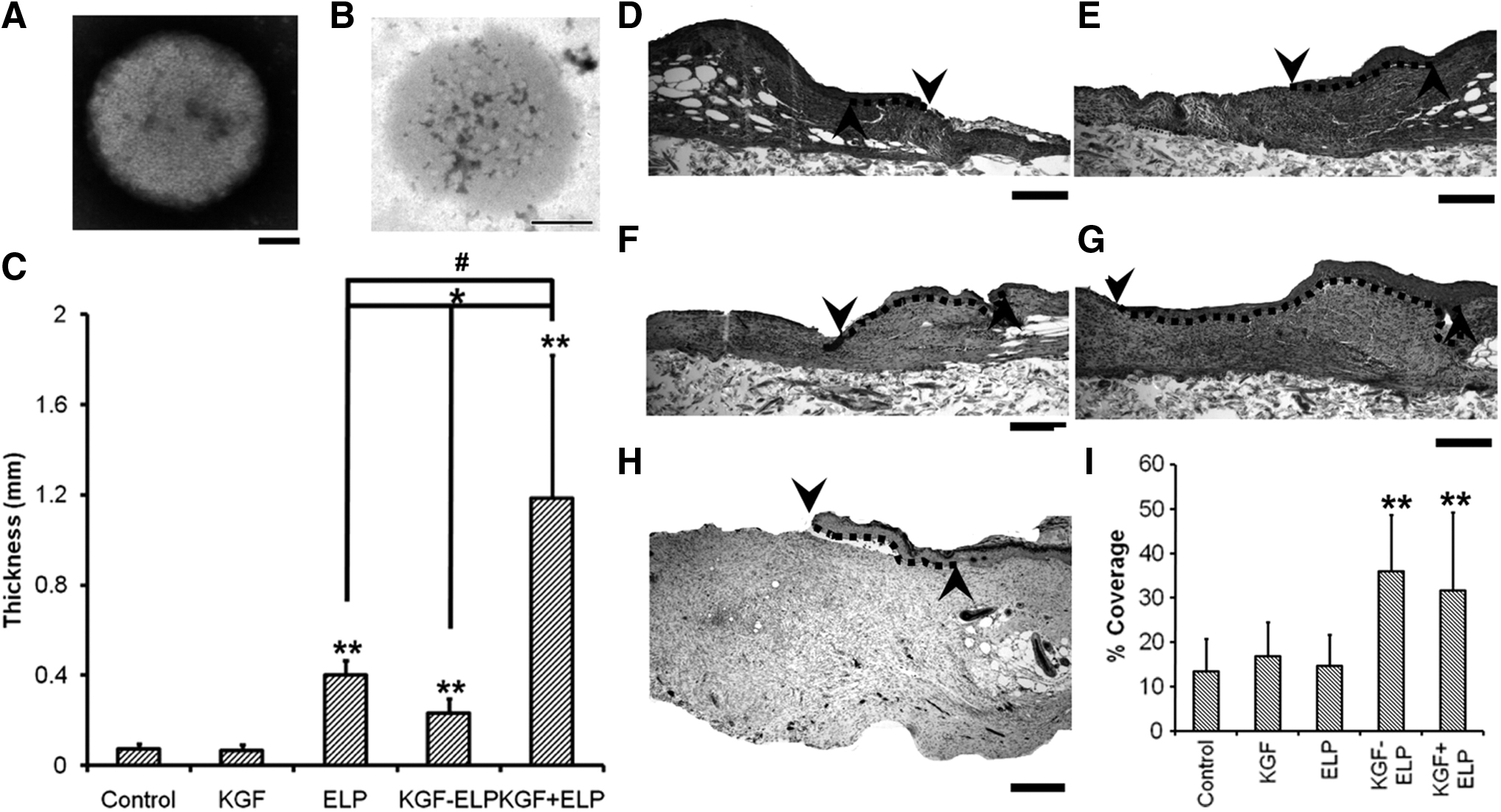
NPs of fusion protein of ELP and KGF enhance wound healing in diabetic mice by promoting reepithelialization and granulation tissue formation.
Nanofibers
Nanofibers are filaments with diameters within the nanoscale. They are usually produced by the electrospinning technique due to its low cost and simplicity. This technique uses a high electric force between a needle point capillary tip and a collector to spin the polymeric solutions and obtain fiber meshes. Nanofiber meshes are a promising tool in the field of chronic wounds as they can partially reproduce the ECM due to its organization and random alignment. Indeed, its high surface area-to-volume ratio and tunable porous morphology can promote the wound homeostasis, as well as allow the gas/nutrient interchange. 88
Moreover, nanofiber meshes should also provide moisture to avoid the wound dehydration and bacteria contamination. They can also encapsulate biological molecules, drugs, or nanocarriers encapsulating those, which consequently allow their topical administration with the subsequent advantages (lower dose and less side effects). In contrast, nanofiber meshes have also been tested as artificial skin. When MSCs are used they can differentiate into endothelial cells or release GFs to trigger the wound healing process. 89
Nanofibers can be categorized depending on their composition (natural polymers, artificial polymers, polymer blends). Table 3 describes the strategies followed for diabetic wound healing.
Nanofiber formulations used for the treatment of diabetic wounds in animal models
Diabetes type 1 was inducted with aloxan (rabbits) or streptozocin (mice and rats) (*times for complete wound closure or more than 90% of full thickness wounds).
HPMC, hydroxypropyl methylcellulose; MP, microparticles; MSC, mesenchymal stem cell; MSNP, mesoporous silica nanoparticles; PEO, polyethylene oxide; PLA, poly(lactide); rhPDGF, recombinant human platelet-derived growth factor; SF, silk fibroin; ZnO, zinc oxide.
Natural polymers
Natural polymers offer an excellent biocompatibility and biodegradability, low antigenicity, and even, some of them have innate properties for wound healing (antibacterial and hemostatic activity).
Among them, polysaccharides and proteins are often used for nanofiber preparation. The main limitation for its use is its innate variability and the poor mechanical properties, normally requiring their combination with synthetic polymers.
Polysaccharides
Polysaccharides such as chitosan, alginate, and hyaluronic acid have emerged as good candidates in wound dressings due to their innate properties, similarities with the skin ECM, and abundance. However, its use in chronic wounds is still limited. The fabrication of polysaccharide nanofibers through electrospinning is challenging, due to the critical chain entanglement concentration (CEC), 90 that it might be too high (hyaluronic) provoking high or insufficient viscosity (alginate).
Alginate is one of the most used biomaterials for the developing of wound dressings, 91 being even some commercially available options (Tegagen™). It is generally combined with synthetic polymers like polyethylene oxide (PEO) to be electrospun. 92 Its use in chronic wounds has not been tested yet.
Chitosan has innate antibacterial and hemostatic activity. 93 However, its chemical characteristics (hydrogen bonds, amino groups) reduce its chain flexibility, limiting the fabrication of nanofibers. 93 Chitosan has been electrospun using strong acids to break chemical interactions or combining it with other polymers, such as PEO, PVA, or PCL. 94 Xie et al. created a scaffold made of chitosan and PEO, loaded with VEGF and NPs encapsulating platelet derived growth factor-BB (PDGF-BB). The scaffold had antibacterial activity due to chitosan and released VEGF in the early stage to promote blood vessel formation. 94
In addition, NPs were able to slow the release of PDGF-BB over time promoting the formation of new blood vessels and cell proliferation during the wound healing process.
Chitosan/PVA nanofibers have a good wound healing profile by itself, 95 and they were also combined with other therapeutics like desferrioxamine. 96 These nanofibers sustained desferrioxamine release for 3 days and were able to recruit cells to promote angiogenesis in chronic wounds through the hypoxia-inducible factor 1-alpha (HIF-1a) expression and other pro-angiogenic GFs.
ZnO was also encapsulated into chitosan/PVA fibers to implement its antimicrobial and antioxidant activities. 91 Chitosan/gelatin nanofibers containing BG were also tested in chronic wound treatment, proving their antibacterial activity and healing properties. 92
Hyaluronic acid is a natural constituent of the ECM, having a relevant physiological role in inflammation and wound healing. 93 Its molecular weight (MW) determines its activity; MWs greater than 15 kDa render polymers recognized by the CD44 receptor, which induces fibroblast migration and proliferation and cell growth, 93 and are beneficial for wound healing. 93 Hyaluronic electrospinning is challenging due to its high viscosity at the CEC, forcing the combination with other materials. 93 Nevertheless, some authors have reported the fabrication of nanofibers when it is dissolved in strong acids or bases and dimethylformamide. 93 Collagen/hyaluronic nanofibers encapsulating angiogenic GFs (VEGF, PDGF) and GF-loaded gelatin NPs (EGF and bFGF) were assayed as skin substitutes. The nanofibrous membrane possessed similar mechanical properties to human skin and allowed a faster wound regeneration than the control. The formulation was able to release EGF and bFGF in the early stage of the wound (to promote epithelialization and angiogenesis), and PDGF and VEGF in the late stage (to aid vasculature maturation), promoting enhanced wound healing. 15
Abdel-Mohsen et al. prepared hyaluronan nanofibers containing AgNPs. The nanofibers had antibacterial activity against gram negative bacteria and higher wound repair efficacy compared to controls, proving its efficacy in wound and chronic ulcers. 99
Cellulose derivatives are also used for the preparation of nanofibers through electrospinning. Grip et al. used hydroxypropyl methylcellulose combined with PEO to form nanofibers encapsulating beta-glucan. Nanofibers were prepared by the Nanospider™ technology. When used in vivo in diabetic mice, they showed an improved wound healing capacity. 100
Proteins
The most used proteins for the fabrication of nanofibers for wound healing are silk fibroin (SF), gelatin, and collagen. Insects and arachnids naturally produce SF, which is a very common protein applied in the electrospinning process to produce strong fibers due to its mechanical properties. These nanofibers have demonstrated to accelerate wound dressing progress. 102 Chouhan et al. showed that SF nanofibers loaded with antibiotic and EGF had a faster wound healing in diabetic rabbits than other commercially available bandages. 103
These authors also fabricated fibers combining SF with PVA and encapsulating EGF together with an antimicrobial peptide. They observed a remarkably faster healing, progress of the granulation tissue formation, angiogenesis, and reepithelialization of the wounds in diabetic rabbits. 104
Li et al. prepared nanofiber dressing of SF encapsulating microparticles loaded with insulin. 105 Insulin stimulates keratinocyte and endothelial cell proliferation and migration, promoting wound reepithelialization and vascularization. These authors observed that the dressing improved the wound healing in diabetic rats due to a sustained release of the insulin during the wound healing progress.
Chouhan and coworkers developed nanofibrous meshes of SF coated with two classes of recombinant silk fusion proteins from arachnids: FN-4RepCT (contains fibronectin-derived binding motifs) and Lac-4RepCT (includes a cationic antibacterial peptide) (Fig. 5). When mats were coated with both spider silk proteins, they had a faster wound healing, improved granulation, angiogenesis, collagen deposition, and reepithelialization than the uncoated or one single coat in diabetic wounds. 105 SF scaffolds were also used as skin substitutes, by seeding human adipose-MSCs on them. 106 Interestingly, when the scaffolds were decellularized they were almost as effective as the seeded scaffolds in the treatment of diabetic wounds.
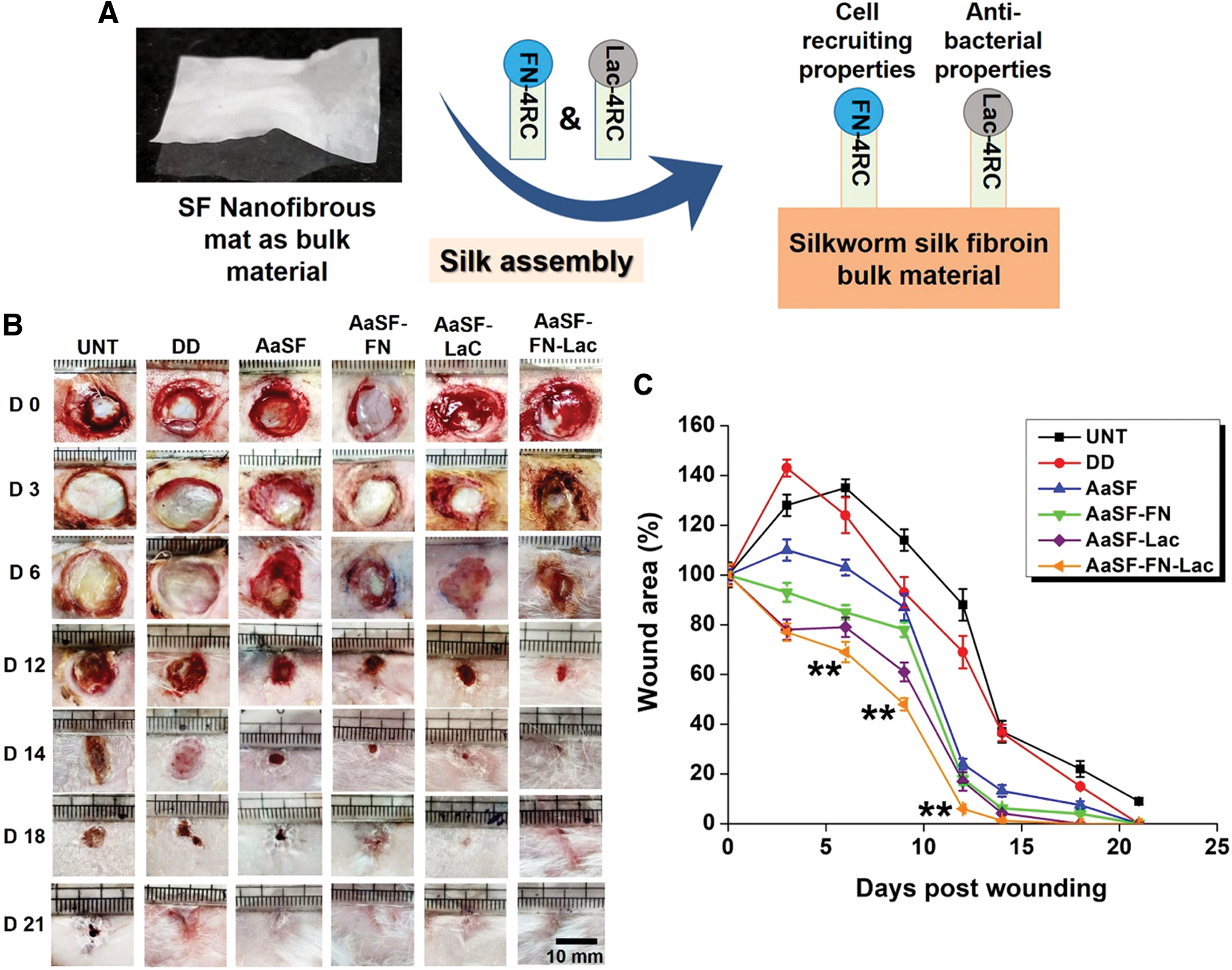
SF nanofiber meshes coated with spider silk fusion proteins FN-4RC (contains motifs of fibronectin for cell adhesion) and/or Lac-4RC (contains lactoferrin, an antimicrobial peptide). When both fusion proteins are used, a faster wound healing in a diabetic model is observed, provoked by a better granulation tissue formation and reepithelialization compared to a positive control.
Gelatin is a polyaminoacid obtained by the partial acid or alkaline hydrolysis of natural collagen.
It has been widely applied in the area of biomaterials for tissue engineering because of its hemostatic activity, high number of Arg-Gly-Asp (RGD) sequences to promote cell adhesion, low antigenicity, and easy chemical modification.
Dongargaonkar et al. were able to produce gelatin nanofibers using water solvents by then increasing its water stability crosslinking them with oxidized sucrose, reducing the toxicity associated to other cross-linkers like glutaraldehyde. 107 Aduba et al. electrospun gelatin and arabinoxylan encapsulating silver sulfadiazine, obtaining trifunctional fibers due to its antioxidant and antimicrobial activities and similarities with the ECM. However, its instability in water forced to cross-link the fibers, reducing its mechanical properties. 108
Gelatin nanofibers encapsulating AgNPs and PDGF-BB showed a better antibacterial activity, promotion of angiogenesis, reepithelialization, collagen deposition, and granulation tissue formation in diabetic wounds than the gelatin scaffold (Fig. 6). 109 PCL was also used for electrospinning gelatin. Lv et al. prepared gelatin/PCL nanofibers encapsulating silicate-based bioceramic particles with a sustained release of Si ions. In vivo, an enhanced angiogenesis, collagen deposition, reepithelialization, and reduction of inflammation were observed. 110
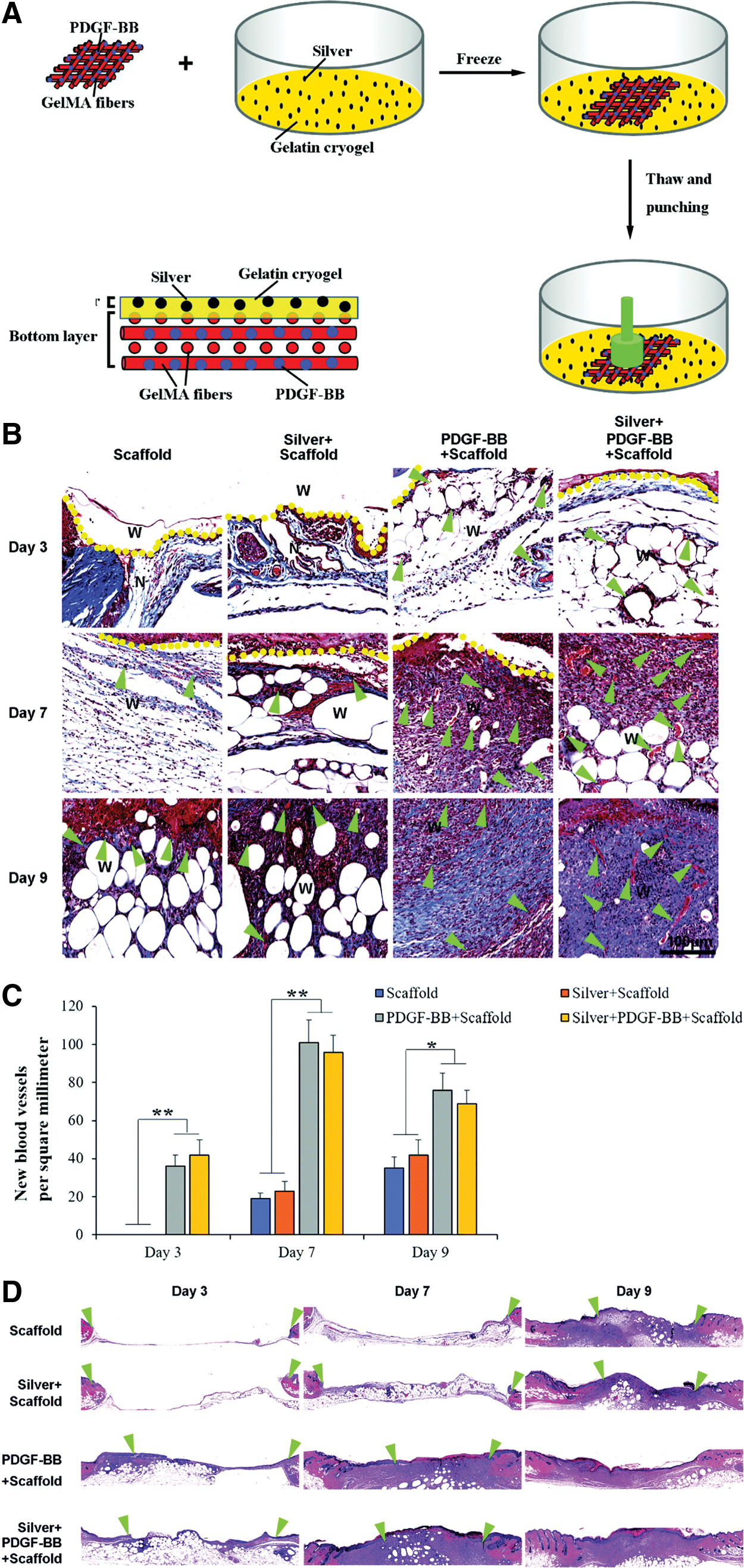
A skin-inspired 3D bilayer scaffold made of gelatin, AgNPs, and PDGF-BB had a faster wound healing, more collagen deposition, blood vessel formation, and reepithelialization in diabetic wounds.
Collagen is the main constituent in the ECM, skin, and connective tissues, and its role in ECM regeneration has been demonstrated. Collagen has been combined with other materials for fabricating dressings by electrospinning. Sun et al. prepared nanofibers of collagen I and PCL with different patterns: mimicking the collagen fibril pattern in vivo (crossed), random, and aligned (Fig. 7). In vitro, fibroblasts responded differently in each nanofiber configuration, having differences in the wound healing related gene expression. Moreover, diabetic rats treated with crossed nanofibers had a faster healing, increased angiogenesis, and lower inflammation compared to the other nanofiber architectures. 111
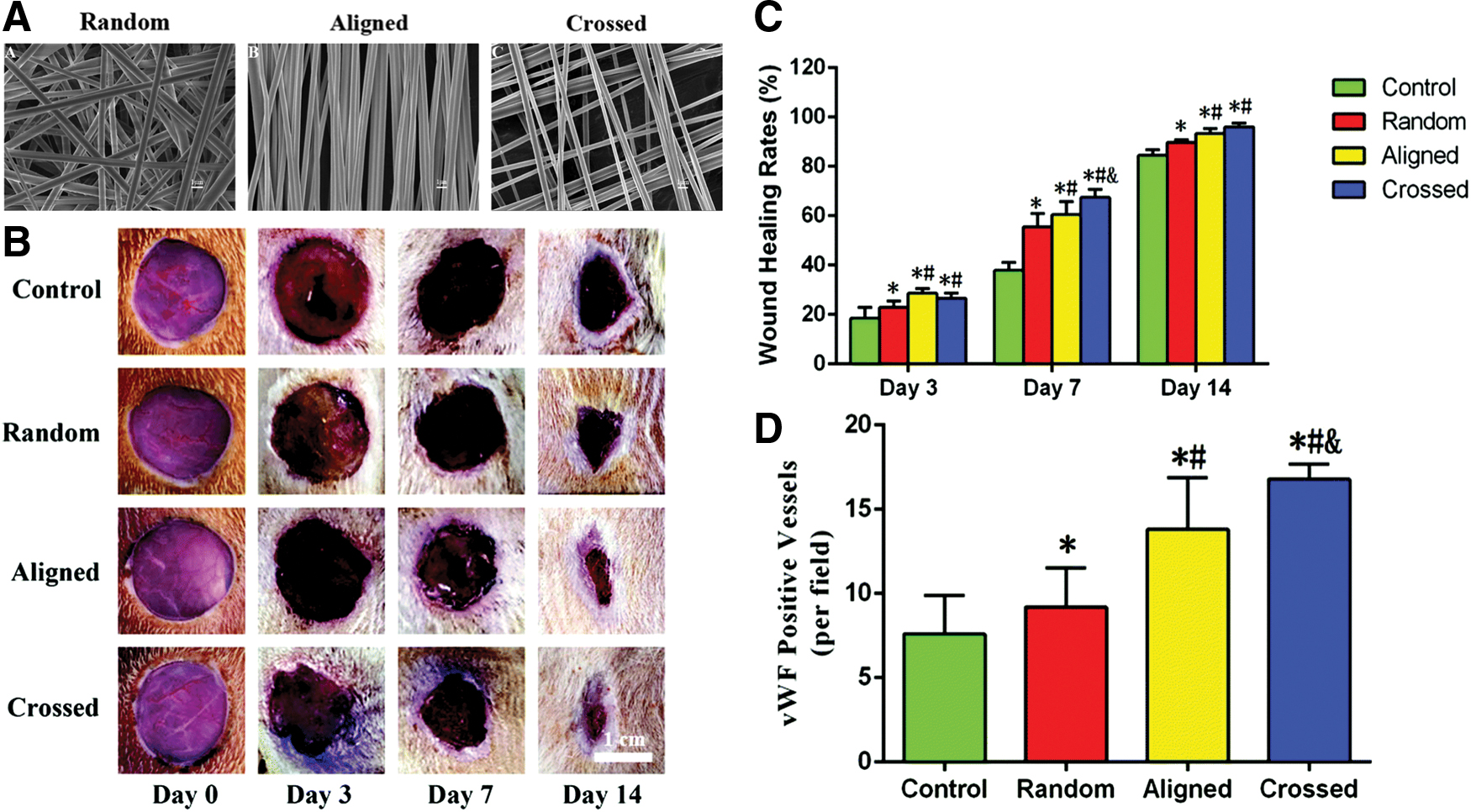
Nanofiber meshes made of Collagen I and PCL with different fiber organizations have different outputs in wound healing. Crossed nanofibers, which mimic the collagen pattern in skin, have a better wound healing rate and promote angiogenesis in diabetic rats.
Gao et al. also fabricated Collagen 1/PCL nanofibers encapsulating an inhibitor of the prolyl hydroxylases: dimethyloxalylglycine, which is able to avoid HIF-1-alpha degradation.
These fibers were produced by co-axial electrospinning, having a drug/polymer core and a polymer shell, showing sustained biomolecule release for 2 weeks and a stabilization of HIF-1a in vivo.
The nanofibers improved wound healing in diabetic rats. 112 They also prepared similar nanofibers encapsulating BG NPs instead. These new nanofibers mimicking the bone ECM improved angiogenesis, granulation tissue formation, ECM remodeling, and epidermis differentiation. 113
Lee et al. encapsulated recombinant human PDGF in collagen/PLGA nanofibers to test its suitability in chronic wound healing, and they also observed a faster closure rate of the wounds, combined with a higher reepithelialization and collagen I deposition. 114 When Glucophage is loaded in collagen/PLGA nanofibers, a downregulation of MMP-9 is observed in murine diabetic models, promoting faster healing. 115
Synthetic polymers have a more defined molecular structure and a better solubility in organic solvents than natural materials, easing its formulation in nanofibers. In addition, most of them have better mechanical properties than natural polymers.
Polyesters
Polyesters are the most used materials for nanofiber formation, owing to their tunable biodegradability, their innate biocompatibility, and their approval by the FDA. For example, poly(lactide) (PLA) fibers embedding mesoporous silica NPs loaded with a pro-angiogenic drug (dimethyloxalylglycine) enhanced new blood vessel formation reepithelialization and collagen deposition, as well as a decrease in inflammation in a diabetic wound model. 116
Curcumin-encapsulated PCL nanofibers had also proved its benefits as antioxidants and anti-inflammation in wound healing in diabetic mice. 117 When combining PCL with the curcumin and gum tragacanth, the nanofibers were active against bacteria. MSC seeded scaffolds improved the wound closure rates and it enhanced granulation tissue formation, reepithelialization and collagenous synthesis, and even sweat gland and hair follicle formation. 118 Bixin encapsulated in PCL nanofibers also proved its efficacy in reducing scar formation and accelerating the wound healing process in diabetic models. 119 PCL nanofibers encapsulating GFs have been also synthetized and tested in chronic wound healing. Choi et al. prepared PCL/PCL-PEG copolymer blends for electrospinning, making nanofibers with a core of bFGF, that afterward were chemically modified in their surface with EGF. Animal studies showed that the double encapsulation with biphasic release profiles rendered a higher collagen accumulation and keratin cement formation, which implemented the wound closure and reduced the scar formation. 120
PLGA nanofibers have also a great potential in the development of new wound dressings for chronic wound healing. Molecules such as metformin or recombinant human PDGF 121 have been encapsulated in the fiber meshes, showing remarkable wound healing. PLGA has also been combined with cellulose nanocrystals or aloe vera to form nanofibers. 122,123 Neurotensin encapsulated PLGA/cellulose nanocrystals induced a faster healing than controls, with a decrease in inflammatory cytokines and a higher epidermal/dermal regeneration. 122 PLGA/aloe vera nanofibers encapsulating rhEGF had antimicrobial activity and a faster wound closure and reepithelialization. 123
Hydrophilic polymers
Hydrophilic polymers like PEG or PVA have also been studied in wound healing due to their hydrophilicity that allows moisture of the wounds and their similarities with the ECM. PVA has been combined with curdlan and silver nitrate to fabricate nanofiber meshes effective against gram positive and gram negative bacteria. The in vivo results showed an anti-inflammatory activity and a faster wound healing. 124 Yang et al. tested whether the incorporation of a GF 125 into PLGA-PEG copolymer fibers with a core-shell structure could be beneficial in chronic healing. They found out that the scaffolds had a higher neovascularization, faster wound closure, better reepithelialization, and regeneration of skin appendages. 126
Self-assembled peptides
Milder fabrication methods for the encapsulation of biomolecules have also been tested to avoid degradation problems of the encapsulated molecules. Self-assembled peptides like the Ac-RADARADARADARADA-CONH2 (RADA16) form 3D nanofibers when deposited into wounds and can be used as skin bioequivalents. Schneider et al. prepared RAD16 nanofiber encapsulating EGF that increased wound closure rate by fivefold compared to controls in an in vitro human skin equivalent wound healing model. 127 Balaji et al. proved that the use of angiogenic injectable peptide nanofibers (ACN–RARADADARARADADA–CNH2) in diabetic wounds promoted the angiogenesis and wound closure and reduced the inflammation. 128 Multidomain peptide nanofibers were also checked in chronic wounds, and they showed an accelerated wound healing rate, high vascularization, granulation, and hair follicle regeneration 129
Nanofibers made of heparin-mimic amphiphilic peptides also accelerated wound healing in vivo in diabetic-induced and diabetic mice. 130 Treated diabetic mice showed an accelerated wound closure, better reepithelialization, induction of angiogenesis, and high levels of VEGF during time. TNF-α was elevated only at early stages proving a transition from inflammation to proliferative phases. 130 Pro-inflammatory cytokines were elevated only at early stages proving a transition from inflammation to proliferative phases. 130
Liposomes and other self-assembled structures
Liposomes are promising topical drug delivery systems, because they allow the reduction of the drug dosage and it increases the transdermal absorption compared with traditional emulsions and ointments. Liposomes are sphere-shaped vesicles having one or more lipid bilayers. Liposomes can be classified according to their size (from nm to mm), number of bilayers, or the method of fabrication. They are generally prepared from phospholipids and cholesterol.
They can encapsulate hydrophilic (in the internal aqueous compartments) and hydrophobic (in the bilayer) molecules in their structure, making them very suitable for drug delivery 131 to have a slower and constant release of the drug. Liposomal formulations used in the treatment of diabetic rodent wounds are shown in Table 4.
Liposomal formulations used for the treatment of diabetic wounds in animal models
Diabetes type 1 was inducted with aloxan (rabbits) or streptozocin (mice and rats) (*times for complete wound closure or more than 90% of full thickness wounds).
ATP, adenosine triphosphate; DOTAP, 1,2-dioleoyl-3-trimethylammonium-propane; IGF-1, insulin-like growth factor-1; RGDK, Arg-Gly-Asp-Lys.
Cationic liposomes can work as gene delivery systems by forming complexes with the negatively charged nucleic acids. They are made of 1,2-dioleoyl-3-trimethylammonium-propane (DOTAP). The encapsulation of genes protects them from degradation, increasing the circulation half-life. Moreover, the overall positive charge of the liposome enhances its endocytosis due to interactions with the cell membrane. They can be administered topically or by intradermic/subcutaneous injections. Rabbani et al. prepared cationic liposomes and peptide-based ternary complexes to increase the transfection of Keap1 siRNA. This molecule can activate antioxidant mechanisms, proving tissue regeneration. They observed that wounds regenerate faster in murine diabetic model. 132
Li et al. encapsulated miR-132-loaded liposomes in pluronic F127 gels and applied them to diabetic mice on human ex vivo skin wounds. The gels were administered intradermal in the edges of the diabetic wounds, resulting in an accelerated wound healing closure, which repressed the inflammation and increased proliferation of keratinocytes.
Moreover, in human ex vivo skin wounds, a faster reepithelialization of the wounds was observed. 23 They can also encapsulate genes encoding GFs. Bhattacharyya et al. encapsulated the gene encoding for PDGF into liposomes, and with only one subcutaneous administration, wounds were healed with higher degree of epithelialization, keratinization, collagen deposition, and blood vessel formation compared to controls (Fig. 8). 133
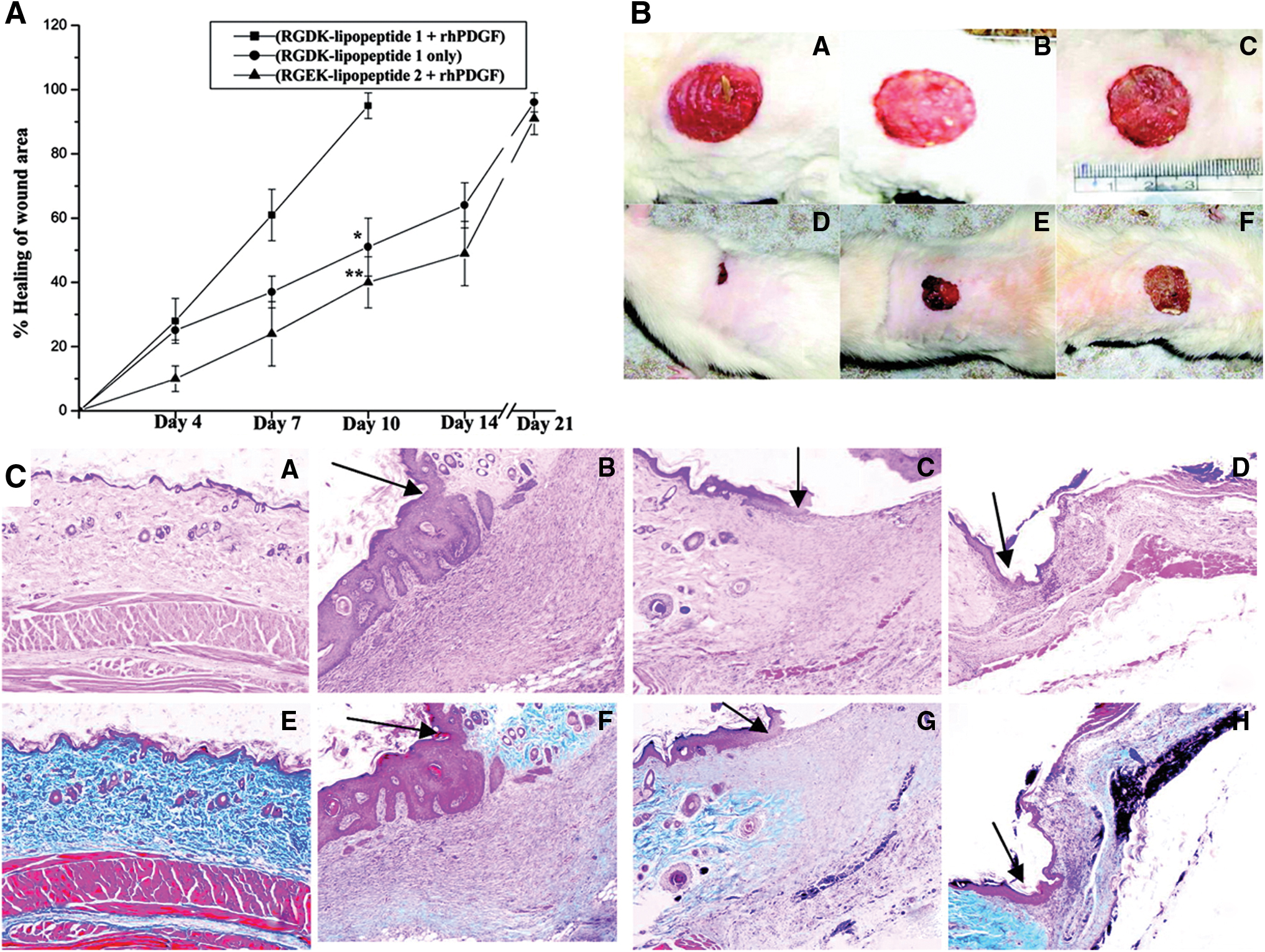
Cationic liposomes made of an electrostatic complex between the plasmid of human recombinant PDGF-B, integrin receptor selective RGDK-lipopeptide, and cholesterol are able to improve wound healing in diabetic rats. The administration of RGDK-lipopeptide 1:rhPDGF-B on wound of diabetic animals shows a faster wound healing rate, reepithelialization and fibrocollagen, and keratin and vessel formation.
Chronic wounds are more likely to develop wound infections, especially with multidrug resistance microorganisms. Thus, new approaches like the phage therapy are appearing. Chhibber et al. encapsulated bacteriophages into cationic liposomes to resolve S. aureus-infected diabetic mice wounds. 134 Liposome-treated mice evidenced an accelerated wound closure and healing than the free phages, proving that the reduction of clearance can increase the activity of the phages.
Insulin-loaded liposomes included into a chitosan hydrogel demonstrated its efficacy in chronic wounds in patients, reducing the erythema and the time of wound duration. 135 Wang et al. tried the liposomes using a model of diabetic rabbit with ischemic tissue. They topically administered adenosine triphosphate liposomes in the wounds and observed a faster wound closure than the control. 136
The encapsulation of GF into liposomes increases its stability and prolongs its release as it protects against degradation in the wound site. 137 Choi et al. prepared cationic liposome encapsulating EGF, insulin-like growth factor-1, and PDGF-A. All the GFs were combined with a low-MW protamine, complexed with hyaluronic acid, and then encapsulated in cationic liposomes made of hydrogenated phosphatidylcholine, cholesterol, and DOTAP. Liposomes were able to increase the wound healing ratio and showed reepithelialization and dermal tissue remodeling in diabetic mice ulcers because of the combination of GFs and hyaluronic acid and a sustained release of them. 138 SDF-1, known to enhance angiogenesis in ischemic tissues, was encapsulated into liposomes and then included in decellularized dermis scaffolds. 139 A higher cell proliferation in the dermis was observed, which resulted in faster wound closure and increased granulation.
Another approach followed for the increase of the activity of GFs was developed by Das et al. 140 They studied the delivery of syndecan-4 (a proteoglycan that works as coreceptor of many GFs) into liposomes in combination with PDGF-BB, all embedded in an alginate dressing. They observed an increase in wound closure rate, angiogenesis, and a reduced inflammation.
Micelles are self-assembled structures made of polymers or surfactants that have a hydrophobic and hydrophilic part. They have sizes on the range of 10–100 nm and can encapsulate hydrophobic molecules in its core. Nevertheless, micelles were also poorly explored in wound healing field. Only few authors have reported the use of PLA-PEG, 141 PEG-PCL-PEG, 142 or pluronic micelles 143 for encapsulation of drugs like curcumin. Nanogels 144 and nanoemulsions 145 have also been poorly explored in the field of wound healing.
Future Directions
The appearance of new biomolecules active in wound healing, such as GFs or nucleic acids, shows the necessity of designing new formulations to protect them from degradation and to deliver them at specific rates. The emergence of nanotechnology, especially the fabrication and characterization of nanoparticulate systems, has increased the number of available interventions for healing of chronic wounds.
The new chronic wound nanotherapeutics are multifunctional platforms that promote wound healing with minimal scar formation, avoid/treat bacteria contamination, and can even release the active biomolecules encapsulated at specific rates that match wound healing necessities. In addition, they need to be highly biocompatible and encapsulate high amounts of the biomolecule. It is also required that they are easy to apply into the wound, which means, for NPs and self-assembling carriers, to be included in another formulation. 146
The translation of these technologies into the market and, therefore, in the development of new healing therapies has several hurdles that should be addressed. From a biological perspective, the limited knowledge of the pathophysiology of patients is the major one. Both in the healthy and diseased states, there is a need to understand the in vivo fate of the interactions of NPs with blood, tissue, cellular, and intracellular compartments. 147
On the other side, from a technological point of view, the major obstacle is to gain insight into the physicochemical properties of such nanoscale systems, as well as their in vivo behavior and toxicity. 67
For nanotechnology systems to have a feasible clinical scalability and market transfer potential, the difficulty in their development requires to be simplified. The goal is to fabricate reproducible, controlled, and monitored nanotechnology platforms. Thus, there is a need to improve the synthesis and characterization of the nanotechnology-based wound healing systems, as well as to introduce site-specificity and targeting ability to decrease the undesirable effects of these nanosystems in the human body. In addition, some aspects like systemic absorption or the polymers/materials used for their fabrication, that in general are no-FDA approved materials, need also to be addressed.
Summary
Chronic wounds present a disrupted repair process, taking several months to show progress. They cause pain, infections, costs, and frequently lead to amputations or sepsis, persisting as a silent epidemic affecting over 40 million people worldwide. Traditional dressings cannot fully address all the wound healing necessities. Thus, new technologies are needed. A high variety of nanoplatforms are being explored for chronic wound treatment, specifically in the case of diabetic wounds. Herein, we focused on NPs, nanofibers, and self-assembling nanocarriers used for the treatment of diabetic wounds. Among NPs, we can categorize them in two groups, active NPs and delivery systems. Metallic (AgNPs, AuNPs, etc.) and ion release NPs have shown their potential as antimicrobial agents and for enhancing the wound closure. On the other side, NPs for drug delivery have been applied for the sustained release of GFs, drugs, or nucleic acids and can be made from different polymers like polyesters, lipids, polysaccharides, or peptides. In general, these systems are included in other formulations (gels, nanofibers) to ease its application. Nanofibers are ideal wound dressings as they can mimic the ECM of the skin and allow the oxygen/nutrient interchange. Moreover, they can load biomolecules in their matrix or even NPs encapsulating biomolecules to render different release profiles of the biomolecules that can match the needs of the wound physiopathology. Polymers like hyaluronic acid, collagen, SF, polyesters, or self-assembled peptides have proved their potential for the fabrication of nanofiber as wound dressing. Liposomes are also interesting approaches for the treatment of wounds, especially for nucleic acids, as they can protect them from degradation and deliver them intracellularly, working as gen delivery systems. Nevertheless, more efforts are required for the obtaining of new nanomaterials that can be used and approved by the regulatory agencies.
Take-Home Messages
Traditional dressings cannot fully address all the chronic wound healing necessities, and new technologies are needed.
Current new nanoplatforms used for chronic wound healing include NPs, nanofibers, and self-assembling nanocarriers.
Metallic and ion release NPs have shown their potential as antimicrobial agents and for improving wound closure. NPs can also be used as delivery systems for therapeutics like GFs, drugs, or nucleic acids.
Nanofibers are ideal wound dressings as they can mimic the skin ECM and allow the oxygen/nutrient interchange. Moreover, they can load biomolecules in their matrix or even nanocarriers encapsulating the active ingredients.
Liposomes have a high potential for the intracellular delivery of genes involved in wound healing.
Bigger efforts are needed to develop new nanomaterials that can be approved by the regulatory agencies. Safety assessment, differences in bioavailability, and scale-up problems, among others, are some of the issues that need to be addressed.
Footnotes
Acknowledgments and Funding Sources
This work was supported by the Spanish Ministry of Economy and Competitiveness (MINECO/FEDER) through the project MAT2012–38793 and MAT2015-68906-R and the Dermoglass project funded by CaixaImpulse Programme of Obra Social La Caixa (CaixaImpulse CI0015). Barbara Blanco-Fernandez acknowledges the Marie Skłodowska-Curie grant (agreement no. 712754) and the Severo Ochoa grant (SEV-2014-0425). O. Castano acknowledges the support from the Serra Hunter programme.
Author Disclosure and Ghostwriting
No competing financial interests exist. The content of this article was expressly written by the authors listed. No ghostwriters were used to write this article.
About the Authors