
Abstract
Significance:
Negative pressure wound therapy (NPWT) has become a valuable adjunct in the treatment of acute and chronic wounds in several surgical disciplines. Retained foams are among its side effects, and they pose a rare but devastating complication at the site of this therapy, which might be associated with wound-healing complications, infection persistence, repeated surgical revisions, and prolonged antibiotic courses.
Recent Advances:
In the past 15 years, an increasing number of studies have identified this potential problem. Although the exact incidence remains unknown, initial studies have indicated rates of up to 10% in large collectives being treated by NPWT.
Critical Issues:
The lack of radiopaque markers does not allow for the visual control of retained foams using plain radiographs. Further imaging methods (e.g., CT and MRI) also do not help in adequate differential diagnosis. The lack of routine documentation of the number, type, and localization of the inserted foam(s) and unplanned surgery with a different surgical team pose risk factors for foam retainment.
Future Directions:
Introducing new documentation records for wounds treated with NPWT is recommended. At foam removal, all dressing materials should be examined for integrity. The development of foams with radiopaque markers by the industry, such as those routinely used in surgical gauze swabs, might also be a useful step to minimize the risk of foam retainment within wounds.

Scope and Significance
Negative pressure wound therapy (NPWT) or vacuum-assisted closure (VAC) therapy was first introduced into clinical practice in the early 1990s by Fleischmann et al. 1 Following the breakthrough works of Argenta and Morykwas 2 and Morykwas et al., 3 NPWT was established as a valuable adjunct in the treatment of acute and chronic wounds in various surgical disciplines, such as orthopedic and trauma surgery, 4 –7 dermatology, 8,9 and cardiac, 10 tumor, 11 –14 abdominal, 15 and gynecological surgery. 16 This increasing popularity of VAC therapy over the past years has been substantiated by hard numbers in certain countries. In Germany alone, the number of cases treated with NPWT increased by 369% between 2005 and 2015. 17
Translational Relevance
Several advantages have been attributed to NPWT, such as edema elimination, stimulation of perfusion, granulation tissue formation, and bacterial clearance. 18,19 Whereas bacterial clearance from NPWT has been described in clinical and in vitro studies, 20 –22 the exact mechanisms for this phenomenon are not fully understood. The presence of foreign materials, that is, cellulose gauze 23 and polyurethane (PU) and polyvinyl alcohol (PVA) foams, in infected wounds 24 might act under certain circumstances as a colonization medium for bacteria that might have survived surgical debridement. 25,26 The patient would then have a prolonged hospitalization with additional surgical procedures to eliminate the infection.
Clinical Relevance
The accidental retainment of NPWT foams in acute, chronic, or infected wounds might further complicate the clinical course. 27 –35 Over the past two decades, various commercially available NPWT systems have been introduced into clinical practice, which has made familiarity with all systems difficult (Table 1). The different systems in combination with the several surgical indications used, the lack of standardized documentation of the number and localization of inserted foams, and unplanned or emergency surgeries with different surgical teams, might act as predisposing factors for the emergence of this rare complication.
Overview of manufacturer and brand names of devices of negative pressure wound therapy with the use of foam dressings
Discussion
As with every surgical procedure, intra- and perioperative complications can never be excluded, but they can be minimized. Besides the usual complications (e.g., prolonged wound healing, infection, or thrombosis) that might occur in every surgical discipline, retained materials pose relatively rare complications; however, such complications result in serious consequences for patients. Gawande et al. analyzed the risk factors for retained instruments and sponges after surgery in 61 cases. 36 Although difficult to determine, it was estimated that the risk of retained materials was 1 per 3,000 cases of all surgical interventions. Furthermore, 69% of the cases involved sponges, and 31% involved instruments. Fifty-four percent of the foreign bodies were left in the abdomen or pelvis, 22% in the vagina, 7.4% in the thorax, and 17% were left in the spinal canal, face, brain, and extremities. Emergency surgery, unplanned changes in procedures, and high body mass index were identified as risk factors.
A variety of complications have been reported at the NWPT site. Minor complications mostly involve device malfunctions, loss of pressure, and leakage or damage to periwound skin caused by the trac pad. 37,38 Major complications include toxic shock syndrome, 39 bleeding complications, 40 arterial erosion and hemorrhage, 41 empyema, 42 uncontrolled sepsis, 43 and major bleeding complications due to cardiac rupture. 44 Based on these reports, the United States Food and Drug Administration (FDA) has identified bleeding, infection, and retained dressing material as three potentially life-threatening complications of NPWT. 38
Bacterial clearance of the NPWT
Before focusing on the bacterial clearance associated with NPWT, knowledge regarding normal flora and the microbiological spectrum found in acute and chronic wounds is crucial and necessary for the successful management of such cases.
Normal skin flora is usually predominated by Gram-positive organisms, such as staphylococci, micrococci, and diptheroids. 45 In gastrointestinal tract flora, streptococci, lactobacilli, Bacteroides, and Clostridium species are typically present. 45 Urogenital flora usually includes Eschericia coli, staphylococci, streptococci, diptheroids, lactobacilli, and enterococci. 45
In acute wounds, the microbiological spectrum depends primarily on the cause of the emergence of the wound. For example, in burn wounds, an increased abundance of thermophile microbes, such as Aeribacillus, Caldalkalibacillus, and Nesterenkonia, and a decreased abundance of Corynebacterium have been reported. 46 At the site of open fracture wounds, the microbial spectrum is frequently associated with the mechanism of injury and involves mostly staphylococci, Corynebacterium, streptococci, Acinetobacter, anaerococci, and pseudomonas species. 46
In chronic wounds, polymicrobial infections are common, with pseudomonas and staphylococci species being frequently identified. A greater prevalence in biofilm production has been observed in chronic wounds compared with acute ones. 46
It is somewhat paradoxical that retained NPWT foams might act as a cause for infection persistence, when bacterial clearance is claimed to be one of its advantages. As mentioned previously, the exact mechanisms of this action are not fully understood. It has been hypothesized that the application of negative atmospheric pressure leads to decreased interstitial edema, increased tissue blood flow, enhanced oxygenation of local tissues, restoration of capillary basement membrane integrity, stimulation of endothelial cell proliferation, and enhancement of neutrophil oxidative bursts, which then result in the reduction of local bacterial toxins and promotes wound healing. 1,2,18,19 However, an analysis of the available literature reveals little information about this topic, and understanding of the mechanism remains inconclusive.
In their initial study, Morykwas et al. investigated the bacterial kinetics in acute wounds in an animal model. 3 A significant decrease in bacterial counts could be observed only after the fifth day of NPWT, although the therapy was applied from day 1 onward. 3 In another animal model, Lalliss et al. observed a significant decrease of Ps. aeruginosa over 1 week after NPWT compared with traditional wet-to-dry dressings, whereas no significant difference was seen for S. aureus. 20 The positive effect of NPWT on Ps. aeruginosa was further confirmed in another animal model by Wang et al. 47 In a clinical study, Moues et al. examined microbiological findings from tissue samples in 29 cases. 21 Whereas the number of Enterobacteriaceae or anaerobes did not significantly change during therapy, a decrease in the number of nonfermentative rods could be observed. In addition, an increase was evident in the number of S. aureus. In an analysis of tissue and foam samples in an in vitro wound model, Assadian et al. discovered that bacterial levels at sites with and without NPWT were not significantly different after 24, 48, and 72 h. 22 Ćirković et al. demonstrated that NPWT could significantly prevent biofilm formation of a range of methicillin-resistant S. aureus wound isolates. 48 NPWT dressings that were changed one or two times per week had significantly greater antibiofilm activity than those changed at 3-day intervals. Weed et al. retrospectively investigated the degree of bacterial bioburden during NPWT in the treatment of acute and chronic wounds. 49 During therapy, 43% of the wounds exhibited an increase in bacterial bioburden, 35% displayed no change, and 22% displayed a decrease in bacterial load; however, these values were not significantly different.
In their systematic review on the effect of the VAC therapy on bacterial load and bacterial type, Patmo et al. evaluated data from five clinical studies (two randomized and two nonrandomized retrospective studies comparing NPWT to conventional therapy and one study describing a retrospective cohort of patients treated with NPWT). 50 Due to various heterogeneous data among the studies, the authors concluded that there was low-quality evidence that NPWT had no effect on bacterial load.
Besides these inhomogeneous literature data, the effects of pressure height and type (continuous vs. intermittent) on bacterial clearance also remain unknown. Moreover, it is unclear whether a difference exists among the different systems of the different manufacturers.
Retained foams in NPWT–literature overview
A literature search up to June 2019 in PubMed revealed nine studies reporting on foam retainment after NPWT (Table 2). 27 –35 All studies had an evidence level of IV. All publications, except for one, were case reports. Several surgical disciplines were involved, including abdominal, gynecological, orthopedic, trauma, and pediatric surgery. In the great majority of cases, the retained foams were PU (Table 2).
Overview of studies reporting on retained negative pressure wound therapy foams
n.r., not reported; n.c.s., not clearly stated; ESR, erythrocyte sedimentation rate; CRP, C-reactive protein; CT, computed tomography; MRI, magnetic resonance imaging; PU, polyurethane.
Although the small number of included studies does not allow for generalization of conclusions, the foam composition and the associated surface roughness might pose a relevant risk factor for retainment of NPWT foams. Due to their synthetic route and chemistry, PU foams are hydrophobic, whereas PVA foams are hydrophilic. 51 There are great differences with regard to thickness, density, tensile strength, and elongation, with the PVA foams having a smaller pore size than PU foams. 51 PU foams present large pores with interconnectivity, whereas PVA foams present broader pore size distribution with poor interconnectivity. 51 Therefore, PVA foams are usually used in wounds where lower adherence to or restriction of granulation tissue ingrowth is required. 51 Based on these facts, PU foams theoretically have a higher risk of fragmentation during foam removal due to the more aggressive ingrowth into surrounding tissue compared with PVA foams.
The precise incidence of retained foams after VAC therapy is unknown and difficult to determine due to therapy setting (inpatient vs. outpatient). Most identified studies are case reports with no exact statements about the incidence of this complication within a large collective. 27–28,31 –35 Only two studies provide some information about this topic. Caniano et al. described the presence of retained VAC foams in 2 out of 21 patients (9.5%) suffering from pilonidal disease. 29 Dessy et al. observed this complication in 11 out of 345 patients (3.2%) with chronic ulcers. 30 Unfortunately, no study has provided any information about the rate of fragmented foams in clinical practice, although it could be assumed that there might be a high rate of unrecognized fragmented foams left in situ among several surgical disciplines.
The Manufacturer and User Facility Device Experience Database, maintained by the FDA, might serve as a tool for an approximate determination of this rate. However, this is a voluntary self-reporting system. Therefore, the actual incidence could be under-reported if no reports are sent to the particular device manufacturer.
Due to the variability in symptoms and therapy settings, the correct and timely diagnosis of retained foam(s) after NPWT on the one hand and the ideal imaging method on the other hand pose two major difficulties at the site of these cases. Our literature review revealed a broad range of time intervals between the primary and revision surgery, varying from 1 month to 5 years (Table 2). Information about laboratory parameters were provided only in one study 34 and showed a slight elevation of the erythrocyte sedimentation rate and C-reactive protein levels (Table 2). However, such parameters are not always helpful and reliable in the differential diagnoses of these cases. Furthermore, six of the nine studies reported that various imaging methods involving plain radiographs and/or computed tomography (CT) and/or magnetic resonance imaging were used for further clarification (Table 2). However, the particular imaging method was not indicative of the retained foams but rather of abscess formations or cavities in these studies.
Another potential risk factor at the NWPT site regards the number of dressing changes over a long time period. In the management of chronic wounds, it is not unusual that more than one change is required to achieve good granulation of the wound or even complete closure. In Dessy et al., an average of 14.5 [6–28] dressing changes were conducted during a mean of 6.3 weeks [4–8]. 30 Such results may have implications for foam retainment: The higher the number of dressing changes, the higher the risk of complications and in particular the risk of retained foam might become.
At the site of the surgical revision and removal of retained foams, it is not uncommon that the retained foam is heavily encapsulated or strongly adherent to the surrounding soft tissues. 27–28 In most reported cases, repeated incisions, drainage procedures, or even rotational flaps and a prolonged antibiotic course were required for wound healing. 30,32 –35
The complexity of the interpretation of the imaging methods as well as the surgical revision at the site of the complication is illustrated at the sites of two clinical cases in our own collective (Figs. 1 –11).

Case 1: Anteroposterior (left) and lateral (right) radiographs of the distal femur and knee joint of a 59-year old man. The patient underwent 12 revisions over a time period of 3 months due to a soft tissue abscess of the distal lateral femur 9 months before his presentation in our department. Seven of the revisions involved NPWT. NPWT, negative pressure wound therapy
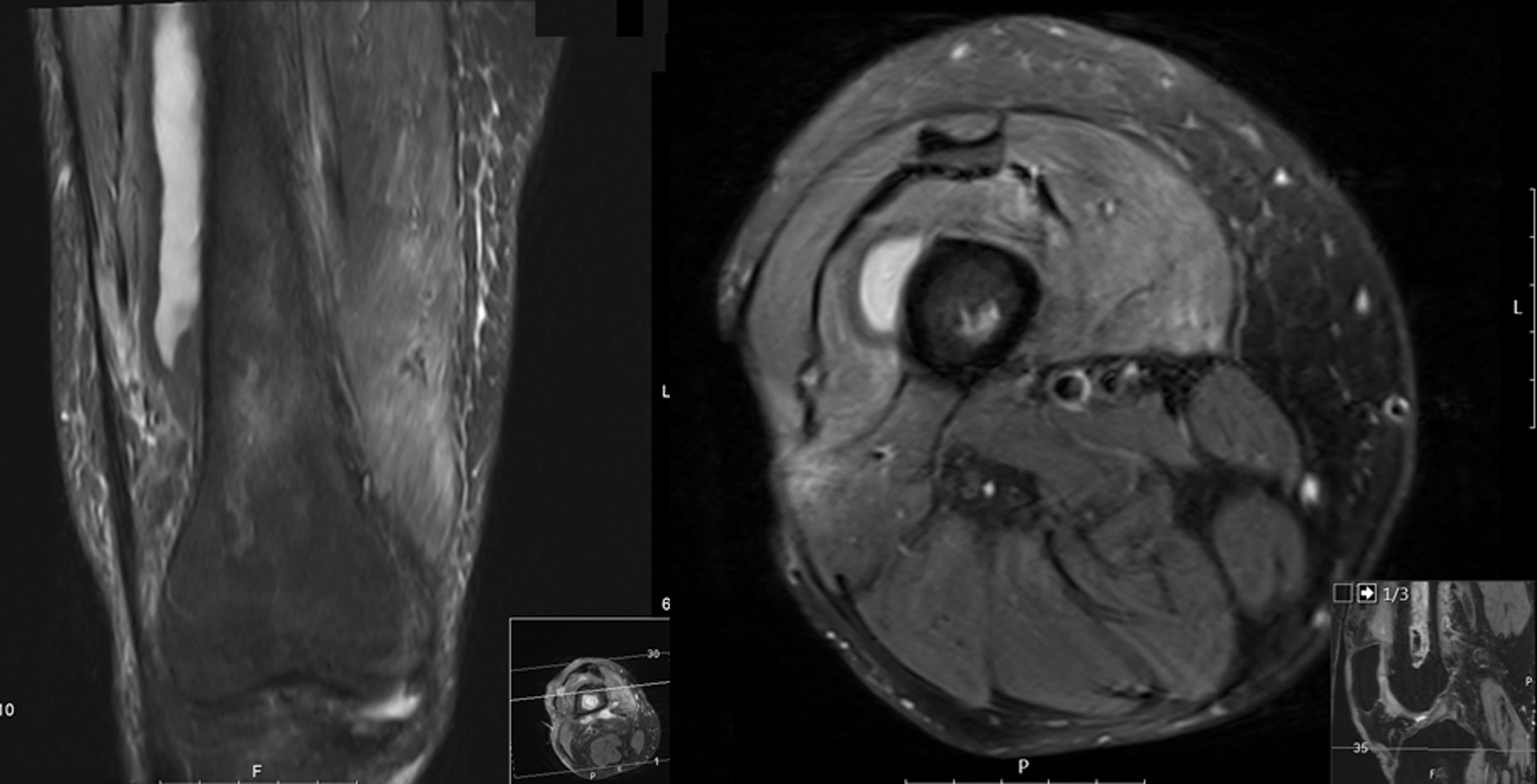
The T2-weighted MRI (left: coronal; right: axial views) revealed a 10 × 1.5 × 2 cm large formation over the anterolateral femur, being indicative for an abscess persistence.

After mobilization of the proximal parts of the fibers of the M. vastus lateralis, a retained polyurethane foam became evident.

At further exposure, the polyurethane foam was identified to be partly embedded in the M. vastus intermedius.

The surgical sites after complete removal of the retained foam.

The excised polyurethane foam (16 × 4 × 2 cm).
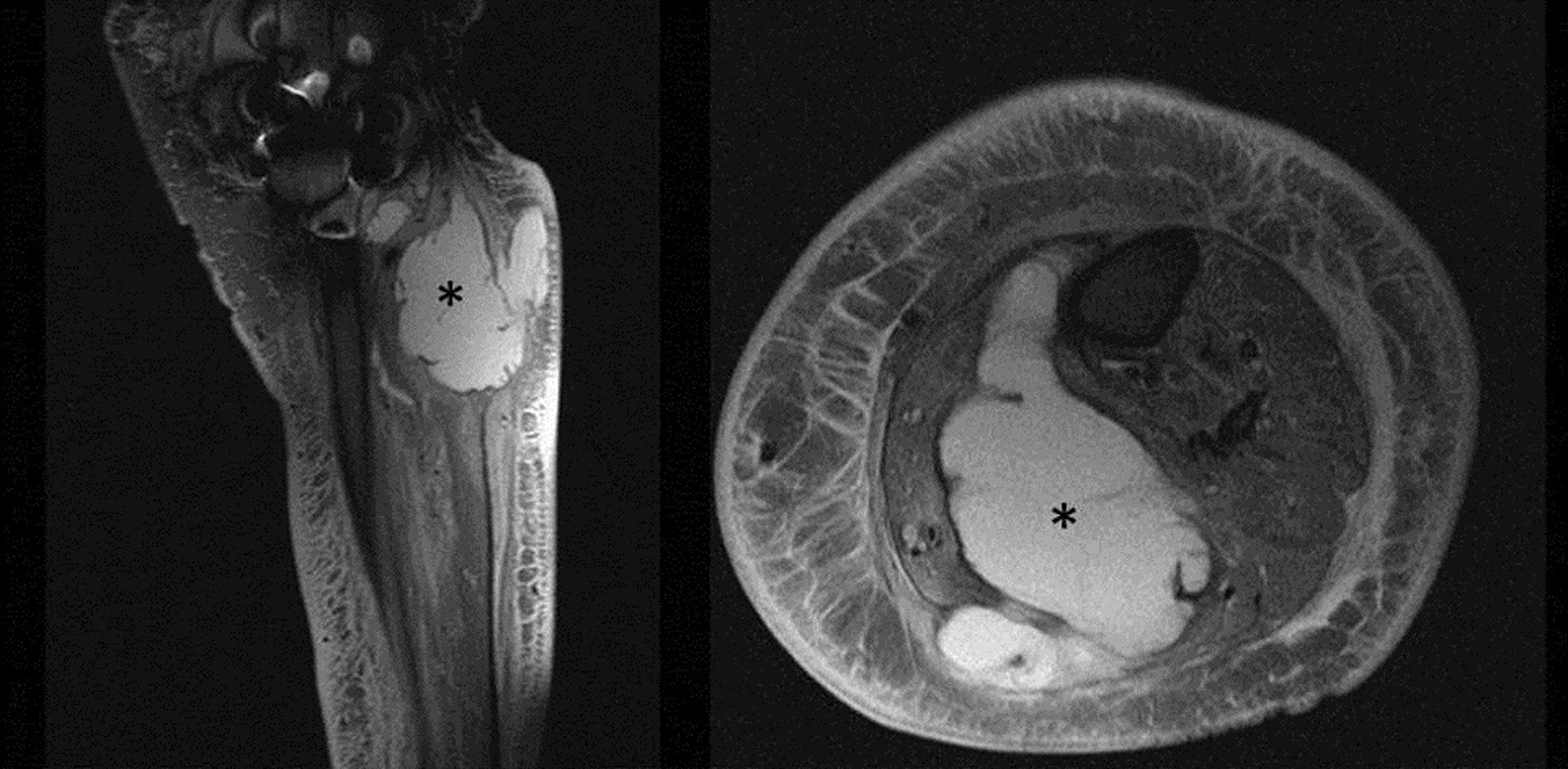
Case 2: Preoperative MRI (left: sagittal; right: axial views) of the left proximal dorsal shank of a 52-year old female patient showing a large abscess formation (“*”) between the medial and lateral head of the M. gastrocnemius. The patient was treated with abscess drainage and means of the NPWT in another hospital.
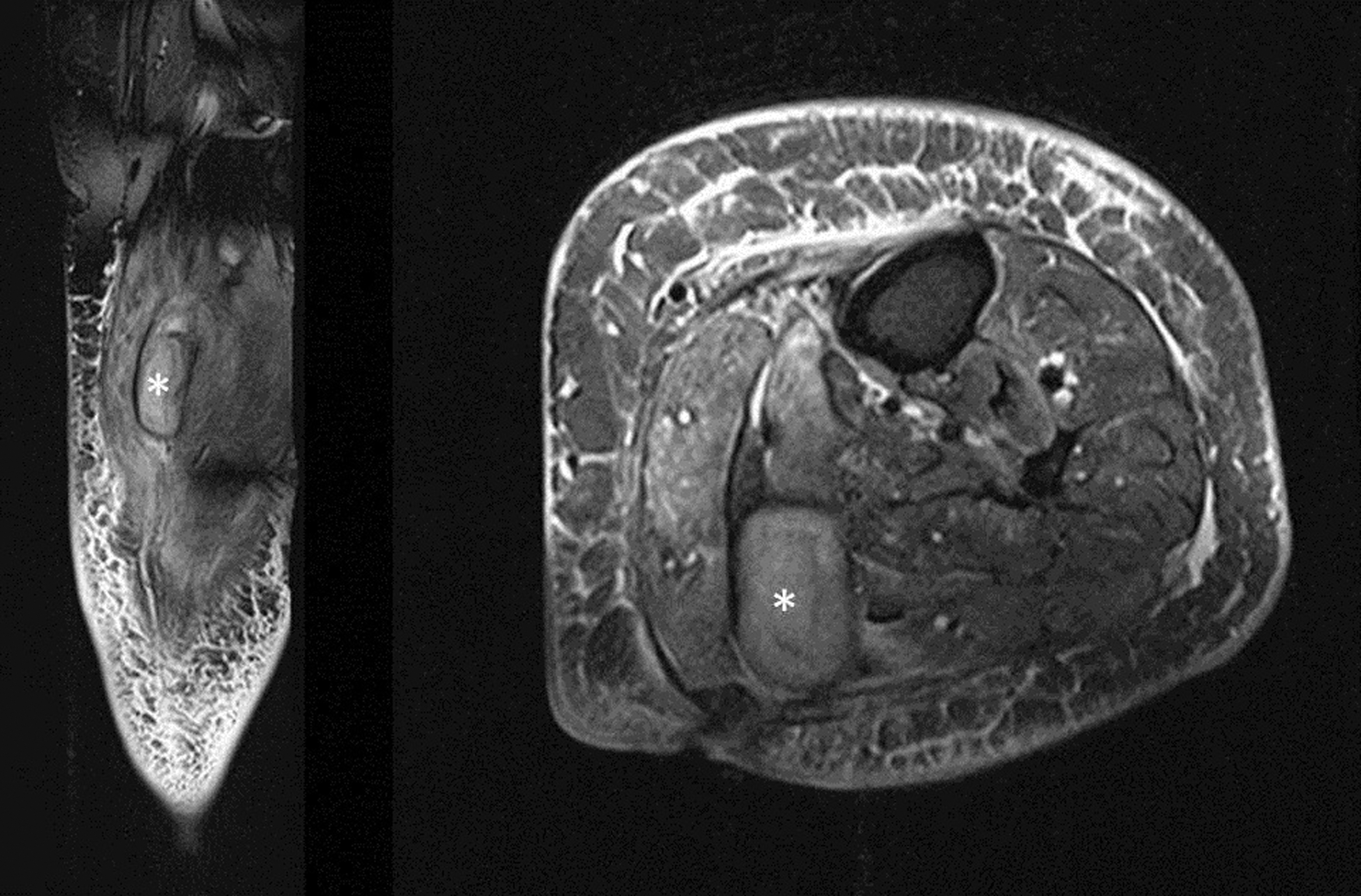
Three months after NPWT ending, a new MRI (left: sagittal; right: axial views) was performed due to persistence of complaints. A structure between the medial and lateral head of the M. gastrocnemius (“*”) was evident, highly suspicious for a recurrent abscess.
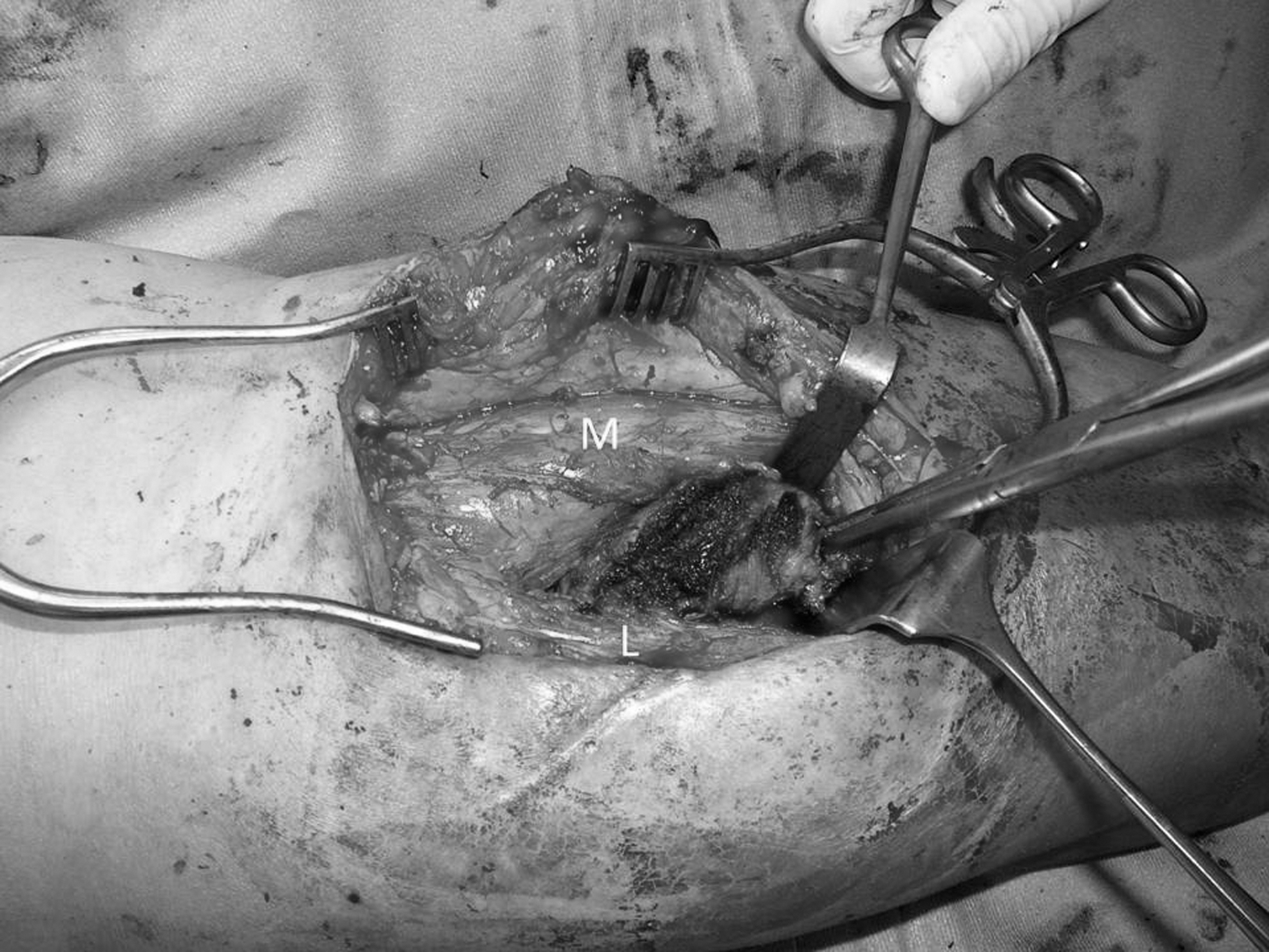
Intraoperative findings. Between the medial (“M”) and lateral (“L”) head of the M. gastrocnemius a polyurethane foam was found, mostly covered by fibrous tissue.
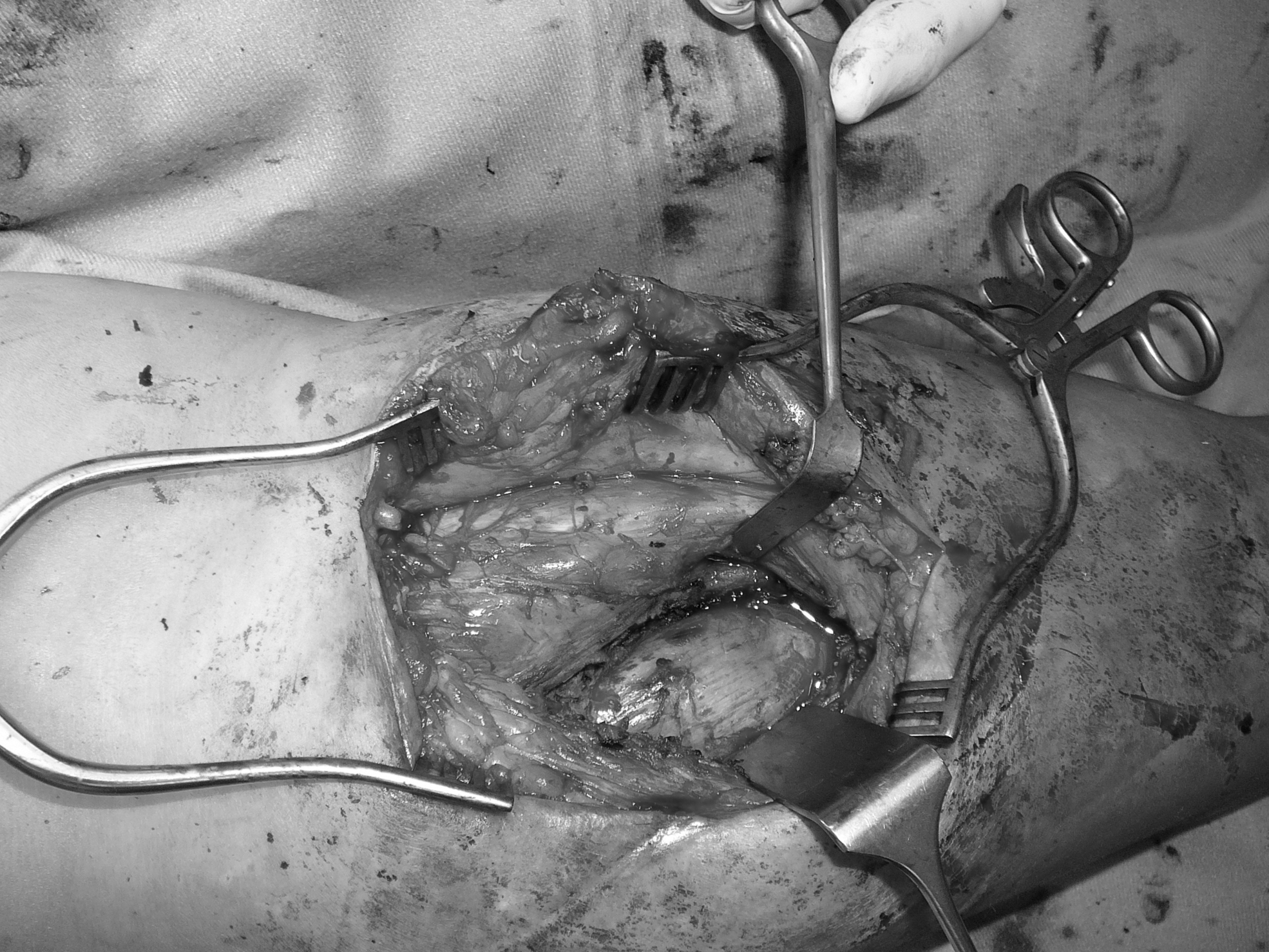
The polyurethane foam could be completely excised.
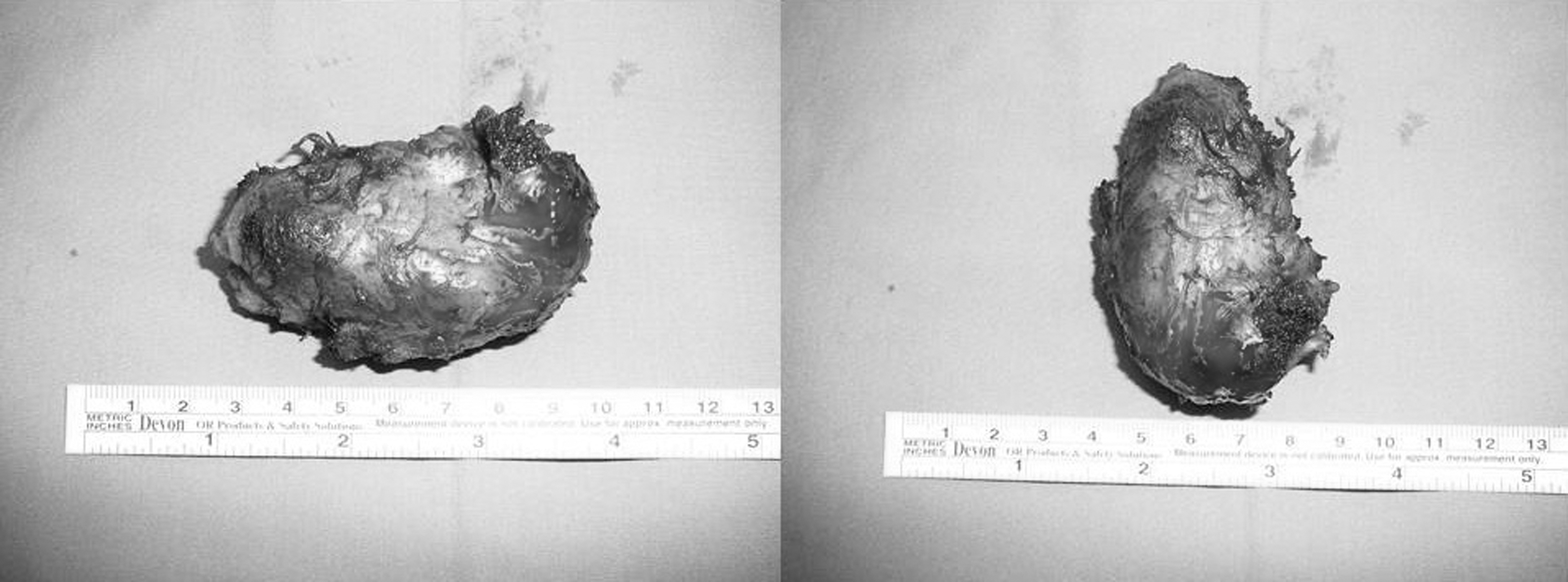
The excised polyurethane foam (8 × 4 × 4 cm).
Why do retained foams pose a risk for persistence of infection?
The effects of wound dressing incorporation as a foreign body into wound granulation tissue is a broader issue that has not only been observed at NPWT sites. Increased infection rates have also been reported when gauze dressings have been used on acute 52 and chronic 53 wounds.
There exists a variety of reasons why retained foams might pose a risk for infection persistence. During therapy, NPWT foams can be colonized by various pathogen organisms. Anagnostakos and Mosser investigated the microbiological cultures of 101 NPWT dressings in 64 orthopedic patients and compared them with those isolated from tissue samples. 25 At least one organism could be identified in 39% of cases, with Enterococcus faecalis and Staphylococcus epidermidis being the most frequent isolated organisms on the foams. In 31% of these cases, the organisms in the tissue samples and on the foams were identical. In 5% of cases, a different organism was isolated on the foam than in the tissue samples. In 15% of cases, the microbiological findings of the tissue samples were negative but positive on foam samples. In 49% of cases, an organism was detected on the foams, whereas no tissue samples were microbiologically examined.
Since microorganisms are attached to the large surface of the foam as biofilm, Yusuf et al. speculated that special methods are required to dislodge and quantify such organisms. 26 In their study, 68 foams from 17 consecutive patients were examined by means of sonication. No comparison was made with tissue samples. Colonized foams were observed in 54% of cases. In 22% of cases, more than three types of bacteria were cultured, and in 32% of cases, two bacteria species were cultured. A single type of bacteria was found in 43% of foams, whereas in 3% of the foams, no bacteria were evident. In polymicrobial NPWT foams, the most common bacteria were from the family of Enterobacteriaceae, followed by Staphylococcus aureus. In NPWT foams with a growth of a single bacterium, the most common bacterium was E. coli. Foams originating from a central location had a significantly higher bacterial load than those from the lower extremities, and these foams were also significantly associated with having more polymicrobial colonization. The authors interpreted the higher rate of bacterial growth compared with the study of Anagnostakos and Mosser 25 by suggesting that sonication had a higher sensitivity and specificity compared with normal cultures. Scherrer et al. studied the diagnostic value of microorganisms cultured from NPWT foam samples compared with that of microorganisms cultured from deep tissue samples from patients with vascular graft infections. 54 A total of 192 samples from 54 patients were examined. In 20% of wounds and in 18% of foam samples, multiple organisms were found (no significant difference). In 19 NPWT foam samples, 26 different microorganisms that were not found in the deep tissue samples were detected. Fourteen microorganisms had been previously detected in tissue/graft or blood culture samples from respective patients, and an additional three were discovered at a later time point. One of these three organisms was judged as clinically relevant, meaning that the detection did lead to treatment adaptation. The overall sensitivity, specificity, positive, and negative predictive values were 58%, 86%, 81%, and 66%, respectively. The authors concluded that the diagnostic value of microbiological cultures from NPWT foams was therefore poor.
These findings provide some important information in the interpretation of the clinical consequences of retained foams. Although most manufacturers suggest that therapy can be discontinued for up to 2 h before a dressing must be replaced, 55 a longer pause of suction during therapy might lead to an increase of anaerobic bacteria, 56 thereby further complicating the wound healing process.
Since various bacterial and mycotic species can potentially adhere to or colonize both foam materials, 57 –61 and these organisms frequently differ from those isolated in tissue samples, 25,54 the type and length of systemic antibiotic is also an important factor to consider. In most surgical disciplines, there exists no strict guidelines in which the length of systemic antibiotic therapy is clearly defined. Therefore, it is possible that at the site of a retained foam, ending systemic antibiotic therapy too early might promote infection persistence. Furthermore, since some clinicians do not send parts of the foam removed along with tissue samples for further microbiological examination, it is possible that the systemic antibiotic therapy is not completely effective if a polymicrobial infection is present and the antibiotic therapy is solely based on the microbiological findings of the tissue samples. Hence, systemic antibiotic therapy needs to be adapted based on microbiological findings. Due to the ability of various bacteria to produce biofilm, 57,61 –64 the theoretical risk of infection persistence rises when a foam is retained and with any bacteria that have survived the surgical debridement as well as the effect of the systemic antibiotic therapy.
Lastly, it is important to know that the local pharmacokinetic properties of the systemically applied antibiotics might vary at the site of the VAC therapy. In a prospective, observational study of burn and trauma patients, Rowan et al. investigated serum levels of vancomycin, ciprofloxacin, cefazolin, and piperacillin/tazobactam, as well as the total and unbound antibiotic concentrations in the wound exudate. 65 It was observed that vancomycin, ciprofloxacin, and piperacillin/tazobactam all penetrated wounds with exudate-to-plasma concentration ratios of more than 0.8. Cefazolin did not demonstrate the same effectiveness, with an average exudate-to-plasma concentration of 0.51. The authors concluded that despite limited available clinical data on the wound penetration of antibiotics in patients undergoing NPWT, these data suggest that antibiotics have different capacities for wound penetration during NPWT that should be borne in mind when making clinical decisions.
Measures for prevention and detection of retainment of NPWT foams in wounds
The European Wound Management Association (EWMA) recently recognized the need to improve documentation, communication, and patient safety regarding the use of NPWT.
55
Several authors have emphasized the necessity for introduction and establishment of different processes for the prevention and detection of NPWT foam retainment in wounds: - Although frequently difficult in clinical practice, the same surgical team should ideally perform all VAC revisions until the end of the therapy. - The surgical team should be familiar with the device and the foams of VAC therapy. In some cases, complications might occur due to lack of experience with the particular therapy. Caniano et al. stated that complications after NPWT, such as retained materials and device malfunction, were seen early in their series and that increased skill and familiarity with the device by home health care nurses in their referral region have eliminated these issues.
29
- A count of the inserted foams should be made at each procedure (similar to the standard practice for swabs, needles, and instruments).
27,34,38
- Attempts should be made to use the largest single piece of foam in the wound bed. Whenever possible, the use of more than one piece of foam should be avoided.
38
- If foams have to be trimmed for any reason, this should occur in a manner that does not promote fragmentation upon removal. The trimming itself should take place away from the wound and the patient to reduce the risk of fragments in the wound.
38
- The precise number of the inserted foams and their localization(s) should be consistently documented in the operative note, so that even if another team should carry out the next revision surgery, all foams could be easily and reliably identified.
27,34,35,38
In some hospitals, new documentation records for wounds treated with vacuum therapy have been introduced for avoidance of such errors.
28
Even if some newer therapy device (e.g., InfoVAC®) allows the individual changing the dressing to electronically record the number of foam fragments in the wound, such devices are not used in every hospital and in every discipline. Furthermore, it is the responsibility of the surgical team and not of the electronic device to provide a precise and errorless documentation of all used materials. - The team should be consulted if wound characteristics change in a manner that might result in fragmentation of the foams.
38
- The removal of the foams should be done carefully. In some cases, the foams are so adherent to the surrounding soft tissues that local application of saline or sterile water is recommended to loosen the foam before removal is reattempted.
38,66
- At foam removal, all dressing materials should be examined for integrity. Should any discrepancy be evident with regard to the number or size of the removed foams, the wound should be further explored to resolve this discrepancy.
34,38
- The development of foams with radiopaque markers, such as those routinely used in surgical gauze swabs, would minimize the risk of retaining a foam within the wound, since an intraoperative fluoroscopic control at the end of surgery would easily help in identifying any foams.
27,32,34,35
Patients with deep, complex, and large wounds are theoretically more prone to have a complication than those with small or superficial wounds (“low-risk wounds”). The correct definition of low-risk wounds might be difficult and partly subjective, especially when several medical disciplines are involved. However, from a clinical perspective, all wounds that are solely limited to the skin and that do not have any tunnels through different anatomic layers might be defined as low risk. Small precautions could make a difference in the management of these wounds (e.g., placement of a paraffin gauze between the NPWT foams and the wound bed). Therefore, these cases may not require such advanced procedures as mentioned above. 38 However, we believe that having a standardized procedure for all treatment cases of the same kind would be more effective than dividing patients into several categories, because by that it is only a matter of time until errors and/or complications occur.
Summary
Empirical data from the past 15 years along with announcements by the FDA have emphasized the potential risk of foam retainment at NPWT sites. Although the precise rate of this complication is unknown, it could be assumed that it is underestimated. Prolonged clinical courses with unclear imaging findings and various differential diagnoses are the consequences. Acknowledgement of this possible complication, sensitization of participating medical staff, and introduction of several measures for prevention and detection of retained VAC foams should build the foundation for minimizing this complication in the future.
Take-Home Messages
The retainment of NPWT foams is a rare but threatening complication, which might endanger the postoperative course and requires repeated incisions, drainage procedures, and prolonged antibiotic therapy.
In cases of infection persistence following multiple dressing changes at the NPWT site and for unclear or suspicious imaging findings, the possibility of a retained foam should be considered as a differential diagnosis.
The documentation of the number, size, type, and localization of all inserted foams should be routinely done in every surgical procedure.
At foam removal, all dressing materials should be carefully examined for integrity. At the smallest doubt that all foams are fully removed, the wound should be further explored.
Footnotes
Acknowledgments and Funding Sources
The present work did not have any financial support.
Author Disclosure and Ghostwriting
No competing financial interests exist. The content of the article was expressly written by the authors listed. No ghostwriters were used to write this article.
About the Authors