
Abstract
Objective:
The goal of this research was to identify a population of diabetic foot ulcer patients who demonstrate a significant response to hyperbaric oxygen therapy (HBOT) using a large sample size to provide guidance for clinicians when treating these complicated patients.
Approach:
The effect of HBOT on diabetic foot ulcers, Wagner grades 3 and 4, was evaluated using a retrospective observational real-world data set. The study reported on the overall healing rate, (74.2%) at the population level, for >2 million wounds.
Results:
When a subgroup of patients of only foot ulcers with a Wagner grade 3 or 4 were considered, the healing rate was only 56.04%. The use of HBOT, without filtering for the number of treatments received, improved the healing rate to 60.01% overall. Healing rates for this same subgroup, however, were improved to 75.24% for patients who completed the prescribed number of hyperbaric treatments.
Innovation:
This observational study discusses the importance of reporting at the population level, specific wound etiology level, a risk-stratified level, and to then overlay the effect of treatment adherence on those outcomes to provide clinicians with a comprehensive understanding of when to prescribe an advanced modality such as hyperbaric oxygen.
Conclusion:
The authors provide healing outcomes data from several prior HBOT studies as well as other advanced modalities that have been used in diabetic foot ulcer care for comparison and context.
William J. Ennis, DO, MBA, MMM, CPE

Introduction
T
The primary focus of this study is to report on the mITT outcomes of HBOT on diabetic ulcers limited to the foot and specifically only the more complex Wagner grades 3 and 4 using the world's largest wound care database. The goal of this research was to identify a population of diabetic foot ulcer patients that demonstrate a significant response to HBOT using a large sample size to provide guidance for clinicians when faced with treating these complicated patients. In addition, this study expands the previously reported mITT wound-healing outcomes to provide continued updates on the outcomes of patients who were still in treatment, and therefore excluded, at the conclusion of the last study period. The wounds in the study are an extension of the previously reported data and, therefore, any concerns about the final outcomes of those patients still in treatment at the end of the last study period should be answered by a similar healing rate and the large sample size in the present trial. Finally, this report adds granularity into specific wound etiology healing outcomes at a population level. Specifically, we studied diabetic foot ulcers that were Wagner grade 3 or 4.
Clinical Problem Addressed
There has been much debate in the literature surrounding the overall benefits of HBOT in wound care. 1,2 Many of the initial studies that resulted in positive outcomes, payment policies, and physician adoption were performed in hospital settings ensuring compliance and thereby, not surprisingly, the results did not translate to an outpatient clinic reality. Studies also reported various primary outcome objectives, making comparisons difficult while confusing clinicians when confronted with an individual case. 3 –5 This observational study discusses the importance of reporting at the population level, specific wound etiology level, a risk-stratified level, and to then overlay the effect of treatment adherence on those outcomes to provide clinicians with a comprehensive understanding of when to prescribe an advanced modality such as hyperbaric oxygen.
Materials and Methods
The initial phase of this study was to review and update the retrospective data on wounds, HBOT, and the final clinical disposition from 682 outpatient wound care centers nationwide between January 1, 2014, and April 28, 2018. The time frame for data inclusion was determined by the availability of aggregate data at the time of analysis. The data were obtained from a proprietary clinical database and collected using a specialized wound data capture system that tracks wound-related treatments and patient outcomes. Nurses and physicians document visits at the point of care. A subset of centers document using paper-based forms, which were then entered into a central system at the end of each work day. Other centers document visits on a fully electronic medical record basis. The data used for the study were compiled into a deidentified research database table distinct from the enterprise data warehouse, before the beginning of the analysis. All patient identifiers were removed from the research file. Deidentified data were extracted using SQL software and analyzed using Stata 14.1. The study was exempt from IRB review by Quorum Review IRB (QR no. 33110).
All centers in the sample were managed by a wound care management company and staffed by a provider panel that consisted of a combination of contract physicians in private practice and a subset of employed providers who practiced wound care full-time. All providers whether contracted or affiliated undergo a formal standardized course in wound healing that includes the management of diabetic foot ulcers before providing care at a wound center. All programs are hospital based and have program directors, managers, nurses, and access to hyperbaric oxygen, and needed specialty consultants. All providers who order and utilize HBOT have completed at a minimum a 40-h course approved by either the Undersea Hyperbaric Medical Society or the American College of Hyperbaric Medicine. All diabetic patients in either HBOT or standard of care only received care based on evidence-based clinical practice guidelines that are used at all centers. All patients, whether offered HBOT or not, undergo glycemic control, debridement as needed, off-loading, appropriate wound care dressings, assessment and revascularization if needed, control of bioburden and, overall management of their comorbid medical conditions. All patients regardless of wound etiology undergo a medical surveillance review process every 4 weeks throughout the course of their wound care treatment to identify patients who are not healing along an anticipated trajectory. Specifically, patients who are being considered for HBOT undergo pretreatment reviews of the medical record to ensure that standard of care was met and that patients did not show meaningful signs of improvement before starting their treatment.
The next phase of the analysis was to create an analytic subsample of diabetic wounds. All Wagner grade 3 or 4 diabetic ulcers that were located on the foot or toe were assessed. The decision to only utilize wounds located on the foot and toe was to focus the outcomes on purely diabetic foot ulcers and not the broader category of diabetic wounds of the lower extremity (DWLE), also an approved HBOT indication. As previously stated, most of the initial HBOT trials were limited to wound locations below the ankle, making more direct comparisons from this study to the existing published literature possible. The sample was further limited to cases in which a single wound was noted to ensure the ability to accurately identify the ulcer for which HBOT was prescribed, including those in active treatment at the time of study closure. The final population size included 25,562 diabetic foot ulcers. The study reports retrospective observational data on healing and amputation outcomes using a mITT framework for outcomes measurement. Additional information regarding the mITT model for outcomes in wound healing has been reported elsewhere, but briefly represents the percentage of all nonactive nonconsultation wounds, with greater than 7 days between first and last assessment, that were healed. In addition, population level healing results were collected and reported by wound etiology. This allows clinicians to put healing rates in context with other types of wound care cases. Cases were then compared by the variable of either receiving or not receiving HBOT. Physicians in the centers contributing data in this study are trained to provide the best standard of care for a minimum of 30 days to assess for a positive healing response. Those who fail to improve are considered potential candidates for several advanced modalities, including HBOT. There would likely be more heterogeneity in the DWLE population as diabetic patients might have ischemic wounds, venous ulcers, or traumatic wounds located somewhere on the lower extremity, which might be coded as having a diabetic etiology. The software used by providers in this study has fields that allow for the documentation of both the primary wound etiology and concomitant medical conditions that could contribute to the patients overall healing capacity. To focus on the potential impact of HBOT on diabetic foot ulcers, the study restricted the location of the wound to below the ankle.
Results
During the study time frame, a total of 2,651,878 wounds were evaluated (Table 1). The population level mITT healing rate was 74.2%, which is consistent with the previously reported 74.6% based on 1,006,690 wounds at the time of that publication. There was variability in the specific wound mITT healing rates from 55.3% to 80.6%. Not surprisingly, arterial wounds demonstrated the lowest healing rates and venous leg ulcers healed at the highest level. The overall healing rate for all wounds classified as diabetic was 70.9% (328,158/462,888) at the population level. At this level of stratification, there does not seem to be a major difference in the overall healing rate for the aggregated overall population of wounds and the rate of healing specifically diabetic wounds using the mITT method previously described. Only patients with a single wound of Wagner grades 3 and 4 located on the foot or toe were included for additional study. The healing and amputation rates for the full sample of Wagner grades 3 and 4 diabetic foot ulcers are reported in Table 2. Once the mITT exclusions are applied, the sample is reduced to 19,057 ulcers with a 56.04% healing rate and a 4.09% amputation rate. This rate is comparable with the mITT population level healing rate for arterial ulcers. By comparison, the mITT healing rate for all wound etiologies previously published by Ennis et al. was 74.6%. 6 The lower healing rate for Wagner grades 3 and 4 is an indication of the difficulty in healing these patients who often have confounding medical comorbid conditions and emphasizes the importance of risk stratification when reporting outcomes. The mITT subpopulation represents 75% of the total population of diabetic foot ulcer patients with the largest group excluded being those still in treatment at the end of the study time frame, which accounted for 18.1% of the total.
Wound healing rates by etiology and aggregate
mITT, modified intent-to-treat.
Modified intent-to-treat healing rate and amputation rate: diabetic single wound Wagner grade 3/4 on foot or toe
Table 3 reports further granular outcomes for patients who received at least one HBOT treatment (6,616) compared with patients who did not receive any HBOT (18,946). After the same mITT exclusions are applied, the patients who received HBOT demonstrated a slightly higher mITT healing rate (60.01%) than patients who did not receive HBOT (54.33%), which results in a 9.47% delta. The mITT amputation rates were consistent between the two groups with a 4.16% amputation rate in the HBOT sample and a 4.06% amputation rate in the non-HBOT group. This improvement in healing rate, however, does not take into account the actual amount of HBOT received or whether the patients completed their entire overall clinical course of care. Table 4 analyzes the patients' treatment based on whether the patients completed their entire clinical treatment protocol divided into those who did or did not receive HBOT. More patients who received HBOT went on to complete their entire wound care treatment protocol. The wound treatment protocol refers to the entire course of therapy that patients receive during their care at the wound center. For example, a patient might receive HBOT and still undergo several more weeks of advanced wound care before reaching a final discharge disposition. Patients who commit to such an intensive therapy such as HBOT, requiring every day treatments for up to 8 weeks, are likely to also be more committed to completing the entire course of therapy. This correlation could also, however, prove to be a confounder and represent a surrogate marker for healthier patients or those with more adherence to their treatment plans. This is a descriptive retrospective study using big data and although correlation may not equal causality, we further analyzed the demographics and wound characteristics for the two groups (HBO and non-HBO) to further identify the potential impact for the therapeutic intervention. Of the 5,742 patients who received HBOT, only 2,597 completed their hyperbaric treatment (45.2%); however, of those patients who did receive a full HBOT course, 75.24% versus 47.44% were healed for a delta of 36.9% (Table 5). These data provide insight into why there are differences in the literature describing efficacy outcomes and how the therapy potentially might lose effectiveness in the outpatient clinic setting when patients fail to adhere to the full treatment regimen. Patients who complete their HBOT received 89% of the prescribed treatments, whereas those marked as incomplete only received 57% of their prescribed treatments (Table 6). The reasons for incomplete HBOT are further detailed in Table 7. These options are preloaded drop-down choices built into the software. The most common reason for an incomplete treatment course was indicated as “Patient Choice” followed by “Wound Progress Plateaued.” Patients who did not complete the ordered treatment course on average only completed 57% (standard deviation [SD] 34) of the mean 38 treatments (SD 12) ordered and discontinued treatment an average of 40 days after the first HBOT treatment (Table 7). Overall, patients who were marked as having chosen to discontinue treatment by their own request completed the lowest percentage of treatments (40%; SD 31), whereas patients marked as “Wound Progress Plateaued” completed the highest percentage of ordered treatments with an average of 88% (SD 21) of the mean 40 treatments ordered (SD 13). A hypothesis to explain this phenomenon is that a provider might continue to treat a patient with the goal of establishing a positive healing trajectory and would, in that case, want to ensure a full course of HBOT was administered before deeming the treatment ineffective. Further information from patients who choose to quit is needed for future studies. Another group that did not complete the course of HBOT are those in which the wound healed during the treatment course. For obvious reasons, this group had no clinical reason to complete their course of therapy. When treatment adherence is not included (data separated by any HBOT vs. no HBOT), the previously noted 60.01% healing rate was observed. Stated another way, patients demonstrated a 23% improvement delta when HBOT is delivered as ordered and the overall treatment plan is adhered to. Of course, this assumes that the patient was medically stabilized, revascularization was performed if indicated and clinically possible, infection was controlled, offloading provided, and the wound received debridement when indicated before, during, and after HBOT was delivered. It is, therefore, imperative that future research includes patient adherence information to fully appreciate the therapeutic benefit achieved with HBOT. These data can also help support patient engagement opportunities, not unlike those employed in pharmaceutical industry to assist providers in achieving the best possible outcomes when using HBOT or any other modality in which total dosing is important. These tables clearly identify two variables critical to considerations of the effectiveness of HBOT in real-world samples: first patients need to complete their overall care in the wound center as HBOT is only adjunctive to good care, and second, when HBOT is ordered, it is critical to complete the course of therapy. Figure 1 identifies mITT healing rates for various subgroups and provides background for topics covered in the discussion section that follows.
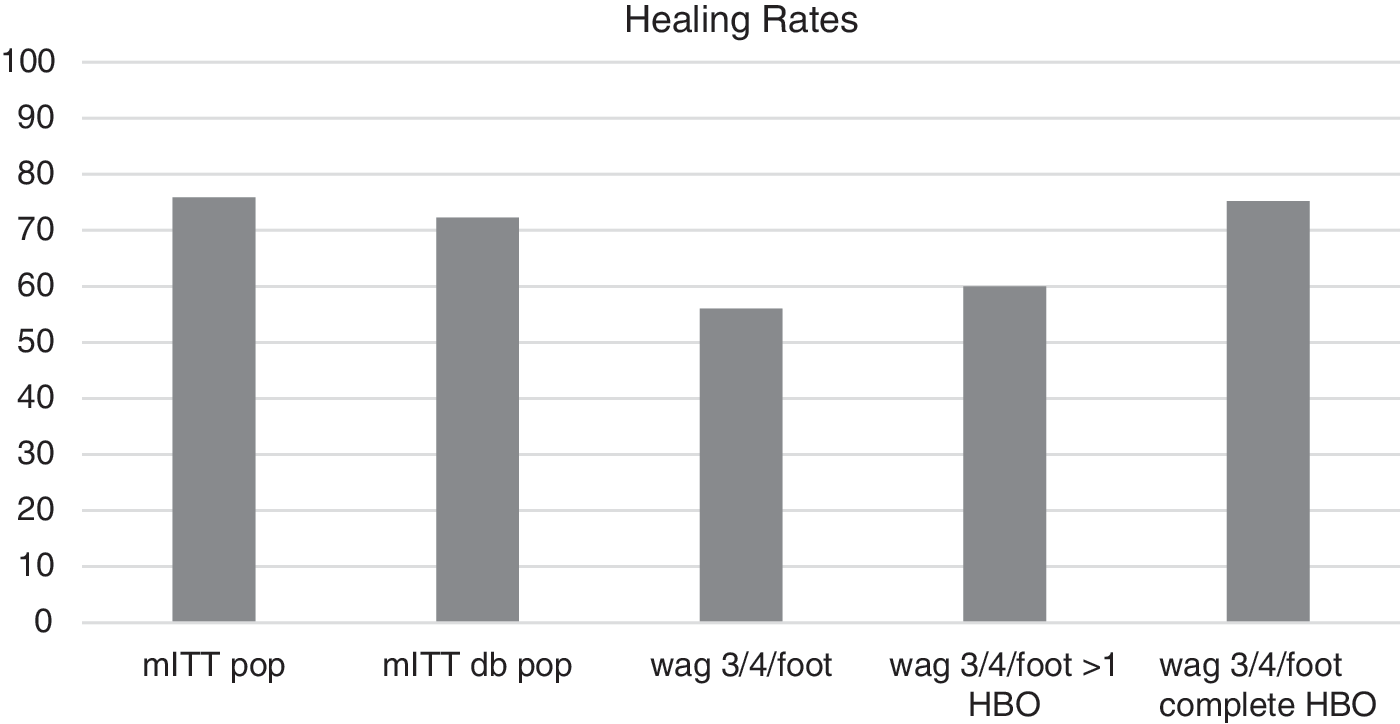
Healing Rates. mITT pop: modified intent-to-treat population level. mITT db pop: modified intent-to-treat diabetic population. wag 3/4/foot: Wagner Grade 3 or 4 on foot. wag 3/4/foot>1 HBO: Wagner Grade 3 or 4 on foot incomplete HBOT. wag 3/4/foot complete HBO: Wagner Grade 3 or 4 on foot completed HBOT treatment course. HBOT, hyperbaric oxygen therapy; mITT, modified intent-to-treat.
Modified intent-to-treat healing rate and amputation rate
Hyperbaric oxygen vs. nonhyperbaric oxygen diabetic Wagner grade 3/4 single wound located on the foot or toe.
HBO, hyperbaric oxygen.
Admission marked as “completed treatment” by hyperbaric oxygen therapy status
Modified intent-to-treat by hyperbaric oxygen therapy course completion hyperbaric oxygen therapy group only
HBOT, hyperbaric oxygen therapy.
Summary statistics for hyperbaric oxygen therapy sample by hyperbaric oxygen therapy course completion
Summary statistics for hyperbaric oxygen therapy sample by reason for incomplete treatment course, hyperbaric oxygen therapy incomplete only
SD, standard deviation.
Discussion
This retrospective study suggests that HBOT can be effective for hard-to-heal Wagner grades 3 and 4 diabetic foot ulcers and demonstrates the complexities of studying the therapy using observational real-world data. Specifically, the results underscore the importance of treatment adherence when analyzing the effectiveness of HBOT. Furthermore, using the mITT framework to report healing outcomes allows for both transparency of results and the ability to compare programs, individual centers, and ultimately providers. Although the population level healing rate provides an overall picture of the effectiveness of wound care centers in general, we also need to analyze results on more granular levels. Venous ulcer healing rates, for example, are frequently reported without segregation into various clinical, etiology, anatomy, and pathophysiology (CEAP) classifications, making it difficult to project an individual patients potential for healing. 7 Arterial ulcer healing rates rarely describe the level and extent of peripheral arterial disease when reporting healing rates. In addition, the methods of establishing revascularization are often not a variable that is considered in the final analysis. Given the fact that HBOT is approved for DWLE, a highly heterogeneous group, separating wounds by anatomic location and Wagner grade may provide different results. Variations in diabetic foot ulcer healing rates have been reported based on hospital designation, that is, community versus tertiary academic center, further complicating how results are interpreted. 8 In that study, the same clinical team provided care using the same protocols at two very different hospital settings. The first, a small community 200-bed hospital and the second, a 700-bed level one trauma tertiary setting. The noted difference in healing rates at these two centers (73.7% vs. 59.5%) achieved by the same clinicians sheds light on patient referral patterns and risk stratification.
There have been several randomized studies that have noted improvements in healing rates of diabetic foot ulcers. A few highly cited articles are described herein. Löndahl et al. published a randomized single-center double-blinded placebo-controlled trial in 2010. 9 The study was conducted in an outpatient setting using a multiplace chamber. Patients received either oxygen or air at 2.5 atmospheres of pressure. The investigators did, however, include Wagner grade 2 ulcers (24% of the cases) in this study, making comparisons with the present study more difficult. More patients healed in the intent-to-treat group (p < 0.03); however, this effect was improved in a per-protocol subgroup, when >35 treatments were received (p < 0.009). This fact supports the findings of this study in that total treatments received matters to the overall outcome. The study was designed for a 1-year time frame and significance was achieved at 9 months. Kessler et al. randomized 28 patients with diabetic foot ulcers who were admitted to an inpatient hospital unit to receive HBOT or standard of care. The patients were given two HBOT treatments per day, 5 days a week for 2 weeks. 10 All patients had normal vascular examinations before enrollment. There was a significant reduction in wound area at the end of the 2 weeks in the HBOT patients, but upon discharge the significant improvement was lost as both groups improved similarly. The HBOT impact in the first 2 weeks was significant given that both groups were receiving intense inpatient management and the only differential treatment was the use of HBOT. Questions raised by this trial design include why was the healing trajectory benefits of early HBOT lost once the HBOT was discontinued. Duzgan et al. demonstrated a 66% healing rate compared with 0% in an inpatient setting treating infected diabetic foot ulcers. 11 The protocol included two treatments per day followed by one treatment a day on a basis for 20–30 days. Many subsequent reviewers were troubled by the control group having no patients healed. The inpatient setting likely had an impact on diet, offloading, medication adherence, and glucose control, all of which are more difficult to manage in the outpatient setting. In addition, the patients were not in the hospital for >1 month, so it is not unreasonable that the healing rate for this site of care would not be comparable with an outpatient trial, for example. Abidia et al. studied nonreconstructable vascular patients with a diabetic foot ulcer and found statistically improved healing at 6 weeks and 1 year. 12 The protocol was daily HBOT at 2.4 air pressure absolute, 5 days a week for 30 treatments. Interestingly in this study even though the ulcer dimensions in the control group became smaller, they did not go on to healing at the 1 -year mark. This concept has been discussed by the FDA as a reason that wound-healing studies need to include total closure as one of the outcomes to ensure that early rapid healing does not actually negatively impact the ultimate outcome of healing. 13 This is also why studies looking at alternative surrogate markers for healing need to ensure that complete healing is in fact predicted by the earlier time frame-based surrogate. 14 Kalani et al. reported on 38 patients with nonreconstructable vascular disease and diabetic foot ulcers for a 3-year period. 15 HBOT-treated patients reported a 76% healing rate compared with 48% in the control arm. Patients received between 40 and 60 treatments. In all of these studies, there was a positive trend for HBOT when healing outcomes are measured. The problem with all of the studies, however, is the variation in HBOT treatment frequency, total number of HBOT treatments, small sample size, various sites of care that impacted adherence, and variations in major comorbid conditions such as infection and vascular status. The published outcomes of other advanced modalities, for example, ultrasound therapy, have also been challenged due to various protocols, dosing regimens, and the use of various wound etiologies without risk adjustment being used in a single trial. 16
Not all studies have found a positive correlation with the use of HBOT and the healing of diabetic foot ulcers however. As with the literature purporting a positive impact of HBOT, the publications that found no effect have limitations as well. Margolis et al. published a retrospective review of a large database using propensity scoring. 17 There was a median of 29 treatments delivered in the HBOT arm but no description of healing rates correlating with the number of treatments actually received. This study on a cohort of 6,259 patients failed to demonstrate an improvement in healing for nonischemic diabetic foot ulcers. An article published in 2016 that used a double-blinded sham protocol for diabetic foot ulcer treatment with HBOT found no statistical reduction in the recommendation for amputation. 18 Surprisingly, these patients did not actually receive amputations, they were simply evaluated by a single surgeon through photographs and a decision for amputation was created at that point. There was much disagreement with this study as documented by published letters to the editor requesting further clarifications. 19
A Cochrane review also failed to support HBOT but noted the positive trends in wound healing in the short term but not the long term and recommended additional, higher quality studies to be performed in the future. 20
The importance in selecting an appropriate delta is critical when doing a power calculation to determine the total number of patients needed for a study. Given the paucity of consistent findings in the HBOT literature, this poses a challenge to researchers conducting power calculations for studies of HBOT. As a result, studies that are often conducted using underpowered designs or clinical criteria for inclusion may be extended to patients who would not typically benefit from the therapy to meet the needed sample size. Recent literature describes the risks of using random methods to assign delta values and the bias introduced by doing so. A recent trial conducted at several centers in the Netherlands evaluated diabetic foot ulcers with a study powered to an anticipated delta of 12% improvement of limb salvage. When enrollment failed to meet targets, the delta was increased to a 25% limb salvage benefit and a 29% improvement in healing. 21 By arbitrarily doubling the expected delta, the findings of the study are at substantial risk of bias and unlikely to detect a significant effect of the therapy. Although the authors clearly articulate this limitation, its nuance may be overlooked by clinical audiences. In addition to the underpowered study design, patients were combined and crossed over due to patient preference, leaving only 39 patients who completed HBOT. Despite these shortcomings, the trends were all in favor of HBOT. It is of interest to note that in this study, only 65% of patients undergoing HBOT were able to complete their course of treatment. A per-protocol analysis did show that the patients who completed HBOT did have statistically significantly less amputations and higher amputation-free survival. This is consistent with the findings in this report.
Providers have other advanced treatment options when caring for diabetic foot ulcer patients. There have been few treatments, however, that have undergone rigorous clinical trials at the randomized controlled trial (RCT) level. Guidelines have been proposed by several professional societies for treatment of diabetic foot ulcers. 22,23 Most guidelines recommend performing standard of care for at least 1 month before considering any of the advanced modalities. The percentage area reduction in 1 month has repeatedly been found to be a useful surrogate for predicting those patients who will likely go on to heal compared with those in which advanced treatments should be considered. 24 –26 The providers practicing in the centers whose data comprise this study are all trained to provide at least 1 month of standard of care, and to monitor wound-healing trajectories before using advanced therapies. All coverage and reimbursement criteria include these standards as well. A well-documented method of off-loading for diabetic foot ulcer patients is the use of total contact casting. Despite having strong evidence to support its effectiveness, total contact casting is not frequently used in many wound care centers. 27,28 Once a patient has been identified as being hard to heal, and having failed standard of care, the clinician has several options that have been studied for the treatment of diabetic foot ulcers. Becaplermin, a recombinant platelet-derived growth factor product, was the first drug available for diabetic foot ulcers and underwent several prospective randomized placebo-controlled trials and a meta-analysis. 29 –31 In the meta-analysis, 50% of ulcers versus 36% with placebo gel healed at 20 weeks (28% delta). The patients in these trials, however, were well perfused and were clinically assessed as Wagner grade 2, making it difficult to compare with the findings from this study. Dermagraft, a human cellular-based product, produced a higher percentage (30%) of healed ulcers compared with controls (18%) in a single-blinded RCT that enrolled 314 patients (40% delta). Again in this trial, well-perfused Wagner grade 2 wounds were evaluated. 32 Apligraf, a human cellular bilayered construct, demonstrated a 56% versus 38% healing against controls at 12 weeks of therapy (32% delta). 33 Negative pressure wound therapy has also been studied with respect to diabetic foot ulcer healing. 34 The studies evaluating negative pressure have looked at surgical diabetic wounds and chronic wounds, whereas the advanced modalities have focused primarily on more superficial well-perfused noninfected Wagner grade 2 ulcers. Although achieving significance in efficacy trials, many of these methods have not performed as well in effectiveness evaluations due to the heterogeneity of the patients seen in a real-world clinical setting.
Needless to say, this study is a descriptive observational study and as such has limitations that must be recognized. It does, however, double the number of wounds available for healing outcomes, and by doubling our prior work makes this the largest study of its kind. The clinical procedures, policies, and protocols at the clinical sites have now consistently achieved similar repeatable healing outcomes at an aggregate rolled up population level, which implies adherence to the agreed-upon clinical practice guidelines developed by the company. This is a retrospective analysis and as such carries all the standard potential for bias that observational studies are known to be vulnerable to. However, the purpose of the study was to leverage a large database and standard outcomes reporting framework to identify the directionality and magnitude of possible treatment effects. Using the mITT method of outcomes reporting provides a consistent comparable measure by which to compare and analyze results and to more realistically calculate treatment effects that are achievable in an outpatient setting.
In Table 8, the overall wound-healing rate at the population level is reported as 75.9% and this drops to 72.3% when the data set is further modified to include the condition of diabetes. When the more advanced Wagner grades 3 and 4 diabetic ulcers located on the foot are used as filters, the healing rate drops to 56.04%. The use of any HBOT brings that value up to 60.01%, but when only completed HBOT cases are evaluated, the healing rate is 75.24%. Although big data analysis identifies correlations, it does not imply causation, so one could argue that those patients who complete their HBOT are healthier, have less comorbid conditions that would make completing their HBOT more likely, or any number of other hypotheses. A randomized study by Faglia et al. found a significant reduction in amputations when using HBOT, again in a controlled inpatient environment where treatment adherence was extremely high, providing further support for both the treatment and the need to complete the course of therapy. 35 For the purposes of this descriptive analysis, we stratified ulcers using the Wagner scale. However, there are currently a number of broader scoring systems that warrant consideration for future studies as well as other clinical characteristics that should be measured in subsequent analyses. 36,37
Summary characteristics
A further consideration should be to balance the cost of care relative to the likelihood of healing and the likelihood that the patient will complete treatment. If we make the case that Wagner grade 3 or 4 wounds on the foot that do not respond to standard of care can be healed at the overall rate for all wounds, we need to know how much we need to spend to achieve this clinical parity. What about recidivism? Overall mortality? The results of this big data analysis identify a potential set of patients for whom HBOT might provide a substantial improvement in wound healing. Other available advanced modalities have been proven to achieve significant improvements over controls for less severe cases and might offer a good option for those cases. Future studies should more completely explore questions related to patient adherence and possible incremental benefits of HBOT. Patients need to be engaged and adherent in order for this treatment approach to work. We are now looking at gaining more granularity into the vascular status of these patients, their social determinants of health, cost of care, and their recurrence rates over time to continue to provide the most value-based wound care possible for this complex group of patients. Ultimately, we need to use big data to help create value-based algorithms of care along a spectrum of various clinical complexities.
Innovation
This retrospective study has clinical relevance because it suggests HBOT can be effective for hard-to-heal Wagner grades 3 and 4 diabetic foot ulcers and demonstrates the complexities of studying the therapy using observational real-world data. Specifically, the results underscore the importance of treatment adherence when analyzing the effectiveness of HBOT. Furthermore, using the mITT framework to report healing outcomes allows for both transparency of results and the ability to compare programs, individual centers, and ultimately providers.
HBOT can be effective for hard-to-heal Wagner grades 3 and 4 diabetic foot ulcers.
Results underscore the importance of treatment adherence when analyzing the effectiveness of HBOT.
Using an mITT framework to report healing outcomes allows for both transparency of results and the ability to compare programs, individual centers, and ultimately providers.
Footnotes
Acknowledgments and Funding Sources
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author Disclosure and Ghostwriting
Hanna Gordon, PhD, and William J. Ennis, DO, are employees of Healogics, Inc. H.G. serves as the Executive Director of Research. W.J.E. is the Chief Medical Officer of Healogics. Enoch T. Huang, MD, MPH&TM, FUHM, FACEP, has no conflict of interest to declare. The content of this article was expressly written by the authors listed. No ghostwriters were used to write this article.
About the Authors